
Tear and serum electrolyte concentrations as a biomarker in primary glaucoma subjects
2021-02-07 04:56:10EzekielNkemakonamEkweremaduCharlesOgbonnaEzeh
Life Research 2021年1期
Ezekiel Nkemakonam Ekweremadu,Charles Ogbonna Ezeh
1Department of Ophthalmology,Enugu State University Teaching Hospital,Enugu,Nigeria.2 Department of Medical Biochemistry,University of Nigeria,Enugu Campus,Enugu,Nigeria.
Abstract Glaucoma progresses with stealth and late presentation is not unusual.This study explored the relationship between tear and serum ions concentration and glaucoma.The concentration of sodium,potassium and chloride in tear and serum of 50 glaucoma patients and 50 age and sex-matched controls were measured.Test and control groups had a mean age of 55.98 ± 11.91 and 52.24 ± 13.17 years respectively.The difference in their age was not statistically significant.Mean sodium,potassium and chloride concentrations (mmol/L) in tear of test subjects were 133.74 ±4.30,17.13 ± 1.74 and 125.54 ± 5.56 respectively while for control subjects,the values were 131.06 ± 6.39,21.40 ±1.57 and 122.86 ± 7.12 respectively.A paired comparison of mean between the 2 groups was statistically significant for potassium and sodium.A higher chloride ion concentration in test subjects was not statistically significant.The mean concentrations of sodium,potassium and chloride ions in the serum test subjects were 135.42 ± 3.84,4.07 ±0.66 and 101.00 ± 2.82 respectively while the mean concentrations in control subjects were 135.56 ± 3.84,4.14 ±0.69 and 101.58 ± 3.25 respectively.The comparison of means was not statistically significant.Sex did not significantly influence any of the measured variables but increasing age was related to decreasing potassium ion concentration in tear of glaucoma subjects in a statistically significant manner.Using a tear potassium concentration of 20 mmol/L as the lower limit of normal,the calculated sensitivity and specificity for making a diagnosis of glaucoma was 94% and 88% respectively.Low potassium ion concentration in tear of glaucoma subjects could be a useful biomarker in the disease but further research is needed.An effective glaucoma screening test can hold at-risk individuals from a greater distance of irreversible glaucoma blindness.
Key words:Tear,Glaucoma,Electrolytes,Biomarker,Apoptosis
Background
Glaucoma is a blinding optic nerve disease characterized by excessive attrition of retinal ganglion cells (RGC) by apoptotic death mechanism.Apoptosis in glaucoma is dysregulated and excessive,an equivalent of a physiological process gone rogue.The disease is characterized by a remarkable subterfuge because visual symptoms are delayed even as it progresses.Consequently,late presentation is the norm and glaucoma is the leading cause of irreversible blindness globally [1].It is projected that over 110 million individuals will be living with the disease and its burdens by the year 2040 [2].The population with the highest proportion of glaucoma-related blindness is found in Sub-Saharan Africa and other African-derived populations [3].In Nigeria,widespread superstition,endemic poverty and restricted access to quality eye care have created a fertile ground for late presentation of the disease [4].People of Igbo ethnic extraction,the predominant ethnic group in our study area,seems to be the most affected in Nigeria [5].Primary Glaucoma manifests in the absence of underlying eye disease and accounts for most glaucomas encountered in clinical practice (92% of all glaucomas).Secondary glaucoma is much less common (8% of all glaucomas) and is an occasional complication of significant eye trauma.The primary glaucomas are further sub-classified according to the anatomical configuration of the aqueous humour outflow structure as Primary Open Angle Glaucoma and Primary Angle-Closure Glaucoma.Primary Open Angle Glaucoma accounts for up to 70% of primary glaucoma and it is the predominant phenotype seen in people of African descent [6].
The list of candidate genes linked to glaucoma is growing and their expression may lead to reduced facility of aqueous humor outflow with an attendant increase in intraocular pressure (IOP) [7,8].The optic nerve appears to be vulnerable in its transit through the rigid posterior sclera.An increase in IOP can induce biomechanical changes injurious to the nerve at this point of exit [8].Additional mechanisms in glaucoma include ocular tissue ischemia and oxidative stress affecting both the trabecular meshwork and retinal elements [9].Ambient t light contains ultraviolet (UV)radiation which is normally absorbed by the cornea and the lens before it gets to the retina where it may be cytotoxic.Traces of ultraviolet-B (UVB) radiation do eventually reach the anterior chamber and the retina despite these tissue filtrations.UVB increases the tissue level of reactive oxygen species (ROS) that in turn upregulates the expression of apoptosis-related genes in a time-dependent manner [10].In the retina,ROS tissue level is further amplified by the mitochondrial energy generation through oxidative phosphorylation which is critically needed by unmyelinated nerves such as RGC.Oxidative phosphorylation inevitably leads to the leakage of highly reactive unpaired electrons.Both mechanisms can combine and raise ROS to pathological levels [11].Cells with high concentrations of ROS experience oxidative stress that can alter electrolyte flux across RCG cell membrane in manner that favors accelerated apoptosis seen in glaucoma [12,13].
Potassium (K+) is the principal intracellular cation while sodium (Na+) is the major extracellular cation.These positive ions are associated with negative anions,principally chloride (Cl-) and bicarbonate (HCO3-) to ensure electrical neutrality in the two compartments[14].The maintenance of this concentration gradient is principally mediated by the Na+/K+electrogenic pump.These electrolytes,which exist as ions in blood and tear,are electrically-charged inorganic molecules and mediate various physiological functions including fluid balance,impulse transmission and protection of cellular functions [15,16].A low level of extracellular potassium can cause its efflux from the intracellular to the extracellular fluid compartment resulting in contraction of cell volume.Cytochrome-c diffuses into the cytosol from the mitochondria,committing cells to intrinsic apoptotic death mechanism [17-21].Agents that block K+channels such as barium ion (Ba2+) or high extracellular K+have been shown to prevent apoptosis[22].High potassium concentration in tears helps in maintaining cornea epithelium by reducing the electrochemical gradient between intracellular and extracellular levels thus attenuating intracellular loss of potassium and minimizing cornea epithelial loss by apoptosis [21,23,24].A healthy cornea epithelium is a more efficient absorber of UVB,potentially preventing distal damage to vulnerable ocular tissues notably the trabecular meshwork,lens and RGC [10,25].To a lesser degree,perturbations of intracellular sodium and chloride concentrations have also been linked to increased cell death by apoptosis [26,27].
Biomarkers are entities within the body capable of providing impartial information regarding the current physiologic state of a living organism [28].Tear offers an advantage as a body fluid for study because of the ease of its collection in a non-invasive manner,being an exterior (proximal) fluid.Tear electrolyte concentration principally determines its osmolarity which is the basis for the diagnosis of dry eye disease (DED) [29].Studies have suggested that the measurement of certain tear electrolytes could be a useful adjunct in the assessment of patients with diabetes mellitus [30,31].Advances in tear Proteomics is currently being exploited in a frenzied “man-hurt” for biomarkers in tear of glaucoma patients [32,33].Hagan et al have done an excellent review of proteomic techniques in research for tearrelated biomarkers in ocular and systemic diseases [34].
Serum is derived from clotted blood and with whole blood,is the “guinea pig” of laboratory medicine.Higher chloride concentration,red blood cell count and immunoglobulin-G concentration have been reported in the blood and sera of glaucoma subjects [35].
Tear and serum concentrations of the major extracellular fluid ions namely sodium,potassium and chloride will be measured in glaucoma subjects and ageand sex-matched controls in this study.The findings will be discussed in the context of any association(s)between the measured variables and the presence or absence of glaucoma phenotype.
Methods
Study design
This was a case-controlled cross-sectional hospitalbased study of eligible and consenting adult subjects attending the eye clinic of Enugu State University teaching hospital,Parklane,Enugu.Enugu is a cosmopolitan city located on latitude 6° 27' 35.8704'' N and longitude 7° 32' 56.2164'' E in south-eastern part of Nigeria with about 722,664 inhabitants [36].The study was done between December 2nd,2015 and February 25th,2016.A primary glaucoma prevalence of 2.1%among adults aged 30 years and above was reported in a population-based study done in south-eastern Nigeria by Ekwerekwu and Umeh in 2002 [37].This prevalence and age limit were adopted for the present study.
(1) The estimated sample size for the study was calculated with Cochran equation for sample size as under [38]:
Where n = required sample size,t = confidence level at 95% [1.96],P = estimated prevalence of primary glaucoma at 2.1%,m = margin of error at 5% [0.05].
(2) Substituting the values:

Correcting for contingencies including patient attrition.
(3) Final sample size is:

The final sample size was adjusted upwards to fifty(50) subjects after unsuitable subjects have been excluded to enhance the validity of the study.Fifty (50)age- and sex-matched subjects were recruited to serve as controls.
Ethical clearance was obtained from Health Research Ethics Committee of Enugu State University Teaching Hospital,Park Lane,Enugu (Appendix I).The tenets of the Helsinki Declaration regarding the conduct of research involving human Subjects were adhered to[39].Informed verbal consent was duly obtained from all the participants (Appendix II).
Inclusion and exclusion criteria
A total of 100 patients with completed questionnaires and valid test results were analyzed in the study.Out of these,50 subjects were glaucoma patients and henceforth may be referred to as “test subjects”/group and 50 non-glaucoma subjects that served as control and henceforth may be referred to as “control subjects”/group.
The inclusion criteria for test subjects were age of 30 years or above and a diagnosis of glaucoma as evidenced by a pale or absent neuroretinal rim,vertical cup to disc ratio ≥ 0.7 and associated visual field abnormalities [40.41].In control subjects,the inclusion criteria were age of 30years or above and absence of glaucoma as evidenced by a pink neuroretinal rim,a vertical cup to disc ratio > 0.6 and intraocular pressure of > 21 mmHg and the absence of family history of glaucoma.
In bothgroups,age less than 30 years,presence of metabolic disease especially diabetes mellitus or chronic systemic disease,use of elemental supplements,presence of ocular surface disease and pregnancy were exclusion criteria [42,43].Presence of diabetes mellitus was further excluded with a fasting or random blood sugar of 126 mg/dl (7.0 mmol/L) for fasting plasma glucose and value of ≥ 200 mg/dl (11.1 mmol/L) for random blood sugar using Accu-ChekR Active (Roche)glucometer [44].
Demographic and medical history of study subjects were filled using a standardized questionnaire(Appendix III).The visual acuity of each eye was tested using Snellen’s chart.Both eyes were examined under magnification with a slit lamp biomicroscope (Haag Streit BM900R) and GoldmannR three-mirror goniolens to exclude causes of secondary glaucoma.IOP was measured with Haag Streit Goldmann R-type applanation tonometer.The posterior pole with emphasis on the optic nerve heSad was examined with a + 78D superfield aspheric lens by VolkR (USA).
A central visual of field test was done using OptopolTM 1000 projection perimeter.A CVF test done within 3 months of commencement of the study was accepted as valid.All examinations were done or supervised by the principal investigator.Representative central visual field tests of a test and a control subject are shown in appendix IV and V.
Sample collection and analyses
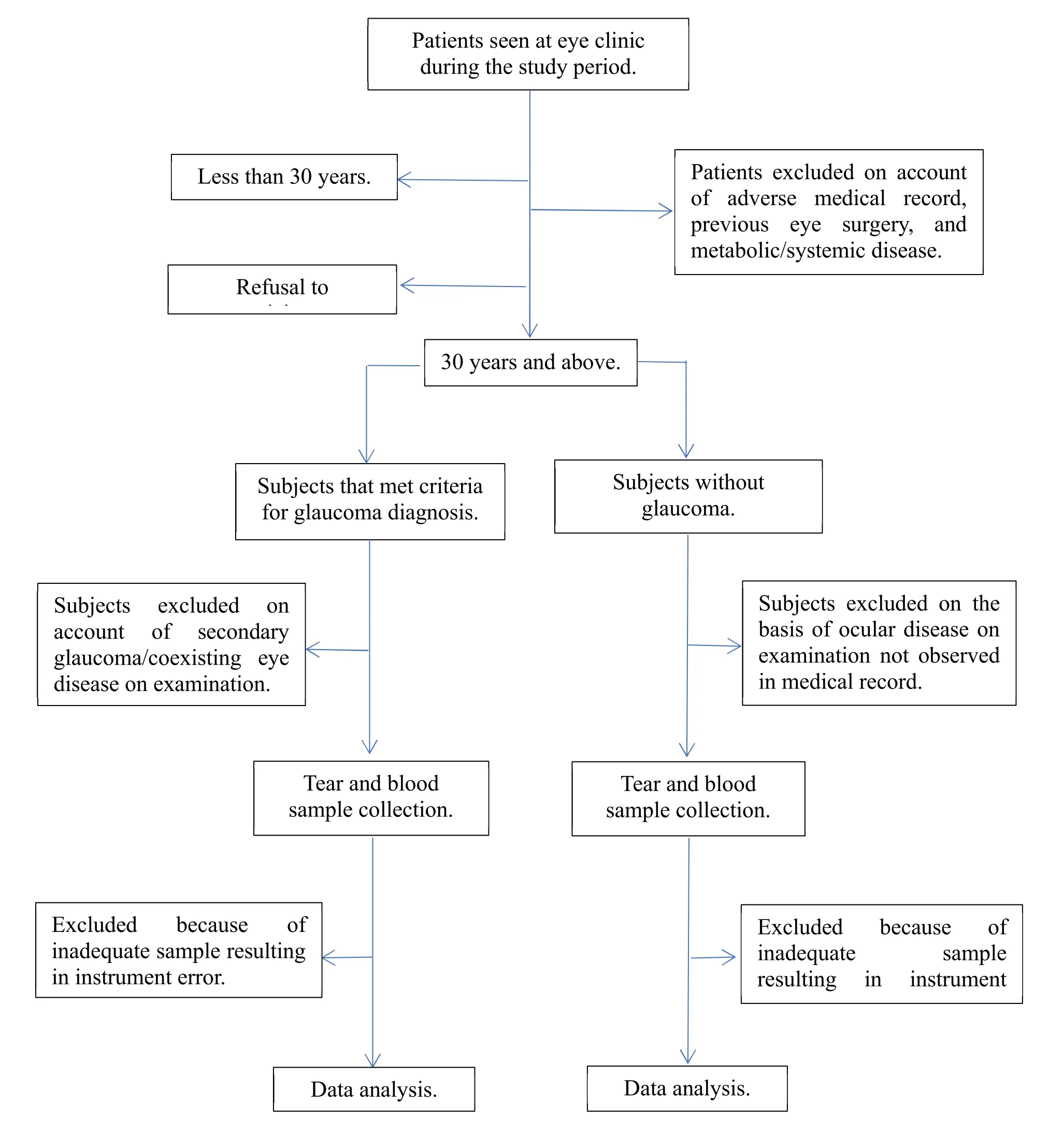
Figure1 A flowchart showing the reticulation of research subjects.
All samples were taken between 10 am and 12 pm to minimize the effect of diurnal variation on electrolyte composition of body fluids [45].Four milliliters of the venous blood sample was collected from the antecubital vein with a sterile 5 mL hypodermic needle and syringe and transferred to a sterile plane glass tube.The blood was allowed to stand for 30 minutes to clot and was centrifuged with TechmelTM centrifuge (USA) at a speed of 5,000 revolutions/minute to yield a supernatant serum.
200 ul of tear sample was collected from the inferior lateral tear meniscus of the ocular surface with a dry and sterile 50 ul plane capillary tube over four collections and emptied into a sterile plane glass test tube [46].Basal tear collection is difficult in practice,even from anesthetized cornea [47].However,basal and reflex tears seem to differ mainly in their protein content [48-50].Tilting the head facilitates tear collection from the lateral canthal area and contact with the conjunctiva was avoided to minimize reflex tearing.Tear sample was taken from a maximum of 4 subjects (test and control)per weekday considering the time needed to obtain adequate tear volume required for a valid result from the measuring instrument.Both serum and tear samples were analyzed as native samples within two hours of sample collection using ST-100B electrolyte analyzer by Sensa CoreR,Hydarabad India,an automated electrolyte analyzer which operates on the principle of direct ion selective electrode (ISE).The electrolyte tests were carried out by the same laboratory scientist who was blinded with respect to whether the sample was from a test or a control subject.The flow chart below illustrates the pattern of progression of the subjects during the study (Figure1).
Statistical analysis
The measured variables were presented in tables,chart and prose.Data analysis was done with SPSS version 16 (SPSS,Inc,Chicago,USA).Bivariate analysis was performed using cross-tabulations and 2-tailedt-test was used to evaluate associations between means of tested variables with the calculatedP-value stated.A value ofP< 0.05 was considered statistically significant.Multi-linear regression was used to analyze associations of age and the various electrolyte concentrations.Diagnostic accuracy test was performed to determine sensitivity and specificity of the test.
Results
Measurement of tear and serum concentrations of sodium,potassium and chloride ions from 25 females and 25 males were analyzed in the test group and 26 females and 24 males in the control group.The test subjects were older in age with a mean age of 55.98 ±11.91 years while the control group had a mean age of 52.24 ± 13.17 years (Table1).However,this age difference was not statistically significant (P= 0.140).The mean sodium,potassium and chloride concentrations in tear of test and control subjects(mmol/L) were 133.74 ± 4.30,17.13 ± 1.74,125.54 ±5.56 and 131.06 ± 6.39,21.40 ± 1.57,122.86 ± 7.12 respectively (Table2).The means of the two groups were compared and theP-values were 0.019,< 0.001 and 0.056 for sodium,potassium and chloride concentrations respectively,implying a significant difference in sodium and potassium concentrations between the 2 groups.Although chloride concentration was higher in the tear of test subjects,this was not statistically significant (P= 0.56).The mean sodium,potassium and chloride concentrations in the serum of test and control subjects (mmol/L) were 135.42 ± 3.84,4.07 ± 0.66,101.00 ± 2.82 and 135.56 ± 3.84,4.14 ±0.69,101.58 ± 3.25 respectively.A comparison of the means in the 2 groups hadP-values of 0.860,0.630 and 0.900 for sodium,potassium and chloride respectively.TheseP-values imply that no statistically significant electrolyte concentration existed in the serum of test and control groups.These comparisons are further illustrated in Figure2.
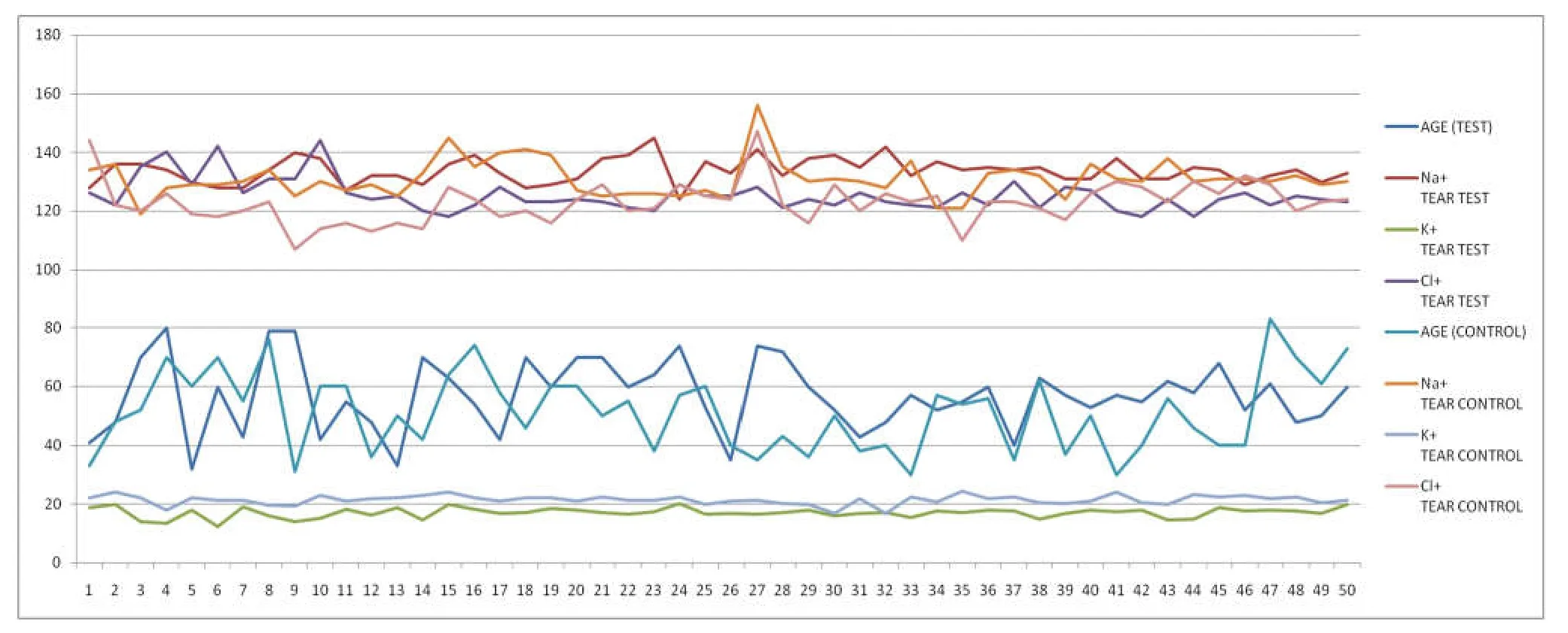
Figure2 Composite graph comparing tear electrolytes in test and control subject in relation to their ages.The composite graph shows the interplay of all the tear parameters in both the test and control groups and the age of the subjects.The graph in the top panel shows the sodium and chloride concentrations in serum against their concentration in tear.The graph in the middle panel represents the ages of the subjects while the graph in the lowest panel highlighted the relationship between potassium ion concentration in tear of test and control subjects.The vertical axis represents the various ionic concentrations while the horizontal axis stands for the consecutive subjects.
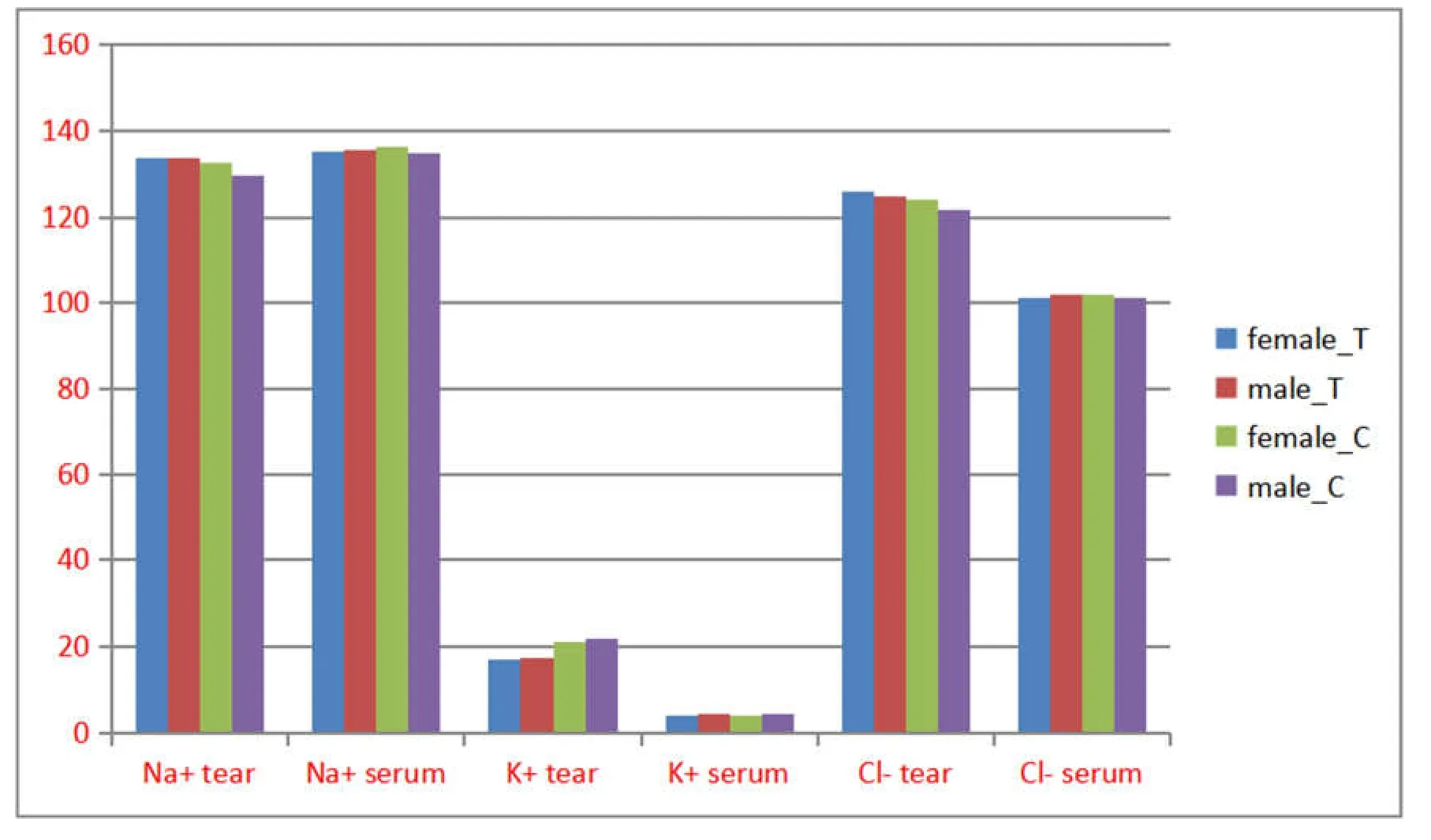
Figure3 Comparison of mean electrolyte concentration in the tear and serum of test and control subjects according to sex (concentrations in mmol/L).There was a consistently higher sodium electrolyte among female subjects in serum of both test and control subjects.The same trend can be observed in tear chloride concentration but these were not statistically significant.Tear potassium ion concentration was however higher in males in both test and control subjects compared to female subjects.Female_T,mean electrolyte concentration of females in test subjects; Male_T,mean electrolyte concentration of males in test subjects; Female_C,mean electrolyte concentration of females in control subjects; Male_C,mean electrolyte concentration of males in control subjects.
On the basis of sex,females in the test group had higher sodium and chloride concentrations while males had higher potassium concentration in tear.The correspondingP-values were 0.355,0.524 and 0.683 respectively and were not statistically significant (Table3).In the serum of the same group,males had higher sodium,potassium and chloride but the differences were not statistically significant; 0.475,0.793 and 0.324 respectively.In the tear of control group,sodium and chloride concentrations in female were higher than in males while potassium concentration was higher in males.The correspondingP-values were 0.054,0.897 and 0.060 and were not statistically significant.In the serum of the control group,females also had a higher sodium and chloride concentrations than males while males had a higher potassium concentrations withPvalues of 0.477,0.159 and 0.297 respectively.None was statistically significant.A bar chart representation is depicted in Figure3.
A multiple linear regression was done using age as a predictor of electrolyte concentration in both tear and serum of both groups.A negative correlation of decreasing potassium concentration with increasing age was seen in tear of test subjects (R2= 0.997,F= 1050 andP< 0.000*).The poorest fit was seen in tear chloride concentration (R2= 0.000,F= 0.000 andP=0.987) (Table4).

Table1 A statistical analysis of comparison of mean age between test and control groups
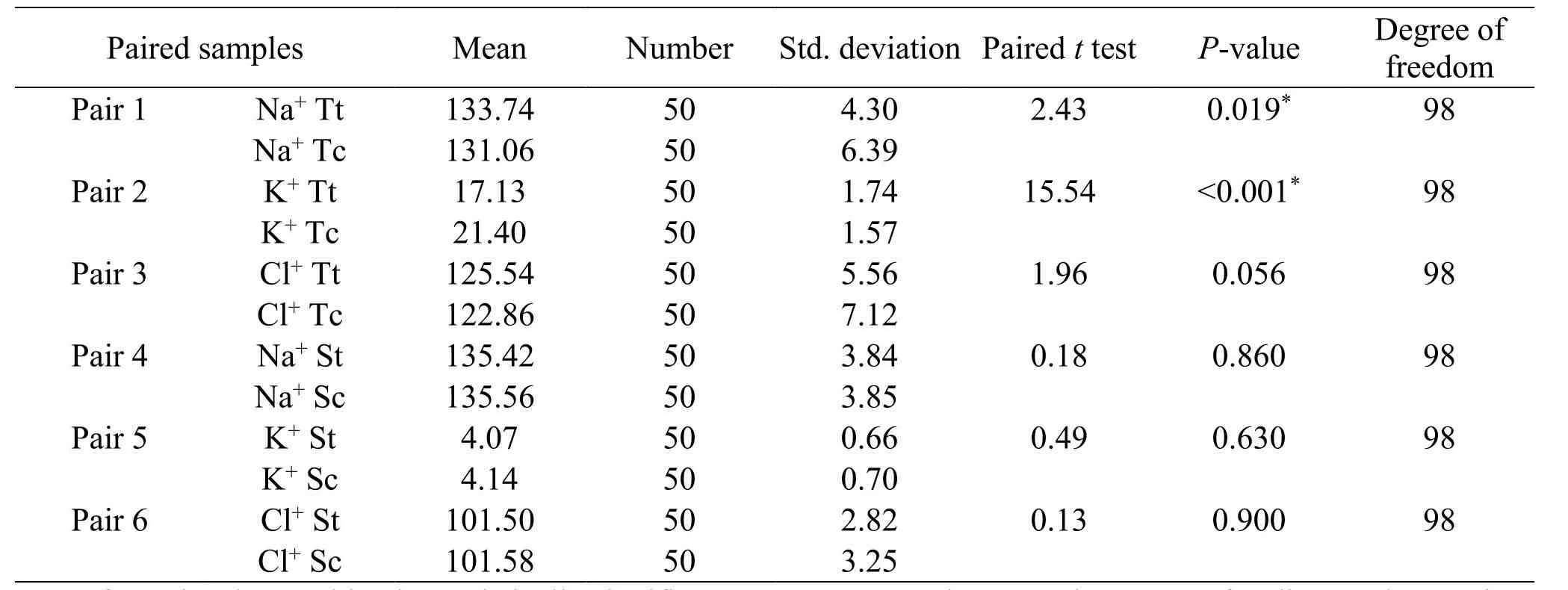
Table2 A paired sample statistics between test and control subjects and their electrolyte concentrations
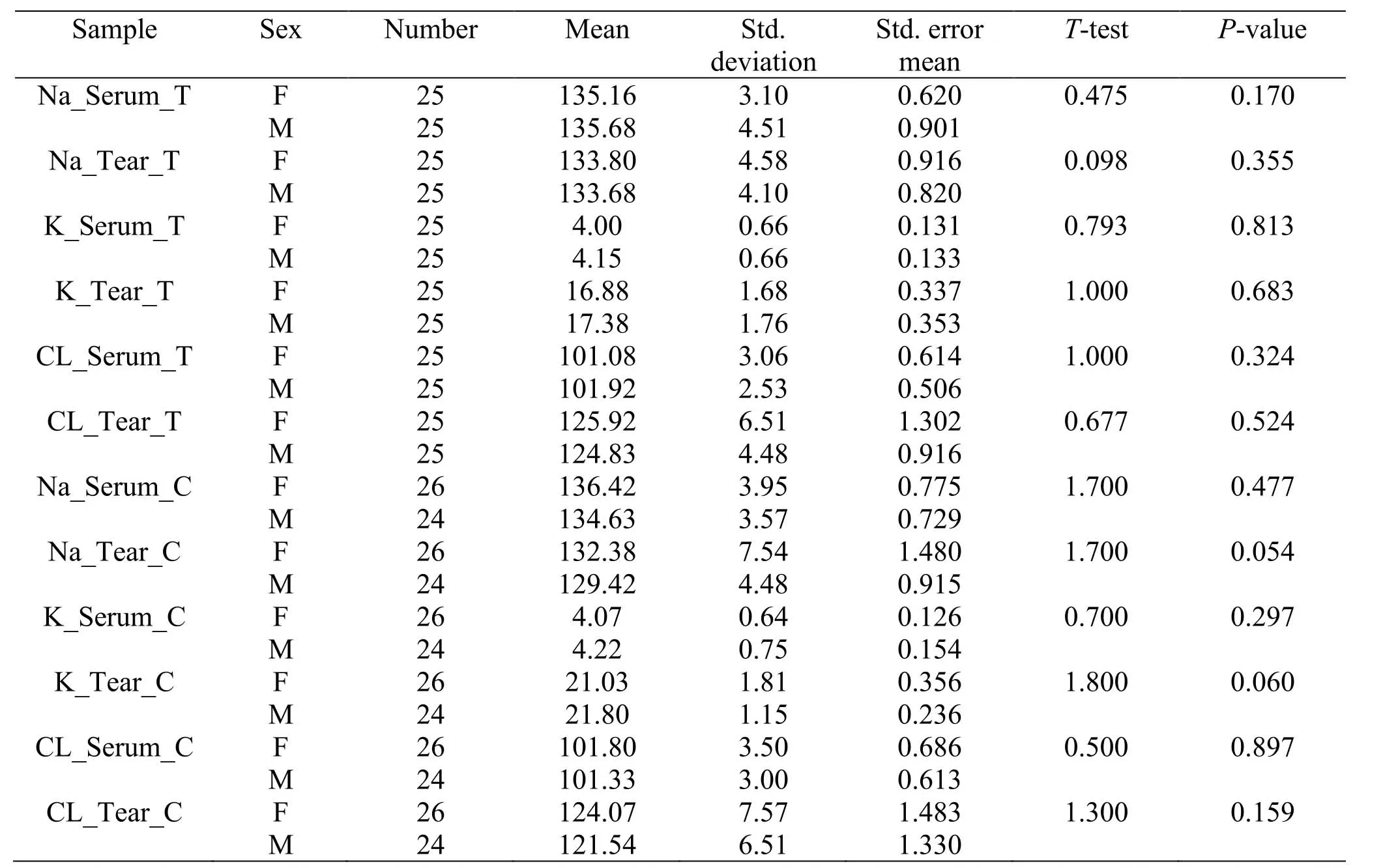
Table3 A comparison of electrolyte concentrations between female and male subjects in both test and control groups

Table4 A multiple linear regression using age to predict the concentration of tear and serum electrolytes in the 2 groups
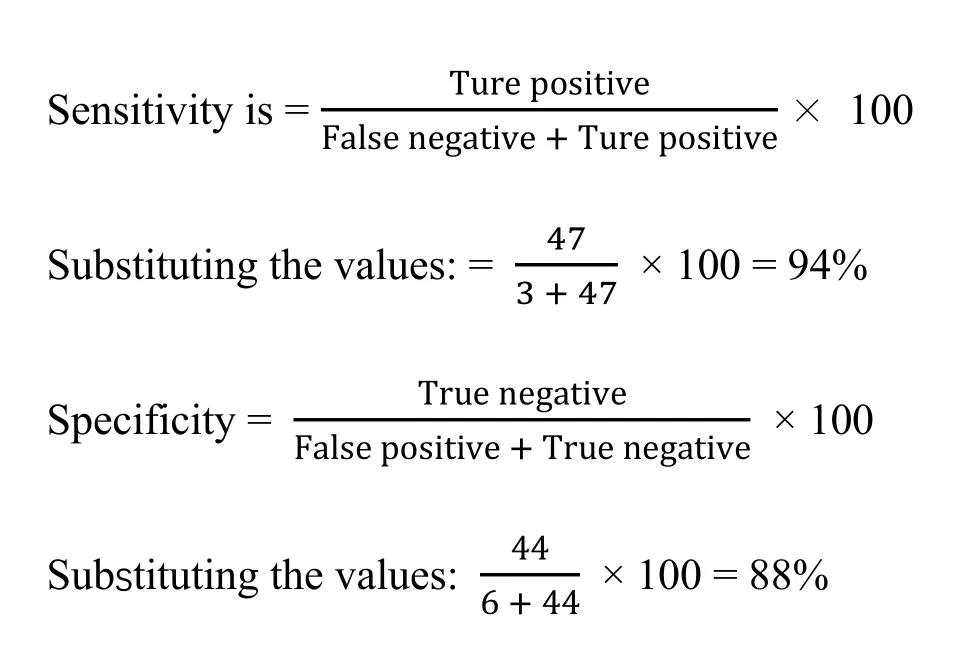
Diagnostic accuracy test
The sensitivity of a clinical test is the probability that a test gives a positive result when a disorder is present,while specificity is the probability that a test gives a negative result when the disorder is absent.In this study,mean tear [K+] between test and control subjects had the strongest significance (P< 0.001).Using 20 mmol/L as the cut-off point between normal and abnormal [K+].The diagnostic accuracy tests were calculated as under:
Discussion
Glaucoma is an eye disease of major public health importance.There is no overstating the relevance of an affordable and effective test that can detect the nascent stages of the disease since no cure is presently possible and its blindness is irreversible.In the present study,the concentration of major cations and anion namely sodium [Na+],potassium [K+] and chloride [Cl-] in tear and serum of 50 primary glaucoma and 50 nonglaucoma control subjects who were 30 years and above were assayed.Both groups were sex- and aged-matched(Table1).The mean electrolyte concentration in tear of both test and control subjects showed that both groups had significantly higher [K+] and [Cl-] but lower [Na+]when compared to the serum of the same group (P<0.05,P> 0.05 andP= 0.42 respectively) (Table2).These concentration disparities have been documented in other studies,even with different measuring algorithms [23-25].It has been suggested that there is an active secretion of K+and Cl+into tear fluid by apical acinar cells of the lachrymal gland [51-52].Studies have shown that high tear [K+] is essential in maintaining a proper cornea epithelial thickness which in turn can mitigate both proximal and distal UVBinduced cell injury including RGC death [22,25].
In the present study,the mean [K+] in tear of test subjects was found to be significantly lower than the mean of control subjects (17.13 mmol/L and 21.40 mmol/L respectively,P< 0.001).A multivariate linear regression analysis using age to predict electrolyte concentration showed that a significant decrease in tear[K+] occurred with increasing age in test subjects but was not observed in the control group (Table4).No related study was seen in literature that can be used to make comparisons with these findings.However,it is known that older age is one of the major risk factors for glaucoma [53].It is possible that a compromised corneal epithelium as a result of low tear [K+] can affect its ability to absorb incident UVB,potentially exposing the trabecular meshwork elements and RGC to the damaging effect of UVB.It might also represent a generalized abnormality in potassium channels that predispose affected cells to increased apoptotic death.Further research will be needed to clarify these observations.The significance of higher [Na+] in tear of test subjects compared to controls (P= 0.019) is unclear but it might be a compensatory mechanism to offset the high [K+] or vice-versa.Further appraisals are needed.Paucity of published data makes drawing inferences from these results conjectural.Sex was not a significant determinant of electrolyte concentration in both tear and serum (P> 05) (Table3).However,the mean concentrations of sodium and chloride were higher than potassium concentration in tear of test and control subjects and vice versa.
The serum concentration of the 3 electrolytes in the glaucoma group was similar to values observed in the control group and no significant variation occurred(Table2).The values in the present study appeared to be in a median position when compared to results of studies done within the country and elsewhere [54-57].It thus appears that different instruments which employ different measurement principles (flame photometry versus ion selective electrode) give different results and that has to be considered in the interpretation of any given result.One study found chloride in significantly higher concentration in the serum of glaucoma subjects when compared to controls [35].While there was a higher chloride concentration in the serum of test subjects when compared to controls in this study,the difference was not statistically significant (P= 0.90).The lowest concentration of potassium in tear considered to be normal as seen in literature was 20 mmol/L.This value was adopted in this study for the calculation of sensitivity and specificity of glaucoma screening using tear [K+].A sensitivity and specificity of 94% and 88% respectively were obtained which if replicated in other studies,could make for a possible use of [K+] as a stand-alone test or adjunct in glaucoma screening protocols.
The strength of case-controlled studies lies in the fact that both test and control subjects are tested with the same instrument(s) within the same time frame thereby effectively eliminating the problem of differential lab measurement error.The native samples were used to avoid any confounding influence of diluting fluid.The same number of test and control subjects were tested and were weighted for sex and age.On the downside,the use of hospital patients who might not reveal all aspects of their medical history cannot be excluded.That reflex tearing occurred cannot be totally excluded in the course of obtaining tear sample and its effect on measured variables is unknown.However,it is reasonable to assume that this affected both test and control tear samples and is unlikely to invalidate the findings in this study.A cause-effect relationship between low tear potassium concentration and development of glaucoma cannot be drawn from the findings in this study and will await further research.A larger population-based study with ‘virgin’ treatmentnaïve eyes will generate a more reliable data.
Conclusion
Human cells are subject to the modulating influence of the major electrolytes in health and disease.Potassium is the major intracellular cation but its extracellular concentration can lead to changes in cell volume which is a harbinger of a programmed cell death.The present study did show that the ocular surface of glaucoma subjects is exposed to low tear [K+] in an age-dependent manner.There is need to improve the ease of collecting tear sample and standardizing its measurement to enhance the feasibility of using this fluid for populationscale glaucoma screening.The role of potassium and its secretory channels in the evolution of glaucoma phenotype will await further research and by extension the suitability of tear [K+] as a biomarker in glaucoma.Its relationship to IOP,positive family history and severity of the disease can be litigated in follow-up studies preferably of prospective and large-scale nature.Understanding these relationships might lift the veil in the epistemic limitations that has hindered progress in an early and effective management of glaucoma.That will represent a significant advance in combating the misery of ocular morbidity and mortality that glaucoma has come to represent.
- Life Research的其它文章
- Science in Chinese medicine
- Artificial intelligence and the future of medicine:a multidimensional analysis
- Growth retrieval of stressed bacterial cells:logic and contradictions
- Amyloid beta peptides,tau protein acetylation and therapeutic strategies for treating Alzheimer’s disease:a review
- A cross-sectional study of the relationships between ethnicity and occupational classes with mental wellbeing in the UK
- Aqueous wood-ash extract of Parkia biglobosa causes reproductive toxicity in female mice