
Epidemiological characteristics and disease spectrum of emergency patients in two cities in China: Hong Kong and Shenzhen
2020-12-09 05:40ShaoxiChenKarrenFanLingpongLeung
Shao-xi Chen, Karren Fan, Ling-pong Leung
1 Accident and Emergency Department, University of Hong Kong-Shenzhen Hospital, Shenzhen 518053, China
2 University of Hong Kong, Hong Kong, China
Dear editor,
China is the most populated country and the second economic entity worldwide. Hong Kong and Shenzhen are two adjacent cities in southern China, with similar environmental, cultural, ethnic groups, and economic development. They both have a very interesting turning point in their destiny, leading to a miraculous economic development. However, their government structure and health care system are totally different.[1]This is a vivid example of Deng Xiaoping’s formulation of the principle of “one country, two systems”.[2]
Emergency medical service reflects the basic capacity of health service in a region. The government of China improved the emergency medical system after the 2003 SARS outbreak.[3]But the emergency medicine developed unevenly across regions.[4,5]Shenzhen ranks the first economic city in China and had dramatical improvement of emergency medical services in the past decades. Thus, the performance of emergency medical system in Shenzhen is informative for further development of emergency care systems in other regions.[6,7]The data of epidemiological characteristics and disease spectrum helps to allocate first-aid resources reasonably,earlier detection and differential diagnosis, improve work efficiency and quality in emergency department, which is important and valuable reference on management and construction for emergency department.
To date, limited reports are available on epidemiological characteristics and disease spectrum in the emergency department.[3,8]The Hongkong Emergency Hospital and the Shenzhen Hospital of University of Hong Kong in Shenzhen are emergency centers in both cities and had well-established electronic medical record(EMR) system. The emergency medicine (EM) model in Shenzhen followed the Hongkong model, thus the differences between the EM in Shenzhen and Hong Kong provide valuable information for other areas where struggle for western EM models. The differences of these hospitals may provide new ideas for the clinical, teaching and research cooperation. Therefore, the objective of this study was to compare the epidemiological feature and disease spectrum of patients in emergency departments in these hospitals during the period from 2013 to 2016.
METHOD
This is a cross-sectional observational study examined EMR data of all emergency admissions at study hospitals between May 2013 and June 2016.
Study setting
Both Hongkong Emergency Hospital and the Shenzhen Hospital of University of Hong Kong in Shenzhen are large urban teaching hospitals and major emergency centers. Both hospitals locate in the central area of the city. The annual attendance volume of emergency in Hongkong Emergency Hospital was 19,528 cases. During the study period, the attendance volume fluctuated slightly, but there was no significant change. For Shenzhen Hospital, the attendance volumes increased from 267 cases in May 2013 to 10,953 cases in March 2016.
Patients
All emergency department attendees with completed electronic clinical data were included, incorporating both ambulatory and ambulance service presentations. The study period was limited from May 2013 to June 2016.The re-visit patients and unknown gender patients with the unique medical record ID were excluded from the analyses.
Data collection and analysis
The following data were collected from the MHR databases in emergency departments in two hospitals:patient ID, age, gender, mode of arrival, arrival and departure time, waiting time, visiting month, chief complaints, final discharge diagnosis. The statistical analyses were performed using SPSS 17.0 (Chicago,IL, USA). The normality of the data distribution for continuous variables was verified by the Kolmogorov–Smirnov test. Regarding continuous variables, Student’s t-test was used for normally distributed variables.Because this is an explorative analysis, the sample size was not calculated. The continuous variables were expressed by mean and standard deviation (SD). The chisquare test was used to analyze the categorical variables.A P-value less than 0.05 was considered as statistically significant.
RESULTS
This study included 686,837 patients from Hongkong Emergency Hospital and 183,389 patients from Shenzhen Hospital of University of Hong Kong. The sex proportion of patients in both hospitals was similar, with male of 49.18% in Hong Kong and of 48.18% in Shenzhen. The patient age ranged from 20 days to 110 years in Hong Kong and from 6 days to 116 years in Shenzhen (Figure 1A). The emergency patients from Hong Kong hospital was significantly older than that in Shenzhen hospital(P=0.0478), with the mean age of 46.61±22.68 in Hong Kong and 25.22±19.75 in Shenzhen, respectively (Figure 1B). In Hong Kong hospital, 17.03% patients were under 18 year old and 23.08% patients were aged over 65 years. In Shenzhen hospital, 44.98% patients were aged under 18 years and only 4.76% patients were aged over 65 years.
Figure 2 shows the pattern of whole day visiting time in both hospitals. In Shenzhen hospital, the trough of attendance volume was at 5:00 am, and the visit patients significantly increased at 8:00 am. The majority (80%)of patients arrived hospital from 8:00 am to 20:00 pm.There were three peaks in the whole day, including 10:00 am, 14:00 pm, and 20:00 pm. In Hong Kong hospital,the trough of attendance volume was at 4:00 am, and the visit patients significantly increased at 8:00 am. The three peaks of the visiting volume were 9:00 am, 15:00 pm and 20:00 pm. The 9:00 am was the highest peak in the whole day.
The waiting times showed skewed distribution in two hospitals (Figure 3A). The median waiting time was 13 minutes in Hong Kong and 14 minutes in Shenzhen.The average waiting time in Hong Kong hospital was significantly longer than that in emergency department in Shenzhen hospital (Figure 3B), with 104.75±20.63 minutes in Hong Kong and 42.15±15.78 minutes in Shenzhen (P=0.002), respectively.
Figure 4 shows the distribution of visiting month and season in two hospitals. In Hong Kong, the attendance volume was highest during May and June, and no significant difference in other months (P>0.05). In Shenzhen, the attendance volume was highest in June and lowest in February. The attendance volume was highest in Summer, followed by Spring, Autumn, and lowest in Winter.
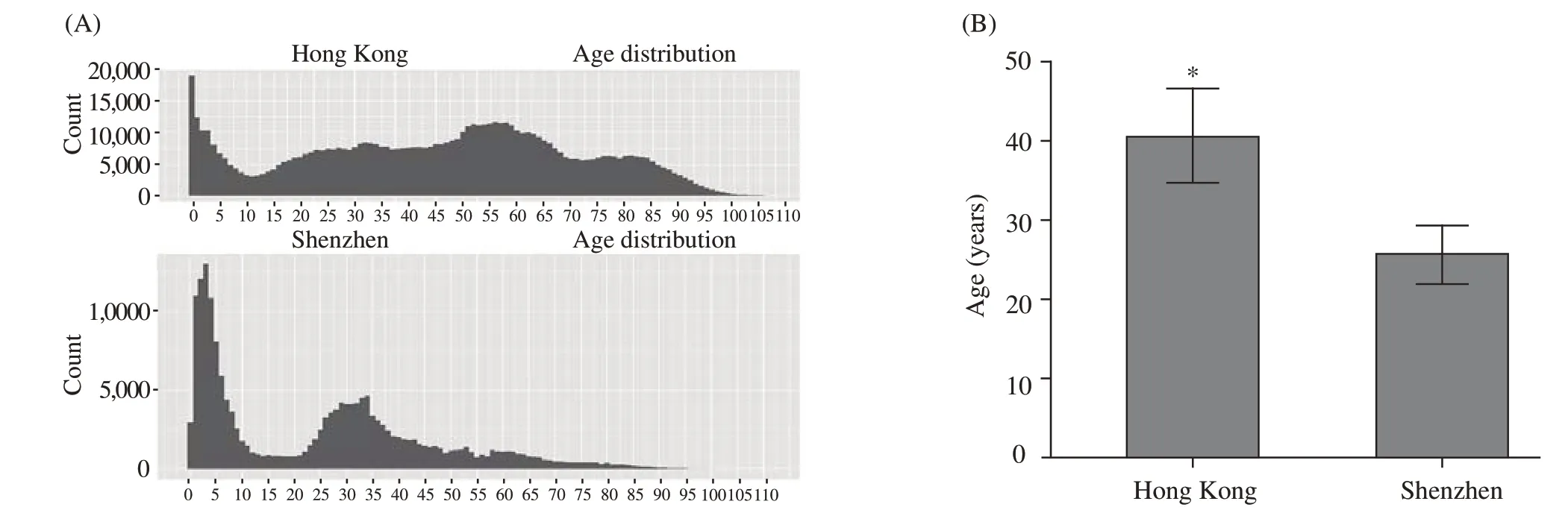
Figure 1. Age distribution of emergency attendees in both hospitals. A: age distribution area map; B: age distribution histogram.
Table 1 shows the disease spectrum of emergency department in both hospitals. In Hong Kong, the most common disease was respiratory system diseases(22.89%), followed by digestive system (19.91%), cardio cerebral vascular system (12.72%), urogenital system(11.50), trauma and poisoning (9.42%). In Shenzhen,the top five diseases were digestive system (22.69%),respiratory system (17.62%), genitourinary system(13.94%), nervous system (12.23%), and the trauma and poisoning (8.91%).

Figure 2. Distribution of visiting time in both hospitals in the whole day.
Table 2 shows the common diagnosis of emergency in Hong Kong and Shenzhen during the period between 2013 and 2016. The upper respiratory tract infection,cough, pharyngitis, tonsillitis were the most common diseases of emergency visiting in both hospitals.
DISCUSSION
This study firstly analyzed the epidemiological characteristics and disease spectrum in emergency departments in Hong Kong and Shenzhen. The results showed that the emergency patients in Hong Kong were older than those in Shenzhen, with 20% and 5% of patients aged over 65 years. The majority of patients inboth hospitals were middle-aged people (20–65 years old). The time of peak visiting in two cities was similar,with peak at 9:00–10:00 am and trough at 5:00 am in the whole day. The pattern of visiting time in both hospitals was different, with a single peak distribution in Hong Kong and three visiting peaks in Shenzhen. Hong Kong had longer waiting time for emergency service than Shenzhen (104.75 vs. 42.15 minutes). Both cities had highest volume of attendance in summer and lowest in winter. The diseases of respiratory system and digestive system were the most common cause of emergency visiting.

Table 1. Disease spectrum of emergency department in both hospitals

Table 2. Top 15 causes of emergency in both hospitals in 2013–2016
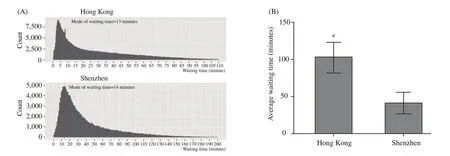
Figure 3. Distribution of patient waiting time in both hospitals. A: waiting time area map; B: waiting time histogram.
The younger patients in Shenzhen compared to Hong Kong may be related to the difference in the age structure of the population in both cities. Hong Kong is an aging society, while Shenzhen is a young immigrant city. The life expectancy in Hong Kong was 81 years for men and 86 years for women.[1]The majority of the people in Shenzhen are young workers from different provinces across the nation, with the median of age of 30 year old.There are 14% people in Hong Kong aged 65 years and older, whereas only 2% in Shenzhen.

Figure 4. Distribution of visiting season and month in both hospitals.
The time of peak visiting was similar in both hospitals (9:00–10:00 am), which is consistent with the normal schedule and social activities time in the population. However, the overall pattern of visiting time differed in both hospitals. Hong Kong showed a single peak distribution after 9:00, whereas Shenzhen showed three visiting peaks like hump in the whole day. This may be related to the difference in emergency system. The public hospitals in Hong Kong adopted an emergency triage system.[9]The patients were arranged to treating areas and order according to the severity of the condition. Triage allowed critical patients to receive the fastest treatment, on the one hand, to exclude patients who do not belong to the emergency department, to avoid the waste of emergency resources. This model was introduced to Shenzhen, but it was not strictly adopted.The several visiting peaks in emergency department in Shenzhen may be related to attendance of non-emergency patients.
This study showed that in Hong Kong the average visiting time was significantly higher than that in Shenzhen hospital, which may be related to different triages in two hospitals. Emergency triage system divided the patients into 5 levels, level I patients with medical treatment immediately, the waiting time of patients with level II 5 minutes, the waiting time in patients with level III <30 minutes, levels IV and V in patients with stable disease, no waiting time, so some mild illness, no lifethreatening patients waited a long time.[10]The health system in Hong Kong is well established and aligned with international standard. The biggest shortcoming was a prolonged waiting time, with 90% of the patients waiting for as long as 60 days for surgery since diagnosis. However, even the marginalized groups of the society have easy access to high quality treatment.

Temperature and seasonal pattern have been documented to be associated with emergency attendance in several cities.[11,12]It was reported that all-cause mortality was around 30% higher in winter than in summer in northern China.[13]Furthermore, volume of emergency attendance was highest in winter in Shandong and Jilin province (northern China), especially for respiratory and circulatory systems.[14]This study observed that emergency attendances peaked during the period at the end of spring and the beginning of summer in both Hong Kong and Shenzhen. The discrepancy may be related to climate differences. Hong Kong and Shenzhen locate in the region with tropical marine climate, so it is warm in winter with relatively stable temperature in the whole year. However, it is extremely hot in summer. Respiratory diseases would be caused by internal and external temperature difference due to internal air conditioner. Trauma would be caused by thin clothes. Food is easily to spoilage, which would increase the risk of digestive system disease.
Previous studies[8,15]have reported sex disparities in disease spectrum of emergency department. It has noted that male patients aged 20–45 years old had higher risk for fracture, craniocerebral trauma, cardiovascular and cerebrovascular diseases than female patients and male patients in other age group. This study also observed similar sex disparities. Several factors may account for this phenomenon. Firstly, male subjects in this age group underwent works related to industrial and agricultural production; secondly, these people had higher risk of exposure to transportation and work-related injuries; in addition, male subjects may had higher mental stress and unhealthy lifestyles, such as smoking and alcohol abuse,which further increase the risk for cardiovascular and cerebrovascular diseases.
Similar disease spectrum was noted in this study,with respiratory, digestive, cardio-cerebral vascular system ranking the top system disease. The geographical location of Hong Kong and Shenzhen is very close,leading to the similar epidemiological characteristics of disease. However, the capacity of emergency medical services varied across regions in mainland of China.[16,17]Health administrative departments should strengthen the training of health emergency knowledge and skills of the primary care medical staffs to enhance their health emergency response capabilities.[18]
This study has limitations. Firstly, data of two typical hospitals were used to analyze. It cannot be assumed that the patients in other hospitals present with similar complaints and diagnosis. Secondly, there were 3-year data. The situation would be changed in the long-term. Thus, the longitudinal patterns of disease spectrum warranted for elucidation in further studies.Thirdly, the use of routine EMR databases had inherent limitations for diagnosis coding and def inition. Fourthly,many risk factors were not analyzed due to the lack of corresponding data, such as air pollution, patient socioeconomic status, private ownership of primary care providers, and healthcare utilization factors.[19,20]Fifthly, many potential confounding factors were not investigated. For examples, a follow-up interview with the ED patients, and ED doctors and other related clinicians. We will analyze the EM data deeply and reported in the future. Finally, the knowledge, attitude and behavior about public health emergencies and the response capacity of primary care varied across regions in mainland of China.[21]Therefore, the generalization of the findings to other regions should be taken a cautious.
CONCLUSION
In summary, this study documented the epidemiological characteristics and disease spectrum in emergency departments in Hong Kong and Shenzhen.Hong Kong had older patients of emergency and longer waiting time than that in Shenzhen. The pattern of visiting time in both hospitals was different. Both cities had highest volume of attendance in summer and lowest in winter. The diseases of respiratory system and digestive system were the most common cause of emergency visiting. These finding will help to resource allocation and development of emergency departments.
Funding:This research received no specific grant from any funding agency in the public, commercial or not-for-prof it sectors.
Ethical approval:Not needed.
Conflicts of interest:None declared.
Contributors:SXC proposed the study and wrote the paper. All authors contributed to the design and interpretation of the study and to further drafts.
REFERENCESS
1 Lee AW, Sze H, Lam KO, Chen X. A tale of two cities in China:Hong Kong and Shenzhen. Int J Radiat Oncol Biol Phys.2014;89:704-8.
2 Young AL, Jhanji V, Liang Y, Congdon N, Chow S, Wang F, et al. A survey of perceived training differences between ophthalmology residents in Hong Kong and mainland China.Bmc Med Educ. 2015;15:158.
3 Sun M, Xu N, Li C, Wu D, Zou J, Wang Y, et al. The public health emergency management system in China: trends from 2002 to 2012. BMC Public Health. 2018;18(1):474.
4 Habib MI, Khan K. Prof ile and outcomes of critically ill children in a lower middle-income country. Emerg Med J. 2018;35(1):52-5.
5 Pope I, Ismail S, Bloom B, Jansen G, Burn H, McCoy D, et al.Short-stay admissions at an inner city hospital: a cross-sectional analysis. Emerg Med J. 2018;35(4):238-46.
6 Chen CY, Lin MJ, Yang WC, Chang YJ, Gao FX, Wu HP.Clinical spectrum of intra-abdominal abscesses in children admitted to the pediatric emergency department. J Microbiol Immunol Infect. 2018 Aug 9. pii: S1684-1182(18)30286-X.
7 Jones A, Donald MJ, Jansen JO. Evaluation of the provision of helicopter emergency medical services in Europe. Emerg Med J.2018;35(12):720-5.
8 Wang W, Wang C, Wang J. Epidemiological analysis and disease spectrum characteristics of emergency patients with critical illness: 3 176 emergency cases in 2017 in a hospital in Beijing were analyzed. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue.2018;30(10):987-90.
9 Rainer TH, Sollich P, Piotrowski T, Coolen AC, Cheng B,Graham CA. Evaluating acute medical admissions through emergency departments in Hong Kong: can one adjust for casemix variation? Emerg Med J. 2012;29(12):978-82.
10 Kang H, Nembhard HB, Rafferty C, DeFlitch CJ. Patient flow in the emergency department: a classification and analysis of admission process policies. Ann Emerg Med. 2014;64(4):335-342.e8.
11 Guo Y, Ma Y, Ji J, Liu N, Zhou G, Fang D, et al. The relationship between extreme temperature and emergency incidences: a time series analysis in Shenzhen, China. Environ Sci Pollut Res Int.2018;25(36):36239-55.
12 Zhao Q, Zhang Y, Zhang W, Li S, Chen G, Wu Y, et al. Ambient temperature and emergency department visits: Time-series analysis in 12 Chinese cities. Environ Pollut. 2017;224:310-6.
13 Pan C, Huang XR, Pang JJ, Cheng K, Xu F, Chen YG. Trends in mortality of emergency departments patients in China. World J Emerg Med. 2019;10(3):152-5.
14 Ou CQ, Song YF, Yang J, Chau PY, Yang L, Chen PY, et al.Excess winter mortality and cold temperatures in a subtropical city, Guangzhou, China. PLoS One. 2013;8(10):e77150.
15 Zhang XF, Hu DY, Ding RJ, Wang HC, Yan LX. Status and trend of cardio-cerebral-vascular diseases mortality in China:data from national disease surveillance system between 2004 and 2008. Zhonghua Xin Xue Guan Bing Za Zhi. 2012;40(3):179-87.
16 Yan K, Jiang Y, Qiu J, Zhong X, Wang Y, Deng J, et al. The equity of China’s emergency medical services from 2010-2014.Int J Equity Health. 2017;16(1):10.
17 Li Y, Li C, Xu J, Zhang H, Zheng L, Yao D, et al. Emergency department enlargement in China: exciting or bothering. J Thorac Dis. 2016;8(5):842-7.
18 Zhiheng Z, Caixia W, Jiaji W, Huajie Y, Chao W, Wannian L. The knowledge, attitude and behavior about public health emergencies and the response capacity of primary care medical staffs of Guangdong Province, China. BMC Health Serv Res.2012;12:338.
19 Ge E, Lai K, Xiao X, Luo M, Fang Z, Zeng Y, et al. Differential effects of size-specific particulate matter on emergency department visits for respiratory and cardiovascular diseases in Guangzhou, China. Environ Pollut. 2018;243(Pt A):336-45.
20 Wei X, Yin J, Wong SY, Griffiths SM, Zou G, Shi L. Private ownership of primary care providers associated with patient perceived quality of care: A comparative cross-sectional survey in three big Chinese cities. Medicine (Baltimore).2017;96(1):e5755.
21 Wei X, Li H, Yang N, Wong SY, Chong MC, Shi L, et al.Changes in the perceived quality of primary care in Shanghai and Shenzhen, China: a difference-in-difference analysis. Bull World Health Organ. 2015;93(6):407-16.
 World journal of emergency medicine2020年1期
World journal of emergency medicine2020年1期
- World journal of emergency medicine的其它文章
- Surgical closure of large splenorenal shunt may accelerate recovery from hepato-pulmonary syndrome in liver transplant patients
- Role of penehyclidine in acute organophosphorus pesticide poisoning
- Mobile technology: Usage and perspective of patients and caregivers presenting to a tertiary care emergency department
- Retrospective analysis of eFAST ultrasounds performed on trauma activations at an academic level-1 trauma center
- A pulmonary source of infection in patients with sepsis-associated acute kidney injury leads to a worse outcome and poor recovery of kidney function
- Admission delay is associated with worse surgical outcomes for elderly hip fracture patients: A retrospective observational study