
Clinicopathological characteristics and surgical outcomes of sarcomatoid hepatocellular carcinoma
2020-11-30 06:53JianPingWangZhiGangYaoYaWenSunXiHanLiuFengKaiSunCunHuLinFuXinRenBeiBeiLvShuaiJunZhangYangWangFanYingMengShunZhenZhengWeiGongJunLiu
World Journal of Gastroenterology 2020年29期
Jian-Ping Wang, Zhi-Gang Yao, Ya-Wen Sun, Xi-Han Liu, Feng-Kai Sun, Cun-Hu Lin, Fu-Xin Ren, Bei-Bei Lv,Shuai-Jun Zhang, Yang Wang, Fan-Ying Meng, Shun-Zhen Zheng, Wei Gong, Jun Liu
Abstract
Key words: Sarcomatoid hepatocellular carcinoma; Histological composition; Liver resection; Overall survival; Recurrence-free survival
INTRODUCTION
Hepatocellular carcinoma (HCC) is the sixth most common type of cancer and the fourth leading cause of cancer-related death worldwide[1]. Sarcomatoid HCC is a histological subtype of HCC that differs from conventional HCC and presents with an unusual characteristic: sarcomatoid HCCs contain variable proportions of sarcomatous and carcinomatous components, wherein the sarcomatous component usually consists of spindle-shaped cells that form interlacing bundles and show a partial storiform pattern, and the carcinomatous component commonly comprises poorly differentiated [Edmondson-Steiner (ES) grade III or IV] conventional HCC cells[2,3]. Previous studies have indicated that certain anticancer therapies, such as transcatheter arterial chemoembolization (TACE), can lead to more frequent sarcomatous changes in HCC[4,5]. However, an increasing number of sarcomatoid HCC cases without previous anticancer therapy have been reported[6-8]. To date, the pathogenesis of the sarcomatous change has not been elucidated.
Sarcomatoid HCC is a rare malignancy, with an incidence of 1.7%-1.9% among surgically resected HCC cases and 3.9%-9.4% among autopsied HCC patients[3,4,8-11]. A few studies have reported that sarcomatoid HCC is associated with a higher recurrence rate, more frequent metastasis and poorer survival than conventional HCC[2,3,8,12]. However, these studies did not further stratify conventional HCC into low- (ES grade I and II) and high-grade (ES grade III and IV) HCC; in particular, high-grade HCC is considered similar to sarcomatoid HCC in terms of histological differentiation, more aggressive nature and poor prognosis[2,3,13,14]. In addition, although sarcomatoid HCC has a high incidence of adjacent organ invasion and metastasis[8], the underlying mechanisms remain unknown. One previous study reported that most portal venous invasions and metastases had sarcomatous components, indicating that the sarcomatous component is responsible for metastasis[3].
In this study, we comprehensively compared the clinicopathological characteristics and surgical outcomes of sarcomatoid HCC and high-grade HCC patients. We also analyzed the histological composition of metastatic and invasive sarcomatoid HCCs to study the relative importance of sarcomatous and carcinomatous components in highly aggressive behavior.
MATERIALS AND METHODS
Patient selection
From January 2007 to December 2017, a total of 2287 patients underwent surgical resection for HCC at Shandong Provincial Hospital. We retrospectively reviewed the pathological records of these patients, of which 186 were diagnosed with high-grade HCC defined as grade III or IV differentiated HCC according to the ES classification[15]. In addition, 45 patients who underwent surgical resection for sarcomatoid HCC were identified from the pathology database of Shandong Provincial Hospital. We excluded patients who had previous interventions (including TACE, radiofrequency ablation and previous surgical resection) or missing data. A total of 41 sarcomatoid HCC and 155 high-grade HCC patients were included in the final analysis. The flowchart of patient selection is shown in Figure 1.
Data collection
The medical records of the included patients were retrospectively reviewed. A standardized record form was used to collect clinical information, including age, sex, symptoms, alcoholism, hepatitis virus B or C infection, liver cirrhosis, laboratory test results, Child-Pugh classification and tumor-specific characteristics, such as tumor size, tumor number and macrovascular invasion. Tumor staging was classified according to the Barcelona Clinic Liver Cancer staging system and the American Joint Committee on Cancer (AJCC) staging system (8thedition, 2017). Computed tomography (CT) and magnetic resonance imaging (MRI) images were also reviewed.
Postoperative follow-up
Routine follow-ups were conducted during the 1stand 3rdmo after resection and subsequently every 2 to 3 mo during the first postoperative year and every 3 to 6 mo thereafter. At each follow-up, serum alpha-fetoprotein (AFP) levels and liver function were assessed, and abdominal ultrasonography was completed. An abdominal CT or MRI was performed at an interval of 6 to 12 mo depending on the postoperative time. If recurrence was suspected, an additional CT or MRI scan was performed immediately. Overall survival (OS) was defined as the time from the date of surgery to the date of death or last follow-up. Recurrence was defined as the appearance of a new lesion as confirmed by CT or MRI during follow-up. Recurrence-free survival (RFS) was calculated from the date of surgery to the date of the first documented recurrence, death or last follow-up.
Statistical analysis
Numerical data are presented as the median (range) or mean ± standard deviation. Differences between groups were compared using Pearson’sχ2test or the two-tailed Fisher’s exact test for categorical data and the Mann-WhitneyUtest for numerical data. OS and RFS were determined using the Kaplan-Meier method, and differences between groups were assessed by the log-rank test. To evaluate further the impact of histological subtype on prognosis, univariate analyses of prognostic factors were performed using univariate Cox regression analysis. Among the parameters withP< 0.1 in the univariate analyses, age, serum AFP level, AJCC stage, differentiation grade of the carcinomatous component and histological subtype were used to build a basic multivariate Cox proportional hazard model since they reflect multiple aspects of a patient’s condition. We also adjusted for variables that changed the matched hazard ratio of the histological subtype by at least 5% upon addition into the model[16]. APvalue < 0.05 was considered to indicate statistical significance. Kaplan-Meier curves were generated and analyzed using GraphPad Prism 7 (GraphPad Software Inc., San Diego, CA, United States). All other statistical analyses were performed using IBM SPSS 23.0 software (SPSS Inc., Armonk, NY, United States).
RESULTS
Clinical and laboratory characteristics of the studied patients
A total of 196 patients, including 41 sarcomatoid and 155 high-grade HCC patients, were included in this study, and the clinical and laboratory characteristics are shown in Table 1. In both the sarcomatoid and high-grade HCC groups, the majority of the patients were men (80.5% and 86.5%,P= 0.339), with a median age of 54 years and 55 years (P= 0.942), respectively. During the first hospital visit, sarcomatoid HCC patients had a higher incidence of concomitant symptoms than high-grade HCC patients (78.0%vs55.5%,P= 0.009), including symptoms of epigastric discomfort (63.4%vs43.2%), weight loss (34.1%vs18.1%) and fever (22%vs2.6%). The etiology of hepatopathy, presence of cirrhosis, Child-Pugh classification and laboratory test results were comparable between the two groups (allP> 0.05). However, serum AFP levels were significantly lower in the sarcomatoid group than in the high-grade group (5.8 ng/mLvs348.0 ng/mL,P< 0.001).
Tumor-specific characteristics of the studied patients
The tumor-specific characteristics are shown in Table 2. At the time of diagnosis, the frequency of sarcomatoid HCC patients presenting with typical dynamic image patterns (arterial phase enhancement and portal and delayed phase washout) was significantly lower than that of patients with high-grade HCC (44.4%vs72.7%,P= 0.001). Some sarcomatoid HCCs might be misdiagnosed as intrahepatic cholangiocarcinoma (iCCA) or a hepatic abscess (Figure 2). Compared to high-grade HCC patients, sarcomatoid HCC patients had larger tumors, a lower incidence of tumor encapsulation and higher frequencies of tumor necrosis, adjacent organ invasion, lymph node metastasis and advanced AJCC stage (allP< 0.05). In addition, the two groups showed significant differences in the differentiation grades of carcinomatous components (P< 0.05). Patients in the sarcomatoid HCC group showed a trend towards a higher postoperative recurrence rate than those in the high-grade HCC group, but the difference was not significant (P= 0.091).
Sarcomatoid HCC patients have a worse prognosis than high-grade HCC patients
The sarcomatoid HCC patients had a shorter median OS than high-grade HCC patients (10.5 movs48.1 mo,P< 0.0001, Figure 3A). The 1-, 3- and 5-year OS rates were 48.8%, 17.3% and 11.5% for the sarcomatoid group and 85.2%, 53.4% and 41.1% for the high-grade group, respectively. Moreover, the sarcomatoid HCC group had a shorter median RFS than the high-grade HCC group (5.6 movs16.4 mo,P< 0.0001, Figure 3B). The RFS rates post resection were 49.7% and 83.1% at 6 mo, 20.9% and 60.2% at 1 year and 6.3% and 31.8% at 3 years for the sarcomatoid and high-grade groups, respectively. Even after stratification by AJCC stage (Figure 4) or differentiation grade of the carcinomatous component (Figure 5), the sarcomatoid HCC patients still had worse OS and shorter RFS than the high-grade HCC patients in each subgroup (allP< 0.05).
Sarcomatoid subtype is an independent predictor of poor prognosis
Cox regression analysis was used to verify whether the sarcomatoid type is an independent prognostic factor for HCC patients. Our univariate analysis showed that larger tumors, multiple tumors, a lack of tumor encapsulation, tumor necrosis, macro- and microvascular invasion, adjacent organ invasion, lymph node metastasis, advanced AJCC stage, poorer differentiation of the carcinomatous component and sarcomatoid subtype were significantly associated with increased mortality (Table 3) and recurrence (Table 4) in the total population (allP< 0.05). In addition, age < 55 years, Child-Pugh B and lower serum AFP levels were significantly related to increased mortality (allP< 0.05, Table 3). After controlling for confounding factors, sarcomatoid subtype was identified as an independent predictor of poorer OS and RFSin the multivariable analysis (allP< 0.05, Table 3 and Table 4).

Table 1 Clinical and laboratory characteristics of the studied patients, n (%)
Invasive and metastatic sarcomatoid HCCs mainly comprise carcinomatous components
Sarcomatoid HCC is composed of both sarcomatous and carcinomatous components (Figure 6); however, it remains unknown which component is the primary contributor to the highly aggressive nature of sarcomatoid HCC. To explore further this, the histological composition of lymph node metastases, macrovascular invasions, bile duct invasions and multiple liver tumor lesions of sarcomatoid HCCs were analyzed. Nine patients showed a total of 33 lymph node metastases. Of these, 26 (78.8%) metastases contained purely carcinomatous components, two (6.1%) were purely sarcomatous and five (15.1%) had mixed carcinomatous and sarcomatous components. Seven macrovascular invasions and two bile duct invasions were observed in eight patients (one patient had both macrovascular and bile duct invasion). Six of these invasions were evaluated by pathological examination, and only two (33.3%) had sarcomatous components. A total of 16 patients were confirmed to have multiple liver tumors (10 patients with multinodular HCC and six with satellite nodules). Of the 10 patients with multinodular HCC, only two (20.0%) had concurrent sarcomatoid HCC, whereas the others had simultaneous sarcomatoid and conventional HCC. In addition, of the six patients with satellite nodules, sarcomatous changes were found in only two patients (33.3%).
Proportion of sarcomatous components in sarcomatoid HCC does not predict survival
Next, we divided the sarcomatoid HCC patients into three subgroups according to the proportion of sarcomatous components in the tumor: (1) Mixed subgroup ≤ 50% (n= 14 patients); (2) Mixed subgroup > 50% (n= 16); and (3) Pure subgroup (n= 11). The OS and RFS were similar among these subgroups (Figure 7).

Table 2 Tumor-specific characteristics of the studied patients, n (%)

Table 3 Univariable and multivariable analyses of overall survival of the studied patients
DISCUSSION
Sarcomatoid HCC is a rare histological subtype of HCC, with an incidence of approximately 2% of surgically resected cases[3,8]. A few studies have reported that sarcomatoid HCC is more aggressive than conventional HCC and associated with a worse prognosis[2,3,8,12]. However, sarcomatoid HCC usually has a worse differentiation grade[12], which is regarded as a prognostic factor for HCC, and this fact can lead to inaccurate comparisons between sarcomatoid HCC and conventional HCC. In this study, high-grade HCC, which is thought to be similar to sarcomatoid HCC in terms of histological differentiation, was used as the control in a detailed examination of the clinicopathological characteristics and surgical outcomes of sarcomatoid HCC. Moreover, this study analyzed the histological composition of metastatic and invasive sarcomatoid HCCs.
Our results demonstrate that sarcomatoid HCC is more frequently diagnosed at an advanced AJCC stage with relatively larger tumors and higher rates of adjacent organ invasion and lymph node metastasis. During the first visit to the hospital, sarcomatoid HCC patients have a higher incidence of epigastric discomfort, weight loss and fever than high-grade HCC patients. In particular, the incidence of fever was nearly 10 times higher in the sarcomatoid HCC group than in the high-grade HCC group, perhaps due to the higher frequency of tumor necrosis caused by the relatively larger size and faster progression of sarcomatoid HCC tumors. Imaging plays a critical role in HCC diagnosis. There are typical dynamic image patterns considered specific for HCC[17]. However, more than 60% of sarcomatoid HCCs show MRI features more similar toiCCA than to HCC[18]. In our study, only 44.4% of sarcomatoid HCC patients presented with typical dynamic image patterns of HCC, and some patients with sarcomatoid HCC may be misdiagnosed with iCCA or a hepatic abscess. Consistent with the results of previous studies[8,12], our findings show that the majority of patients with sarcomatoid HCC had a history of chronic viral hepatitis and liver cirrhosis, which are key risk factors for the development of HCC[19]. Regular ultrasound screening of these high-risk patients could help detect tumors at an early stage and reduce the risk of death[19,20]. Of note, only 36.6% of sarcomatoid HCC patients had serum AFP levels > 20 ng/mL in the current study. Therefore, serum AFP tests may have no use for the early detection of sarcomatoid HCC. Moreover, both serologic and radiologic examinations could not help in distinguishing the sarcomatoid subtype from conventional HCC or other intrahepatic masses, and this might be problematic when selecting a potential recipient of liver transplantation because the sarcomatoid subtype usually predicts a poor prognosis[2].

Table 4 Univariable and multivariable analyses of recurrence-free survival of the studied patients
Previous studies have demonstrated that patients with resected sarcomatoid HCC have a worse RFS than those with resected conventional HCC[2,8]. Similar to the findings of previous studies, we found that the median RFS of sarcomatoid HCC patients was significantly shorter than that of high-grade HCC patients (5.6 movs16.4 mo,P< 0.0001). A previous study from Taiwan indicated that sarcomatoid HCC is more prone to extrahepatic metastasis than conventional HCC after curative therapy[12]. Nevertheless, in our study, there was no difference in the recurrence pattern between the sarcomatoid and high-grade HCC groups, perhaps due to their similar histological differentiation. Several previous studies have also indicated that the OS of sarcomatoid HCC patients is significantly worse than that of conventional HCC patients, with a 3-year OS rate ranging from 8.0% to 17.5%[2,8,12,21]. Consistent with previous studies, the current study showed that patients with resected sarcomatoid HCC had an elevated risk of death, with an abysmal 3-year OS compared with the prognosis of resected high-grade HCC patients (17.3%vs53.4%,P< 0.0001). Even after controlling for confounding factors, the association between sarcomatoid HCC and worse RFS and OS persisted. These results strongly suggest that sarcomatoid HCC is more aggressive than high-grade HCC, although they are similar in terms of histological differentiation.

Figure 2 Imaging findings of sarcomatoid hepatocellular carcinoma in patients with various initial diagnoses based on radiologic findings. A: Hepatocellular carcinoma; B: Intrahepatic cholangiocarcinoma; C: Hepatic abscess.

Figure 3 Kaplan-Meier estimated overall and recurrence-free survival curves. A: Sarcomatoid hepatocellular carcinoma (HCC) is associated with worse overall survival (log-rank P < 0.0001); B: Sarcomatoid HCC is associated with worse recurrence-free survival (log-rank P < 0.0001).

Figure 4 Kaplan-Meier curves of the estimated overall survival and recurrence-free survival of patients with sarcomatoid or high-grade hepatocellular carcinoma stratified by American Joint Committee on Cancer stage. A: Sarcomatoid hepatocellular carcinoma (HCC) is associated with worse overall survival (OS) in patients with American Joint Committee on Cancer (AJCC) stage I-II disease (log-rank P < 0.0001); B: Sarcomatoid HCC is associated with worse recurrence-free survival (RFS) in patients with AJCC stage I-II disease (log-rank P = 0.0004); C: Sarcomatoid HCC is associated with worse OS in patients with AJCC stage III-IV disease (log-rank P = 0.0004); D: Sarcomatoid HCC is associated with worse RFS in patients with AJCC stage III-IV disease (log-rank P = 0.0004).
The histogenesis of sarcomatous tissue in cancers, including HCC, has not yet been elucidated. The most widely accepted theory is the conversion theory, which postulates that the sarcomatous element derives from the carcinoma during tumor evolution[3,9,22-25]. Several recent studies indicate that epithelial-mesenchymal transition is an important mechanism underlying the sarcomatous change, which further confirms the conversion theory[26-28]. Sarcomatoid HCCs comprise variable proportions of sarcomatous and carcinomatous components. A previous study reported no survival difference between mixed and pure sarcomatoid HCC patients[12]. However, the proportion of sarcomatous tissue in some patients could not be precisely evaluated because of pathological diagnosis by biopsy[12]. In our study, all patients with sarcomatoid HCC underwent surgical resection and were divided into three subgroups according to the proportion of the sarcomatous component. Our results indicated that the OS and RFS were similar among the three subgroups, suggesting that the proportion of the sarcomatoid component is not associated with prognosis.
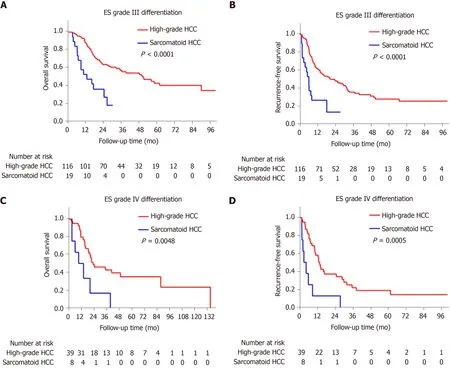
Figure 5 Kaplan-Meier curves of the estimated overall survival and recurrence-free survival of patients with sarcomatoid or high-grade hepatocellular carcinoma stratified by differentiation grade of the carcinomatous component. A: Sarcomatoid hepatocellular carcinoma (HCC) is associated with worse overall survival (OS) in patients with Edmondson-Steiner (ES) grade III differentiation (log-rank P < 0.0001); B: Sarcomatoid HCC is associated with worse recurrence-free survival (RFS) in patients with ES grade III differentiation (log-rank P < 0.0001); C: Sarcomatoid HCC is associated with worse OS in patients with ES grade IV differentiation (log-rank P = 0.0048); D: Sarcomatoid HCC is associated with worse RFS in patients with ES grade IV differentiation (logrank P = 0.0005).
Several previous studies demonstrated that sarcomatoid HCC is associated with a high frequency of portal venous invasion and metastasis[3,11,29,30]; our study showed a higher rate of lymph node metastasis but not of venous invasion. However, few studies have explored the related mechanisms, and only Maedaet al[3]have reported the composition of portal venous invasions and metastases. They studied 13 cases of sarcomatoid HCC treated by surgical resection and found that most portal venous invasions and metastases had sarcomatous components, which were postulated to be responsible for metastasis. Contrary to their results, our study demonstrated that the majority of lymph node metastases, macrovascular/bile duct invasions and satellite nodules were composed of carcinomatous components. This apparent inconsistency may be because in Maeda’s study, five (38%) patients underwent preoperative treatment, such as TACE, and their analysis included an autopsied case with extensive postoperative metastases comprising sarcomatoid components[3]. In line with our findings, however, they showed that the metastatic lymph nodes in two patients comprised carcinomatous components. In addition, some invasions and metastases had mixed carcinomatous and sarcomatous components. Based on these findings, we speculate that the carcinomatous component might be the dominant factor mediating the highly aggressive nature of sarcomatoid HCC. Furthermore, the carcinomatous components might exist in a “presarcomatoid” state[31], in which the tumor cells have cellular morphology typical of conventional HCC but greatly enhanced invasive ability. As a result, sarcomatous changes might occur after invasion or metastasis in some cases (Figure 8). This could also explain the phenomenon of sarcomatoid HCC being associated with more frequent lymph node metastasis and poorer prognosis than high-grade HCC even when they are similar in terms of histological differentiation. Further studies focusing on the underlying molecular pathogenesis of sarcomatoid HCC are urgently needed to understand better its highly aggressive biological features.

Figure 6 Pathological findings of sarcomatoid hepatocellular carcinoma. A: The lower left area of the image shows the sarcomatous change, with spindle-shaped cells forming interlacing bundles. The upper right region represents conventional hepatocellular carcinoma, with tumor cells at Edmondson-Steiner (ES) grade II differentiation (hematoxylin & eosin staining, × 200 magnification). (B) Scattered patchy carcinomatous components with ES grade III differentiation in sarcomatous regions (Hematoxylin and eosin staining, × 100 magnification). Star: Carcinomatous components, Triangle: Tumor necrosis.

Figure 7 Kaplan-Meier curves of the estimated overall survival and recurrence-free survival of patients with sarcomatoid hepatocellular carcinoma stratified by the proportion of the sarcomatous component in the tumor. Sarcomatoid hepatocellular carcinoma patients were divided into three subgroups based on the proportion of the sarcomatous component in the tumor: (1) mixed subgroup ≤ 50% (n = 14); (2) mixed subgroup > 50% (n = 16); and (3) pure subgroup (n = 11). Kaplan-Meier analyses of (A) overall survival and (B) recurrence-free survival showed no differences among the three subgroups.
There are limitations of our study. First, this was a retrospective study conducted in a single center, and randomized studies should be performed in multiple centers. Second, although this study presented an analysis of one of the largest series of sarcomatoid HCC cases, the relatively small number of patients may have influenced the accuracy of the results, and additional studies with more cases should be performed. Third, in this study, we discovered that carcinomatous components occupied the predominant proportion of invasions and metastases and developed a hypothesis regarding the occurrence of sarcomatoid HCC. The related mechanisms were not further explored, and future studies should address these issues.
In conclusion, compared with high-grade HCC, sarcomatoid HCC is associated with more advanced AJCC stage, an atypical dynamic image pattern and lower serum AFP levels. Patients with sarcomatoid HCC have significantly worse RFS and OS than those with high-grade HCC. Furthermore, the highly aggressive nature of sarcomatoid HCC seems to be mediated by its carcinomatous components.

Figure 8 Schematic of the hypothesis. HCC: Hepatocellular carcinoma.
ARTICLE HIGHLIGHTS

Research results
Sarcomatoid HCC was more frequently diagnosed at an advanced stage with a larger tumor and higher rates of nonspecific symptom, adjacent organ invasion and lymph node metastasis than high-grade HCC (allP< 0.05). Compared with high-grade HCC patients, sarcomatoid HCC patients are less likely to have typical dynamic imaging features of HCC (44.4%vs72.7%,P= 0.001) and elevated serum alpha-fetoprotein levels (> 20 ng/mL; 36.6%vs78.7%,P< 0.001). The sarcomatoid group had a significantly shorter median recurrence-free survival (5.6 movs16.4 mo, log-rankP< 0.0001) and overall survival (10.5 movs48.1 mo, log-rankP< 0.0001) than the highgrade group. After controlling for confounding factors, the sarcomatoid subtype was identified as an independent predictor of poor prognosis. Pathological analyses indicated that invasive and metastatic lesions were mainly composed of carcinomatous components.
Research conclusions
Sarcomatoid HCC was associated with a more advanced stage, atypical dynamic imaging, lower serum alpha-fetoprotein levels and a worse prognosis. The highly aggressive nature of sarcomatoid HCC is perhaps mediated by carcinomatous components.
Research perspectives
Studies focusing on the underlying molecular pathogenesis of sarcomatoid HCC are urgently needed to understand better its highly aggressive biological features.
 World Journal of Gastroenterology2020年29期
World Journal of Gastroenterology2020年29期
- World Journal of Gastroenterology的其它文章
- Endoscopic management of gastrointestinal leaks and fistulae: What option do we have?
- Watch and wait approach in rectal cancer: Current controversies and future directions
- Evaluation of intrahepatic manifestation and distant extrahepatic disease in alveolar echinococcosis
- Multivariate predictive model for asymptomatic spontaneous bacterial peritonitis in patients with liver cirrhosis
- Patients' perspectives on smoking and inflammatory bowel disease: An online survey in collaboration with European Federation of Crohn's and Ulcerative Colitis Associations
- Dysregulation of microRNA in cholangiocarcinoma identified through a meta-analysis of microRNA profiling