
Impact of mobile health and medical applications on clinical practice in gastroenterology
2020-11-30 06:59SvenKernebeckTheresaBusseMaximilianBottcherJuirgenWeitzJanEhlersUlrichBork
World Journal of Gastroenterology 2020年29期
Sven Kernebeck, Theresa S Busse, Maximilian D Bottcher, Juirgen Weitz, Jan Ehlers, Ulrich Bork
Abstract Mobile health apps (MHAs) and medical apps (MAs) are becoming increasingly popular as digital interventions in a wide range of health-related applications in almost all sectors of healthcare. The surge in demand for digital medical solutions has been accelerated by the need for new diagnostic and therapeutic methods in the current coronavirus disease 2019 pandemic. This also applies to clinical practice in gastroenterology, which has, in many respects, undergone a recent digital transformation with numerous consequences that will impact patients and health care professionals in the near future. MHAs and MAs are considered to have great potential, especially for chronic diseases, as they can support the selfmanagement of patients in many ways. Despite the great potential associated with the application of MHAs and MAs in gastroenterology and health care in general, there are numerous challenges to be met in the future, including both the ethical and legal aspects of applying this technology. The aim of this article is to provide an overview of the current status of MHA and MA use in the field of gastroenterology, describe the future perspectives in this field and point out some of the challenges that need to be addressed.
Key words: Mobile health; Health applications; Medical applications; Technology; Telemedicine; Mobile applications; Smartphone; eHealth; mHealth; Digital biomarker; Electronic health records
INTRODUCTION
The first smartphone, Apple’s iPhone, was introduced in 2007, only 13 years ago. Since then, the widespread adoption of smartphones and digital innovations, such as tablets, wearables, smartwatches and other devices, has tremendously changed everyday life and consumer behavior in many ways. The introduction of modern information and communication technologies (ICT) has been one of the most disruptive technological innovations in recent decades. The ubiquitous availability of smartphones, wearables and tablet computers and the widespread internet connectivity have led to a significant change in human-technology interaction[1]. At the same time, the exponential development of computer performance and storage capacities, cloud computing and the application and improvement of artificial intelligence (AI) methods have opened new possibilities for the design of ICT[2]. Mobile health apps (MHAs) and medical apps (MAs) are becoming increasingly popular as digital interventions in a wide range of health-related applications in almost all sectors of healthcare[3]. This also applies to clinical practice in gastroenterology, which has, in many respects, recently undergone a digital transformation that will have numerous consequences for patients and health care professionals in the near future[4-8]. The functionalities and intentions of MHAs and MAs use in gastroenterology are extremely diverse. They range from electronic health record (EHR)[9-11]and workflow management systems to specific mobile apps for the management of chronic or acute pain or the management[12-13]of specific diseases in specific settings[14-16]. MHAs and MAs are considered to have great potential, especially for chronic diseases, as they can support the self-management of patients in many ways[17,18].
During the current pandemic outbreak of the novel coronavirus caused respiratory disease (coronavirus disease 2019) the use of MHAs and MAs and telemedical solutions has tremendously increased[19]. The use of these digital technologies to set up virtual clinics, telemedical consultations, remote interpreting of data and virtual education platforms is ideal for continuing medical care during situations of local government issued curfews and shortage of specialized workforces[19]. Therefore, during the current pandemic situation in the field of gastroenterology the use of ICT has been already used for managing patients with chronic liver disease (CLD)[20]or new-onset type 1 diabetes[21]– to name just a few. Guidelines have already been published by the European Association for the Study of the Liver for telemedical management of patients with CLD[22].
Despite the great potential associated with the application of MHAs and MAs in gastroenterology and health care in general, there are numerous challenges to be met in the future, including both the ethical and legal aspects of applying this technology[23]as well as the proof of benefit in terms of evidence-based medical care[24]. The aim of this article is to provide an overview of the status quo of MHA and MA use in the field of gastroenterology, describe the future perspectives in this field and point out some of the challenges that need to be addressed.
TECHNOLOGICAL BACKGROUND
In the context of the application of digital ICT in general and MHAs and MAs in particular, there are numerous terms used to define this field more specifically (see Table 1 for a glossary). The term eHealth is probably one of the best known terms inthis context. One of the most popular definitions was made by Eysenbach in 2001, who defined eHealth as “an emerging field in the intersection of medical informatics, public health and business, referring to health services and information delivered or enhanced through the internet and related technologies. In a broader sense, the term characterizes not only a technical development but also a state-of-mind, a way of thinking, an attitude, and a commitment for networked, global thinking, to improve health care locally, regionally, and worldwide, by using information and communication technology”[25]. For a more pragmatic perspective, the World Health Organization (WHO) postulated that “eHealth (electronic health) is the cost-effective and secure use of ICT for health and health-related fields”. Due to the great relevance of smartphone apps in healthcare, the term mHealth has been added to the term eHealth in recent years. The term mHealth or mobile health is a component of eHealth and is defined by the WHO as “medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants, and other wireless devices”[26]. However, general definitions of these terms have not yet been established. With regard to the properties of smartphone applications, it is important to make a distinction between the terms MHAs and MAs. MHAs, often referred to as health apps, are smartphone apps that are dedicated to consumers and are supposed to support a health-promoting lifestyle as a preventive measure. In contrast, MAs, also called smartphone apps, are subject to a medical purpose limitation and therefore have to be classified under the legal regulations for medical devices[27]. According to recent estimates, there are currently approximately 325000 smartphone apps available on health-related topics[28]. In addition, there are certainly smartphone apps that are not specifically availableviaan online platform and are not available for public download. The areas of application and functionalization of MHAs and MAs are extremely diverse and range from the management of chronic diseases, the support of health behaviors and even self-diagnostics[29]. MHAs and MAs can also provide infrastructure or support clinicians with clinical decision-making[29].
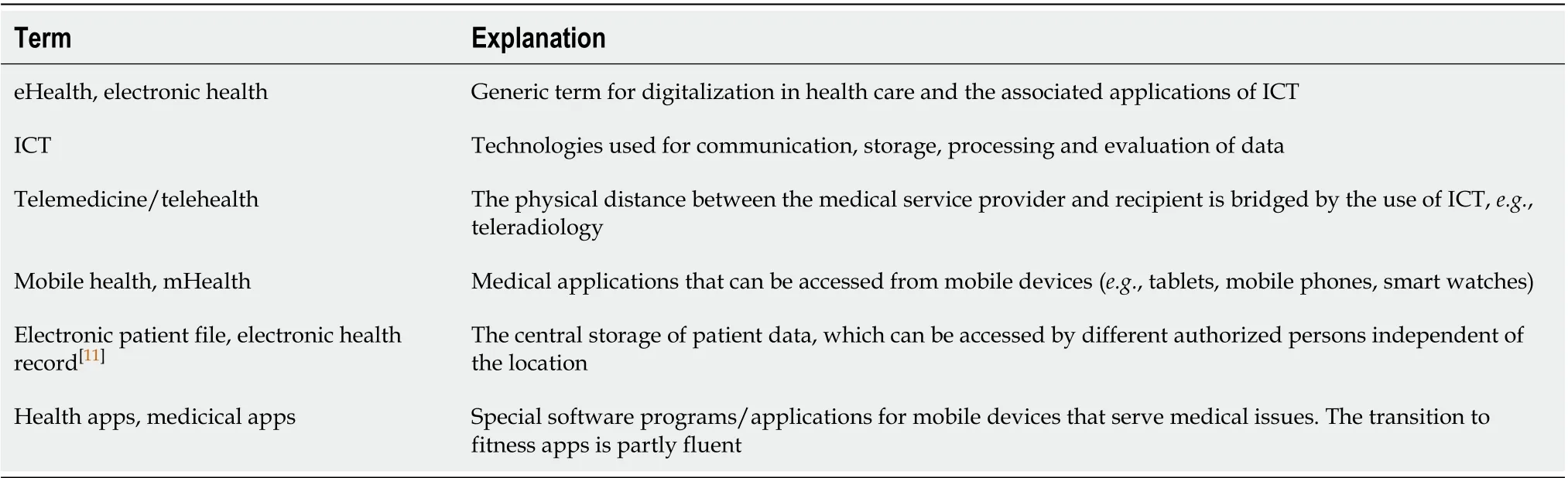
Table 1 Glossary and explanation of digital health terms
OPPORTUNITIES
Digital therapeutics and diagnostics
Clinical care integration: The integration of MHAs and MAs in clinical care is changing practice in gastroenterological care and other fields of healthcare (see Table 2 for examples)[30]. One example is MHAs and MAs used as a digital intervention to improve patient education in the area of preparation for a colonoscopy[31]. The usefulness of patient education before colonoscopy is well established, and optimizing preparation results improves clinical care[32]. There are many different tools and methods to provide educational material to increase adequate bowel preparation ahead of a colonoscopy. These can be booklets, cartoon-based visual aids, educational videos, short message services or social media-based interventions[33]. A major goal of digital interventions is to provide patients with essential knowledge regarding good health information about the aim of the preparation procedure to improve adherence and the overall quality of the colonoscopy[34,35]. In particular, this kind of digital intervention aims to increase the adequate cleaning of the colon before the actualprocedure. The reason for such an intervention is that, in up to 25% of the patients who undergo colonoscopy, inadequate bowel cleansing is present[36]. Adequate bowel cleansing can increase the detection rate of polyps and reduce complications[37]. In a recently published meta-analysis[36], the authors included 6 studies out of 520 records identified in a major database. In the included studies, smartphone apps interventions were compared with standard education. The outcome was reported as adequate bowel preparationvsinadequate bowel preparation, measuredviaa bowel preparation scale (e.g., Boston Bowel Preparation Scale)[36]. The authors pooled data from 1665 patients and concluded that – despite some limitations of the meta-analysis – appbased interventions were an effective tool for an increased improvement of bowel cleansing[36]. In addition to MHAs and MAs, which focus on improving patient education, digital interventions are often specifically designed to improve and support chronic disease management[17]. A recent trial, which included 716 patients with nonalcoholic fatty liver disease found that an internet based program with a web-based intervention was not inferior to common lifestyle programs in terms for improving clinical outcomes. At the same time participation in the web-based intervention was more suitable for people with time and job constraints[38]. In the field of gastroenterology, MHAs can also improve the support of patients with inflammatory bowel disease (IBD). Potential use cases are patient education, the management of disease monitoring, tracking of symptoms, support of medication adherence, the tracking of dietary logs and the support of patient empowerment through access to social media channels[39]. There is a large number of literature reviews that have summarized the potential of using MHAs to support patients with IBD[15,39-41]. In a recently published review from Yinet al[15], apps available in the official Google and Apple digital stores were investigated. Eleven MHAs and 4 MAs were identified in this review. These MHAs focused on patient education, self-monitoring of symptoms, treatment support, follow-up support after diagnosis and patient satisfaction. In a study conducted with gastroenterologic patients’ willingness to use different types of health-related smartphone apps, the investigators found that most of the participants were willing to use apps up to 5 min a day. Trial participants raised concerns that location or social networking activity should not be tracked during their use of the technology[42]. Overall, patients are willing to use health-related apps to manage health problems, but they have high concerns about privacy as well as out-of-pocked payment[42].

Table 2 Examples for use of mobile health applications and medical apps
Telemedicine and telehealth interventions
Telemedicine is a digital health intervention, used in many fields of health care, that provides medical services at a distance. Telemedicine services are provided for varying conditions, such as hypertension[43], chronic heart disease[44], diabetes management[45]and mental illnesses[46]. Telemedicine and telehealth are defined by the WHO, in the global observatory for eHealth, as “The delivery of health care services, where distance is a critical factor, by all health care professionals using ICT for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interest of advancing the health of individuals and their communities”[47]. The potential for telemedicine and telehealth for the field of gastroenterology is high because of the chronic nature of many digestive diseases[48]; liver cirrhosis is an example[49]. Telemedicine is provided using different technologies, such as smartphones, tablet computers, wearables or other medical devices. Traditional components such as monitoring of disease activities, monitoring of symptoms or teleconsultation with medical professionals are also used[50]. There are various advantages associated with telemedicine and telehealth. These are increased access to general or specialized services in healthcare and the offer of greater flexibility in scheduling appointments for health care providers and patients, saving time and money in seeking care[51]. Patients are increasingly using smartphones and the internet for more effective and efficient modalities to receive medical information and treatment descriptions[6]. Traditionally, highly specialized medical care is condensed in urban areas rather than in rural areas. Telemedicine can provide people living in rural areas with specialized care services, thus ensuring ubiquitous access to specialized treatments[52]. In the field of gastroenterology, there are numerous application scenarios for telemedical care concepts, such as general digestive disease management programs[53]. Other telemedical tools are offered for IBD[54,55], CLDs[6], liver transplant patients[56]or diabetes patients[57]. In a literature review from Serperet al[6], the authors illustrated different uses for telemedicine in CLDs. They included 20 published articles about telemedicine in patients with CLD. Nine of the included studies were prospective trials, three were retrospective studies, two were case reports, and six were case series. Only one of the included studies was randomized prospectively, and 10 were uncontrolled studies[6]. The authors categorized the studies into four main fields based on the aspect of CLD management in which telemedicine was used: Hepatitis C treatment, procedural or surgical management, evaluation and management of hepatocellular carcinoma and remote monitoring interventions[6]. In treatment for hepatitis C virus (HCV), many studies have investigated the use of teleconferencing for the management of HCV and reported a sustained virologic response rate in the intervention groups with telemedicine. There were low discontinuation rates and promising results for the management of side effects[6]. Generally, the satisfaction of patients who received in-person visits was high in the intervention groups with telemedicine. The authors stated that telemedicine can improve access to specialty care and can improve care of patients with liver diseases between in-person visits[6]. In addition, they emphasized that the main barriers to the widespread use of telemedicine are regulatory issues and unclear reimbursement for the provided services. Another systematic review on the use of telemedicine and mobile health technology for the management of digestive diseases included seven studies with a focus on inflammatory bowel disease, four studies with a focus on ulcerative colitis, one with a focus on Crohn’s disease, six with a focus on irritable bowel syndrome, and two studies with a focus on colorectal cancer[53]. The outcomes were patient compliance, patient satisfaction, disease activity and quality of life[53]. The studies that were included were mainly pilot trials and feasibility studies, which leads to only limited generalization of the overall results[53]. In addition, only a small number of studies addressed telemedicine for gastroenterological diseases[53]. To support patients with cirrhosis, there are three main types of telemedicine: Teleconsultation, televisits and telemonitoring[49].
eHealth records
Different kinds of digitally stored health information exist. The following are the most common and important: EHR[11]are managed by health care providers. These systematic, longitudinal collections of health information can refer to one person or a whole population. EHR can facilitate the sharing of stored patient data across hospitals, doctors and other health care providers and institutions. The EHR collects medical histories, laboratory test results, medications, allergy information, vital signs, age, weight, height and insurance and billing information. Primary stakeholders of EHRs are physicians, caregivers and nurses, therapists, patients, pharmacists, clinics and hospitals, laboratories, care services and nursing homes. Secondary stakeholders are insurance companies, family and the relatives of patients and employers. The tertiary stakeholders are society, research institutes, public authorities and the health care industry[58].
Electronic medical records (EMR) are created by health care practitioners for specific treatments and can be integrated into EHR[59]. Personal health records are patient managed and can contain additional information, such as data from wearables or health apps. The patient can decide who is able to see which information[11]. The exact shape of the eHealth records differs depending on the country and provider. The primary aim of electronically stored health data is to establish a record of present and future care received from the same or different practitioners. Additionally, EHR can be used to create evidence of the provided care or to improve quality of care by performance monitoring and benchmarking[60]. Other benefits are administrative uses (e.g., billing and scheduling), decision support and care management, patient support and public health research[61].
In the field of gastroenterology, various advantages result from the use of eHealth records: Elective procedures and interventions can be scheduled on the admission day as a part of just-in-time medicine. The use of eHealth records can ensure the completeness of information for pre-existing conditions[60]. Treatment of the acute abdomen is another scope for EHR; being able to have access to an entire patient’s history can prevent medical malpractice in this case and others[62]. Patients are often not able to provide detailed information about prior treatments. In the case of complex diseases, multidisciplinary treatment[63]. Or if patients demand a second opinion, decisions were made based on the provided information[60]. If more extensive information is available in the EHR, decisions can be made better and faster. This is especially important for people undergoing palliative treatment and cancer care and/or patients under multidisciplinary treatment. In these cases, EHR can provide access to relevant information for all stakeholders and ensure efficient and individualized treatment[64]. In 2015, the WHO[65]conducted the third global survey on eHealth to describe the use of eHealth. Only 58% of the countries had an existing national eHealth policy or strategy at that point. A total of 66% of the countries had a national health information system policy or strategy. The study asked for the use of EHR in different health care provider/institutional groups. Primary care facilities compromised clinics and health care centers. Secondary care facilities encompassed hospitals and emergency care. Specialized care and referrals from primary or secondary care were named tertiary care. The use of EHR in health facilities differed substantially. In Finland, more than 75% of facilities were using EHR in primary, secondary and tertiary care facilities. In contrast, Jamaica had less than 25% of primary care facilities that were using EHR in 2015. Less than 25% of secondary care facilities in Panama used EHR. In Austria, less than 25% of tertiary care facilities had implemented EHR; while 50%-75% of secondary care facilities used EHR, less than 25% used EHR in primary care facilities. Apparently, there are different reasons for the slow integration of EHR. In a systematic literature review, Kruseet al[66]. assembled a list of barriers to EHR system adoption in the United States. The initial cost was the most frequent barrier. Technical support, technical concerns, resistance to changing work habits, maintenance, ongoing costs, training, privacy concerns and insufficient time and workflow challenges were other barriers. The most important driving force for the implementation of EHR systems was funding. Seventy-seven percent of the countries had public funding for eHealth, and 40% could confirm private or commercial funding. Donor or non-public funding was set in 63% of the countries. Forty-two percent had funding through public-private partnerships[67]. Practitioners need help to integrate EHRs into their work habits, adapt the workflow and work with EHR effectively. In the third global survey on eHealth, 74% of all countries reported that health science students were receiving pre-service training in eHealth. A total of 77% claimed that health professionals in their country were receiving in-service training in eHealth[67]. Training, money and information about use cases, problems and advantages of EHR are important to expand worldwide use.
Digital biomarkers
Biological markers quantify observations that refer to an interaction between a biological system and a potential hazard[68]. Valuable biomarkers are objectively measured and change in response to changes in therapy or condition. Pulse, blood pressure and blood test outcomes are examples of objective and quantifiable biomarkers. The association between biomarkers and relevant clinical endpoints is used for research and treatment decisions[69]. In recent years, digital biomarkers have been described and measured[70]. Digital biomarkers are defined as characteristic quantifiable measurements made by means of digital devices[71]. They are objectively measured and evaluated as an indicator of normal or pathologic biological processes or biological responses to a therapeutic intervention[72]. There are various sources from which digital biomarkers can be collected, including body sensors, image processing, health platforms and EMR as well as smartphones, wearables or other digital devices[73]. Digital biomarkers are increasingly important sources of data in health care. Related to the field of neurodegenerative diseases, Kourtiset al[74]pointed out different reasons why digital biomarkers collected from mobile devices and wearables present a unique opportunity for collecting data. There is widespread usage of these technologies in society and immediate access to information due to our inherent connectivity. Moreover, the sensitivity and plurality of onboard sensors is increasing, and such mobile devices are uniquely equipped with sensors; thus, the burden on the health care system is low because large segments of the population are already using such devices. From these devices, a broad range of different data can be collected actively or passively. Biomarkers measuredviasmartphones can be movements and geopositioning, speech and language or sleep patterns[74]. A systematic survey of apps listed in international curated health app libraries focused on mobile health apps using built-in smartphone sensors for diagnosis and treatment. After excluding 762 apps according to the applied inclusion and exclusion criteria, 18 apps remained. Onefourth of those apps were aligned with the diagnosis of health conditions. One half was exclusively treatment oriented. Thirty-nine percent of the apps used the camera as a mobile phone sensor. Thirty-three percent of them used the touch screen. In the identified apps, microphones, mobile phone speakers and accelerometers were used more rarely. None of the included apps used GPS[75]. These data can be correlated longitudinally and continuously to forecast critical or medically relevant situations[76]. A smartwatch measuring heart rate, for example, can be matched with a smartphone app that can alert care providers in case of conspicuous abnormalities[70]. There are different categories of digital biomarkers: Risk biomarkers indicate the diseasedevelopment potential in individuals who are not currently ill or having medical problems. Diagnostic biomarkers can detect or confirm the presence of a disease. Serial measurement by monitoring biomarkers can be used to assess the status of a disease or medical condition or to provide evidence of exposure to a medical product. If interested in the likelihood of a clinical event, prognostic biomarkers of progress or disease recurrence can be used. Some people are more likely to experience a (un)favorable effect from exposure to a medical product or the environment. To identify those people, the use of predictive biomarkers is recommended. Biological responses to exposure to medical products or environmental agents can be assessed by response biomarkers. Safety biomarkers indicate the likelihood, presence or extent of toxicity by measuring them before and after exposure to a medical product or environmental agent[70]. Platforms connecting technologies can help to raise the diagnostic and prognostic value of the information collected by using multi-sourced biomarkers. Connecting data such as height, weight and step accuracy, for example, helps to estimate information and create meaningful endpoints. Using AI, patients participate in the ongoing process of a deep learning digital health system[70]. In the case of gastroenterology, digital biomarkers play an important role, as they do, for example, in cancer patients. Digital biomarkers deliver more precise prognostic information for cancer patients than conventional survey methods[73]. This can be explained by the fact that clinicians no longer collect data only at one or a few points in time; digital biomarkers allow the continuous collection of data in a real-world setting[73]. Despite the increasing prevalence of digital devices, there is still little research on biomarkers in the field of gastroenterology.
CHALLENGES
In the section above, we described various examples, such as the use of smartphone apps for self-management, as well as the use of EHR and telemedicine. While the benefits for such digital interventions on self-management and the management of diseases in general in the field of gastroenterology have been described, there are various challenges that have to be resolved. While the challenges are complex, we will first address an overview of topics. Then we will describe selected specific aspects of these challenges in detail. Currently, all digital interventions are highly complex, which means that both the development and the evaluation and implementation of such interventions are difficult and context dependent[77]. Gaining and accumulating evidence-based knowledge is difficult in a number of ways because the interventions are often not comparable due to the many different components that are often not evidence-based[29]. Moreover, as we mentioned before, even if a digital intervention has a profound evidence base, there is a significant regulatory ambiguity, especially for market access and reimbursement[78]. In many fields of digital health care, the current evidence of the efficacy and efficiency is limited, and research is in its infancy[5]. Furthermore, the development of digital interventions often takes place in interdisciplinary teams in the professional context of computer interaction and social sciences and medicine. Such studies are usually complicated and suffer from limitations resulting from the interdisciplinary aspects[65].
Quality of apps
The main challenge regarding smartphone health apps is the disparity between their proclaimed benefits and their objectively proven and evidence-based benefits[79]. This is a challenge for apps in all fields of health care. The limited evidence demonstrating the quality of apps has been a research topic for apps in mental health selfmanagement of asthma[79], self-management of diabetes[80]management of postoperative pain[12]and sleep management[81]. A systematic review conducted by Vilardagaet al[82]on smartphone applications to support smoking cessation suggested that the majority of the studies in this field have been performed in early stages of app development, such as user-centered design studies, and the vast majority of the apps use only a limited number of theoretical mechanisms of intervention delivery. Furthermore, the study revealed that the vast majority of apps were not tested in welldesigned randomized controlled trials, which leads to only limited evidence regarding possible benefit. In another review, Alessaet al[83]aimed to describe and assess apps in to support the management of hypertension available in different app stores. The authors included 186 apps in their analysis and identified that only a small number of the included apps were likely to be effective. This is because most of the included apps were missing an underlying theoretical foundation in behavioral theories or even basic strategies relating to self-management interventions[83]. The one major single function of most of the apps was to provide educational information, and just a few apps included comprehensive functionalities, which are probably more effective than just a single functionality[83]. Related to the field of gastroenterology, a systematic assessment of apps for the self-management of IBD identified similar problems[40]. From the 238 identified apps in the major app stores, the investigators included twenty-six apps in the final analysis of the app content. A major result was that the overwhelming majority of the apps for IBD suffered from a lack of involvement of medical and health professionals and had only limited coverage of international consensus guidelines for IBD[40]. Currently, there are no generally accepted criteria for the qualitative evaluation of apps[27]. In a systematic review to identify and summarize criteria for the assessment of the quality of apps, the authors reported large heterogeneity of different criteria for evaluating the quality of an app[84]. They identified thirty-eight classes of assessment criteria for the quality of health-related apps. Later, they were able to aggregate these thirty-eight criteria into seven main categories with thirty-seven subclasses. The seven main categories were design, information/content, usability, functionality, ethical issues, security and privacy, and user-perceived value of the app[84]. Although various methods have been developed in recent years to improve the quality of smartphone apps, these methods have not been applied in many studies[84]. One of the most widely established methods for evaluating the quality of apps is the Mobile Application Rating Scale (MARS)[85]. By using the MARS, a score is calculated with four multi-item sections: Engagement (5 items), functionality (4 items), aesthetics (3 items), and information quality (7 items); additionally, there is a subjective section (4 items)[86]. MARS is a validated scale and is now available in different languages, such as German[87]and Spanish[88].
Synthesis of app evidence
One of the central research topics regarding digital health tools is the evaluation of the effectiveness and efficiency of such digital interventions. There is currently only little evidence, and only a few randomized controlled trials exist. The question is which level of evidence is necessary prior to widespread use of digital health apps[89]. A systematic literature review of the evidence-based evaluations, conducted by Enamet al[90], revealed that a lack of standardization of eHealth interventions is a substantial barrier to assessing the full potential of eHealth interventions. Standardization could significantly improve the quality of intervention studies and, furthermore, could also ease the implementation of eHealth interventions. To generate evidence in the field of digital interventions, it is important that trials are carried out according to standardized procedures, evaluation models and theoretical frameworks[91]. In the field of telemedicine, standardized methods are available, such as the[92]model for the assessment of telemedicine, which is an evaluation framework for telemedicine that focuses on the measurement of effectiveness as well as the quality of care[93]. The MAST includes three domains including assessment, multidisciplinary assessment and transferability of the results[94]. Kidholmet al[94]conducted a scoping review of studies in which the MAST was used. They included twenty-two studies and summarized that, in the predominant number of studies in which the MAST was used, a single domain was used rather than the complete framework. The authors emphasize that the MAST was developed to be used as a complete framework and to the use of single domains was not recommended[93]. The overall conclusion in the context of the MAST is that the model is not stringently used, which leads to a lack of standardization and comparability between trials on digital interventions. The discussion about the evidence base of digital interventions has intensified with the publication of the evidence standards framework for digital health technologies from the National Institute for Health and Care Excellence[95]of the National Health Service.
Patient-physician relationship
The use of mobile health applications and medical apps in clinical practice changes the relationship between patients and physicians. There are several opportunities as well as risks in the use of eHealth and the effects on patient-physician communication. One aim of eHealth services is to increase the participation of patients in their own health care. Patients and caregivers should work together in a collaborative process. Grunlohet al[96]evaluated the descriptions of daily physician practice on information about patient participation. All physicians reported that they focus on patient participation, but only little objective proof of this could be found. If physicians do not provide participation support, it is possible for patients to use the internet for information and to increase their participation. The attitudes towards patients who bring information from the internet to a consultation differ. Physicians who use the internet professionally and use a diverse form of media have the most positive attitude towards those patients, and an improvement of the physician-patient relationship was observed in this context. However, some physicians argue that patients are not able to differentiate between accurate and inaccurate content. Regardless of how their own internet use was described, many physicians reported that internet-informed patients are often misinformed. Physicians who were critical internet users were least likely to expect a more time-consuming consultation with patients who used the internet in advance[97]. Fifty-five percent of patients using the internet to find health information reported a change in the way they think about their health. Most of them reported that they were making subsequent health-related behavioral changes, such as asking more questions during office visits (66%), increasing their adherence to physician advice (54%). Another study discovered that patient-physician agreement on the medical situation and recommended treatment is important for patient compliance. Physician quality itself is also important for compliance[98]. This implies that internet information can help to build a new partnership between patients and physicians, where informed decisions can be made. Physicians view their role as responsible and trusted[96]. Luet al[99]conducted a study about the use of online health communities (OHCs), which supports the previous information. They found that OHCs have a positive impact on patient compliance, which can be enforced even more by guiding physician-patient communication in the OHCs. The opportunity to share high-quality health information with patients and discuss the benefits, risks and costs of treatment options encourages the patients. Patients can participate in health-related decision-making, and the misunderstanding of information decreases[99]. eHealth applications not only change the way people inform themselves or track health information but also change communication. The face-to-face interaction is no longer the only way for physicians and patients to interact with each other. Telehealth and telemedicine are a part of the history of technology in healthcare, and they have the potential to increase health care for people with limited access. As we pointed out before, the use of telecommunications technologies offers people in remote locations, people with poor health and people with other limitations new ways to interact with health care professionals[100]. However, while the use of the internet for health purposes has increased[101], online communication between physicians and patients is still rare. Scheduling an appointment, requesting or renewing a prescription or asking questions are important future eHealth applications. Consultations with health professionals online are still rather uncommon in most countries, but the interest among citizens is high and increasing[102]. The physician’s perspective on telemedicine has differed between studies. Less than half of responding physicians in a study in Lebanon believed that web-based apps and social media could be useful for patient-physician communication. The other half (47.5%) was strictly against the use of virtual forms of communication as they feared breaching privacy and confidentiality[103]. In another study, physicians who frequently used the internet for professional use were more likely to take a positive position towards the use of the internet for communication with patients[97]. Online consultation is a possible solution for people living in rural areas or working full time. Practitioners feared this might be more time consuming and a threat to confidentiality[103]. However, studies have reported that the length of telemedicine consultations did not differ from that of the in-person consultations[104]; in some instances, online consultations were even time saving[101]. However, trial findings indicate that telemedicine consultations are more physician centered. It happens more often that the physician controls the dialogue, while the patient is more passive than they are in in-person consultations[104]. However, patient-physician communication can still benefit from eHealth. The benefit can be even stronger if eHealth literacy helps patients to keep control in online consultations and everyone is better informed about the limitations and security needs of eHealth.
eHealth literacy among patients and physicians
In addition to the above-described aspects of a changing communication, interaction and relationship between patients and physicians as well as the ubiquitous availability of online information, there are many barriers for internet users seeking information on health-related topics. There are also barriers to the interpretation of medical jargon and inconsistencies of information found in online research across different sources[105]. Barriers arise not only from the unmanageable mass of freely available health information but also from the limited access to medical articles that are not freely available, from which information may be required[105]. Due to these manifold problems, internet users sometimes find it difficult to draw the correct conclusions and apply the information found to their individual situation. In this context, finding health-related information is centrally linked to the concept of health literacy. Patient health literacy is understood as the motivation, ability and knowledge to identify, understand and evaluate information relevant to one's own health and the ability to use this information to maintain health and to obtain support from the health system when needing assistance or treatment. From the representative HLS-GER study about the health literacy of the German population, it can be assumed that 54.3% of Germans have limited health literacy. People with low health literacy are more likely to assess their own health as wors[106]. In this context, the concept of eHealth literacy is becoming increasingly important. eHealth literacy was defined by Normanet al[107]as the ability to search for, find, understand and critically evaluate health-related information in electronic media in order to apply the knowledge to solve specific health problems. eHealth literacy is the most commonly used term when describing the competence of users searching for health information in the context of digital media[108]. Normanet al[107]understand eHealth literacy as a kind of meta-competence consisting of six different sub-competences: Basic reading and numeracy, health literacy, competencies in the use of computers, scientific literacy, and media and information literacy. eHealth literacy is not only the ability to search for good health information on the Internet but also implies a literacy and competence in the use of social networks such as Twitter Inc. (which has been dubbed “health twitteracy” by Sorensen)[109]. In the context of gastroenterology, it is known that Internet users with a high eHealth literacy are more likely to have knowledge and previous screening practices related to colorectal cancer compared to users with a low level of eHealth literacy[110]. In view of the increasing relevance of digital health information, it is important for doctors to take an in-depth look at changing information needs. In general, healthcare providers should be able to critically assess health information on the Internet to advise patients on how to deal with internet research and critically evaluate digital content[111].
Ethical considerations
The implementation of new digital technologies in routine clinical practice will bring fundamental changes to the field of medicine. However, there are several ethical issues that need to be critically discussed and addressed. MHAs will have the potential to change and hopefully improve medical systems in many ways, including access to specialized medical services in rural, underserved areas and low-barrier and low-cost access to medical treatments[112]. However, at the same time, the traditional patient–physician interaction is going to change, as described in the chapter above. Therefore, several points need to be taken into account.
Apple’s iOS and Google’s Android system have a combined market share of more than 95%. Both systems differ in terms of data security, privacy settings, regulations and security surveillance of their app marketplaces. The development of apps should not prioritize one of the two predominant smartphone systems so that access to medical apps is available to all smartphone users and not just for those who can opt to pay for more expensive and secure devices[113].
Today, there is no possible international regulation of smartphone apps, even if they serve as medical apps and, therefore, as diagnostic or therapeutic tools. Under ethical considerations, a way to ensure that all users of health-related apps understand the apps they are using needs to be established. Users have to comprehend the positive and negative implications that the use of these digital medical tools can have on their health. As patient-physician interactions will be changing due to digital medicine, there is also a risk that real-life doctors will only be affordable for patients with adequate insurance or financial resources, while others will be predominantly treated by avatars or telemedical consultants.
Many digital innovations will be designed for chronically ill people. These patients are typically older people with no or limited access to modern ICT devices, such as smartphones or wearables, and this population has nonexistent or only limited digital literacy. This needs to be taken into account when planning digital medical solutions.
Legal and data privacy considerations
Health care sectors around the world are among the most strictly regulated markets for a good reason. Health data and medical treatment data are among the most vulnerable and sensitive existing data. This makes innovative digital interventions more difficult to establish in the medical community, as medical products need to be highly safe before widespread use and market adoption[114].
Many people and health care professionals are critical towards the implementation of (mobile) digital solutions in medicine. This is mostly due to their fear of data security and protection. There are no questions that, for digital medical products, as for any other conventional medical treatment, the same strict data security and protection regulations need to be validated. However, when correctly used, digital services can provide the highest levels of data security and protection. Correct and secure implementation of data security and integrity in digital services has been shown, for example, for secure online banking, insurance services or online retail for many years. Correctly implemented secure EHR or telemedical services will provide much higher security levels than traditionally used services, such as unsecure email or messenger correspondence. However, many health and fitness apps provide only very low or no data security for stored patient data, and this cannot easily be seen or understood by the naïve user. To date, there exists no seal or certification that makes it easy for the end user to understand which products use high industry-standard levels of security and are safe to use. The remuneration of digital medical services has also not been clearly solved in most countries. While certain regulations exist regarding payment for telemedical treatment, many issues have not yet been solved. Most health or fitness apps, for example, currently either finance themselves with advertisements or by selling data, or they have to be paid for by the individual patients[115].
Interoperability – technical aspects
The health system is one of the industries with the highest level of data production and storage needs. What makes this difficult is that all of the data exist in multiple silos, which are usually not compatible with each other. For one single patient, data will exist and be stored in different electronic or analogue hospital files where the patient was treated, in different outpatient clinics or ambulatory care services, and in different pharmacies. In addition, data that the patient himself has recordedviawearable devices,etc.will exist in the future. All of the data are stored in different systems and different file formats, which makes data use and interoperability difficult. This is one of the main reasons why the introduction of the EHR, which must use common interoperable standards and interfaces, is one of the most important aspects in terms of the useful implementation of digital medical innovations[116].
CONCLUSION
Digital interventions, such as MHAs and MAs, offer potential for diagnostic and treatment advances in the field of gastroenterology and the management of chronic diseases in general. In particular, patients with chronic diseases and health care professionals will benefit from these interventions in many different ways. Sufficient proof of benefit, however, depends on high-quality evaluation, which must be based on the standards of evidence-based medicine. This issue is complicated for digital interventions for many reasons, and to date, the specific standards for development and evaluation are generally missing. In this context, it should be clearly emphasized that frameworks of standardization, at least in many parts, can harmonize the research in the field of digital interventions. Continuous work on standardization with a clear focus on the rules of evidence-based medicine would lead to a better understanding and interpretation of the actual evidence.
Moreover, this is also necessary for the assessment of the reimbursement of such digital interventions. This would be particularly useful in guiding health care professionals in almost all health care systems worldwide to apply comparable criteria to better evaluate the reimbursement of digital interventions. Currently, the inclusion of the users concerned, in the sense of user-centered design, does not take place. In addition to the characteristics of this research field mentioned so far, no uniform quality criteria have yet been established that would allow affected users to adequately assess the quality of a medical app. This can lead to patients using an app of insufficient quality or, in the worst case, with the potential to harm the patient and to cause damage or even death. On the basis of this, a strengthening of eHealth literacy must be a central concern of society as a whole and for persons with health-related professions in particular.
 World Journal of Gastroenterology2020年29期
World Journal of Gastroenterology2020年29期
- World Journal of Gastroenterology的其它文章
- Endoscopic management of gastrointestinal leaks and fistulae: What option do we have?
- Watch and wait approach in rectal cancer: Current controversies and future directions
- Evaluation of intrahepatic manifestation and distant extrahepatic disease in alveolar echinococcosis
- Multivariate predictive model for asymptomatic spontaneous bacterial peritonitis in patients with liver cirrhosis
- Clinicopathological characteristics and surgical outcomes of sarcomatoid hepatocellular carcinoma
- Patients' perspectives on smoking and inflammatory bowel disease: An online survey in collaboration with European Federation of Crohn's and Ulcerative Colitis Associations