
Effect of proximal femur nail anti-rotation on unstable intertrochanteric fractures: A prospective observational study
2020-09-04 08:25FaizanIqbalOsamaBinZiaNomanMemonSajidYounusAkramAliuddin
Journal of Acute Disease 2020年5期
Faizan Iqbal, Osama Bin Zia, Noman Memon, Sajid Younus, Akram Aliuddin
1Department of Orthopaedic Surgery, Liaquat National Hospital, Karachi, Pakistan
ABSTRACT Objective: To assess the effect of proximal femur nail antirotation on the functional and radiological outcome of unstable intertrochanteric fractures.Methods: This prospective observational study was conducted in the orthopedic department of a tertiary care hospital. Altogether 86 patients with unstable intertrochanteric fractures treated with proximal femur nail anti-rotation between January 2010 and January 2015 were included. Patients were followed in the outpatient clinic at regular intervals after discharge to assess the radiological union of fractures and complications. The functional outcomes were evaluated after 2 years by Harris hip score.Results: All patients achieved a radiological union of fractures after a mean duration of 24.6 weeks. The follow up showed 23 complications (systemic and local). Eight patients developed urinary tract infections, and three patients developed chest infections, two patients had screw cut-out, one patient had knee stiffness, one patient developed superficial surgical site infection,and four patients developed varus collapse and shortening subsequently. The two year follow up showed that 69 (80.2%)patients had an excellent and good functional outcome according to Harris hip score.Conclusions: With lower complication rates, proximal femur nail is a valid and reasonable option especially in treating unstable intertrochanteric fractures.
KEYWORDS: Hip; Motor vehicle accident; Intertrochanteric fractures; Proximal femur nail anti-rotation
1. Introduction
The incidence of intertrochanteric fractures is increasing rapidly due to the aging of the human population[1]. It is mainly caused by trivial traumas in the elderly such as falls and high energy trauma in the young population[2]. There are several implants invented for fixation of intertrochanteric fractures including both extramedullary[dynamic hip screw (DHS)] and intramedullary devices (proximal femur nail, Gamma nail). With a high incidence of screw cut-out(DHS) can cause significant medial displacement of shaft due to excessive sliding of screws within the barrel[3]. On the other hand,DHS along with trochanteric stabilizing plate can stabilize the trochanteric fracture but could cause significant blood loss[4]. Intact lateral wall plays an important role in the stabilization of unstable intertrochanteric fractures by providing a lateral buttress for the proximal fragment, while it’s deficiency leads to excessive collapse and varus malpositioning[5]. Biomechanically intramedullary nailing is a better choice of implant for fixation of unstable intertrochanteric fractures as nail itself gives support to the posteromedial wall and resist excessive collapse as well[6]. This study aims to evaluate the functional and radiological outcomes of unstable intertrochanteric fractures treated by proximal femur nail anti-rotation (PFNA).
2. Patients and methods
2.1. Ethical approval
The study was approved by the Ethical Review Committee of Liaquat National Hospital, Karachi, Pakistan (0197-2010). The data was collected with informed consent from the patient and their relatives.
2.2. Participants
This prospective observational study was conducted at the department of orthopedic surgery in a tertiary care hospital. A total of 92 patients with unstable intertrochanteric fractures, who referred to hospital in between January 2010 and January 2015 were enrolled.
2.3. Inclusion and exclusion criteria
Patients were included based on inclusion criteria as follows:(1) Unstable intertrochanteric fractures [presence of any or combination of four-part fractures, medial cortical comminution(loss of calcar support), reverse oblique fractures, intertrochanteric fractures with subtrochanteric extension and large or separate posterior greater trochanter fragment are considered as unstable intertrochanteric fractures]; (2) Age >20 years.
Exclusion criteria: (1) Pathological fractures; (2) Open fractures or compound fractures; (3) Age <20 years; (4) Patients with associated injuries in the same or contralateral limb; (5) Simple two-part fracture (Arbeitsgemeinschaft für Osteosynthesefragen class 31-A1). The AO/Orthopedic trauma association fracture classification was used to classify the fractures. The fractures were classified based on pre-operative radiographs. 31-A1: Simple two-part fracture with typical fracture line extending from greater trochanter to medial cortex; 31-A2: Comminuted fracture with a posteromedial fragment, the lateral cortex of greater trochanter, however, remains intact. These are unstable fractures depending upon the size of the medial fragment; 31-A3: The fracture line extends across both the medial and lateral cortex; this group includes both reverse oblique or subtrochanteric extensions.
2.4. Treatment and data collection
On admission, the medical condition of all the patients was assessed and classified according to the American Society of Anaesthesiologists (ASA) grade[7]. The health status of patients was considered good if ASA grade was 1-2, or poor if ASA grade was 3-4. Factors including age, gender, mechanism of injury, the time between injury and surgery (by day), comorbid diseases (diabetes mellitus, hypertension, ischemic heart disease) were recorded. The 1st generation cephalosporin (cefazolin) at a dose of 3 mg/kg was used for prophylaxis. Prophylactic antibiotics were discontinued within 24 h after surgery.
We used a long and standard proximal femur nail for unstable intertrochanteric fractures. The desired position of the helical blade was in the anteroposterior view, in the center of the femoral neck.In the lateral view, it should lie in the center of the femoral neck,and the tip of the blade should lie within 5-10 mm of subchondral bone[8]. The location of the blade within the femoral head was recorded as per the Cleveland method[9]. According to the Cleveland method, the blade position should be center/center.
In most of the cases, we used a cerclage wireviawire passer with a minimally invasive approach to aid and maintain a reduction in intertrochanteric fractures with subtrochanteric extension.
Intra-operative bleeding was calculated from wound suction plus the estimated amount of blood in the gauze. We use 4×4 cm sponge in our study which has an average capacity of (10±2) cm3. We counted the number of completely soaked sponges at the end of the procedure and multiplied it by 10.
Radiographs of the operated limb including both anteroposterior and lateral views were taken to measure TAD, fracture reduction,and position of the blade. TAD was assessed using the method proposed by Baumgärtneret al.[10] who also proposed a three-grade classification system of fracture reduction as well. Varus-Valgus and anteversion-retroversion angulation of <5 degrees is considered an anatomical reduction. If angulation lies between 5 to 10 degrees,then reduction is considered acceptable, while angulation more than 10 degrees on immediate postoperative radiographs is considered poor reduction. Full weight-bearing was allowed three months after surgery based on the evidence of the stability of construct and callus formation on radiographs, except in patients with osteoporosis in which full weight-bearing was allowed after 4 months. Patients were followed up at 6 weeks, 3 months, 6 months, 9 months, and then 6 months thereafter until 2 years. At each follow-up, patients were assessed with radiographs both anteroposterior and lateral views of the operated limb.
Along with intertrochanteric fracture, we also addressed osteoporosis in our study as it may also affect functional outcomes.Singh index is a method to determine the extent of osteoporosis,which is based on radiological appearance of the trabecular bone structure of proximal femur on plain anteroposterior hip radiographs.Based on this grading, patients were divided into two groups, those with osteoporosis (Grade 1-3) and those with little or no osteoporosis(Grade 4-6).
2.5. Statistical analysis
The data were analyzed statistically using IBM SPSS Statistics version 20.0 (IBM Co. Armonk, NY, USA). Descriptive statistics were expressed as frequencies and precentage. Categorical variables were compared by the Fisher exact test. The level of significance was set at α<0.05.
3. Results
3.1. Baseline characteristics
The study included 92 cases of unstable intertrochanteric fractures, in whom 4 patients were lost in follow-up and 2 patients died due to diseases unrelated to fracture. Therefore, 86 patients with complete follow-up were included in this study, among which 46 (53.4%) were male and 40 (46.5%) were female. The mean age was (62.20±12.25) years. The average time of healing was 4.6 weeks.The average delay from the time of injury to surgery was 3.7 d,which was mostly due to the underlying comorbidities. The mean duration of surgery was (65.25±10.10) min. The mean blood loss was (50±10) mL. The mean packed red blood cell transfused was 1.4 mL. The mean length of hospital stay was 10.5 d.
Out of 86 patients, 43 patients were hypertensive, 18 patients had diabetes, 8 patients had ischemic heart disease, and 17 patients had no comorbid. According to the AO classification, 52 patients were of type 31-A2, and 34 patients of type 31-A3. There were 38(44.1%) patients with grade 1 to 3 osteoporosis on Singh’s index and 48 (55.8%) patients with little or no osteoporosis (grade 4 to 6). Besides, motor vehicle accident (MVA) was the main cause for admissions [58 (67.4%)], followed by fall [28 (32.5%)] (Table 1).
3.2. Functional and radiological results
The functional outcome was assessed by the Harris hip score at the end of 2 years. Out of 86 patients, 69 (80.2%) patients had excellent to good functional outcomes, whereas fair to poor results obtained in 17 (19.8%) patients. Bridging callus was observed at 6 weeks in 62 (72.1%) patients and 12 weeks in 24 (27.9%)patients. Obliteration of fracture line was observed at 24 weeks in 72 (83.7%) patients and 28 weeks in 14 patients (16.3%). Quality of fracture reduction was assessed on immediate postoperative radiographs. The anatomical reduction was observed in 62 (72.1%)patients, acceptable reduction in 20 (23.3%) patients, whereas poor reduction observed in only 4 (4.7%) cases. The functional outcome according to Singh index is shown in Table 1. Harris hip score were found to be significantly different between patients with and without osteoporosis (P=0.078).
3.3. Complications
Out of 86 patients, we observed complications in 23 (26.7%)patients. The complications were divided into local and systemic ones. Systemic complications include chest infection, urinary tract, myocardial infarction, deep vein thrombosis, or pulmonary embolism whereas local complications include blade cut-out,infection (superficial or deep), knee stiffness, varus collapse,shortening, and non-union. Eight patients developed urine and three patients developed chest infection on the 3rd postoperative day. Two patients developed screw cut-out postoperatively on the 4th month when patients started full weight bear. One patient developed knee stiffness on the 6th week. One patient developed superficial infection over the incision site on the 10th postoperative day.Four patients developed varus collapse along with shortening of about 2 cm. Therefore, systemic complication rate in our study was 12.7% whereas local complication rate was 13.9%. We also evaluate the relation of ASA score and systemic complication rate as shown in Table 2. The systemic complications were found to be significantly different among different ASA score (P=0.001).

Table 1. Functional outcome of patients according to the Singh index [n (%)].
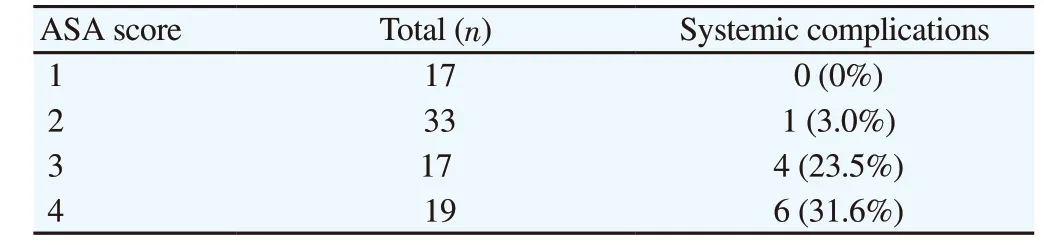
Table 2. Systemic complication rate by ASA score [n(%)].
4. Discussion
The purpose of this study is to evaluate the functional and radiological outcomes of unstable intertrochanteric fractures treated by PFNA. These fractures cause a great financial burden on families and governments, the implants should be carefully selected before treatment.
The management of unstable intertrochanteric fractures is still controversial. There are several ways to address these unstable fractures such as extramedullary devices like DHS with or without trochanteric stabilizing plate, or intramedullary device such as Gamma nail[11,12]. We believe that unstable intertrochanteric fractures should be best managed with PFNA. Proximal femur nail is a more biomechanically stable intramedullary device because of its load-sharing characteristics. With a short lever arm, proximal femur nail can decrease blood loss with minimal soft tissue dissection[13].Surgeons should understand the configuration of fracture before selecting the implant. In this study, we classify fractures according to AO classification, and we exclude type 31-A1 fractures from our study because this study mainly comprises unstable intertrochanteric fractures. Axial loading in type A2 fractures leads to impaction of fracture whereas in type A3 fractures, such impaction doesn’t occur,and medial displacement of distal fragment is common. Traditionally the posteromedial fragment is regarded as an important element in determining the severity of intertrochanteric fractures[14]. In type A2 fractures, the posteromedial fragment is comminuted, but the lateral femoral wall remains intact. Here the proximal femur nail compensates for a posteromedial defect, acting as a buttress to prevent medialization of the distal fragment. In type A3 fractures,the lateral wall might be compromised, which may lead to varus collapse. To prevent varus collapse, abductor muscle force plus internal strength of implant and bone must be equal to or more than the deforming forces. Therefore we used PFNA screw in type A3 fractures, which is then further augmented with cerclage wire to prevent varus collapse. In our study, varus collapse occurred in 4 (4.65%) patients and all 4 patients had underlying osteoporosis.Cerclage wire could not get enough hold on the lateral cortex to prevent varus collapse. In a study conducted by Gadegoneet al.[15],varus collapse of more than 5 degrees was noted in 6 out of 82 patients. In this study, we used screw or cerclage wires to further augment the lateral wall, especially in type A3 fractures. This indicates that augmentation of proximal femur nail either with cerclage wires or screws is necessary to prevent varus collapse.
In the current study, MVA is the most common mode of injury. Out of 86 patients, 58 (67.4%) patients had MVA. This could be due to the increase in MVA in developing countries like Pakistan. Males are more commonly involved than females in the present study. This could be because males in this society are more commonly involved in traveling for various reasons[16]. Tyllianakiset al.[17] observed falls at home are the main cause of injury in elderly patients. Shenet al.[18] also observed that males have more incidence than females.
Shenet al.[18] compared PFNA with other extramedullary devices with respect to blood loss. They concluded that PFNA would be beneficial for patients with unstable intertrochanteric fractures with less blood loss and lower complication rates. In the present study,the mean estimated blood loss was (50±10) mL despite multiple small incisions for the application of cerclage wires. Mean packed red blood cell transfusion is also less in patients with proximal femur nails. We should consider this factor as well especially in patients with underlying comorbidities. In the present study, 48 (55.8%)patients had underlying systemic diseases. Out of 48 patients, 11(12.7%) patients had ischemic heart disease. As post-operative blood count falls, the mortality and morbidity rise[19]. Therefore proximal femur nail is a better option for patients with underlying systemic disease.
In our study, the average length of hospital stay was 10.5 d, which is shorter compared to findings of Sadicet al.[8]. In his study, he concluded that incidences of systemic complications after hip surgery significantly prolonged the length of stay.
Ercinet al.[20] found that the majority of patients with intertrochanteric fractures had underlying systemic diseases, which might require prolonged hospital stay. They also recommend a delay of 24 h to optimize surgery conditions. Efstathopouloset al.[21]suggested early operation within the first 24 h to achieve a good functional outcome and to prevent postoperative complications. In our study, the time interval between injury and surgery was 3.7 d,and these findings are comparable with that of Ercinet al.[20]. We believe that optimizing surgery conditions by treating comorbidities such as hypertension, diabetes mellitus, and ischemic heart disease firstly is more important.
Sadicet al.[8] believe that the ASA class is important, and patients of ASA class 3 & 4 have a higher risk of systemic complications postoperatively than in patients of ASA class 1&2 (P<0.001).Donegan[22] found no relationship between ASA score and systemic complications postoperatively. The majority of patients in our study belong to ASA grade 1 and 2, and 36 (41.8%) patients were in poor health.A total of 69 (80.2%) patients showed excellent to good functional results in this study and 17 (19.7%) patients out of 86 patients showed fair to poor results. Jameset al.[2] found excellent to good functional results in 17 (85%) patients.
We also evaluated the effect of osteoporosis on the functional outcome of these patients as these fractures are common in the elderly. We found excellent to good functional outcome in 31(81.5%) patients with osteoporosis and 38 (79.1%) cases in patients with little or no osteoporosis. We also found fair to poor results in patients with osteoporosis but it was not statistically significant.Akanet al.[23] found inferior outcomes in patients with osteoporosis.
In our study, the radiological outcome of immediate postoperative radiographs displayed anatomical reduction in 62 (72%) patients,acceptable reduction in 20 (23.2%) patients, poor reduction in 4(4.65%) cases which is comparable with the findings of Akanet al.[23]. He found good anatomical reduction in 63 (78.8%) patients,acceptable anatomical reduction in 11 (13.8%) patients, and poor anatomical reduction in 6 (7.5%) patients.
The local complication rate in the present study was 12 (13.9%).The most frequent complication was varus collapse. Salphaleet al.[6] also observed six patients with varus collapse of more than five degrees due to technical problems related to the screw purchase in the femoral head and lateral wall, which caused loosening of screw.He used screws or cerclage wires to augment the lateral wall. The local complication rate in his study was 9 (10.9%), which is slightly lower than our study. Kimet al.[24] used DHS augmented with cement to prevent varus collapse especially in patients with severe osteoporosis. They believed that augmentation of fixation using cement may be a solution in such cases. We believe that the helical blade of PFNA can increase the bone-implant interface and result in compaction of cancellous bone, thereby provide excellent stability of fixation[25].
The drawback of this study is that we used conventional radiographs rather than Dual Energy X-ray absorptiometry scans to assess the extent of osteoporosis due to financial constraints, which makes the result subjective.
PFNA is an excellent implant, especially in treating unstable intertrochanteric fractures. Augmentation of PFNA with cerclage wire in type 31-A3 fracture is a simple and useful technique to prevent varus collapse in unstable fractures.
Conflict of interest statement
The authors report no conflict of interest.
Authors’ contributions
All authors were involved in drafting the article and all authors approved the final version to be published. Study writing and design:F.I. and O.B.Z. Data extraction and Statistics: F.I., N.M., S.Y. Data analysis and interpretation: F.I., N.M., A.A.U., O.B.Z.
 Journal of Acute Disease2020年5期
Journal of Acute Disease2020年5期
- Journal of Acute Disease的其它文章
- Using point-of-care ultrasound in ocular emergencies: A mini review
- Coronavirus disease 2019 (COVID-19), MERS and SARS: Similarity and difference
- An epidemiological report on the burden and trend of injuries in the Philippines from 2011 to 2018
- Epidemiological profile and management of acute pyelonephritis in the emergency department of a tertiary hospital: A retrospective observational study
- Evaluation of the neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and monocyte lymphocyte ratio for diagnosis of testicular torsion
- Antibacterial activity of plant extracts in different solvents against pathogenic bacteria: An in vitro experiment