
0.01%阿托品联合中药离子导入控制儿童中低度近视进展的临床观察
2020-06-03 17:50查桂平汪卓琼
中国现代医生 2020年9期
查桂平 汪卓琼

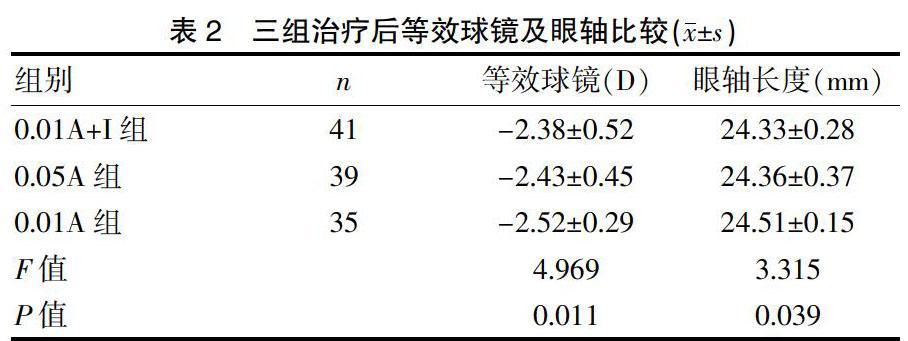
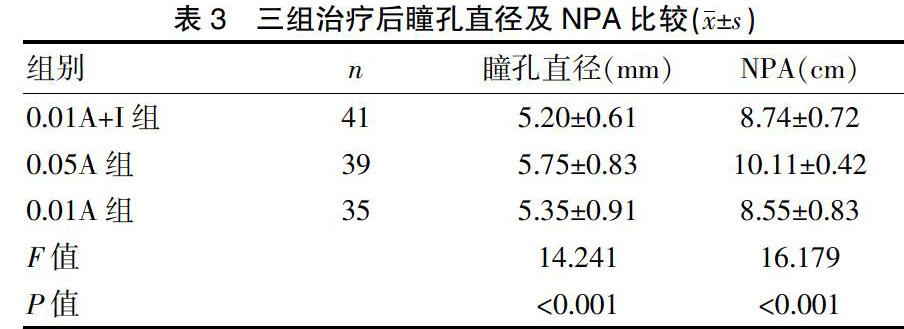
[摘要] 目的 比較单独使用阿托品与阿托品联合中药离子导入控制儿童中低度近视进展的疗效。 方法 收集2017年4月~2018年6月在我院眼科就诊的6~12岁中低度近视儿童115例,随机分为3组,分别接受0.01%阿托品联合中药离子导入、0.05%阿托品、0.01%阿托品治疗12个月。观察治疗后等效球镜、眼轴、视力、瞳孔直径、调节近点的变化。 结果 治疗12个月后,0.01%阿托品联合中药离子导入组、0.05%阿托品组、单独使用0.01%阿托品组等效球镜分别为(-2.38±0.52)D、(-2.43±0.45)D、(-2.52±0.29)D,眼轴长度分别为(24.33±0.28)mm、(24.36±0.37)mm、(24.51±0.15)mm,三组等效球镜度数与眼轴长度比较,差异均有统计学意义(F=4.969,P=0.011;F=3.315,P=0.039)。0.05%阿托品组明室瞳孔直径(5.75±0.83)mm比0.01%阿托品联合中药离子导入组(5.20±0.61)mm、0.01%阿托品组(5.35±0.91)mm增加明显(P<0.001)。调节近点0.05%阿托品组(10.11±0.42)cm比0.01%阿托品联合中药离子导入组(8.74±0.72)cm、0.01%阿托品组(8.55±0.83)cm增加明显(P<0.001)。结论 中药离子导入加强了0.01%阿托品控制近视进展作用,其作用效果相当于0.05%阿托品。同时,需要进一步观察等效球镜及眼轴的变化情况。
[关键词] 0.01%阿托品;中药离子导入;中低度近视;儿童
[中图分类号] R778.11 [文献标识码] B [文章编号] 1673-9701(2020)09-0097-04
[Abstract] Objective To compare the effect of atropine alone and atropine combined with traditional Chinese medicine iontophoresis on the development of middle and low myopia in children. Methods 115 middle and low myopia children aged 6 to 12 years treated in our hospital from April 2017 to June 2018 were selected. They were randomly divided into three groups. And the three groups were given 0.01% atropine combined with traditional Chinese medicine iontophoresis, 0.05% atropine and 0.01% atropine for 12 months respectively. After treatment, the changes of equivalent spherical lens, ocular axis, visual acuity, pupil diameter and accommodation of near point were observed. Results After 12 months of treatment, the spherical equivalent in 0.01% atropine combined with traditional Chinese medicine iontophoresis group, 0.05% atropine group and 0.01% atropine group were (-2.38±0.52) D, (-2.43±0.45) D, (-2.52±0.29) D respectively, and the length of the ocular axis was (24.33±0.28) mm, (24.36±0.37) mm, (24.51±0.15) mm respectively. The differences in the equivalent spherical lens and the length of the ocular axis between the three groups were statistically significant(F=4.969, P=0.011; F=3.315, P=0.039). The pupil diameter (5.75±0.83 mm) in the 0.05% atropine group was significantly higher than that in the 0.01% atropine combined with traditional Chinese medicine iontophoresis group(5.20±0.61 mm) and 0.01% atropine group (5.35±0.91 mm) (P<0.001). The accommodation of near point of 0.05% atropine group(10.11±0.42 cm) was significantly higher than that of 0.01% atropine combined with traditional Chinese medicine iontophoresis group (8.74±0.72 cm) and 0.01% atropine group (8.55±0.83 cm) (P<0.001). Conclusion Iontophoresis of traditional Chinese medicine strengthens the effect of 0.01% atropine on myopia progression, which is equivalent to 0.05% atropine. At the same time, it is necessary to further observe the changes of equivalent spherical lens and ocular axis.
表3 三组治疗后瞳孔直径及NPA比较(x±s)
3讨论
阿托品眼液是非选择性睫状肌麻痹剂,高浓度阿托品作用于M1~M5受体,但低阿托品主要作用于M1受体和M4受体,从而保留了大部分针对控制近视进展的作用,对M3受体影响较小,故对瞳孔及调节影响较小。Lee JJ等[9]尝试使用0.05%阿托品,研究发现0.05%阿托品每年近视进展(-0.28±0.26)D,而对照组进展(-0.75±0.35)D。Fang PC等[10]使用0.025%阿托品每年近视进展(-0.14±0.24)D,对照组(-0.58±0.34)D。同时,Moon JS等[11]发现0.01%阿托品治疗1年后近视增加-0.84 D,0.025%阿托品增加-0.56 D,0.05%阿托品组增加-0.23 D。Chia A等[12]发现0.01%阿托品治疗2年近视加深(-0.49±0.63)D,0.1%阿托品加深(-0.38±0.60)D,0.5%阿托品加深(-0.30±0.60)D,通过对比可以看出控制近视进展与阿托品浓度相关。低浓度阿托品眼液的疗效及安全性一直是研究的热点,学者们试图找到能控制近视进展且副作用小的阿托品浓度。近年来很多研究使用0.01%阿托品,发现0.01%阿托品眼液既能控制近视进展,又能减少副作用[13-14],且停药后近视屈光度反弹要比0.1%、0.5%阿托品小[15],且有研究认为亚洲人群使用阿托品其副作用不引起临床症状的最高浓度为0.02%[16]。但从上述研究中发现阿托品控制近视进展的疗效与其浓度相关,若既要降低阿托品浓度又要达到理想的治疗效果就要考虑联合治疗。Liang CK等[7]发现0.25%阿托品联合眼部针灸治疗比单独使用0.25%阿托品效果好。韩雯婷等[8]认为消旋山莨菪碱联合阿托品滴眼液能有效控制青少年近视进展及眼轴增长。近年来学者们试图通过联合用药来降低阿托品浓度,提升阿托品控制近视进展的作用。
本研究通过治疗1年观察发现0.01%阿托品联合中药离子导入近视加深-0.29 D,眼轴延长0.23 mm;0.05%阿托品组近视加深-0.26 D,眼轴延长0.20 mm;单独使用0.01%阿托品组近视加深-0.61 D,眼轴延长0.36 mm,可见联合治疗比单独使用0.01%浓度阿托品效果更好。再结合治疗后瞳孔大小及调节近点的变化,单独使用0.01%阿托品瞳孔直径约增加0.6 mm,调节近点(NPA)约增加1.2 mm,0.01%阿托品联合中药离子导入瞳孔直径约增加0.5 mm,调节近点约增加1.5 mm,0.05%阿托品瞳孔直径约增加1.1 mm,调节近点约增加2.5 mm。单独使用0.01%阿托品和0.01%阿托品联合中药离子导入均未出现明显的近距离阅读困难、畏光等症状,但0.05%阿托品有部分受试者畏光,近距离阅读需要远视镜片协助,与Kaymak H等[17]报道0.01%阿托品的副作用基本一致。
综上所述,阿托品眼液浓度增加,控制近视进展效果越好,但副作用增加,如瞳孔直径增加、调节障碍,引起畏光、近距离阅读困難。联合治疗既保证了治疗效果又可以降低阿托品浓度,进一步减少副作用。但也有研究认为0.01%阿托品对中低度近视控制有效,对近视进展很快的部分人群可能效果一般[18]。有研究认为以往实验观察到低浓度阿托品的副作用小,但观察时间不够,需5~10年以上的观察,其长期的副作用仍不明确[19],故临床使用阿托品眼液控制近视进展尚未达成共识[20],需要长时间观察疗效及可能的副作用。本研究不足之处没有对照组,且观察时间较短,这些部分将在下一步研究计划中进一步得到完善。
[参考文献]
[1] Holden BA,Jong M,Davis S,et al. Nearly 1 billion myopes at risk of myopia-related sight-threatening conditions by 2050-time to act now[J].Clin Exp Optom,2015, 98(6):491-493.
[2] Flitcroft DI.The complex interactions of retinal,optical and environmental factors in myopia aetiology[J].Prog RetinEye Res,2012,31(6):622-660.
[3] Hayashi K,Ohno-Matsui K,Shimada N,et al.Long-term pattern of progression of myopic maculopathy:A natural history study[J].Ophthalmology,2010,117(8):1595-1611.
[4] Weiss RS,Park S. Recent updates on myopia control: preventing progression 1 diopter at a time[J]. Curr Opin Ophthalmol,2019,30(4):215-219.
[5] Kinoshita N,Konno Y,Hamada N,et al. Additive effects of orthokeratology and atropine 0.01% ophthalmic solution in slowing axial elongation in children with myopia:first year results[J]. Jpn J Ophthalmol,2018,62(5):544-553.
[6] Zhao Y,Feng K,Liu RB,et al.Atropine 0.01% eye drops slow myopia progression:A systematic review and Meta-analysis[J]. Int J Ophthalmol,2019,12(8):1337-1343.
[7] Liang CK,Ho TY,Li TC,et al.A combined therapy using stimulating auricular acupoints enhances lower-level atropine eyedrops when used for myopia control in school-aged children evaluated by a pilot randomized control led clinical trail[J].Complement Ther Med,2008,16:305-310.
[8] 韓雯婷,荣翱,徐蔚.消旋山莨菪碱联合阿托品滴眼液预防青少年近视疗效分析[J].中华医学杂志,2019,99(24):1859-1863.
[9] Lee JJ,Fang PC,Yang IH,et al.Prevention of myopia progression with 0.05% atropine solution[J].J O Cul Pharmacol Ther,2006,22(1):41-46.
[10] Fang PC,Chung MY,Yu HJ,et al.Prevention of myopia onset with 0.025% atropine in premyopic children[J]. J Ocul Pharmacol Ther,2010,26(4):341-345.
[11] Moon JS,Shin SY.The diluted atropine for inhibition of myopia progression[J]. Int J Ophthalmol,2018,11(10):1657-1662.
[12] Chia A,Chua WH,Cheung YB,et al.Atropine for the treatment of childhood myopia:Satety and efficacy of 0.5%,0.1%,and 0.01% doses(Atropine for the Treatment of Myopia2)[J].Ophthalmology,2012,119(2):347-354.
[13] Joachimsen L,B?觟hringer D,Gross NJ,et al. A pilot study on the efficacy and safety of 0.01% atropine in German[J].Schoolchildren with Progressive Myopia[J]. Ophthalmol Ther,2019,8(3):427-433.
[14] Kesarwani SS. Mumbai group of paediatric ophthalmologists and strabismologists.consensus statement and guidelines for use of dilute atropine sulphate in myopia control[J].Indian J Ophthalmol,2019,67(4):461-463.
[15] Chia A,Chua WH,Wen L,et al.Atropine for the treatment of childhood myopia:Changesafter stopping atropine 0.01%,0.1% and 0.5%[J].Am J Ophthalmol,2014, 157(2):451-457.
[16] Cooper J,Eisenberg N,Schulman E,et al.Maximum atropine dose without clinical signs or symptoms[J]. Optom Vis Sci,2013,90(12):1467-1472.
[17] Kaymak H,Fricke A,Mauritz Y,et al. Short-term effects of low-concentration atropine eye drops on pupil size and accommodation in young adult subjects[J]. Graefes Arch Clin Exp Ophthalmol,2018,256(11):2211-2217.
[18] Clark TY,Clark RA. Atropine 0.01%eyedrops significantly reduce the progression of childhood myopia[J]. J Ocul Pharmacol Ther,2015,31(9):541-545.
[19] Prousali E,Haidich AB,Fontalis A,et al.Efficacy and safety of interventions to control myopia progression in children:An overview of systematic reviews and meta-analyses[J]. BMC Ophthalmol,2019,19(1):106.
[20] Zloto O,Wygnanski-Jaffe T,Farzavandi SK,et al. Current trends among pediatric ophthalmologists to decrease myopia progression-an international perspective[J]. Graefes Arch Clin Exp Ophthalmol,2018,256(12):2457-2466.
(收稿日期:2019-10-30)
猜你喜欢
世界最新医学信息文摘(2022年52期)2022-12-16
医学食疗与健康(2022年2期)2022-04-23
人生与伴侣·共同关注(2022年2期)2022-03-14
检验医学与临床(2020年20期)2020-11-02
广东医科大学学报(2020年6期)2020-02-06
国际眼科杂志(2019年7期)2019-07-25
中医眼耳鼻喉杂志(2019年3期)2019-04-13
数理医药学杂志(2019年1期)2019-01-14
37°女人(2018年6期)2018-06-09
中国眼镜科技杂志(2017年14期)2017-07-24
