
乌司他丁辅助治疗重症感染性休克的价值分析
2020-06-01 10:12李炬灵
中国实用医药 2020年12期
李炬灵

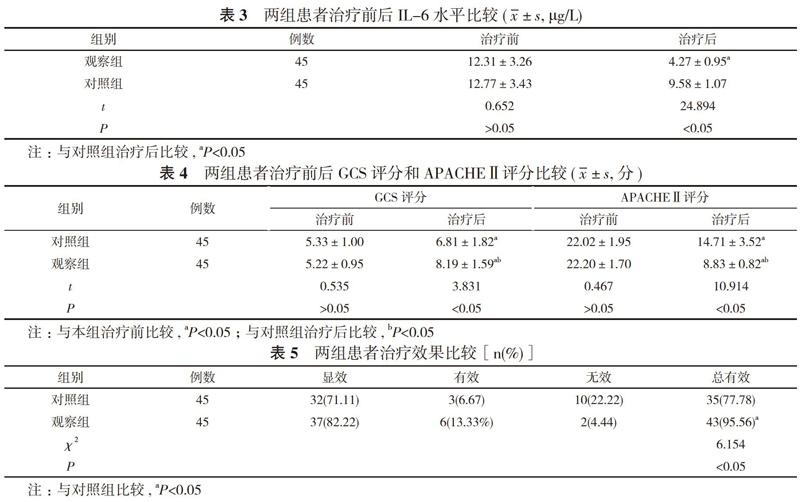
【摘要】 目的 探究临床用乌司他丁辅助治疗重症感染性休克的治疗效果。方法 90例重症感染性休克患者, 随机分为观察组与对照组, 每组45例。对照组患者采用西医常规治疗, 观察组患者在对照组基础上联合乌司他丁治疗。比较两组患者治疗效果、体温情况、感染情况以及治疗前后白细胞计数、白细胞介素-6(IL-6)水平、格拉斯哥昏迷量表(GCS)评分、急性生理功能和慢性健康状况评分系统Ⅱ(APACHEⅡ)评分。结果 治疗后, 观察组白细胞计数(7.34±1.32)×109/L低于对照组的(9.41±1.16)×109/L, 差异具有统计学意义(P<0.05)。治疗后, 观察组高热、感染体征发生率分别为97.78%、86.67%, 均高于对照组的82.22%、62.22%, 差异具有统计学意义(P<0.05);观察组体温恢复时间、感染消失时间分别为(7.19±1.39)、(3.88±0.89)d, 均短于对照组的(9.81±1.88)、(10.76±1.57)d, 差异具有统计学意义(P<0.05)。观察组患者血清IL-6为(4.27±0.95)μg/L低于对照组的(9.58±1.07)μg/L, 差异具有统计学意义(P<0.05)。观察组患者GCS评分和APACHEⅡ评分较治疗前均有所改善, GCS评分(8.19±1.59)分、APACHEⅡ评分(8.83±0.82)分均优于对照组的(6.81±1.82)、(14.71±3.52)分, 差异均具有统计学意义(P<0.05)。观察组患者治疗总有效率95.56%明显高于对照组的77.78%, 差异具有统计学意义(χ2=6.154, P<0.05)。结论 乌司他丁具有较好的抗炎效果, 与西医治疗相结合可以提高临床疗效, 加快重症感染性休克患者退热速度, 缩短感染时間, 降低白细胞计数及血清IL-6水平, 改善GCS评分和APACHEⅡ评分, 临床疗效较好。
【关键词】 乌司他丁;重症感染性休克;白细胞水平;联合治疗
DOI:10.14163/j.cnki.11-5547/r.2020.12.002
【Abstract】 Objective To investigate the therapeutic effect of ulinastatin in the treatment of severe septic shock. Methods A total of 90 severe septic shock patients were randomly divided into observation group and control group, with 45 cases in each group. The control group was treated by conventional Western medicine, and the observation group was treated by ulinastatin on the basis of the control group. The therapeutic effect, body temperature recovery time , infection disappearance time, white blood cell count, interleukin-6 (IL-6) level, Glasgow coma scale (GCS) score, acute physiology and chronic health evaluation Ⅱ (APACHE Ⅱ) score were compared between the two groups. Results After treatment, the white blood cell count (7.34±1.32)×109/L of the observation group was lower than that of the control group (9.41±1.16)×109/L, and the difference was statistically significant (P<0.05). After treatment, the body temperature recovery time and infection disappearance time of the observation group were (7.19±1.39) and (3.88±0.89) d, which were all shorter than those of the control group (9.81±1.88) and (10.76±1.57) d, and the difference was statistically significant (P<0.05). After treatment, the serum IL-6 of the observation group was (4.27±0.95) μg/L, which was lower than that of the control group (9.58±1.07) μg/L, and the difference was statistically significant (P<0.05). GCS score and APACHEⅡ score of the two groups were all better than those before treatment of the same group, and GCS score (8.19±1.59) points and APACHEⅡ score (8.83±0.82) points of the observation group were all better than those of the control group (6.81±1.82) and (14.71±3.52) points, and the difference was statistically significant (P<0.05). The total effective rate of the treatment 95.56% of the observation group was obviously higher than that of the control group 77.78%, and the difference was statistically significant (χ2=6.154, P<0.05). Conclusion Ulinastatin has a good anti-inflammatory effect. Combined with Western medicine, it can improve the clinical efficacy, accelerate the speed of fever reduction in severe septic shock patients, shorten the infection time, reduce the white blood cell count and serum IL-6 levels, improve the GCS score and APACHE Ⅱscore. The clinical efficacy is good.
综上所述, 乌司他丁具有较好的抗炎效果, 与西医治疗相结合可以提高临床疗效, 加快重症感染性休克患者退热速度, 缩短感染时间, 降低白细胞计数及血清IL-6水平, 改善GCS评分和APACHEⅡ评分, 临床疗效较好。
参考文献
[1] 吴然, 杨堃. 乌司他丁在重型颅脑损伤治疗中的作用. 中国临床神经外科杂志, 2019, 24(10):595-597, 601.
[2] 李欣, 张平, 曹琳. 乌司他丁联合奥拉西坦对高血压脑出血患者的临床研究. 中国临床药理学杂志, 2019, 35(18):1982-1984.
[3] 黄康, 吕爱莲, 何峻, 等. 血必凈联合乌司他丁治疗感染性休克临床效果观察. 临床军医杂志, 2019, 47(9):1003-1004.
[4] 高静, 刘磊, 王亮亮. 血必净联合乌司他丁治疗感染性休克临床观察. 安徽中医药大学学报, 2019, 38(4):33-36.
[5] 方旭晨, 叶旭辉, 涂春莲, 等. 连续血液净化联合乌司他丁治疗脓毒症休克疗效观察. 内科急危重症杂志, 2018, 24(5):400-402.
[6] 齐英杰, 陈清阁. 乌司他丁联合CRRT治疗感染性休克效果分析. 中国急救医学, 2018, 38(z2):280.
[7] 陈东娇, 麦叶. 乌司他丁注射剂联合血液净化术治疗重症感染性休克患者的临床研究. 中国临床药理学杂志, 2017, 33(21):2095-2097.
[8] 兀瑞俭, 巩德成, 王强, 等. 乌司他丁联合CRRT治疗老年感染性休克患者临床研究. 国际医药卫生导报, 2018, 24(21):3302-3304.
[9] 李晓蕾, 张连涛, 梁贤栋, 等. 参麦注射液联合乌司他丁治疗感染性休克患者临床疗效. 现代诊断与治疗, 2019(14):2374-2376.
[10] 赵继坤. 乌司他丁对感染性休克患者肝肾功能及血管外肺水指数的影响. 中国民康医学, 2019, 31(19):16-18.
[11] 凌世讳. 生脉注射液联合乌司他丁对感染性休克患者血清炎症因子水平的影响. 临床医药文献电子杂志, 2018, 5(8):148-149.
[收稿日期:2020-01-03]
猜你喜欢
现代仪器与医疗(2016年6期)2017-01-12
中国实用医药(2016年27期)2016-11-30
中外医疗(2016年29期)2016-11-30
医学信息(2016年29期)2016-11-28
中国实用医药(2016年22期)2016-08-19
中国实用医药(2016年10期)2016-05-04
中国实用医药(2016年12期)2016-05-04
中国实用医药(2016年7期)2016-03-17
中国实用医药(2016年4期)2016-02-23
