
Cancer burden and trends in China:A review and comparison with Japan and South Korea
2020-05-17 07:28
National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences&Peking Union Medical College,Beijing 100021,China
Abstract Objective:To summarize the cancer burden and trends in China,compare the differences among China,Japan,and South Korea and discuss possible causes of the disparities.Methods:Incidence and mortality data were extracted from the online cancer database including the GLOBOCAN 2018 and the Global Burden of Disease Study 2017.Trend analysis was conducted using the joinpoint analysis,and annual percent changes were calculated.Results:Cancers resulted in approximately 62.9 million disability-adjusted life years(DALYs)in China in 2017.Lung cancer had the greatest contribution,followed by liver cancer,stomach cancer,and esophageal cancer.The trajectory of progress in the reduction of liver and stomach cancers was observed in China.However,China still faced a heavy burden of lung cancer and a growing burden of cancers related to westernized lifestyle such as colorectal cancer,while Japan and South Korea have achieved reductions in colorectal cancer and lung cancer,respectively.Besides,China had a lower age-standardized cancer incidence rate but higher cancer mortality and DALY rates than Japan and South Korea.Conclusions:China is in the cancer transition stage with a rising burden of colorectal,prostate,and breast cancers along with a heavy burden of lung and upper digestive tract cancers.Taking into consideration the effectiveness of screening and tobacco control in Japan and South Korea,improvement in the current tobacco control policy and cancer screening systems may contribute to cancer control in China.
Keywords:Cancer burden;trend;China;comparison
Introduction
Cancer is the leading cause of death worldwide(1).Distinct geographic disparities exist in cancer burden across the world(2).China,Japan,and South Korea are all located in East Asia.As neighboring countries,Japan and South Korea share similar genetic backgrounds and similar culture with China.Also,in terms of cancer burden,these three countries are all facing a heavy burden of upper digestive tract cancers.But China,Japan,and South Korea are at different stages of socio-economic development.Japan and South Korea are ahead of China in industrialization and urbanization and have higher incidence rates of some westernized lifestyle-related cancers,such as breast cancer and colorectal cancer(3).Besides,Japan and South Korea have a longer history of nationwide cancer control programs than China(4,5).Comparison among these three countries for the cancer burden and trends could be useful to track the effectiveness of national screening programs and to identify modifiable risk factors.The results can serve as a scientific reference for cancer control policy planning.
Thus,we sought to provide an overview of cancer burden and trends in China and to compare them with those in Japan and South Korea.Considering the credibility,availability,and comparability of data,we conducted the analysis based on the online cancer database from the GLOBOCAN 2018(6)and the Global Burden of Disease Study 2017(GBD 2017)(7)and we also reviewed cancer survival data from the CONCORD-3(8),cancer registry reports from China(9,10),Japan(11,12),and South Korea(5,13).We hope that this comparative analysis could contribute to improving measures of cancer control in China.
Materials and methods
Data sources
National estimates of age-standardized incidence and mortality for China,Japan,and South Korea in 2018 were obtained from the GLOBOCAN 2018(6).The GLOBOCAN project initiated by the International Agency for Research on Cancer(IARC)systematically quantified the incidence,mortality,and prevalence in 185 countries or territories for 36 cancer types.The projected national rates for China in the GLOBOCAN 2018 were based on the recent data from 92 cancer registries.Observed national rates,including incidence and mortality in South Korea,and mortality in Japan,were available and applied to predict the corresponding rates in 2018.Incidence rates in Japan were estimated using mortality-to-incidence ratios derived from cancer registries(14).For the trend analysis,we referred to the cancer incidence in five continents(CI5)series(15).The incidence data in CI5 series were derived from high-quality national population-based registries including five registries in China,five in South Korea and four in Japan.All age-standardized rates of incidence and mortality were calculated using the world standard population.Cancer survival data were retrieved from the CONCORD-3(8),which provides the largest and latest international cancer survival data.Age-standardized fiveyear survival rates were calculated using the International Cancer Survival Standard weights(16).
Disability-adjusted life years(DALYs)attributable to cancers for China,Japan,and South Korea in 1990 and 2017 were retrieved from the GBD online results tool(7)engineered by the Institute for Health Metrics and Evaluation(IHME).The GBD annually provides age-sexspecific DALYs for countries across the world.Detailed methods for the GBD 2017 study have been reported in previous studies(17,18).In this study,DALYs per 100,000 population estimates for 29 cancer sites in China,Japan,and South Korea in 2017 were presented by sex and age.To reflect the trends of cancer burden,we also showed the percentage change in all-age and age-standardized DALY rates in China,Japan,and South Korea from 1990 to 2017.The age-standardized DALY rates were based on the GBD reference population(18).
Statistical analysis
Join-point models were used(19)to examine the time trends in age-standardized incidence rates for selected cancer sites in China,Japan,and South Korea.We applied the logarithmic transformation of the rates and a maximum number of two join-points(three line segments)in the models.The annual percent change(APC)was calculated to indicate the direction and magnitude of the trends.The term“increase”or“decrease”was used if the APC was statistically different from zero.P<0.05 was considered statistically significant.The trend analysis was conducted by Joinpoint Regression Program(V.4.7.0.0,National Cancer Institute,2019).
Results
Current cancer burden in China
According to the estimates by the GLOBOCAN 2018,about 4,285,033 new cancer cases were diagnosed in China in 2018,which included 2,366,010 males and 1,919,023 females.The crude and age-standardized incidence rates(ASIR)for all cancers were 301.1 and 201.7 per 100,000,respectively.An estimated 2,865,174 cancer deaths occurred in 2018,with 1,791,805 deaths occurring in males and 1,073,369 in females.The crude and age-standardized mortality rates(ASMR)were 201.3 and 130.1 per 100,000,respectively.The incidence and mortality rates were higher in males than in females.Table 1andFigure 1show that breast cancer has the highest ASIR in both sexes combined,followed by lung cancer,colorectal cancer,and stomach cancer.Lung cancer was the leading cause of cancer death,followed by stomach cancer,liver cancer,and esophageal cancer.
Table 2shows all age and age-standardized DALYs per 100,000 populations in China in 2017.The GBD 2017 estimated that cancers resulted in approximately 62.9 million DALYs in China.Lung cancer had the greatestcontribution(24.3%)to the cancer DALY burden in China in 2017,followed by liver cancer(17.7%),stomach cancer(12.4%),and esophageal cancer(7.1%).These four cancer types accounted for more than 60% of cancer DALYs in China.Figure 2illustrates the etiologic constituent of DALYs by age and sex.Leukemia dominated among the youth(<20 years),but brain and nervous system cancer was also an important cancer among young age groups.Foryoung and middle-aged adult males,liver cancer and lung cancer were the leading causes of DALYs.Breast cancer resulted in the greatest part of the DALY burden among young and middle-aged adult females.Among elderly adults(>50 years),lung cancer and liver cancer represented the highest disease burden for each sex separately and combined.
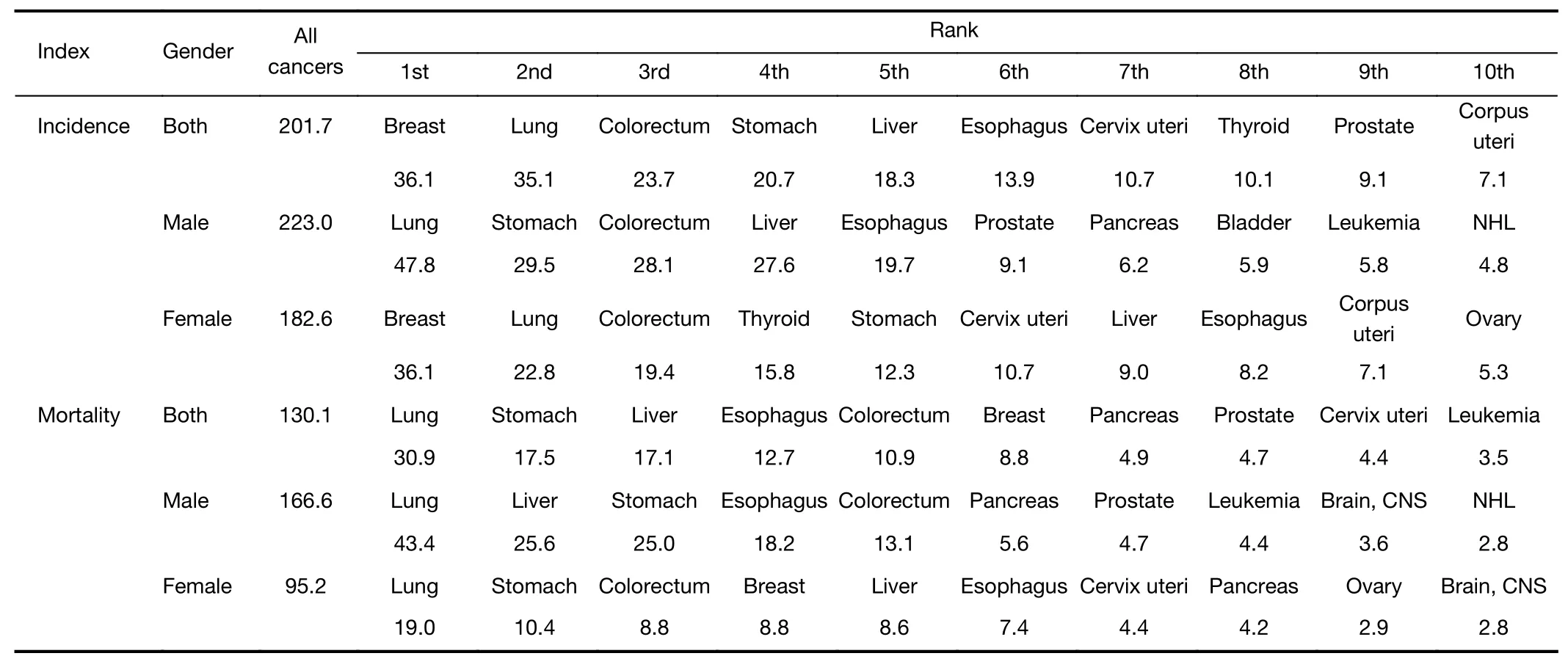
Table 1 Age-standardized cancer incidence and mortality rates per 100,000 populations by gender in China in 2018
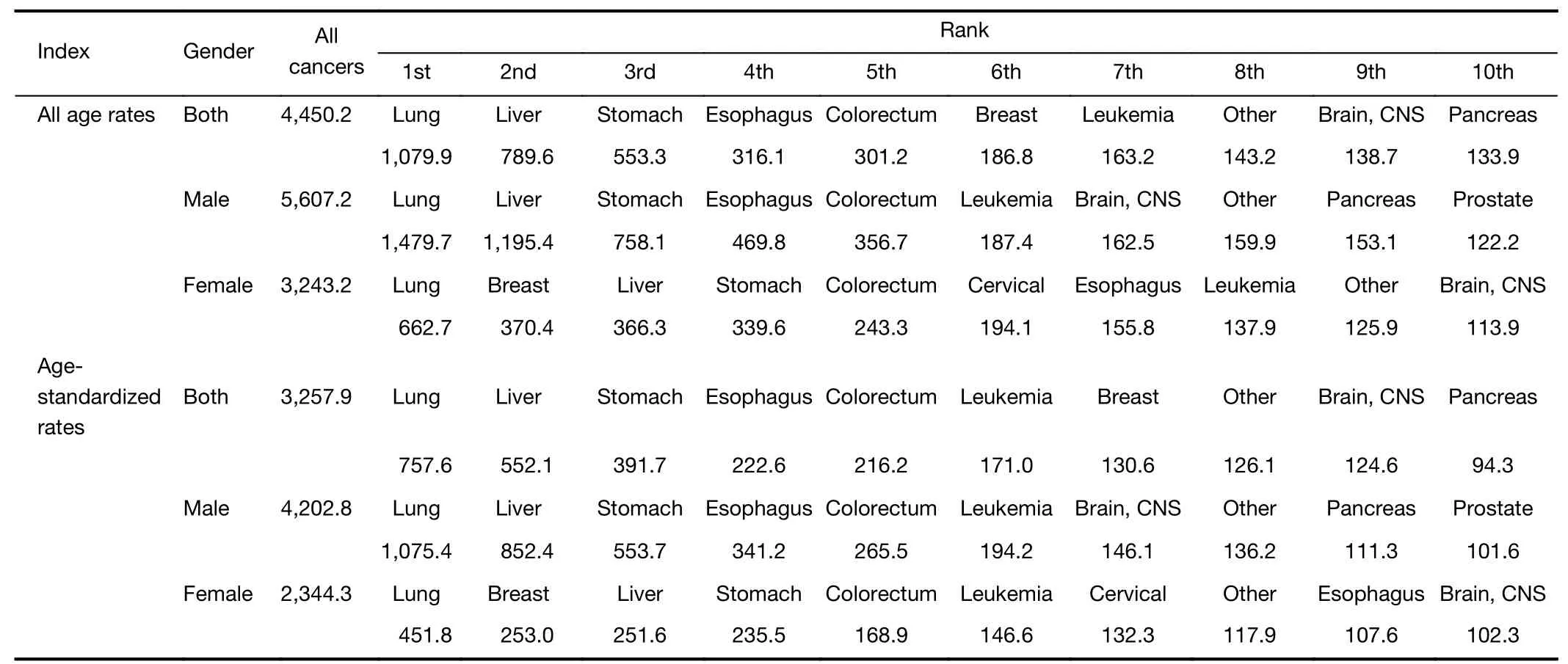
Table 2 All age and age-standardized DALYs rates per 100,000 populations by gender in China in 2017
Time trends in China
Table 3shows that the ASIR for all cancers in females was stable from 1998 to 2012 in China.But a significant downward trend was observed in males during this period.As is shown inFigure 3,the ASIR of lung cancer held steady in both sexes since 2009.Upward trends in the ASIR were observed for colorectal cancer,prostate cancer,and thyroid cancer in males and breast cancer in females.In contrast,the ASIR of stomach cancer,esophageal cancer,and liver cancer showed significant declines for each sex.
Figure 4Ashows the DALYs of 29 cancer types in China,ranked by the number of DALYs in 2017.Lung cancer became the leading cause of DALYs in 2017,replacing liver cancer in 1990.All-age and age-standardized DALY rates of stomach cancer have decreased by 10.7% and 50.3%since 1990,leading to a decrease in its ranking from the second to the third.Esophageal cancer was still the fourth leading cancer for all-cause DALYs,even though the agestandardized DALY rate decreased by 50.1% over the last 27 years.Colorectal cancer and breast cancer both increased in the ranking to become the fifth and sixth leading cancers of all-age DALYs.The all-age DALYs rates increased for colorectal cancer(69.8%)and breast cancer(64.9%)from 1990 to 2017.The all-age and agestandardized DALY rates have increased substantially for pancreatic cancer,ovarian cancer,and lip and oral cavity cancer since 1990.Age-standardized DALY rate of uterine cancer declined by 53% over this period,leading it from 14th in 1990 to fall outside the top 20 causes in 2017.
Comparison with Japan and South Korea in current burden
As estimated by the GLOBOCAN 2018,there was a marked variation in cancer incidence rates among China,Japan,and South Korea,with the incidence in Japan and South Korea being higher than that in China.Overall,the ASIR per 100,000 in South Korea observed among males(332.1)and females(310.6)were nearly 1.5 times higher than the rates among males(223.0)and females(182.6)in China.In contrast to incidence rates,mortality rates in China were nearly 1.5 times higher than those in Japan and South Korea within each sex.
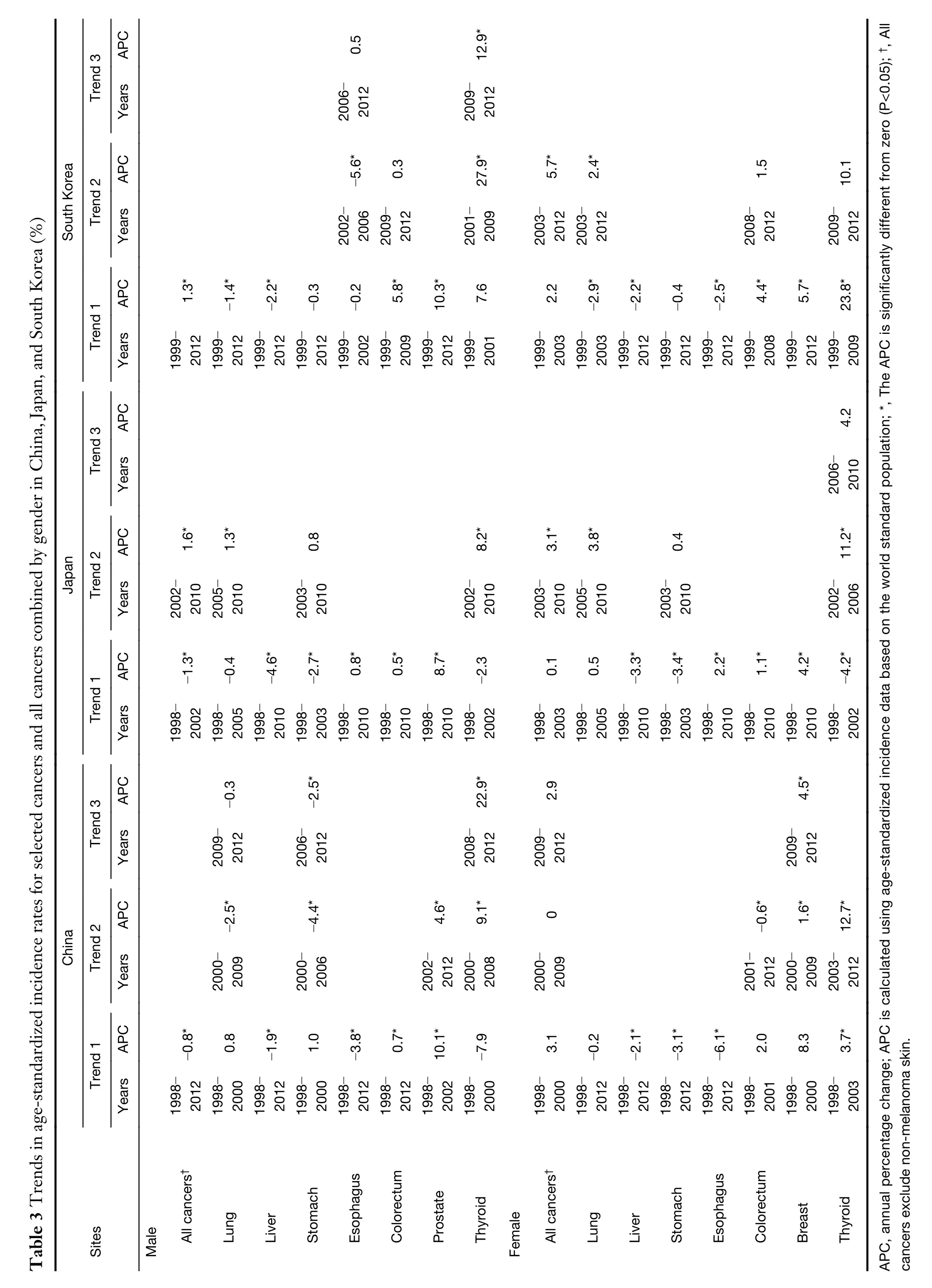
Table 1andSupplementary Table S1show the top ten cancer types by the ASIR and ASMR for males,females,and combined in China,Japan,and South Korea.Lung cancer,stomach cancer,and colorectal cancer were listed in the top five common cancers for males in each country.For females,breast cancer,lung cancer,colorectal cancer,stomach cancer,and thyroid cancer were common cancers in the three countries.Figure 1illustrates the ASIR and ASMR of selected types of cancers in China,Japan,and South Korea in 2018.South Korea had a much higher thyroid cancer incidence than Japan and China.Also,Japan and South Korea had higher incidence rates of breast,colorectal and prostate cancers than China.But the mortality rates of thyroid,breast,colorectal and prostate cancers were similar in these three countries.Another notable aspect was that China had a lower incidence rate but a higher mortality rate of stomach cancer than Japan and South Korea.Correspondingly,Table 4indicates that Chinese cancer patients had lower 5-year survival rates.Especially for stomach cancer,the survival rate in South Korea has achieved 68.9% but its counterpart was less than 36% in China.
Supplementary Table S2shows all age and agestandardized DALYs rates in Japan and South Korea in 2017.Age-standardized DALY per 100,000 populations for all cancers was higher in China when compared with Japan and South Korea.Figure 2shows DALYs per 100,000 populations by age and gender in China,Japan,and South Korea in 2017.Evaluating DALYs by age,we could see that the population with the highest rates of cancer burden in China were younger than those in Japan and South Korea.Lung cancer represented the highest cancer burden for the three countries,followed by gastrointestinal and liver cancers.In terms of the composition of DALYs by age and sex,leukemia was the highest DALY group among the youth in the three countries,followed by brain and nervous system cancer.For young and middle-aged adult males,the largest contributors to DALYs were liver cancer in China and South Korea and colorectal cancer in Japan,respectively.Breast cancer was the leading cause of DALY among young and middle-aged adult females in the three countries.Among elderly adults(>50 years)in the three countries,lung cancer was the top contributor to cancer burden for males,females,and combined,except being replaced with colorectal cancer in Japanese females.
Comparison with Japan and South Korea in time trends
Figure 3shows trends in ASIR by cancer site and gender in China,Japan,and South Korea.In contrast to China,upward trends of ASIR in Japan and South Korea were observed.Rising prostate and female breast cancers contributed the greatest part to the increase of all cancers incidence rates.Lung cancer incidence rate remained generally high in China,Japan,and South Korea.Lung cancer jumped to the first cause of DALYs in 2017,replacing live cancer in China,stomach cancer in Japan andSouth Korea(Figure 4).ButTable 3indicates that the ASIR of lung cancer decreased constantly among males in South Korea.Table 4shows the age-standardized 5-year cancer survival rates in China,Japan,and South Korea from 2000 to 2014.Survival trends were generally increasing in common types of cancers in the three countries,except for the pancreas cancer survival rate in China.
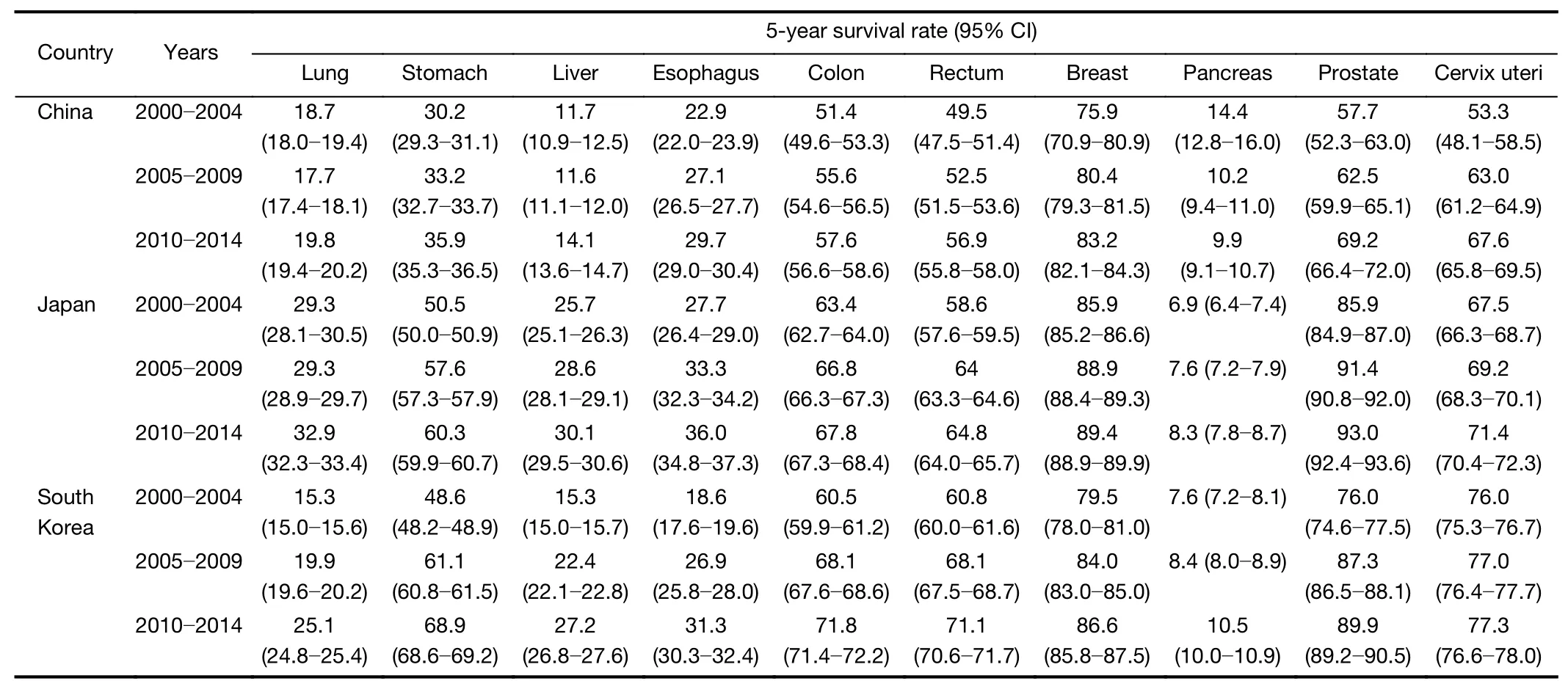
Table 4 Age-standardized 5-year survival rates(%)with 95% CI in adults aged 15−99 years from 2000 to 2014 in China,Japan,and South Korea
China,Japan,and South Korea experienced significant downward trends in ASIR and DALYs for liver cancer.As for stomach cancer,declining incidence was also observed in China and Japan,and the incidence decreased but not statistically significant in South Korea(Table 3).For Japan and South Korea,stomach cancer declined from being the leading cause of all-age DALYs in 1990 to the third in 2017(Figure 4B,C).The trend analysis indicated that the incidence of esophageal cancer decreased in China and South Korea but increased in Japan.The burden of colorectal cancer in China,Japan,and South Korea has increased over the past several decades.In regard with prostate and thyroid cancers,a constantly growing burden was observed in China,Japan,and South Korea.Besides,there was an alarming trend to increase in breast cancer incidence rates in the three countries.
Discussion
In this study,we performed a comprehensive epidemiological analysis of cancer burden and trends in China and compared the differences between China,Japan and South Korea using high-quality data.We found that China was faced with a rising burden of colorectal,prostate,and breast cancers as well as a heavy burden of lung and upper digestive tract cancers.Compared with Japan and South Korea,China has higher ASMR and DALY rates.
China had a higher ASMR and a relatively lower ASIR for all cancers than Japan and South Korea.Several reasons could explain the seemingly paradoxical situation.Firstly,the significant difference in the composition of incident cancers could result in the higher mortality rate in China.The most common incident cancer was lung cancer in China rather than colorectal cancer,which ranked first for ASIR in Japan and South Korea.The ASIR of lung cancer with a poor prognosis,was higher in China(35.1 per 100,000)than that in Japan(27.5 per 100,000)and South Korea(27.8 per 100,000).In addition,prostate cancer with a low fatality rate ranked fourth in Japanese males and South Korean males,while it fell outside the first five common cancers for ASIR in Chinese males.Secondly,China had lower survival rates of thyroid,breast,colorectal,prostate and stomach cancers.One possible explanation is that higher screening uptake rates in Japan and South Korea may drive the inflation of cancer incidence rates and promote the early detection(4,20).For example,endoscopic screening performed in Japan and South Korea(20,21)may bring about the higher survival rates of stomach cancer.Poor access to cancer care in China also could result in the disparities(4).
Concerning the time trends,similar to previous studies(22,23),we found that China,Japan,and South Korea experienced significant downward trends in the burden of liver and stomach cancers.This trend has been explained by a series of lifestyle changes and public health interventions.For example,the spread of hepatitis B virus vaccination(5,24)and reduced aflatoxin exposure(25)are thought to have contributed to the reduction of liver cancer in China.In Japan,it might be associated with the reduced hepatitis C virus infection(26,27).But the increasing prevalence of obesity and diabetes presents a threat to the favorable trend(28).For stomach cancer,the decreasing prevalence of Helicobacter pylori infection,improved living conditions,and better food preservation practices lead to the declining rates(29).Similar to our analysis,an updated analysis from the National Cancer Center of Japan reported an increase of age-standardized esophageal cancer incidence.But the declining mortality was observed(11).Reasons for this divergent trend have yet to be identified.Endoscopic screening conducted in Japan may have an influence.
Another notable sign for optimism is that lung cancer incidence for males in South Korea has been decreasing constantly in recent years,which reflects a corresponding decline in the smoking prevalence in South Korea.Smoking prevalence among South Korean males dropped from 71.7% in 1992 to 39.7% in 2016(30).Tobacco control can prevent lung cancer effectively.Nevertheless,though some progress in tobacco control has been made(31,32),China still faces high smoking rates.The National Health Service Survey conducted in 2013 found that more than 45% of Chinese males are current smokers(33).Also,faltering tobacco control policies is criticized in Japan(34).South Korea serves as an example of tobacco control to China and Japan(35).Stronger tobacco control is urgently needed such as increasing tobacco excise taxes and introducing a national smoke-free law.
In our analysis,colorectal,prostate and breast cancers tended to be more common in China,Japan,and South Korea.But according to the latest data from national cancer registries,colorectal cancer incidence and mortality have shown signs of declining in Japan and South Korea(11,12,36).The long-standing national screening programs may have an impact(37-39).Another notable aspect is that Japan and South Korea set up institutions responsible for providing comprehensive cancer information to enhance public awareness(40,41).The rapid rise of prostate cancer incidence could be explained by the widespread prostatespecific antigen testing.Besides,prostate cancer incidence and mortality in Japan and South Korea has seemingly plateaued in recent years(11,36).The rapidly increasing incidence of thyroid cancer in South Korea(42)sounded the alarm that screening also has the potential to promote overdiagnosis.Limited knowledge could explain the rapid increase in female breast cancer.This trend may reflect a collaboration of changed environmental factors,including the delay of childbearing,increases in the levels of obesity,and the spread of breast cancer screening(3).
Our work has several limitations.First,the comparison of estimates in different countries might be compromised because of variations in data collection and reporting systems across countries.Second,our trend analysis was only based on several registries due to insufficient data availability.The observed trends may not represent national profiles.Moreover,trends in the recent ten years could not be evaluated owing to unavailable up-to-date data.It is required to update the analysis based on more contemporary data and use more compressive analysis such as age-period-cohort analysis.
Conclusions
At the transition cancer stage,China still had a heavy burden of lung and upper digestive tract cancers and faced a rising burden of colorectal,prostate,and breast cancers.China,Japan,and South Korea shared similar cancer profiles and time trends.Although the strategies established in Japan and South Korea should be adapted to the specific contexts of China,we could draw some useful lessons.Compared with Japan and South Korea,China had higher age-standardized cancer mortality and DALY rates but lower incidence.Relatively lower mortality and favorable trends of colorectal and lung cancers appeared in Japan or South Korea indicated the effectiveness of screening and tobacco control.Improvement in the current tobacco control policy and cancer screening systems may contribute to cancer control in China.Also,given huge geographic disparities in cancer burden across China,evidence-based approaches are needed for cancer control programs,and tailored to local profile and population risk.
Acknowledgements
This study was supported by the National Key R&D Program of China(No.2018YFC1313100);Sanming Project of Medicine in Shenzhen(No.SZSM201911015);CAMS Innovation Fund for Medical Sciences(CIFMS)(No.2016-I2M-2-004).
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
 Chinese Journal of Cancer Research2020年2期
Chinese Journal of Cancer Research2020年2期
- Chinese Journal of Cancer Research的其它文章
- The Bethesda System for Reporting Thyroid Cytopathology(TBSRTC):A report of 2,781 cases in a Chinese population
- Efficacy of platinum in advanced triple-negative breast cancer with germline BRCA mutation determined by next generation sequencing
- Clinicopathological analysis of early-stage breast cancer patients that meet indications for BRCA1/2 genetic testing
- Evaluation of human epidermal growth factor receptor 2 status of breast cancer using preoperative multidetector computed tomography with deep learning and handcrafted radiomics features
- Prognostic value and nomograms of proximal margin distance in gastric cancer with radical distal gastrectomy
- Analysis and external validation of a nomogram to predict peritoneal dissemination in gastric cancer