
Co-existence of renal hydatid cyst and renal cell carcinoma in one kidney: A case report
2020-03-04 07:30MaryamMaghboolArminAlivandNajmehZolmajdiAliKharmandar
Maryam Maghbool, Armin Alivand, Najmeh Zolmajdi, Ali Kharmandar
1Pathology Department, Medical School, Fasa University of Medical Sciences, Fasa, Iran
2Urology Department, Medical School, Fasa University of Medical Sciences, Fasa, Iran
3Student Research Committee, Fasa University of Medical Sciences, Fasa, Iran
4Non Communicable Disease Research Center, Fasa University of Medical Sciences, Fasa, Iran
ABSTRACT
KEYWORDS: Renal hydatid cyst; Renal echinococcosis; Renal cell carcinoma
1.Introduction
Cystic echinococcosis, also called hydatid cyst, is caused by the larval stage of Echinococcus (E.) granulosus, a parasitic infestation which affects sheep, cattle and rarely human.Human is an end host of E.granulosus but may be incidentally infected as an intermediate one[1].Echinococcosis is prevalent in the Middle East, especially Mediterranean countries, Africa, Latin America and a few regions in India.It commonly affects liver and lung respectively and hydatid cyst in the urinary system is very infrequent, accounting for about 2%to 5% of all reported human hydatid cysts[2].Kidneys are the most common site of involvement among urinary tract organs.Renal hydatid cyst may remain asymptomatic for several years, even up to 10 years.Renal echinococcosis may occasionally mimic intraabdominal tumors like renal cell carcinoma (RCC)[3].In this report,we present a man with renal cystic mass which was radiologically in favor of RCC but finally, in histopathologic study, co-existence of multifocal papillary RCC and renal echinococcosis was diagnosed.
2.Case report
In August 2017, a 47-year-old man with a past medical history of hypertension from south of Iran, Fars province, visited his familial physician due to mild lower abdominal pain.There was also mild hypogastric tenderness in the physical examination but no flank pain or tenderness, dysuria, urinary frequency, and urinary hesitancy was detected.His physician ordered a pelvic sonography with a clinical suspect to benign prostate hyperplasia.Ultrasound revealed a 50 mm × 52 mm para pelvic cystic solid mass in upper mid pole of the left kidney, in addition to a 3 mm non-obstructive stone and some simple cortical cysts.Then he visited a urologist and underwent contrast-enhanced computed tomography (CECT).The radiologist reported a 59 mm × 50 mm heterogeneously enhancing solid cystic lesion arising from the upper pole of the left kidney with central extension in favor of RCC.No perinephric invasion was seen.Other radiological findings were some simple cortical cysts in the right kidney, multiple reactive enlarged para-aortic retrocaval lymph nodes with the maximum size of 8 mm × 4 mm and a 35 mm × 20 mm cystic lesion in caudate lobe of his liver suggesting cystic echinococcosis (Figure 1).All findings in laboratory blood and biochemical examination, including Complete Blood Count(CBC), serum Creatinine (Cr), Blood Urea Nitrogen (BUN),serum Na+& K+, were in their normal range.The urologist finally decided to remove his left kidney due to high suspect to RCC.Open retroperitoneal nephrectomy was performed for him.The removed left kidney was sent to histopathology laboratory of Fasa Valiasr Hospital.The size of kidney was 80 mm × 40 mm × 40 mm.Serial cut sections showed multi lacunar cystic lesions with the maximum size of 40 mm × 30 mm × 30 mm with multiple globoid floating creamy cystic lesion in medullary portion.Microscopic slides were prepared and stained by Hematoxylin & Eosin staining protocol.Renal cystic echinococcosis in the medullary portion of kidney was the main final diagnosis and there were also some findings suggestive for RCC, with the maximum tumor size of 35 mm × 30 mm × 20 mm located in the cortex, but as the capsule of tumor was present and nuclear gradeⅡ, this lesion was better to be considered as multifocal papillary RCC.The patient was followed by CECT,three and six months later and there were no evidence of metastasis or tumor growing during this time (Figure 2).He also prescribed to take Albendazole (400 mg twice a day) for three months after surgery which is a proper medication regimen for both renal hydatid cyst and liver hydatid cyst.
这项工作的成果确实有助于我们证明天文学家长期以来的猜测,但离严格证明下面这个猜想还差得很远:不仅银河系中心潜藏着一个超大质量黑洞,许多可观测星系的中心都是如此。因此,星系内的所有天体环绕着星系中心运动,但时间和空间在这里终结,任何坠入星系中心的恒星都会永远消失。
This study has obtained the patient’s consent and signed a form to keep his identity private.Also, the patient is free to quit the study whenever he wants without any consequences.The study is conducted with the approval granted by Fasa University of Medical Sciences (Approval No: IR.FUMS.REC.1398.022).

Figure 1.A 47-year-old man with a past medical history of hypertension from south of Iran, Fars province.Contrast-enhanced computed tomography findings suggest multi-organ involvement by echinococcal infection.A:Heterogeneous loculated cystic structure with no perceptible enhancement after injection of contrast is noted in upper pole of left kidney (59 mm× 50 mm), protruding into the renal sinus.B: Another cystic lesion with no soild component is detected in caudate lobe of liver (maximum size of 8 mm× 4 mm and a 35 mm × 20 mm) cystic lesion.
3.Discussion
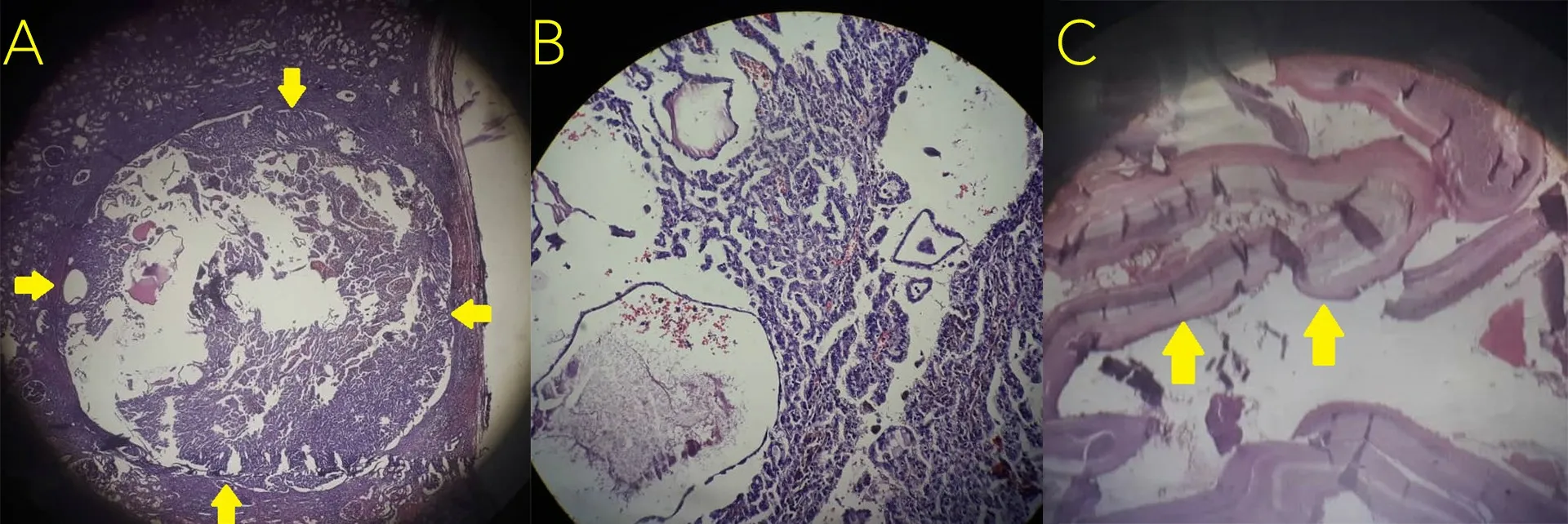
Figure 2.Microscopic features of renal cell carcinoma with H & E staining.A: a hydatid cyst in normal tissue of kidney.B: multifocal renal cell carcinoma in the same kidney.C: the wall of renal hydatid cyst.The magnifications of Figures are: A: 100×; B: 400×; C: 100×.
The life cycle of E.granulosus starts with ingestion of embryonated eggs of this small cestode.Contaminated hands, drinks, foods and other materials are the main containers of these eggs.Human becomes the intermediate host for Echinococcus.It affects people in adult or larval stage.The larvae are hatched and penetrate within the intestinal wall, then migrate to blood and lymphatic system and then transport to liver, lungs and rarely kidneys to become cystic echinococcosis.Cystic echinococcosis is endemic in Middle East countries especially in Iran.The prevalence of cystic echinococcosis is about 4% in the human population and is more common in the rural area in comparison to the urban ones.Women are more likely to be infected due to their higher exposure to contaminated containers[4,5].Kidney involvement is rare and seems to be less than 2% of all human cystic echinococcosis cases[6].This case was first diagnosed as RCC based on radiological reports.However,through histopathological examination, cystic echinococcosis was proved to be the main diagnosis and RCC came to the second line.This misdiagnosis is possible because the cystic echinococcosis may be mistaken for a cystic portion of RCC but co-existing of these two pathologies is extremely rare.As we searched, there were few reports of co-existing RCC and cystic echinococcosis, one of which was a case with cystic echinococcosis and adenocarcinoma in the same kidney[7], and another was a co-existence of cystic echinococcosis and sarcoma in one kidney[8].The other one was a report of RCC and renal cystic echinococcosis[2].There were also two cases with radiologic findings in favor of renal malignancies which were diagnosed with isolated renal cystic echinococcosis after histopathologic study on removed kidney[1,9].This article is probably the first report on renal cystic echinococcosis in association with papillary RCC in the same kidney.
Clinical approaches to urological findings are mostly based on radiologic examinations.But specificity and sensitivity of radiological findings are under question.According to WHO_IWGE classification[4], abdominal cystic echinococcosis are characterized in ultrasound by “double contrast sign” and “snow storm sign” in active stageⅠand by the presence of daughter cysts or “honeycomb pattern” in active stageⅡ.CECT is the gold standard imaging method in extrahepatic abdominal cystic echinococcosis but even CECT is not able to exact differentiation of cystic echinococcosis until terminal stages[4].As presented in this case, both radiological techniques including ultrasound and CECT revealed cystic lesions in the kidney suggestive for RCC, while in the histopathologic examination, as a gold standard diagnostic method, renal cystic echinococcosis in association with papillary RCC was diagnosed.The problem is doubled when, as we presented in this case, there are no specific clinical or laboratory findings to differentiate the diagnoses[1].
The treatment of renal cystic echinococcosis is both surgical and medical.PAIR (Percutaneous aspiration, infusion of scolicidal agents and reaspiration) is the first low invasive choice for treating non complicated cystic echinococcosis but partial and total nephrectomy are the most common surgical treatments of renal hydatid cyst especially in complicated forms.Medical treatment of cystic echinococcosis is predominantly based on long term administration of anthelmintic agents such as Albendazole (15 mg/kg daily in two divided doses) and Praziquantel (50 mg/kg daily), this medical treatment can be used alone or in combination with surgery or PAIR[4,10].
猜你喜欢
军事文摘(2022年16期)2022-08-24
小学阅读指南·低年级版(2021年5期)2021-05-28
军事文摘(2020年14期)2020-12-17
军事文摘(2020年18期)2020-10-27
小学生学习指导(低年级)(2018年9期)2018-09-26
少儿科学周刊·儿童版(2017年9期)2018-03-15
小学阅读指南·低年级版(2016年11期)2017-02-06
作文新天地(初中版)(2016年8期)2016-05-14
作文周刊(中考版)(2014年35期)2014-10-31
小朋友·聪明学堂(2009年7期)2009-07-31
 Asian Pacific Journal of Tropical Medicine2020年2期
Asian Pacific Journal of Tropical Medicine2020年2期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Dengue virus infections and anti-dengue virus activities of Andrographis paniculata
- Human leukocyte antigen class-Ⅱ DRB1 alleles and Giardia lamblia infection in children: A case-control study
- A PCR and RFLP-based molecular diagnostic algorithm for visceral leishmaniasis
- In vitro biological activities of aqueous extracts of Tetrapleura tetraptera (Schumach.& Thonn.) taub.and Aframomum citratum (C.Pereira) K.Schum from three Agroecologic Zones in Cameroon
- Predicting the number of visceral leishmaniasis cases in Kashgar, Xinjiang, China using the ARIMA-EGARCH model
- First evidence of Bartonella phoceensis and Candidatus Mycoplasma haemomuris subsp.ratti in synanthropic rodents in Malaysia