
Moving fast,thinking fast:The relations of physical activity levels and bouts to neuroelectric indices of inhibitory control in preadolescents
2019-10-16 02:35DominikPinusEriDrollttLurnRinShihChunKoNimnKhnDnilWstfllMorgnHmillShorinEmilyClorisiDinshJohn
Dominik M.Pinus*,Eri S.Drolltt,Lurn B.Rin,Shih-Chun Ko,Nimn KhnDnil R.Wstfll,Morgn Hmill,R Shorin,Emily Clorisi,Dinsh John,
Arthur F.Kramerc,Charles H.Hillmanc,f
a Department of Kinesiology and Community Health,University of Illinois at Urbana-Champaign,Urbana,IL 61801,USA b School of Health and Human Sciences,University of North Carolina Greensboro,Greensboro,NC 6170,USA
c Department of Psychology,Northeastern University,Boston,MA 02115,USA
d Department of Health and Kinesiology,Purdue University,West Lafayette,IN 47907,USA
e Department of Health Sciences,Northeastern University,Boston,MA 02115,USA
f Department of Physical Therapy,Movement,&Rehabilitation Sciences,Northeastern University,Boston,MA 02115,USA
Abstract Background:Structured vigorous physical activity(VPA)can improve cognitive control in children,but studies relating daily physical activity(PA)to cognitive control have yielded conflicting findings.While objectively measured daily PA summarizes all occurrences of PA within a registered period, a minimum duration of continuous PA is required for registration of a PA bout. Because brief bouts of high-intensity PA can account for a large proportion of children’s daily activity-related energy expenditure, this study assessed whether daily and bouted VPA were selectively related to cognitive control in preadolescents relative to other PA intensities.Methods:A total of 75 children between the ages of 8 and 10 years(49%girls)wore an ActiGraph wGT3X+on the hip for 7 days.The acceleration signal from the vertical axis was summarized over 1 s,5 s,and 15 s epochs.Daily and bouted moderate PA,moderate-to-vigorous PA,and VPA were measured. PA bouts were expressed as the frequency and time spent in 2 different continuous PA bouts, one lasting ≥10 s and the other lasting ≥30 s at a given intensity. Inhibitory control was assessed using behavioral responses to a modified flanker task (mean reaction time(RTmean)and accuracy).Attentional resource allocation and cognitive processing speed were measured using the amplitude and latency of the P3 component of event-related brain potentials, respectively. Associations between PA, behavioral indices of inhibitory control, P3 amplitude,and latency were assessed using hierarchical regression models.Results:Daily VPA was not related to RTmean or accuracy on either congruent or incongruent trials.In contrast,more time spent in VPA bouts lasting ≥30 s predicted shorter P3 latency across epochs and flanker congruencies(all β ≤-0.24,all p ≤0.04).The associations between shorter P3 latency and the time spent in moderate-to-vigorous PA bouts lasting ≥30 s were less consistent and largely limited to congruent trials(congruent:β(-0.31,-0.34)).No significant associations were observed upon correction for false discovery rate.Conclusion: The pattern of uncorrected associations aligns with the dose-response literature and suggests that brief VPA bouts may yield the greatest benefits to cognitive processing speed in preadolescents. Future studies using measures of brain structure and function are needed to understand the mechanisms linking bouted VPA to neurocognitive function during childhood.2095-2546/© 2019 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords: Accelerometry;Bouts;Children;ERPs;Inhibitory control;P3;Physical activity
1. Introduction
More than 80% of children and adolescents worldwide are physically inactive (i.e., engaging in <60 min of moderateto-vigorous physical activity(MVPA)daily).1Expanding evidence suggests physical inactivity contributes not only to epidemic levels of obesity,2but also to suboptimal brain development3,4and brain function in children.5Because neural plasticity increases in the developing brain during childhood,6it is an important period during which to promote long-term neurocognitive health. Given that the prefrontal cortex, which supports higher order cognition, is particularly responsive to experience7and exercise,8greater engagement in physical activity (PA) during childhood may help to optimize neurocognitive development.9,10
Structured and monitored sessions of MVPA during 3- to 9-month PA interventions promote improvements in cognitive control, namely, the cognitive functions that guide goaldirected behavior.5,10A 9-month PA intervention improved performance on inhibitory control(i.e., the ability to attend to relevant stimuli in the environment and withhold inappropriate responses)and mental flexibility(i.e., the ability to adapt performance to changing rule sets) in preadolescents.5Likewise,a 3-month intervention of structured vigorous PA (VPA)improved children’s performance on a planning task.10These intervention studies thus contribute to our understanding of how increased levels of structured PA relate to cognitive control in children. However, it is also important to understand the relationship between daily PA and cognitive control in the absence of an intervention because of the intermittency of children’s PA and low levels of MVPA in the general population of children.1,11
Observational studies complement experimental studies and can help to identify characteristics of children’s daily PA that may benefit neurocognitive function. However, cross-sectional research examining associations between objectively measured daily MVPA and cognitive control in children and adolescents has yielded equivocal findings. Specifically, positive,12-14null,13,15-18and negative17associations with cognitive control have been reported. One reason for these discrepant findings may be related to the fact that a minimum PA dose is potentially required for the cognitive benefits to emerge. In an attempt to confirm this finding, several studies observed dose-response effects of PA on neurocognitive functions in children.5,10In particular,when the effects of intensity were considered,only VPA was positively related to inhibitory control in preadolescents.19Whether similar relationships may be observed between daily VPA and neurocognitive function in preadolescents warrants further investigation.
Children’s daily PA patterns are spontaneous and intermittent.VPA is accrued in brief bouts of 3-5 s that are interspersed with light PA(LPA)and inactivity.20,21Because accelerometermeasured VPA in children decreases with increasing epoch length,22-26brief VPA bouts may go undetected when longer sampling windows are used.Specifically,3-5 s spikes of highintensity accelerometer signals that indicate such brief bouts of children’s VPA may be averaged with lower intensity accelerometer signals indicative of moderate PA(MPA),LPA and sedentary time.20,21In contrast with VPA, MVPA estimates generally increase with increasing epoch length.23,25,26To the best of our knowledge,only 1 study has investigated the effect of epoch length in relation to health outcomes in children,26and it reported a negligible effect of epoch length on the associations between VPA and aerobic fitness. However, the study only compared the effects of 15 s and 60 s epochs and did not include cognitive outcomes.
The relationship between PA and inhibitory control may also depend on the pattern in which VPA is accumulated. In preadolescents, high-intensity PA bouts lasting on average 25 s accounted for 40% of PA-related energy expenditure.27PA-related energy expenditure was positively related to greater volume within brain structures that subserve cognitive control (i.e., bilateral frontal, temporal, and parietal lobes) in adults.28Positive effects on inhibitory control were observed in preadolescents after a 6-week high-intensity interval training (HIIT) that employed 6-min sessions of high-intensity intervals lasting 20 s.The effects of HIIT on inhibitory control were comparable with the effects of a 9-month PA intervention incorporating ≥60 min of MVPA per session.5Thus, daily engagement in brief VPA bouts may be particularly relevant to children’s neurocognitive function due to their relationship with daily energy expenditure.27To the best of our knowledge,the relationships between bouted daily VPA and neurocognitive function in children have not been investigated.
Event-related brain potentials (ERPs) are used to complement the information available from behavioral measures of cognition and performance.ERPs are neuroelectric responses to an event that are associated with specific cognitive processes engaged between stimulus encoding and response execution.29,30The amplitude of the stimulus-locked P3 component of the ERPs is thought to represent attentional resource allocation during working memory updating,31whereas the latency of the P3 represents the processing speed of stimulus detection and evaluation.32,33In children,greater P3 amplitude is associated with better cognitive control34,35and higher academic achievement.29Higher aerobic fitness has been consistently related to greater P3 amplitude across the lifespan.5,30,36,37Likewise, engagement in a 9-month PA intervention resulted in increases in P3 amplitude and shorter P3 latency,which were specific to more cognitively demanding task conditions.5Studies in adults suggest that selfreported habitual PA is positively related to shorter P3 latency and larger P3 amplitudes.30,37However, the inferences drawn from these studies remain somewhat limited owing to a large bias of measurement inherent in PA estimates from questionnaires.38To the best of our knowledge,only 1 study inspected the relations between objectively measured PA and brain function in children, and it reported null findings.39Specifically,the patterns of activation within anterior prefrontal cortex, as well as middle frontal cortex (measured with near-infrared spectroscopy while children performed a cognitive control task), did not differ with the level of child’s MVPA. Of note, these brain regions are consistently activated when the demand for cognitive control increases.40However,the cut-points applied to define MVPA in the study were not validated for wrist-worn accelerometers,which precludes firm conclusions.
Consequently, the aim of the present study was to address this gap in the literature and to inspect the relations of accelerometer-measured daily VPA and VPA bouts to behavioral and neuroelectric indices of inhibitory control.Given that previous literature suggests the importance of VPA to daily energy expenditure,27inhibitory control,19and more optimal behavioral and neuroelectric profiles among young adults,30,37we hypothesized that children who engage in more daily VPA would demonstrate improved behavioral responses (i.e.,shorter reaction time (RT) and higher accuracy on a flanker task)and neuroelectric responses(i.e.,larger P3 amplitude and shorter P3 latency) indicative of more optimal inhibitory control. For comparison, the associations with MVPA and MPA were also explored. Second, given the high contribution of brief 25 s bouts of VPA to children’s PA-related energy expenditure27and the effects of the HIIT intervention41on inhibitory control,we hypothesized that a greater frequency of and a longer time accumulated in VPA bouts lasting ≥30 s would be positively related to behavioral and neuroelectric indices of inhibitory control.We further hypothesized that these relationships would be stronger for the incongruent task condition,which requires greater inhibitory control.5,30,37Finally,because accelerometer-measured VPA estimates increase with decreasing epoch length,22-26we hypothesized that the relationships between daily and bouted VPA with behavioral and neuroelectric indices of inhibitory control would be stronger in 1 s and 5 s epoch analyses compared with 15 s epoch analyses.
2. Methods
2.1. Study design
Cross-sectional data collected at baseline as a part of the Fitness Improves Thinking in Kids 2 trial (FITKids2; ClinicalTrials.gov: NCT01619826) were included in the study.Briefly, FITKids2 is a randomized, controlled trial designed to test the effects of an aerobic exercise intervention on neurocognitive outcomes in typically developing 8- to 10-year-old children.42The present study used baseline data from a subsample of 106 children who wore an accelerometer between June and September 2013 and June and September 2014.
2.2. Participants
To qualify for the FITKids2 study, children had to be free of (1) neurologic disorders, (2) physical disabilities, and (3) a clinical diagnosis of attention deficit hyperactivity disorder(ADHD; based on parental disclosure). Participants included in the analyses had (1) an intelligence quotient (IQ) score of ≥8543and (2) ≥3 valid days of accelerometer wear (i.e.,≥8 h of valid wear time per day).44-46One child with an IQ of 84 (i.e., 1 point below 1 standard deviation (SD) from the mean) was not a statistical outlier on cognitive measures and was retained in the analyses. After exclusions based on missing neurophysiological data (n=4), insufficient accelerometer wear (n =7), low performance on an inhibitory control task (accuracy of <50%,n =10), missing data on the cognitive task (n =2), and <20 acceptable trials per condition after ERP reduction (n =8), 75 children (mean age,8.7 ± 0.6 years; 49% girls) were included in the analyses.The study was approved by the Institutional Review Board of the University of Illinois at Urbana—Champaign. Parents provided written informed consent and children provided written assent.
2.3. Study procedure
Participants completed a 2-to 3-h testing session in the laboratory on 2 occasions separated by ≥7 days.At the beginning of the first visit,a research assistant explained the experimental procedures to a legal guardian and a child, after which a legal guardian and a child signed informed consent and a written assent,respectively.Next,demographic information and a health history were collected. During the same visit, children completed an intelligence test,anthropometric and aerobic fitness assessments, and were sent home wearing a hip-worn accelerometer(as described in Section 2.4).During the second visit, electroencephalographic (EEG) recordings were made while children completed a modified flanker task in a soundattenuated testing chamber. Children were remunerated at the rate of USD10/h for their participation.
2.4. Accelerometer data processing and PA variables
Participants wore a triaxial wGT3X+ accelerometer (Acti-Graph LLC., Pensacola, FL, USA) on the waist at the right anterior axillary line on an elastic belt for 7 consecutive days.The wGT3X+ used in this study (4.6 cm×3.3 cm×1.5 cm;19 g) had a dynamic range of ±6 g and was initialized to record acceleration at 100 Hz. Children wore the accelerometer during waking hours except during water-based activities.Nonwear time, which was excluded from the analyses, was defined as 60 consecutive min of 0 count, allowing for 2 min of nonzero interruptions.11Although at least 3 valid days of accelerometer wear were adopted as an inclusion criterion,all children except for one(who provided 3 days of wear)contributed ≥4 valid days of wear time,which yielded intraclass reliability coefficients of 0.80 to estimate habitual MVPA in children of a similar age.47
Acceleration data were converted into vertical axis counts over 1 s,5 s,and 15 s epochs using ActiLife software Version 6.13.3 (ActiGraph LLC). The rationale for exploring the impact of the selected epoch lengths on cognitive outcomes are as follows (i) 15 s: used to develop the Evenson intensity cut-points48commonly used in childhood cognitive research;14,15,49(ii) 5 s: compared with longer epochs, a 5 s epoch minimizes root mean square errors in MVPA estimates among children;25and(iii)1 s:this is the shortest possible duration, which may minimize potential misclassification of those motion signals that lie just above the VPA cut-point owing to averaging of the signal over a longer epoch.24
ActiLife software (ActiGraph LLC) was used to calculate time spent in PA intensities (min/day); VPA, MPA, and MVPA were defined using Evenson cut-points (see Supplemental Table 1 for epoch-adjusted thresholds). We also computed the frequency and time spent in PA bouts per day.Bouts were classified as engaging in continuous durations of ≥10 s and ≥30 s in a single PA intensity.We used 10 s to indicate a shorter bout because the majority of children’s VPA and MVPA is accumulated in bouts of <10 s.20,21We defined longer bouts as lasting ≥30 s(i)based on the length of high-intensity PA bouts contributing 40% to activity-related energy expenditure in children(i.e.,25 s),27(ii)based on the duration of a high-intensity PA intervals applied in HIIT,41and (iii) to ensure comparability across epoch lengths.
2.5. Inhibitory control
A modified Eriksen flanker task,50which measures the ability to suppress distractors and attend to relevant information in the environment,was used to measure inhibitory control. Stimuli were presented on a computer screen, from a distance of approximately 1 m, using Neuroscan STIM software (Compumedics NeuroScan, Charlotte, NC, USA). Participants were instructed to respond with a thumb press on a response pad (Current Designs Inc., Philadelphia, PA, USA)to indicate the direction of the centrally presented target stimulus (a 3-cm tall gold fish presented against a blue background),amid 4 identical flanking stimuli,which faced either the same direction (e.g.,or; congruent trials) or the opposite direction (e.g.,or; incongruent trials) as the target. Incongruent trials create perceptual and response conflict, which leads to decreased accuracy and a longer RT. Prior to and following testing blocks, each participant was provided with instructions and encouragement emphasizing accuracy (i.e., “It is important that you respond as accurately as possible”), with secondary instructions encouraging response speed to maintain responding within the allotted response window (i.e.,“but we also want you to respond quickly, so please make sure you respond before the next set of fish appears on the screen”). Participants first completed 40 practice trials. If they were accurate on ≥70% of the trials, they proceeded to experimental blocks. Participants completed 2 blocks of 84 trials,presented randomly with equiprobable congruency and directionality for 200 ms with a randomly varied intertrial interval of 1600 ms, 1800 ms, and 2000 ms. Outcome measures included accuracy and mean RT (RTmean) on congruent and incongruent trials.
2.6. EEG
EEG activity was recorded using a 64-channel Neuroscan Quik-Cap (Compumedics Inc., Charlotte, NC, USA) with Ag/AgCl-sintered electrodes arranged in an extended montage according to the International 10-10 system.51All electrodes maintained pre-recording impedances of <10 kΩ.Online continuous recordings were referenced to a midline centrocentro-parietal electrode,52with a midline anterofrontal electrode serving as the ground electrode. Electro-oculorographic activity was monitored with electrodes placed above and below the left orbit and the outer canthus of each eye;separate bipolar recordings were used to monitor vertical electrooculorographic and horizontal electro-oculorographic activity.Continuous online data were digitized at a sampling rate of 500 Hz, amplified 500 times with a direct current to 70-Hz filter,53and a 60-Hz notch filter was applied using a Neuroscan SynAmps2 amplifier (Compumedics Inc.). Data were processed offline using MATLAB (R2012b), EEGLAB,54and ERPLAB55toolbox plug-ins. EEG data were referenced to average mastoids (M1, M2). Eyeblinks were identified using independent component analyses (ICA) and rejected using an autocorrelation procedure (i.e., EEG.icaact matrix generated by the ICA).56A maximum of 2 ICA components with a correlation coefficient of >0.30 were removed. Stimulus-locked epochs were created for correct trials (-100 to 1000 ms relative to stimulus onset), baseline-corrected to the prestimulus period, and filtered using a zero-phase shift low-pass filter at 30 Hz(24 dB/octave).Artifacts were identified and rejected if a moving window peak-to-peak amplitude exceeded 100 μV(100-ms window width and a 50-ms window step) and if the overall variance of the epoch exceeded±3 SD of the mean of local (by electrode site) and global (all electrode sites)accepted epochs.56Artifact-free trials associated with correct responses were then averaged. Participants with <20 valid congruent or incongruent trials were excluded. The average number of trials was 54.2 ± 10.7 (mean ± SD) on congruent trials and 47.7 ±10.7 (mean ± SD) on incongruent trials.The P3 component was evaluated as the mean amplitude within a 50-ms interval surrounding the largest positivegoing peak within a 300- to 600-ms latency window.57Peak latency was defined as the time point corresponding with the maximum amplitude. Averaged values across the midline electrodes (i.e., frontal, frontocentral, central (Cz), centroparietal (CPz), parietal (Pz), and parieto-occipital (POz),where z (for zero) indicates a midline location58) for P3 amplitude and latency on congruent and incongruent trials were used as outcomes.
2.7. Covariates
2.7.1. Aerobic fitness percentile
Peak oxygen consumption (VO2peak) was measured during a modified Balke protocol59using a computerized indirect calorimetry system (TrueMax 2400; Parvo Medics, Sandy, UT,USA).VO2peakpercentiles were computed based on published norms.60
2.7.2. Body mass index(BMI)percentile
Standing height was measured with a Seca telescopic stadiometer model 220(Seca,Birmingham,UK)to the nearest millimeter, and weight was assessed with a Seca 769 electronic column scale (Seca) while children were in lightweight clothing and shoes. BMI percentiles were computed using Centers for Disease Control and Prevention growth charts.61
2.7.3. IQ
IQ was assessed using the Woodcock-Johnson III Test of Cognitive Abilities43using a standardized score with 100 ±15 points as the mean±SD.
2.7.4. Socioeconomic status(SES)
SES was calculated using a trichotomous index based on parental reports of(1)children’s use of a free or reduced price meal program at school, (2) the highest level of education obtained by the mother and father, and (3) the number of parents working full time.62
2.7.5. Pubertal status
Parents (or legal guardians) provided ratings on a pubertal assessment questionnaire,63a pictorial scale based on criteria specified by Tanner.64Parents rated gender specific-line drawings of breast and pubic hair development for girls or penis and scrotum,as well as pubic hair,development for boys on a 5-point scale with 1 indicating a prepubertal state and 5 indicating the full mature state.63Parental ratings on this scale have acceptable validity in differentiating between prepubertal and pubertal status.65
2.7.6. ADHD
Parents (or legal guardians) completed the ADHD Rating Scale IV.66The Scale is an 18-item checklist of behaviors related to child’s attention and hyperactivity over the last 6 months. Parents rated each behavior on a 4-point Likert scale ranging from 1 (never or rarely) to 4 (very often). The scale contains 2 subscales:hyperactivity and inattention.A composite percentile score across both subscales67was used in the current study and percentiles were based on published norms.67The scale has excellent 4-week test-retest reliability(r=0.92) and good concurrent validity (allr=0.60 and 0.80 assessed against the cognitive and hyperactivity-impulsivity scales, respectively, of Conners Parent Rating Scale Revised).68-70
2.8. Statistical analysis
Three participants (4% of the sample) had missing data on≥1 of the covariates (4 missing values in total: VO2peakpercentile,n=1;BMI percentile,n=1;pubertal stage,n=1;and ADHD percentile,n=1). The data for these participants were imputed as the mean of the sample.Sex differences in the outcomes and PA variables were assessed with analyses of covariance with accelerometer wear time as a covariate. Withinsubject differences in PA variables by epoch length were examined using repeated measures analyses of variance.Where the assumption of sphericity was violated,Greenhouse-Geisser correction was used. Next, bivariate Pearson moment correlation coefficients were computed between demographic variables (i.e., age, sex, and SES), IQ, ADHD percentile, and pubertal status, considered as independent variables, and behavioral (i.e., accuracy and RT on congruent and incongruent trials) and neuroelectric dependent variables (i.e., the amplitude and the latency of the P3 on congruent and incongruent trials).Independent variables which were significantly associated with a specific neurocognitive variable, were then entered as nuisance variables in subsequent regression models.For example,if age was significantly related to P3 latency but not accuracy on congruent trials, it was only entered in the regression models predicting congruent P3 latency.Three-step multiple hierarchical regression models were conducted for each behavioral and neuroelectric dependent variable to assess its relationship with every PA predictor (i.e., daily MPA,VPA,and MVPA(min/day),as well as the frequency and time spent in PA bouts at each intensity). The rationale for using hierarchical regression models was to assess how much variance in neurocognitive outcomes was explained uniquely by objectively measured PA over and above the contribution of(i)factors related to neurocognitive performance in the literature (e.g., age,71sex,72,73IQ,74-76SES,77BMI,78and pubertal status79) and significantly associated with neurocognitive variables in our sample,and(ii)the unique contribution of aerobic fitness because of its established relationship with the P3 ERP component and inhibitory control in preadolescents.36Consequently,accelerometer wear time and covariates significantly related to a given outcome were entered in Step 1,VO2peakpercentile was entered in Step 2,and the PA variable was entered in Step 3. Five models per PA intensity for each outcome within each epoch length were conducted, including the following: 1 model for daily PA (min/day) and 2 models for every PA bout definition (≥10 s and 30 s, accounting for frequency and time in the bouts).All models were assessed for normality of distribution of error terms, univariate and multivariate outliers (Mahalanobis distance), and influential cases using Cook’s distance. Cases with standardized regression residuals of ≥|3| and Cook’s distance of ≥1 were excluded from the models. Cases with Mahalanobis distance of >15 across several models within each intensity were also excluded.Based on these criteria,a maximum of 4 cases were excluded from the analyses. The RTmeanwas log-transformed using a base 10 logarithm to conform to the normality of distribution of error terms.Data were analyzed using the SPSS Version 24.0(IBM Corp.,Armonk,NY,USA).An α level of 0.05 was used to indicate statistical significance.To control for the type I error due to multiple comparisons, the Benjamini and Hochberg80false discovery rate(FDR)procedure was applied within each cognitive variable (n=37). The unadjustedpvalues were ordered from the smallest to the largest.If the unadjustedpvalue for thek-thtest was less than 0.05×k/n, the test was statistically significant.We report unadjustedpvalues for all tests as well as the statistical significance after adjustments for FDR.
3. Results
3.1. Participants
Sample characteristics are presented in Table 1. Participants included in the study did not differ from those excluded from the analyses in VO2peakrelative,BMI,or the distribution of sex, SES, overweight, and obesity status. No differences between those included and excluded from the analyses were observed in VPA. Those excluded from the analyses had higher MPA using 1 s and 5 s epochs (△M=4.21 min and 5.27 min,allp≥0.04).As expected based on the inclusion criterion of ≥50% accuracy, participants included in the study had higher accuracy on congruent (△M=17.5%,p<0.001)and incongruent trials (△M=17.2%,p< 0.001). Those included in the study had longer RTmean(△M=67.7 ms,p=0.01) but shorter P3 latency on the incongruent trials(△M=43.5 ms,p=0.008). No further differences between study participants and those excluded from the analyses were noted.
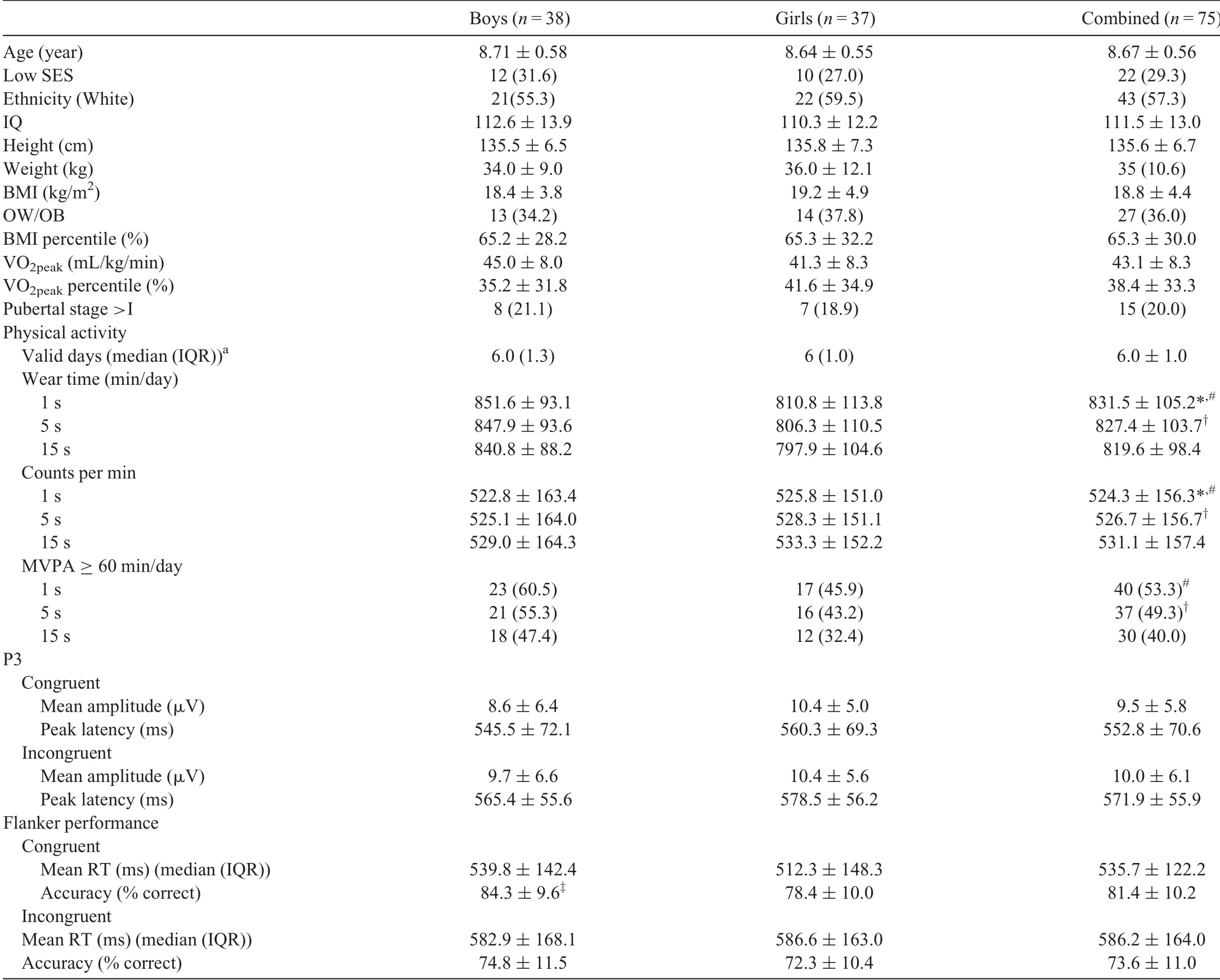
Table 1 Demographic and descriptive sample characteristics.
Within the study sample, compared with girls, boys were more accurate on congruent trials (△M=5.93%,p =0.01).Thus,sex was used as a covariate in models predicting congruent accuracy from PA variables.
3.2. Effects of epoch length on PA
Estimates of minutes spent in daily and bouted PA by intensity and epoch length are presented in Supplemental Table 2. Daily VPA and MVPA decreased with increasing epoch length, with concurrent increases in daily MPA,F(2,148) ≥80.7 (allp<0.001). The largest effect of epoch length was observed for VPA (η2p=0.91; 90% confidence interval (CI):0.89-0.93) compared with MVPA (η2p=0.58, 90%CI:0.50-0.64) and MPA (η2p=0.52, 90%CI:0.43-0.59). All but 1 pairwise comparison between epochs were statistically significant(allp≤0.001).Specifically,a trend was observed for the difference in MVPA estimates comparing 1 s and 5 s epochs(p=0.07). VPA estimates (min/day) decreased with increasing epoch length by 21% and 53% using 5 s and 15 s epochs compared with a 1 s epoch,respectively.Likewise,there was a significant effect of epoch length on the frequency and time spent in PA bouts across intensities,bouts ≥10 s,F(1,74)≥312.3(allp≤0.001)and bouts ≥30 s,F(2,148)≥332.0(p<0.001).The total number of bouts and the time spent in MPA, VPA, and MVPA bouts increased with increasing epoch length.
3.3. Associations between PA and aerobic fitness within epochs
Across epoch lengths, VPA correlated strongly with MPA(Supplemental Table 3). All PA intensities were significantly and positively related to VO2peakpercentile.
3.4. Associations between daily and bouted PA
Within each intensity and across all epochs,the strength of the associations between bouted and daily PA decreased with increasing bout duration(Supplemental Table 4).
3.5. Associations among P3,behavioral outcomes,and demographic covariates
P3 amplitude and RTmean, on congruent trials decreased with age (all r ≤-0.23, all p ≤0.049). P3 latency on incongruent trials decreased with age (r=-0.23, p=0.047), and a trend for shorter P3 latency was observed with higher IQ(r=-0.23, p=0.051). The RTmeanincreased with BMI percentile across congruency(all r ≤-0.26,all p ≤0.02).
3.6. Relations between PA and performance on the flanker task
3.6.1. RTmean
Daily and bouted MPA,VPA,and MVPA were not related to the RTmeanacross congruencies and epochs (all p ≥0.11;uncorrected for FDR).
3.6.2. Accuracy
Supplemental Tables 5 and 6 summarize the last steps of the regression models for accuracy. Before corrections for FDR, daily MPA was negatively associated with congruent accuracy using 5 s and 15 s epochs(all p ≤0.046,Supplemental Table 5). Sporadic negative associations were observed between the frequency and time spent in MPA and MVPA bouts lasting ≥30 s in the 15 s epoch analyses(all p ≤0.047).No other PA variable was related to accuracy(p ≥0.05). Once adjusted for FDR, the associations were attenuated to nonsignificance(p=0.21).
3.6.3. Summary of behavioral findings
Before FDR correction,daily MPA predicted lower congruent accuracy,while daily MVPA predicted poorer incongruent accuracy in 5 s and 15 s epochs. Sporadic associations also emerged between engagement in MPA and MVPA bouts lasting ≥30 s and poorer accuracy across congruencies, which were limited to a 15 s epoch. Once adjusted for FDR, null associations were observed. Daily or bouted VPA was not related to behavioral indices of cognitive control (data not shown).
3.7. Relations of daily and bouted PA to P3 amplitude
Daily and bouted PA across intensities was not related to P3 amplitude(data not shown).
3.8. Relations of daily and bouted PA to P3 latency
Tables 2 and 3 summarize the results of the last steps of the regression models predicting P3 latency from PA variables.
3.8.1. MPA
None of the MPA variables were related to P3 latency (all p ≥0.10;uncorrected).
3.8.2. VPA
Before correction for FDR,daily VPA was not related to P3 latency (all p ≥0.08). In contrast, time spent in bouted VPA predicted shorter P3 latency across epochs and congruencies.Fig.1 illustrates these associations for VPA bouts lasting ≥30 s.The time spent in VPA bouts lasting ≥30 s was associated with shorter congruent P3 latency across epochs, 1 s epoch: F(4,69)=3.00(p <0.05);and 5 s and 15 s epochs:F(4,68)≥2.97 (p ≤0.03). In the incongruent trials, these associations were statistically significant in 5 s and 15 s epoch analyses, F(6,66)≥3.33(p <0.006),and trending in the same direction using a 1 s epoch. The time spent in VPA bouts explained 6%-9%of variance in P3 latency.The strength of these associations was comparable across congruencies and epochs(congruent, β (-0.28, -0.33); incongruent, β (-0.24, -0.29)).Supporting these findings, the frequency of longer VPA bouts lasting ≥30 s predicted shorter incongruent P3 latency using 1 s and 5 s epochs β (-0.28, -0.32); 1 s epoch, F(6, 67)=4.59(all p ≤0.003); 5 s epoch, F(6, 66)=3.65 (p=0.003), and explained 7%-8% of the variance in P3 latency. In contrast,the relationship between the frequency and time spent in shorter VPA bouts lasting ≥10 s and P3 latency, across congruencies, was limited to a 1 s epoch, congruent, F(4, 69) ≥2.58(all p ≤0.045);incongruent,F(6,67)=3.96(p ≤0.002).These associations did not survive correction for FDR (all p for F tests ≥0.27). Among covariates, increasing age predicted shorter congruent P3 latency across epochs: 1 s epoch,F(4,69)≥2.58(all p ≤0.02);5 s and 15 s epochs,F(4,68)≥2.97 (p ≤0.04). A higher IQ predicted shorter P3 latency on incongruent trials across epochs:1 s epoch,F(6,67)≥3.96(p <0.06); 5 s and 15 s epochs, F(6,66) ≥3.00 (p ≤0.005).Pubertal stage was negatively related to incongruent P3 latency in 1 s and 5 s epochs:1 s epoch,F(6,67)≥3.96(p ≤0.03); 15 s epoch, F(6, 66) ≥3.00 (p <0.05). The VO2peakpercentile was not related to P3 latency(all p ≥0.67).
3.8.3. MVPA
Before correction for FDR,daily MVPA was not related to P3 latency (all p ≥0.39). In contrast, bouted MVPA was related to shorter P3 latency, primarily on congruent trials.Only the association between increasing time spent in MVPA bouts lasting ≥30 s and shorter congruent P3 latency was significant across shorter epochs, namely: 1 s and 5 s epochs,F(4,69)≤2.81(p ≤0.03).Associations between the frequency and time spent in MVPA bouts and incongruent P3 latency were limited to the time spent in longer bouts lasting ≥30 s and a single epoch: 5 s epoch, β=-0.23, F(6, 66)=3.24,p=0.01. The strength of these associations was comparableacross epochs: congruent: β (-0.31, -0.34); incongruent: β(-0.23, -0.24). These associations were reduced to nonsignificance upon FDR correction (all p for F tests ≥0.27). Among covariates, only IQ predicted shorter P3 latency on incongruent trials across 1s and 15 s epochs: 1 s epoch, F(6, 68)=4.06 (all p ≤0.006);5 s epoch,F(6,66)=3.24(p ≤0.006).VO2peakpercentile was not associated with P3 latency across all models(all p ≥0.63).
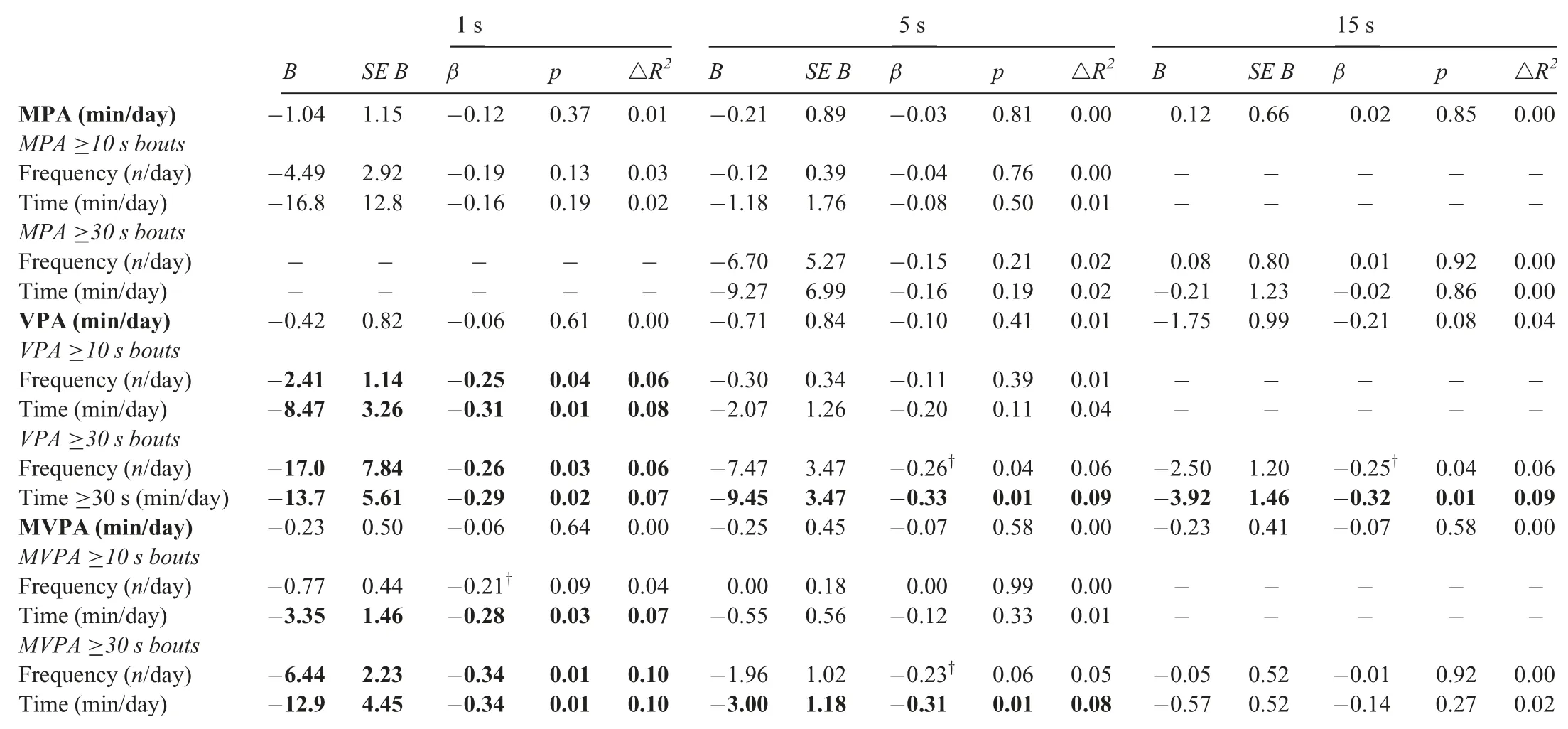
Table 2 Summary of the final steps of the hierarchical regression models predicting peak latency of the P3 component on congruent trials from PA variables adjusting for demographic covariates and VO2peak percentile by epoch length(1 s,5 s,and 15 s).
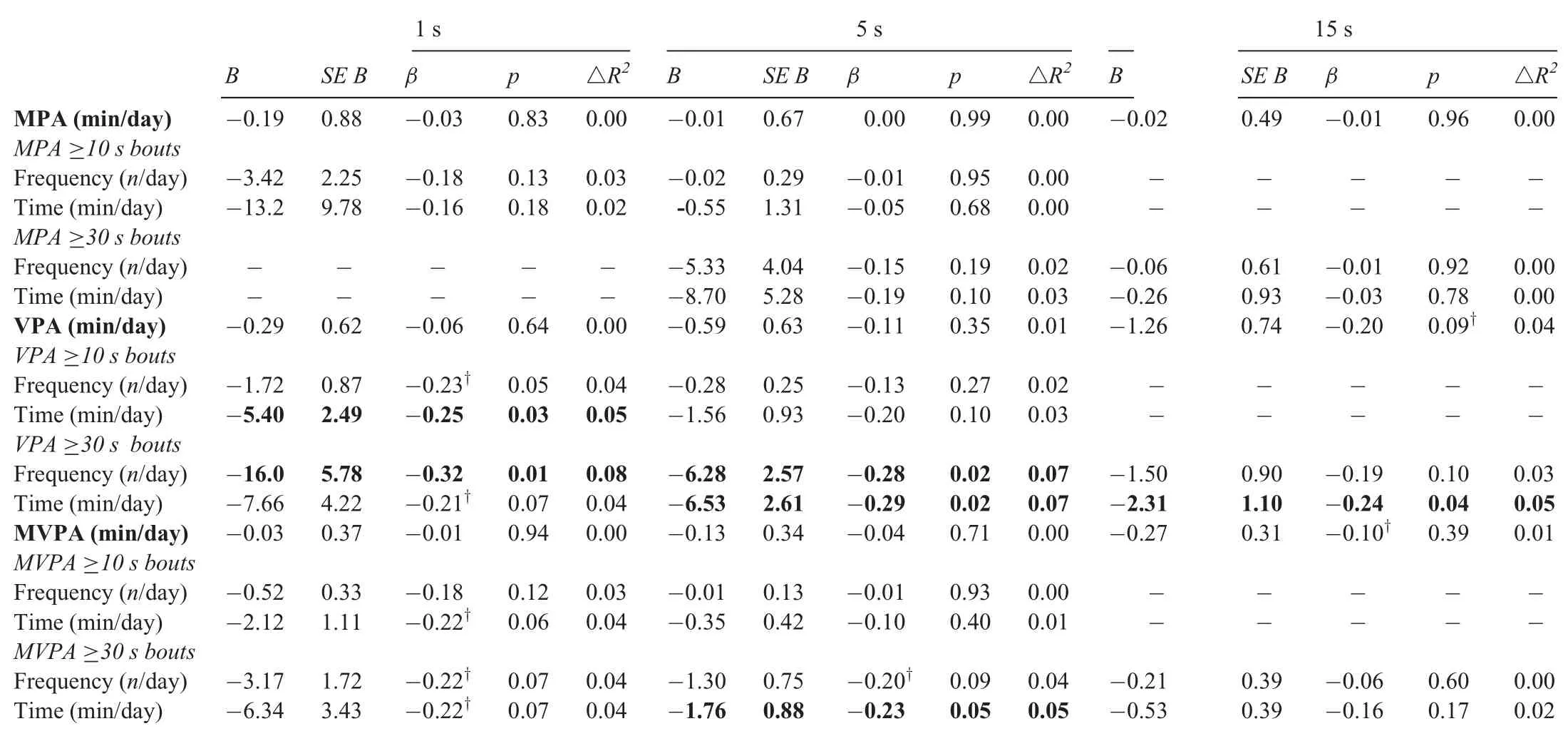
Table 3 Summary of the final steps of the hierarchical regression models predicting peak latency of the P3 component on incongruent trials from PA variables by epoch length(1 s,5 s,and 15 s).
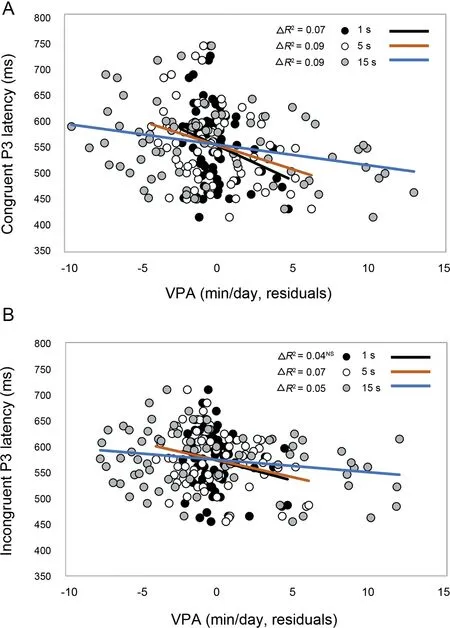
Fig. 1. The relations of the time spent in bouts of VPA lasting ≥30 s to P3 latency on congruent (A) and incongruent (B) trials across epochs. The X axis presents regression residuals where time spent in VPA bouts was regressed on age, accelerometer wear time, and VO2peak percentile (A), and age, IQ, pubertal stage,accelerometer wear time,and VO2peak percentile(B).IQ=intelligence quotient;VO2peak=peak oxygen uptake;VPA=vigorous physical activity.
3.8.4. Summary of P3 findings
Daily and bouted MPA,VPA,and MVPA were not related to P3 amplitude in uncorrected analyses. Likewise, daily MPA, VPA, and MVPA were not associated with P3 latency.In contrast, the time spent in VPA bouts lasting ≥30 s predicted shorter P3 latency before correction for FDR. These associations were largely consistent across congruencies and epochs. Supporting these findings, greater frequency of VPA bouts lasting ≥30 s predicted shorter incongruent P3 latency using shorter epochs(1 s and 5 s).The strength of these associations was comparable across congruencies and epochs. The associations between bouted MVPA and P3 latency were less consistent,were largely limited to congruent trials,and did not generalize across all epochs. The results of the uncorrected analyses suggest that VPA accumulated in longer bouts was the best predictor of shorter P3 latency across congruencies.No significant associations emerged in the corrected analyses.
4. Discussion
4.1. Associations between daily VPA and MVPA and cognitive control
Contrary to our hypothesis, we observed no significant associations between daily VPA with either behavioral or neuroelectric indices of cognitive control across uncorrected and corrected analyses. Likewise, daily MVPA was generally not related to cognitive control. Previous studies on objectively measured daily PA and cognitive control focused primarily on MVPA and reported mixed findings.12-18,81When it was included in the analyses, daily VPA was not related to selective attention14or impulse control17in adolescents. However,the differences in the age of the samples at the time of cognitive assessment,14,17study design,17and cognitive measures17preclude meaningful comparisons between our study and these previous studies.For example, in our study we included preadolescents whose inhibitory control is still dynamically developing; while smaller gains in inhibitory control have been observed in adolescents.71In contrast, Booth et al.12and van der Niet et al.13found that daily MVPA was positively associated with selective attention,12cognitive flexibility,12and planning13in children of similar age to the participants in our study. The reasons for the discrepancy in our findings and the findings of these previous studies may be related to differences in cognitive measures. The cognitive flexibility and planning tasks used by Booth et al.12and van der Niet et al.13would require greater upregulation of cognitive control because these tasks necessitate the integration of inhibition and working memory.Conversely,when inhibitory control was specifically considered, null associations were observed across several measures, including a flanker task,15,81Stroop task,13Go/NoGo,81and the Stop Signal Task.16Thus, our null results in relation to behavioral measures of inhibitory control align with these previous findings. It is possible that tasks that require the integration of cognitive control functions are especially sensitive to differences in daily MVPA and VPA,whereas those assessing solely inhibitory control are less sensitive. Future studies using accelerometry and tasks that require a progressive upregulation of cognitive control are needed to test this hypothesis.
Furthermore,we found no associations between daily VPA,greater attention allocation (greater amplitude of the P3), and faster cognitive processing (shorter latency of the P3 component).82These findings were surprising, because Hillman et al.30and Kamijo and Takeda37reported positive relationships between habitual PA and P3 amplitude in adults.30,37Compared with inactive adults, physically active adults maintained greater P3 amplitudes across conditions of the switch task, which varied in cognitive demands.30Likewise, Kamijo and Takeda37observed a decreased P3 amplitude with increasing task demands among inactive young adults,whereas active adults maintained similar levels of attentional resource allocation across task conditions. The effects measured in these studies may reflect differences in aerobic fitness because both Hillman et al.30and Kamijo and Takeda37purposefully recruited adults to polarized groups based on habitual engagement in aerobic exercise. In contrast, we included participants across the PA continuum. Thus, our measure of PA reflects individual differences in both incidental and structured daily VPA and MVPA.It is also possible that a task that challenges cognitive control to a greater extent than the congruency manipulation in the flanker task is needed for these associations to emerge.83Additional studies using improved accelerometry methodologies and cognitive tasks that flexibly modulate cognitive control are needed to test this hypothesis.
4.2. Associations between moderate daily PA and cognitive control
We found that greater engagement in daily MPA was related to poorer response accuracy on congruent trials in uncorrected analyses. Two previous studies assessed daily MPA in relation to inhibitory control and reported both negative17and positive associations.14However, due to the differences in cognitive measures14,17and accelerometer cut-points,14our studies are not directly comparable. There is a possibility that our MPA findings are spurious because the associations were limited to congruent trials, did not generalize across all epochs, and were not significant after FDR corrections.
4.3. Associations between bouted VPA,MVPA,and cognitive control
The hypothesis that brief VPA bouts would be positively related to increased cognitive control was confirmed in the uncorrected analyses, although it did not survive adjustments for multiple comparisons. The pattern of these associations,which is consistent across epoch lengths and aligns with the literature on the dose response,10,19raises a possibility that the null findings in corrected analyses may be related to the limited power of the study to detect small effects.Thus,we discuss the results of the uncorrected analyses in the light of previous literature,while recognizing the need for cautious interpretation and replication in future studies. We observed shorter P3 latencies with increased time spent in longer VPA bouts, lasting ≥30 s,on incongruent trials.We also observed positive associations of the time spent in VPA bouts lasting ≥30 s and shorter P3 latency on congruent trials. These associations were largely consistent across epochs.As predicted,these relationships were selective to longer VPA bouts as associations with shorter bouts,lasting ≥10 s,were limited to 1 s epoch analyses.The pattern of our results in the uncorrected analyses suggests that these associations were dose dependent in terms of increasing intensity;less consistent associations across epochs emerged for bouted MVPA, whereas MPA bouts were not related to P3 latency.Contrary to our hypothesis, we observed generalized associations between bouted VPA with P3 latency across congruencies.A similar pattern of results emerged for MVPA;however,these associations were less consistent across epoch lengths and congruencies.
Our exploratory findings suggest that the relationship between PA and the P3 in children may be specific to bouted PA,dose dependent,and selective to cognitive processing.Previous studies in adults and children reported a positive relationship between habitual PA status and participation in a 9-month PA intervention on both P3 amplitude5,30,37and latency.5,30In relation to P3 latency, these previous effects were specific to task conditions that upregulated cognitive control(e.g.,the heterogenous trials of the switch task30or incongruent trials on the flanker task5).The main difference between our study and these previous studies is the measured PA construct. While we captured the occurrences of brief VPA bouts with accelerometry,previous studies either measured the differences in aerobic exercise30,37or introduced structured MVPA of sufficient dose to increase aerobic fitness.5The reported effects of aerobic exercise and structured MVPA on P3 amplitude and latency in these studies may be mediated by changes in neural networks that support cognitive control,5,9,42,84as well as by exercise-induced increases in neurotrophic factors.85,86Higher levels of brief VPA bouts may promote greater cognitive efficiency through similar mechanisms. The differences in the observed associations between our study and previous work may, therefore, be the function of greater PA dose because previous studies used a predefined PA threshold as a recruitment criterion30,37or introduced a set dose of PA during a PA intervention.5In the study by Hillman et al.,30active adults spent more than 5 h/week in aerobic exercise, compared with inactive adults who exercised less than 1 h/week. The 9-month PA intervention introduced≥70 min of structured MVPA to children’s daily schedules on most days of the week.5In contrast,in our sample 51%of children did not achieve ≥60 min of intermittent MVPA on an average measurement day. Importantly, higher attendance at the intervention sessions was related to greater neurofunctional improvements, including a greater increase in attention allocation and faster cognitive processing.5This finding supports our interpretation that differences in results may be related to differences in measured PA dose. To our knowledge, this is the first report relating daily patterns of PA to neuroelectric indices of cognitive control in typically developing children. As noted,these exploratory findings require cautious interpretation and replication in future studies. Thus, more studies are needed to further characterize the neurophysiological benefits of brief VPA bouts during childhood and the underlying physiological mechanisms.
4.4. The effect of epoch length on the associations between VPA and cognitive control
Longer epoch lengths have been shown to underestimate VPA volume in children22-26because children accumulate VPA in brief bouts lasting on average 3-5 s.20,21Thus, in a longer epoch (e.g., 15 s), brief segments of high-intensity accelerometer signal indicative of VPA become averaged with proportionally larger segments of lower intensity signal associated with low-intensity physical behaviors (sedentary time,light PA,and MPA). To date,studies of objectively measured PA and cognition in children have used a range of epochs(i.e.,10 s,13,1815 s,14,15,49and 60 s12). Because a 15 s epoch was most common,we chose this duration as the basis for comparisons with shorter epochs identified as more suitable to capture brief VPA bouts in children.20,25Consequently, we hypothesized that stronger relationships would emerge between daily and bouted VPA and neurocognitive outcomes for shorter epochs due to the improved capture of VPA and resulting in greater VPA volume. However, we found consistent associations across epoch lengths in the uncorrected analyses,particularly for the longer VPA bouts lasting ≥30 s. The time accumulated in such VPA bouts predicted faster cognitive processing across congruent and incongruent trials and epochs.There were no meaningful differences in the strength of the associations across epochs. Specifically, we observed no evidence of an increase in standardized betas(suggesting a weakening of the associations) with increasing epoch length. As such, our findings align with those by Nettlefold et al.,26who reported that associations between daily PA, BMI, or aerobic fitness were of similar magnitude using either 15 s or 60 s epochs. Consequently, our results suggest that epoch length does not affect the interpretation of PA associations with health outcomes. Therefore, the results of studies using comparable data-reduction criteria and analytical methods but different epochs can be compared. However, if the patterns in which children accumulate daily PA is of interest, we would suggest the use of a 5 s epoch because it suffices to capture the intermittency of children’s PA and minimizes root mean square errors in MVPA estimates among children as compared with direct observation.25
4.5. Strengths and limitations
To the best of our knowledge,this study is the first to assess the relationship between objectively measured PA and brain function using neuroelectric correlates of cognitive control in typically developing children.By using ERPs,we were able to measure brain function in real time and focus on an early stage in the information processing stream when attention is allocated to task-relevant stimuli, because previous research showed benefits of PA to increased attention allocation and faster stimulus evaluation. Second, we measured PA using shorter epochs compared with the previous studies of PA and cognition in children to accurately capture brief and intermittent bouts of children’s VPA.We further identified a minimum PA intensity (i.e., MVPA as compared with MPA) and a specific accumulation pattern(i.e., PA accumulated in bouts lasting ≥30 s ), which are related to more optimal brain function in preadolescents. Our study extends previous research on the effects of varying epoch lengths on the relationships between PA and health in children to neurocognitive outcomes and shorter epoch lengths (<15 s compared with 15 s and 60 s ).Our findings suggest that, despite the differences in VPA patterns across epochs (i.e., increasing daily VPA but decreasing time spent in longer VPA bouts), the choice of epoch length did not alter the observed relationships. Finally, aerobic fitness, assessed using a gold standard graded exercise test on the treadmill, was controlled for in all models. Finally, our results reinforce the idea that PA behavior makes a unique contribution to brain function in children.
Some limitations of our study need to be recognized. As noted in the Discussion,the positive results of the uncorrected analyses need to be interpreted with caution and require replication in future studies, because null associations were observed in corrected analyses.Second,the adopted cross-sectional study design precludes causal inferences. Although a bidirectional relationship between PA and neurocognitive outcomes has been reported in adult samples,87,88PA engagement among children is partly reliant upon parental instrumental support to facilitate access to PA opportunities(e.g.,safe environment, transport, financial support),89especially during the summer, when the present study was conducted. Therefore, a bidirectional relationship between PA and cognitive outcomes is less likely to account for our results,which are supported by previous research.90Third,the physiological relevance of brief VPA bouts needs further study,although previous research has indicated that 40% of children’s daily activity-related energy expenditure can be accounted for by VPA bouts of comparable duration.27Fourth, certain types of structured PA were not assessed in this study owing to the limitations of accelerometers in capturing cycling and water-based activities. Because PA was measured during the summer months, when cycling and swimming are more common, the time spent in MVPA was likely underestimated. Although the type of PA was not measured in our study,it is unlikely that doing so would have fully explained the associations between greater engagement in bouted VPA and shorter P3 latency. In confirmation, a dose-response effect of PA intensity on cognitive control has been previously reported after a 9-month PA intervention.19Because all children engaged in the same types of PA during intervention sessions,19these results suggest that high PA intensity uniquely contributed to increments in cognitive control,which aligns with our findings.Finally,we adopted a single cut-point to evaluate whether the observed associations change with epoch length. Although PA intensity estimates vary with epoch length,23,24,26,91previous research also suggests that scaled cut-point values are comparable with those developed using a 15 s epoch, as indicated by minimal mean differences in counts (△Mdiff=9 counts and 21 counts for MPA and VPA, respectively) and no influence on classification accuracy.92
5. Conclusion
This study explored the associations between children’s daily PA, brief PA bouts, and behavioral and neuroelectric indices of cognitive control. In the exploratory analyses, we found that the most consistent associations were between the time spent in VPA bouts lasting ≥30 s and the efficiency in cognitive processing across epochs and task conditions that varied in cognitive control demands. Associations for bouted MVPA were less consistent,and bouted MPA was not related to cognitive processing. Taken together, our findings suggest that bouted PA may be related to more efficient cognitive processing in children in a dose-response manner. However,these exploratory findings require replication in future studies.We conclude that bouted VPA in preadolescents may yield the greatest benefit to cognitive control.Our study underscores the importance of objectively measuring PA patterns in relation to neurocognitive health during childhood as well as using timesensitive measures of brain function.By using ERPs,we were able to show for the first time that the effects of bouted VPA and MVPA were specific to earlier stages of information processing. Our findings pave the way for future studies, which include measures of brain function and structure to test the underlying mechanisms.
Acknowledgments
This study was funded in part by National Institute of Child Health and Human Development (NICHD RO1 HD069381)(to CHH and AFK), National Institute of Food and Agriculture, U.S. Department of Agriculture (2011-67001-30101),University of Illinois at Urbana-Champaign and Abbott Nutrition through the Center for Nutrition, Learning, and Memory(ANGC1204)(to CHH and NAK).
The authors thank the participants, their families, and the Urbana School District 116 for participating in the study. In addition, the authors thank Bonnie Hemrick and Jeanine Bensken for their assistance in recruiting study participants,and the numerous undergraduate students and staff who helped with the testing of study participants. The authors thank numerous undergraduate students at Northeastern University for their assistance in the preparation of the Supplementary Tables.
Authors’contributions
DMP conceived of the study and analytical approach, collected the data, reduced accelerometry data, conducted statistical analyses,and drafted the manuscript;ESD collected the data and reduced neurophysiological and cognitive data; LBR and SCK collected the data and reviewed data analyses and early drafts of the manuscript;NK contributed to data interpretation;DRW collected the data and reviewed data analyses; MH, RS,and EC contributed to accelerometry data reduction and reviewed results for accuracy;DJ critically reviewed the methodological and analytical strategy and early versions of the draft; AFK and CHH conceived of the randomized controlled trial (FITKids2 trial, ClinicalTrials.gov: NCT01619826) from which this study drew data,coordinated the trial,supervised the study, and conceptually contributed to data interpretation. All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2019.02.003.
 Journal of Sport and Health Science2019年4期
Journal of Sport and Health Science2019年4期
- Journal of Sport and Health Science的其它文章
- Associations between cardiorespiratory fitness,physical activity,intraindividual variability in behavior,and cingulate cortex in younger adults
- Affect and prefrontal hemodynamics during exercise under immersive audiovisual stimulation:Improving the experience of exercise for overweight adults
- The exercise-cognition relationship:A virtuous circleMichel Audiffren*,Nathalie Andr´e
- An overview of ischemic preconditioning in exercise performance:A systematic review
- The relationship of high-intensity cross-training with arterial stiffness
- Levels and correlates of 24-hour movement behaviors among South Koreans:Results from the Korea National Health and Nutrition Examination Surveys,2014 and 2015