
An overview of ischemic preconditioning in exercise performance:A systematic review
2019-10-16 02:35:22MaximeCaruArianeLevesqueFrancoisLalondeDanielCurnier
Maxime Caru*,Ariane Levesque,e,Fran¸cois Lalonde,Daniel Curnier
a Laboratory of Pathophysiology of EXercise(LPEX),School of Kinesiology and Physical Activity Sciences,Faculty of Medicine,University of Montreal,Montreal,Quebec H3T 1J4,Canada
b Department of Psychology,University of Paris-Nanterre,Nanterre 92000,France
c Laboratoire EA 4430-Clinique Psychanalyse Developpement(CliPsyD),University of Paris-Nanterre,Nanterre 92000,France
d CHU Ste-Justine Research Center,CHU Ste-Justine,Montreal H3T 1C5,Canada
e Department of Psychology,McGill University,Montreal,Quebec H3A 1G1,Canada
f Department of Physical Activity Sciences,Faculty of Sciences,Universit´e du Qu´ebec `a Montr´eal,Montreal,Quebec H2L 2C4,Canada
Abstract Ischemic preconditioning(IPC)is an attractive method for athletes owing to its potential to enhance exercise performance.However,the effectiveness of the IPC intervention in the field of sports science remains mitigated.The number of cycles of ischemia and reperfusion,as well as the duration of the cycle,varies from one study to another.Thus,the aim of this systematic review was to provide a comprehensive review examining the IPC literature in sports science.A systematic literature search was performed in PubMed(MEDLINE)(from 1946 to May 2018),Web of Science(sport sciences)(from 1945 to May 2018),and EMBASE(from 1974 to May 2018).We included all studies investigating the effects of IPC on exercise performance in human subjects. To assess scientific evidence for each study, this review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.The electronic database search generated 441 potential articles that were screened for eligibility.A total of 52 studies were identified as eligible and valid for this systematic review.The studies included were of high quality,with 48 of the 52 studies having a randomized, controlled trial design. Most studied showed that IPC intervention can be beneficial to exercise performance. However, IPC intervention seems to be more beneficial to healthy subjects who wish to enhance their performance in aerobic exercises than athletes.Thus,this systematic review highlights that a better knowledge of the mechanisms generated by the IPC intervention would make it possible to optimize the protocols according to the characteristics of the subjects with the aim of suggesting to the subjects the best possible experience of IPC intervention.2095-2546/© 2019 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords: Exercise;Human performance;IPC protocols;Ischemic preconditioning;Sports science
1. Introduction
Ischemic preconditioning (IPC) is an attractive method for athletes due to its relationship with exercise performance.IPC intervention is a noninvasive procedure that involves inducing 3-4 cycles of brief episodes of ischemia(inflation of a blood pressure cuff)and reperfusion(gradual deflation)via a pressure cuff on a skeletal muscle.1This intervention was initially developed to decrease the damage caused to internal organs by ischemia and reperfusion.2However, it has been speculated that IPC also has an effect on exercise performance,notably by improving muscle oxygenation, vasculature, and blood flow delivery to active tissues and organs.3
The mechanisms involved in these athletic improvements are likely related to both metabolic and vascular pathways.4As a matter of fact,it is thought that IPC can act through 3 main pathways(i.e.,neuronal,humoral,and systemic response).5-7The neuronal pathway,which includes the spinal cord and the autonomous and somatosensory nervous systems, is activated by endogenous substances (i.e., adenosine,8,9bradykinine,10or opioid11,12)generated by the stimulated distant organ.These endogenous substances lead to the activation of afferent nerve fibers that transmit the electrical signal to the targeted organ.This signaling leads to protective cellular processes in the targeted organ.6The humoral pathway has the same underlying mechanism involving endogenous substances,according to the Hausenloy and Yellon6hypothesis. However,these substances are involved in IPC by their entry into the bloodstream,which causes them to activate their specific receptor upon their arrival in an organ of the central nervous system.13This step allows the recruitment of various intracellular pathways of cardioprotection,which are also thought to play a role in exercise performance.14The systemic response is a protective response that involves the elimination of inflammation and apoptosis through the stimulation of transient ischemia and reperfusion of an organ or tissue.As a matter of fact,some studies have proven that there is a decrease in the cell membranes of specific adhesion molecules(intracellular adhesion molecule-1, P-selectin) after IPC.15Even though the number of studies interested in this type of response is limited, it has been shown that this decrease in inflammation can prevent the exacerbation of ischemic injuries.Thus,through these 3 pathways,it is thought that IPC can be important not only in preventing damage to internal organs following a cardiac episode,but also in athletic performance.
The effectiveness of IPC intervention in the field of sports science remains unclear. Indeed, some studies report significant exercise performance benefits(i.e.,time trial performance,maximal oxygen consumption (VO2peak), power output), whereas others demonstrate no effect.4,16Also, there does not appear to be a consensus on the optimal procedure to be used for an IPC intervention, which could explain the differences in results between studies.Although many studies seem to be based on the original study of Przyklenk et al.,17the number of cycles of ischemia and reperfusion, as well as the duration of the cycle varies from one study to another. Thus, the aim of this systematic review was to provide a comprehensive review examining the IPC literature in sports science.
2. Methods
A systematic literature search was performed by 2 independent reviewers (AL and MC) in PubMed (MEDLINE) (from 1946 to May 2018),Web of Science(sport sciences)(from 1945 to May 2018), and EMBASE (from 1974 to May 2018). The search terms for the inclusion criteria were a combination of database specific MeSH terms and keywords:“remote ischemic preconditioning” OR “remote ischaemic preconditioning” OR“remote preconditioning” OR “remote conditioning” OR“remote ischemic conditioning” OR “remote ischaemic conditioning”OR“transient limb ischemia”OR“muscle ischemia”OR “ischemic preconditioning” AND “performance” OR“sport*” OR “exercise” OR “strength training” OR “running”OR“swimming”OR“cycling”OR“athletes”OR“athletic performance”.When it was possible,in the different databases,we added the human filter.Also,the reference lists of all identified studies were scanned manually for additional studies.
2.1. Inclusion and exclusion criteria of studies
We included all studies investigating the effects of IPC on exercise performance in human subjects without any age restriction (age of children ≤18 and age of adults >19). Journal articles written in a language other than English or French were excluded. During the first analysis by abstract, the conference abstracts, case reports, short communications, systematic reviews, meta-analyses, theses, letters to editor, and protocol papers were excluded due to the inability to evaluate the risk of bias of the individual study. Also, studies with animals or nonhealthy subjects were excluded. When the title and the abstract were potentially eligible for inclusion,the full-text was obtained.Studies with a design of randomized, controlled trials, nonrandomized controlled trials, and uncontrolled interventions(i.e.,pretests and post-tests without controls)were included.The last day of the literature search was June 1,2018.
2.2. Data extraction and quality analysis
To assess scientific evidence for each study,this review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.18Two independent researchers(AL and MC)reviewed the articles for eligibility and validity. Data extraction was performed by 1 investigator(AL);when data were lacking in the original article,the authors of the review contacted the original author to obtain additional data.The following data were extracted:characteristics(number,health physical state,sex,and age)of the subjects,IPC sets,ischemia pressure(mmHg),preconditioned limb,time to test,type of exercise,exercise protocol,and findings.
3. Results
3.1. Study selection
A flow chart showing the different phases of this review according to the PRISMA is depicted in Fig. 1. The electronic database search generated 441 potential articles that were screened for eligibility. There were 12 additional records identified through other sources. After the first analysis by title and abstract,58 full-text articles were assessed.Among these full-text articles,6 did not meet our inclusion and exclusion criteria(short TagedFigure communication (n=2), brief communication (n=1), reviews(n=2), letter to the editor (n=1)). Finally, a total of 52 studies were identified as eligible and valid for this systematic review.
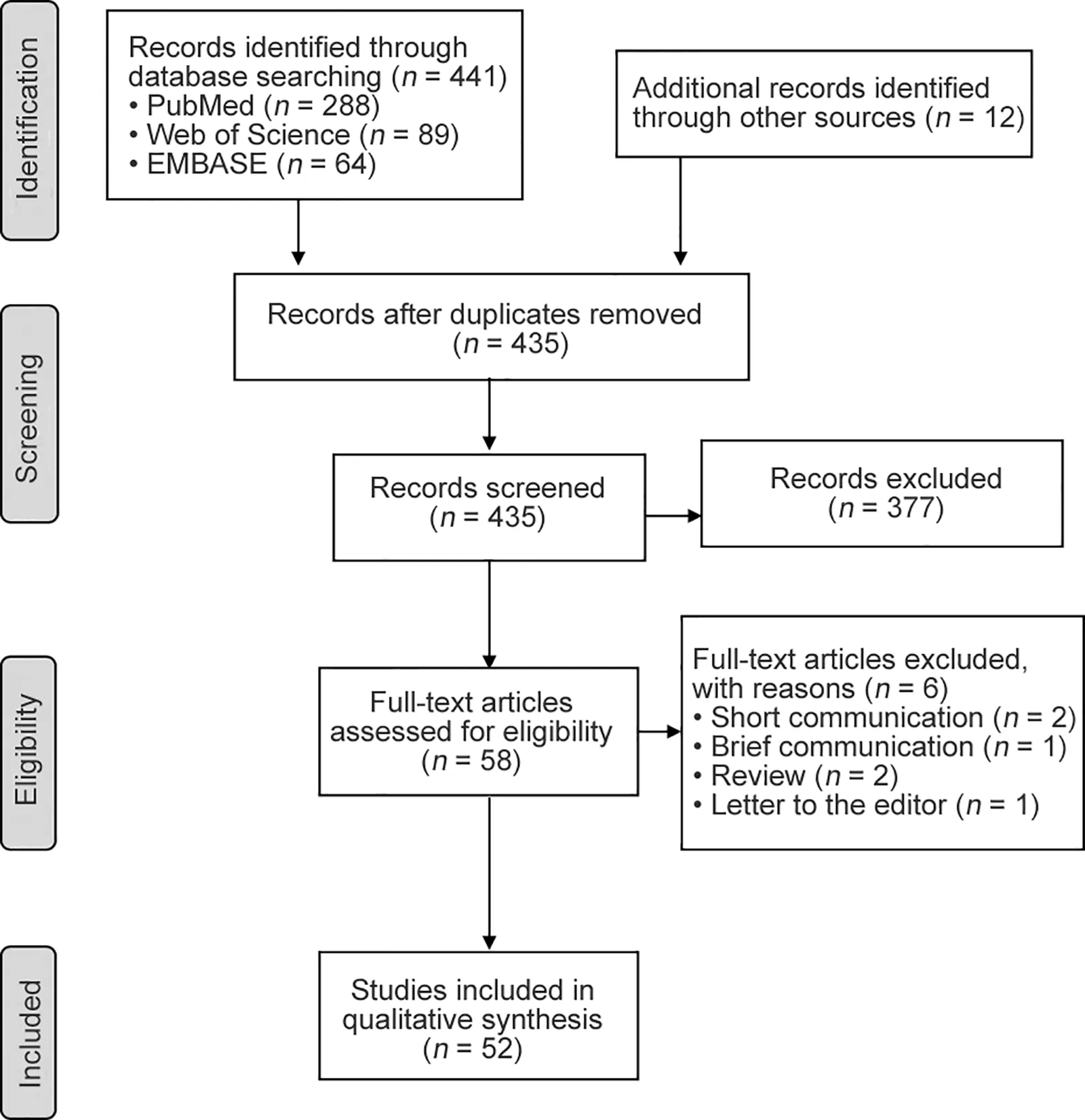
Fig.1. Literature search and study selection from PRISMA statement.
3.2. Characteristics of included studies
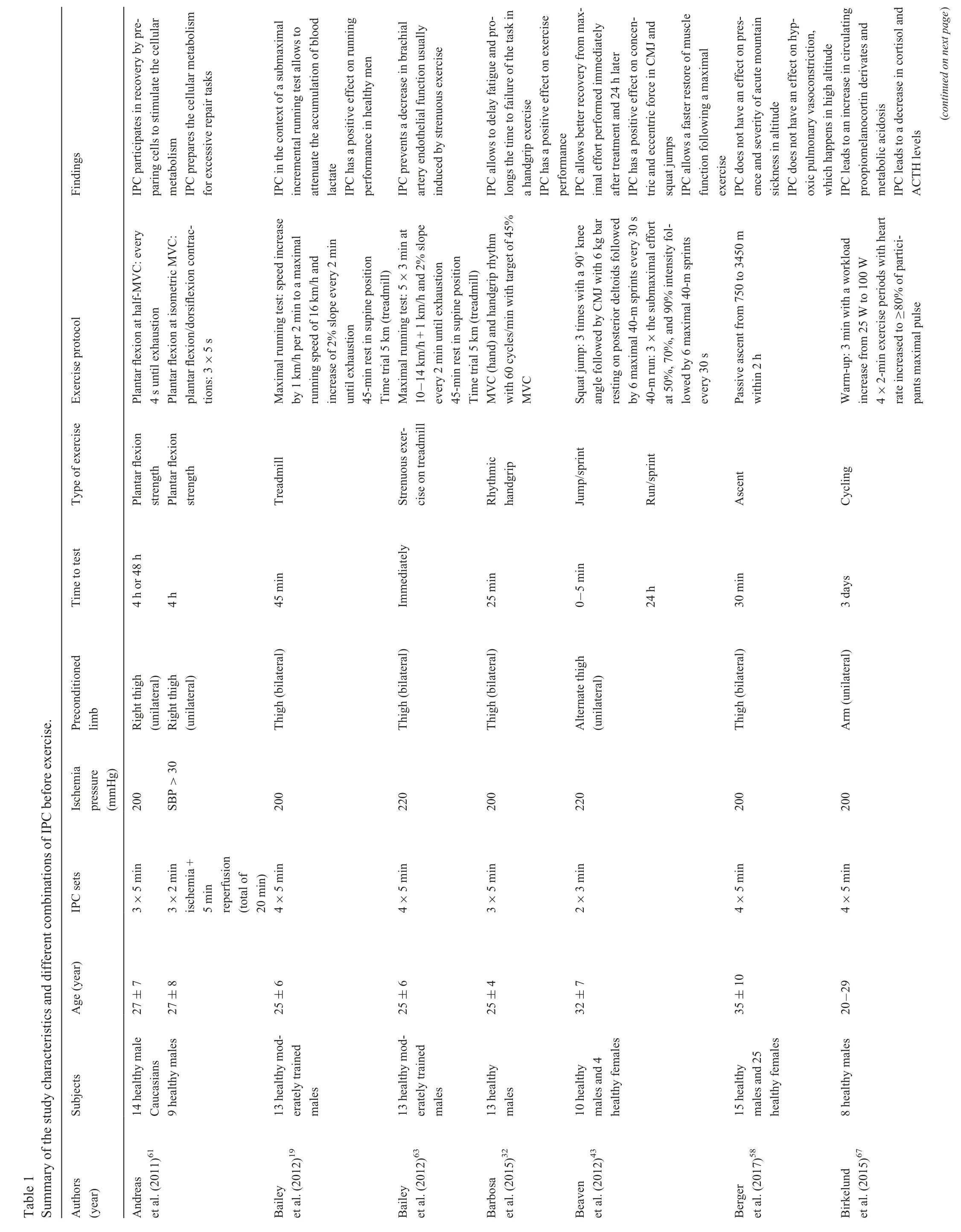
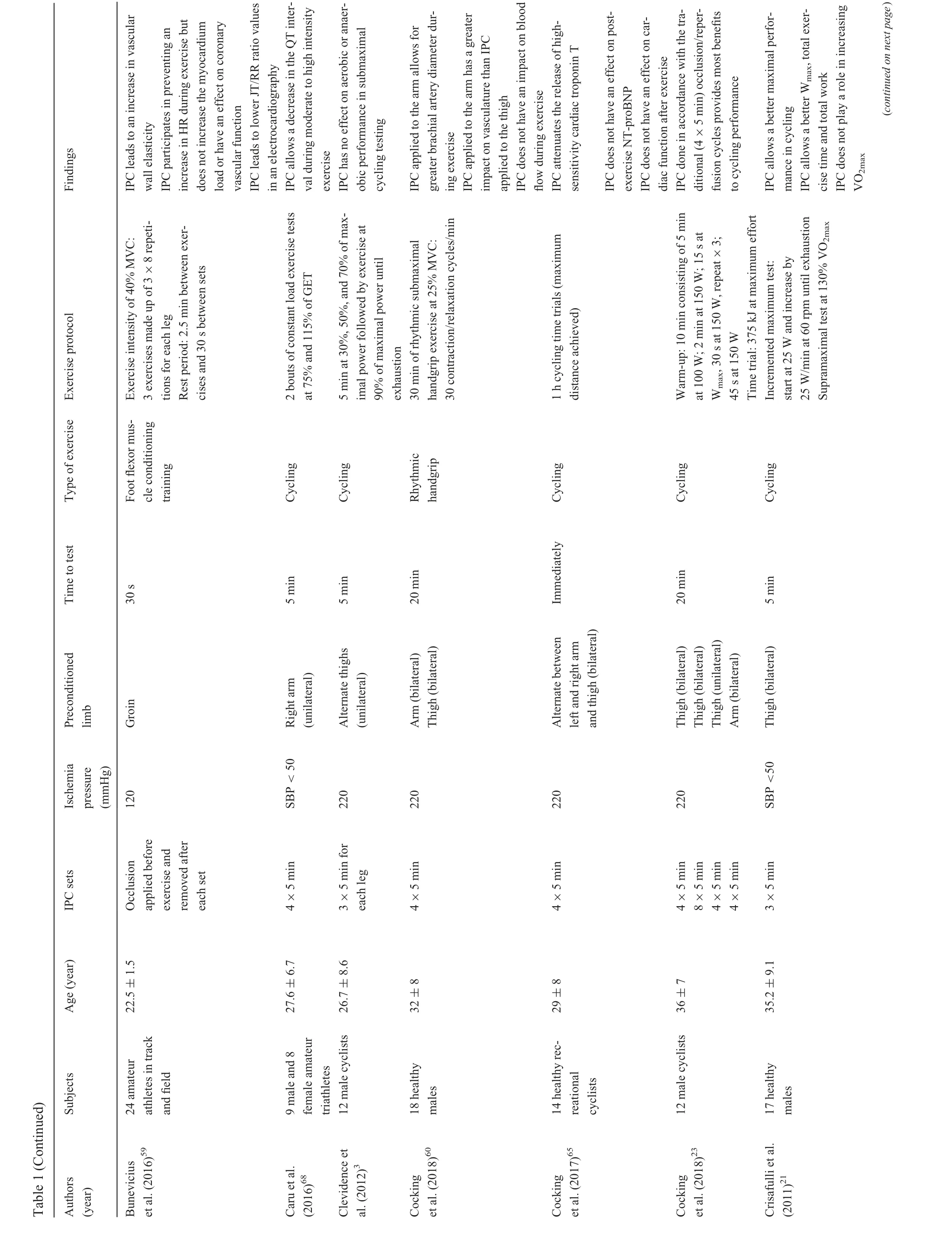
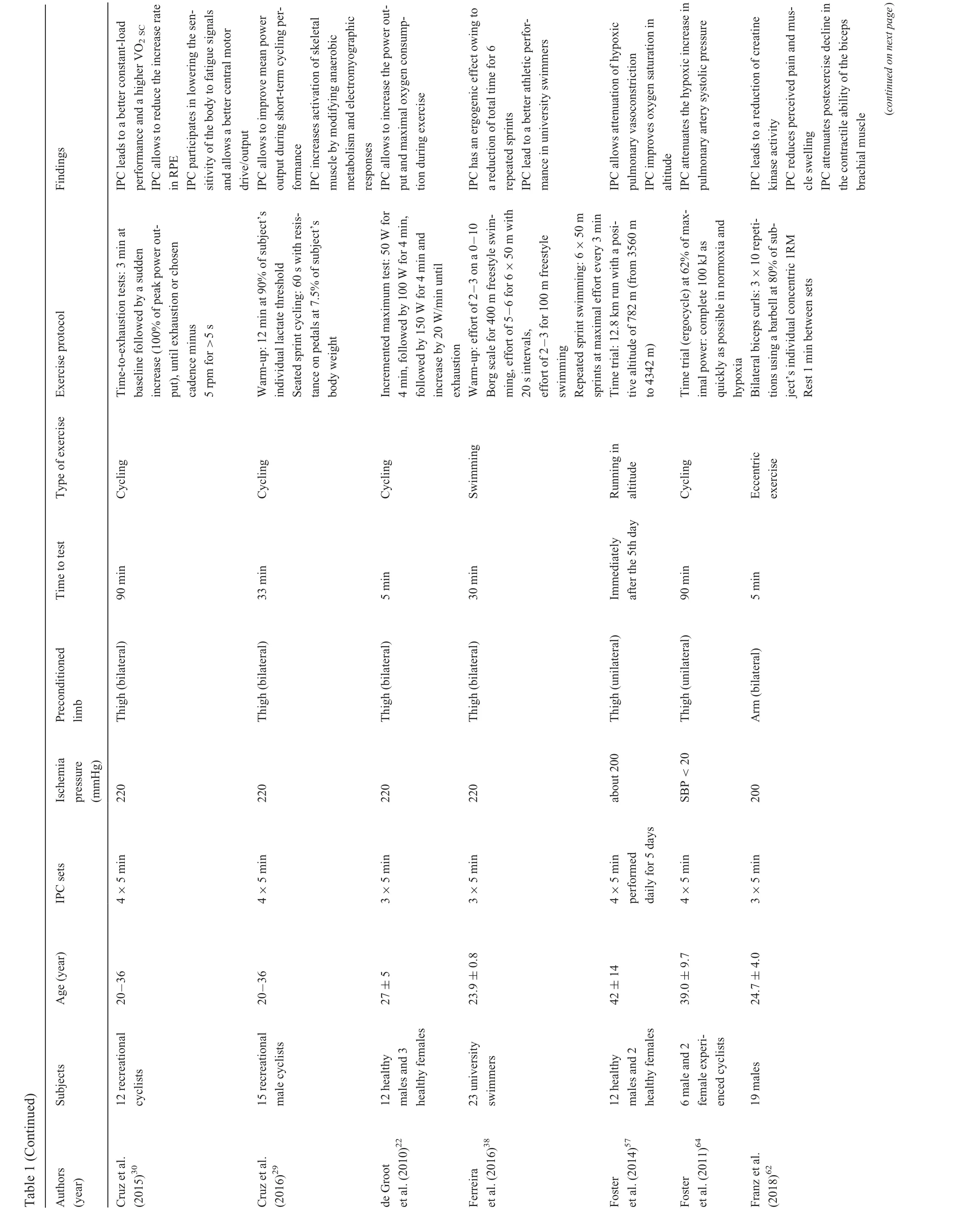
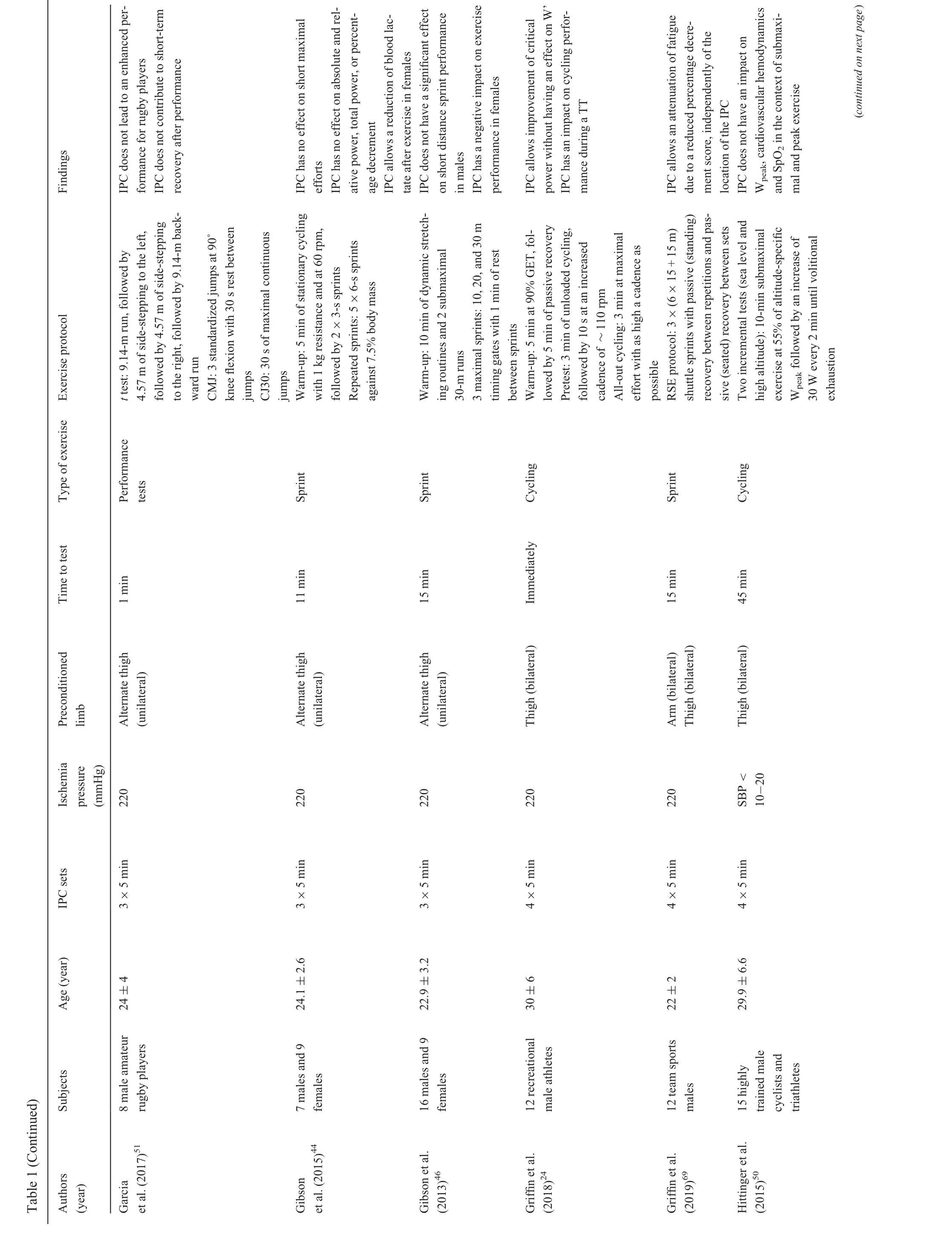
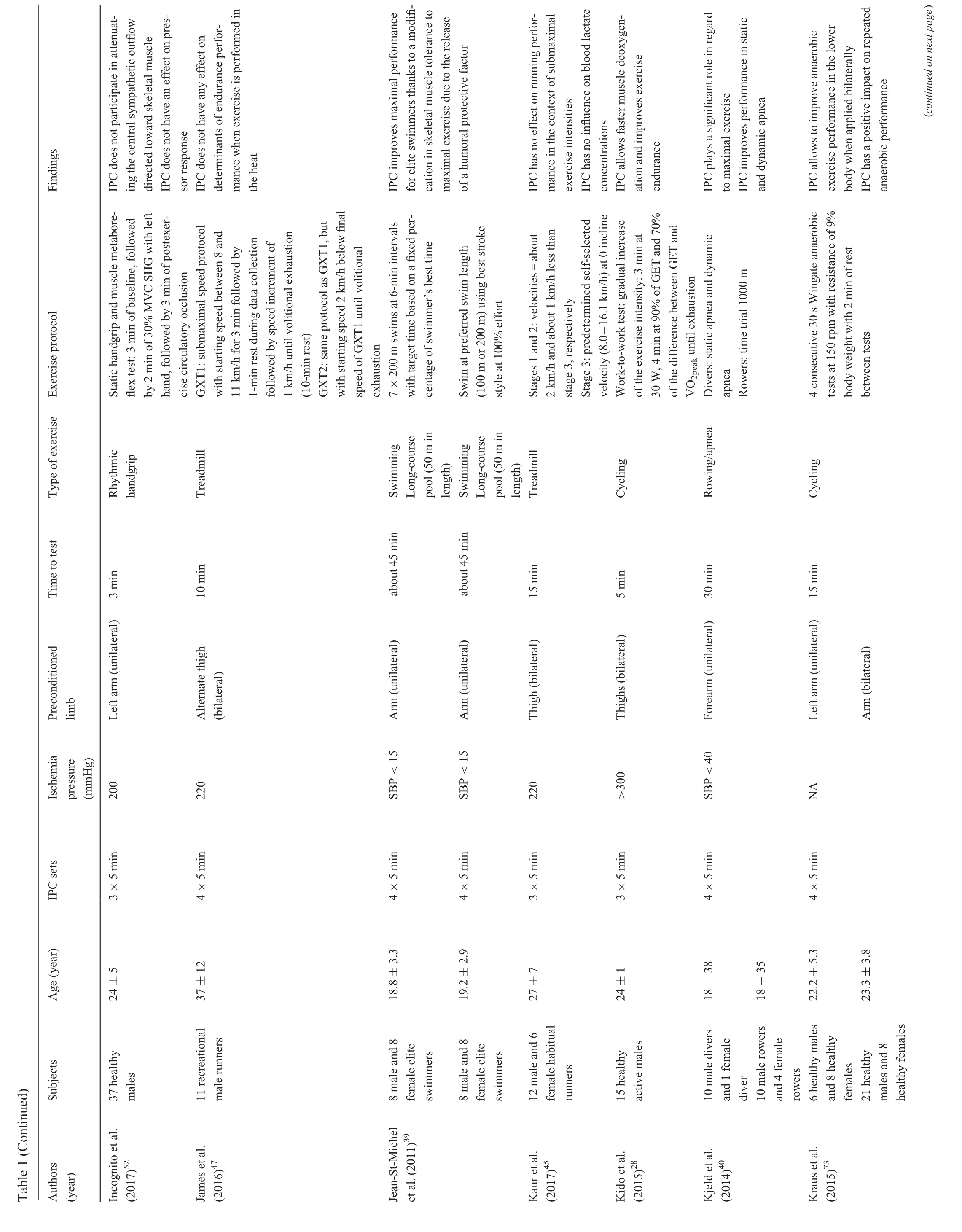
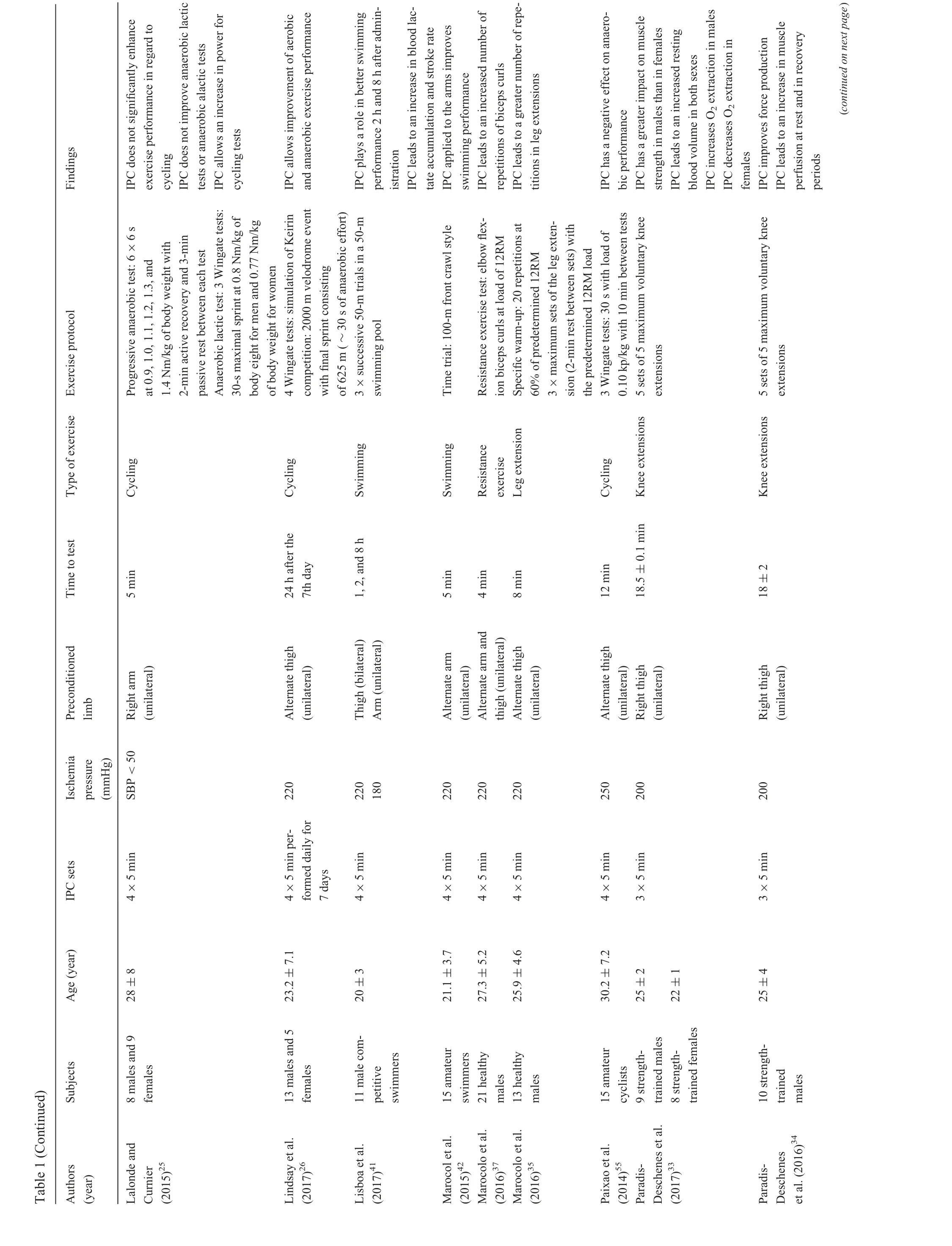
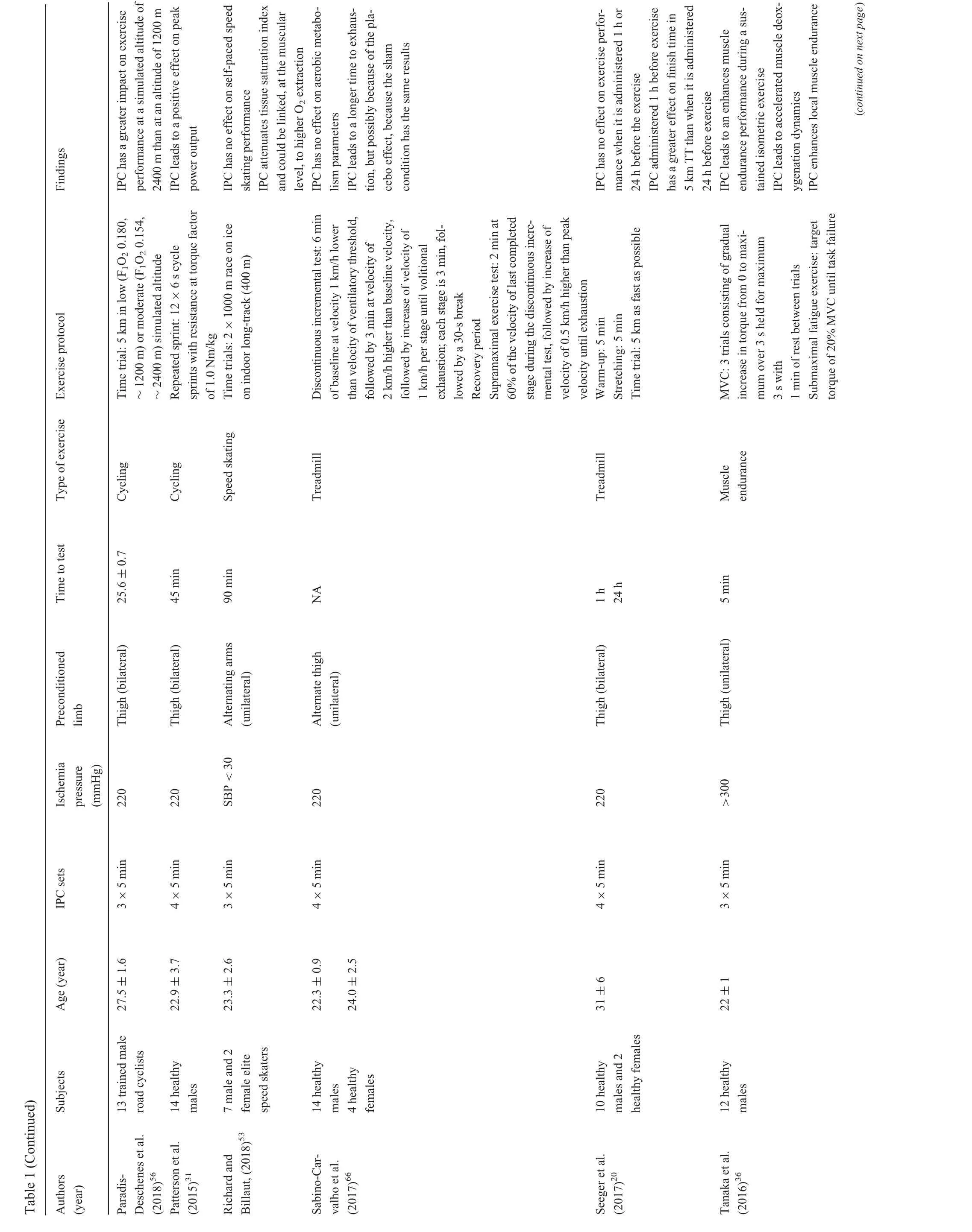
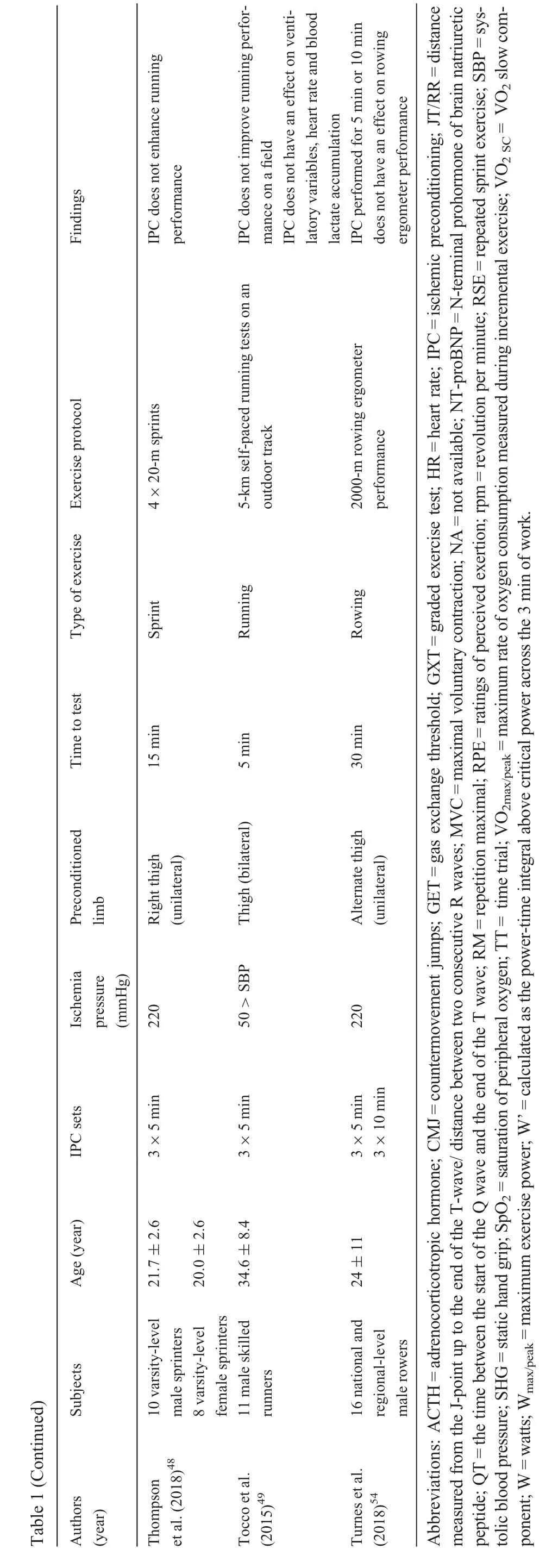
Study characteristics of all 52 included studies are summarized in Table 1. Forty-eight studies were randomized, controlled trials and 4 had a study design that was not available.Among these 48 studies, 44 were crossover trials, 12 were counterbalanced, 11 were single blinded, 2 were double blinded, 3 were controlled, 3 were sham controlled, 2 were placebo and nocebo controlled,and 1 was placebo controlled.
Also,of these 52 articles in this systematic review,19 investigated cycling performance,8 investigated flexion strength performance, 6 investigated treadmill performance, 5 investigated sprint performance, 4 investigated swimming performance,3 investigated handgrip performance, 2 investigated running performance,2 investigated rowing performance,1 investigated ascent performance, 1 investigated diving performance, and 1 investigated speed skating performance. Overall, most studies used IPC sets of three 5-min cycles of ischemia followed by 5-min of reperfusion or four 5-min cycles of ischemia followed by 5-min of reperfusion with a pressure cuff inflated to 200 or 220 mmHg.A total of 873 healthy participants,amateur athletes or trained athletes (730 males and 143 females) performed the IPC intervention before exercise performance.
3.3. Effects of IPC on exercise performance
3.3.1. Positive effect of IPC on exercise performance
Out of the 25 articles that found a positive effect of IPC on exercise performance, 2 showed that IPC enhanced performance in 5-km runs,specifically when IPC was administered 1 h before the exercise.19,20Ten articles found that IPC had a positive effect on cycling performance. The types of performance studied were incremental maximum cycling,21,22time trials,23,24aerobic/anaerobic cycling,25,26Wingate cycling tests,27work-to-work test,28short-term cycling,29time-to-exhaustion tests,30and repeated sprints.31Some of these articles attributed IPC to a better maximal power output(Wmax),total exercise time and total work,21a higher VO2slow component(VO2SC),30a better central motor drive/output,30a better mean power output,29an increase in activation of skeletal muscle,and a better critical power.24Seven articles found a positive effect of IPC on endurance performances. As a matter of fact,one study found an impact of IPC performance on a rhythmic handgrip exercise.32Three studies looked at knee/leg extensions33-35and found a positive effect on muscle strength,33force production,34and number of repetitions.35Two other studies found a positive effect of IPC on muscle endurance performance for isometric exercises36and biceps curls.37Five articles in this systematic review noted a positive effect of IPC on swimming performance. To find this effect, these studies evaluated either time in repeated sprints,38a maximal performance,39static and dynamic apnea,40stroke rates,41or performance in a time trial.42One study looked at performance of counter movement jump and squat jumps,and found a positive effect of IPC on the concentric and eccentric force produced during these jumps.43
3.3.2. No effect of IPC on exercise performance
In this systematic review,15 articles found no effect of IPC on exercise performance. Out of these articles, 7 looked at running exercises.They found no effect during sprints,44submaximal running,45short distance running,46endurance performance in the heat,47time trials,20maximal acceleration,48and running on a field.49Four articles found no effect of IPC during cycling performances, such as submaximal cycling,3maximum cycling,21cycling at high altitude,50and anaerobic cycling.25Four articles found no effect of IPC on other performances. These included rugby,51rhythmic handgrips,52speed skating,53and rowing.54
3.3.3. Negative effect of IPC on exercise performance
Two articles found a negative effect of IPC on performance.One article was in regard to sprint performance in females.46The other article was in regard to anaerobic cycling performance.55
3.4. Effects of IPC on performance in altitude
3.4.1. Positive effect of IPC on performance in altitude
Two studies found a positive effect of IPC on performance in altitude. One study found a greater impact of IPC on exercise performance at a simulated altitude of 2400 m than at an altitude of 1200 m.56The other study found that IPC improved oxygen saturation during a time trial run in altitude.57
3.4.2. No effect of IPC on performance in altitude
One article found that IPC did not have an effect on the presence and severity of acute mountain sickness in altitude.This article also found that IPC had no effect on hypoxic pulmonary vasoconstriction in high altitude.58
3.4.3. Negative effect of IPC on performance in altitude
One article stated that IPC attenuated hypoxic pulmonary vasoconstriction during a time trial run in altitude.57
3.5. Effects of IPC on blood lactate accumulation during exercise
3.5.1. Positive effect of IPC on blood lactate accumulation during exercise
In this systematic review, 2 studies found that IPC attenuated the accumulation of blood lactate during a 5-km run and a sprint.19,44The study that focused on sprints found this result only for females.44
3.5.2. No effect of IPC on blood lactate accumulation during exercise
Two studies reported no effect of IPC on blood lactate accumulation during running exercise.45,49
3.5.3. Negative effect of IPC on blood lactate accumulation during exercise
One study that looked at swimming performance found that IPC had a negative effect on blood lactate accumulation during this exercise.41
?
?
3.6. Effects of IPC on metabolism adaptation
3.6.1. Positive effect of IPC on metabolism adaptation
Nine studies in this systematic review found that IPC had a positive effect on certain metabolism adaptations that occur during exercise.Out of the 7 studies that focused on endurance performances, 1 study found that IPC increased vascular wall elasticity and that IPC participated in preventing an increase in heart rate during exercise for foot flexor muscle conditioning training.59Another article stated that IPC applied to the arm before rhythmic handgrips allowed for greater brachial artery diameter and had a greater impact on vasculature.60One study focused on plantar flexion exercises and found that IPC prepared the cellular metabolism for excessive repair tasks.61The next study discovered that IPC led to a decrease in creatine kinase activity during an eccentric exercise.62Two studies focused on knee extension exercises.The first found that IPC increased O2extraction in males33and the second stated that IPC led to accelerated muscle deoxygenation dynamics, which helped with muscular hypertrophy.36The last study that looked at endurance exercises found that IPC prevented a decrease in brachial artery endothelial function.63One study focused on the effects of IPC on speed skating and discovered that it attenuated the tissue saturation index and could be linked,at the muscular level, to higher O2extraction.53The last article found that IPC attenuated the hypoxic increase in pulmonary artery systolic pressure during a cycling exercise.64
3.6.2. No effect of IPC on metabolism adaptation
In this systematic review, 6 studies found that there was no effect of IPC on different metabolism adaptations of the body.Two studies investigated the impact of IPC on rhythmic handgrip performance. The first found that IPC did not have an impact on blood flow.60The second stated that IPC did not participate in attenuating the central sympathetic outflow directed toward skeletal muscle.52Two other articles focused on the effect of IPC on cycling performance. The first found that IPC did not have an effect on cardiac function after 1-h cycling time trials.65The second found that IPC did not have an impact on cardiovascular hemodynamics and saturation of peripheral oxygen in the context of submaximal and peak exercise.50Two articles investigated running performance. One study found no effect of IPC on aerobic metabolism parameters,66and the other stated that IPC did not have an effect on ventilatory variables and heart rate during running performances on a field.49
3.6.3. Negative effect of IPC on metabolism adaptation
One study found that IPC decreased O2extraction in females during knee extensions.33
3.7. Effects of IPC on blood parameters
The 2 studies in this systematic review that noted the effects of IPC on blood parameters evaluated cycling performance.The first study found that IPC increased circulating pro-opiomelanocortin derivates and metabolic acidosis.This article also stated that IPC decreased cortisol and adrenocorticotropic hormone levels.67The second study found that IPC attenuated the release of high-sensitivity cardiac troponin T after 1 h of cycling time trials.65
3.8. Effects of IPC on electrophysiology parameters
Two studies found positive effects of IPC on electrophysiology parameters.One study found that IPC led to a lower JT/RR ratio value(distance measured from the J-point up to the end of the T-wave/distance between two consecutive R waves) in an electrocardiogram during foot flexor muscle conditioning training.59The other study found that IPC decreased the QT interval(the time between the start of the Q wave and the end of the T wave; represents ventricular repolarization) during moderate-tohigh intensity exercises.68
3.9. Effects of IPC on exercise recovery
3.9.1. Positive effect of IPC on exercise recovery
Five studies in this systematic review found positive effects of IPC on exercise recovery. In regard to plantar flexion/knee extension exercises,studies in this systematic review found that IPC prepared cells to stimulate the cellular metabolism,61increased the resting blood volume,33and increased muscle perfusion at rest and in recovery periods.34For eccentric exercises,IPC decreased perceived pain and muscle swelling.62This practice also attenuated the postexercise decrease in the contractile ability of the biceps brachii muscle.62IPC also had a positive effect on recovery for running exercises.As a matter of fact,one article in this systematic review found that IPC encouraged an easier recovery from maximal jump/sprint efforts43and a faster restore of muscle function following a run/sprint exercise.43
3.9.2. No effect of IPC on exercise recovery
One article in this systematic review found that IPC had no effect on short-term recovery following a rugby performance.51
3.9.3. Unclear effect of UPC on exercise recovery
One article showed that IPC might lead to a longer time to exhaustion for running performance, but this finding could be attributed to the placebo effect, because the sham condition showed the same results.66
3.10. Effects of IPC on fatigue
Three studies in this systematic review found positive effects of IPC on the presence of fatigue during performance.The studies looked at rhythmic handgrip exercises,32time-toexhaustion tests,30and repeated sprint exercises.69
3.11. Effects of IPC on the rating of perceived exertion
One study found that IPC administered before a time-toexhaustion tests reduced the increase rate in the rating of perceived exertion.30
4. Discussion
This systematic review showed an overview of the research done on IPC over the past 28 years. Overall, the studies included were of high quality,with 48 out of 52 studies having a randomized, controlled trial design. The results highlighted in the articles showed the extent to which IPC can be beneficial to exercise performance. Overall, the main finding of this systematic review was that the effects of IPC intervention seemed to be more effective in healthy subjects who wish to enhance their performance in aerobic exercises than in athletes. It is important to note that the first studies about IPC were mainly conducted in healthy subjects, with promising results. However, recent articles studying athletes did not seem to find the same positive effects.This discrepancy could be due to the protocol not being optimized for this population.
4.1. Responders and nonresponders to IPC
In exercise physiology,it has been reported that there are responders and nonresponders to regular physical activity.70Indeed,it has been shown in healthy and untrained populations that there is a great interindividual variability in subjects’capacity to improve their cardiac profile in response to regular exercise.71It has been hypothesized that the same situation exists for IPC,where there are both responders and nonresponders to the intervention. This finding could explain the variation in hemostatic,endothelial,and inflammatory responses to IPC as a tool to enhance exercise performance. Gene expression could explain this phenomenon.4,72The identification of a biomarker aiming to define the optimal preconditioning stimulus remains at the hypothetic stage.However,many studies have been working on elaborating this complex substance.72
4.2. Variation in IPC protocols
In this systematic review, there was a lot of variability between studies regarding the IPC protocol. Thus, there did not seem to be a consensus on the optimal procedure to be used for an IPC intervention. Indeed, the number of cycles of ischemia and reperfusion,the duration of the cycles,as well as the period between the time to test and the end of IPC intervention varied from one study to another.Our results showed that the number of cycles of ischemia and reperfusion ranged from 2 cycles43to 8 cycles.23Also, the duration of occlusion periods ranged from 2 min61to 10 min.54The majority of studies performed IPC on the day of the test.However,a few studies performed IPC on a daily basis from 5 days57to 7 days26before the exercise protocol.The time period from the administration of the IPC protocol to the start of the exercise protocol also varied from immediately24,43,63,65to 72 h67from one study to another.Some studies that explored the second window of protection of IPC20,43,61,67reported encouraging results,43,61,67whereas others reported results inferior to the first window of protection.20Because many different methodologic parameters differed between the studies,the comparison of their results was difficult. As a result, some studies reported no effect of IPC on exercise performance, but this could be due to the IPC protocol not being optimal or to the window of protection not being ideal for the study population.
4.3. Variation in IPC methodologic aspects
There was also an inconsistency between studies regarding the limb that was made ischemic.As a matter of fact,some studies performed IPC sets on the thigh,whereas others opted for the arm.One study23was interested in these different methodologic aspects.Cocking et al.23studied the optimal ischemic preconditioning dose to improve cycling performance.Thus,responses to traditional IPC(4×5 min thigh(bilateral))were compared with 8×5 min thigh (bilateral), 4×5 min thigh (unilateral) and 4×5 min arms(bilateral).The results of this study reported that traditional IPC (4×5 min) provided most benefits to cycling performance. They also found that applying more dose cycles(8×5 min) had no impact on performance and that unilateral IPC was more effective that bilateral cuffs. Regarding another aspect, de Groot et al.22had studied IPC in its beginnings and had shown that with <3 cycles of IPC, the intervention had no clinical interest in sports performance. Also, during a Wingate anaerobic test, Kraus et al.73showed an improvement in the mean and maximal power output when the ischemia was applied bilaterally to the arm,rather than a unilateral cuff.
4.4. Variation in types of studies
Beyond the methodologic aspect of IPC for which there is no consensus for the moment,there needs to be consideration for the diversity in the nature of the studies put forward in this systematic review. As a matter of fact, there was a multitude of designs and results addressed by teams of researchers in different fields;such as cycling,sprint,running,swimming,rowing,ascent,skating,flexion strength,handgrip,and so on.The first studies exploring the effects of IPC in sports science focused on maximizing exercise performance, as well as physiological parameters (i.e., power output,maximal oxygen consumption).19,21,22,64,74Recently, the results have evolved to highlight the innovative effects of IPC on exercise performance. Indeed, altitude performance has been evaluated,56-58along with the effects of IPC on exercise recovery,33,34,43,51,61,62,66fatigue,30,32,69and rating of perceived exertion.30However,research has been reexamined as a result of a lack of evidence to explain the mechanisms responsible for the outcome of IPC.75In this regard,there seems to have been some work done by the scientific community. Indeed, the effects of IPC on metabolism adaptations have been studied in numerous studies33,36,49,50,52,53,59-66to better understand the observed effects of IPC on sports performance.Also,to our knowledge,this is a point that Incognito et al.4and Horiuchi75discussed in their systematic review.This approach is directly related to the exploration of a procedure to optimize IPC protocols and,therefore,a consensus.
4.5. Perspectives
Finally,not all studies directly observed a positive effect of IPC on exercise performance.However,they participated in enriching the scientific knowledge on the matter and they provided additional information about IPC,which is currently an unknown therapeutic intervention to the amateur and high-level sports environment.Thus,this section on the perspectives of research on IPC was constructed from the 52 articles of this systematic review and from the perspectives they put forward in their conclusion.
4.5.1. Further research on mechanisms
Many perspectives in the articles of this systematic review focused on defining the different mechanisms observed in each study.Thus,it is possible to conclude that further research should go in a direction that investigates the mechanisms responsible for a decrease in blood lactate concentration during incremental exercise,19less damage to skeletal muscle,62and positive effects on peak power output during repeated sprint cycling performance.31It would also be interesting for the scientific community to know why IPC can lead to an improved blood flow,an improved efficiency of muscular oxygen usage,43an attenuation of the normal hypoxic increase of pulmonary artery pressures,and an improvement of oxygen saturation in altitude.57,64Future studies should elucidate the cellular and subcellular mechanisms of IPC,21better characterize the molecular mechanisms of IPC-induced changes,68and define the molecular and biological mechanisms behind the effects of IPC on exercise.28
4.5.2. Further research on local factors
Some of the 52 articles in this systematic review noted that further research should find out more about the effect of IPC on local factors, such as working limb flow, oxygen delivery,arteriovenous oxygen difference,50energy cost of endurance events,45and changes in intramuscular metabolism.36These parameters are often forgotten in analyses. Nevertheless, they remain interesting for the reader and they allow a better comprehension of the effects of IPC intervention on local factors.
4.5.3. Further research on variables
There have been some suggestions among the articles included in this systematic review about determining the effects of IPC on different variables. These avenues of research include studying a less healthy population,57testing different performance groups,74and evaluating different training statuses, types of sport, and risk factors.3These parameters have been evaluated recently in other articles,which is shown in our systematic review(Table 1).Nevertheless, it seems essential that researchers continue to investigate the effects of IPC with regard to different sports.
4.5.4. Further research on methods and IPC protocols
A few articles in this systematic review concluded that further research should be done on the methods and protocols associated with the IPC intervention.As a matter of fact,the authors of these articles suggested that there should be further investigation on the differences between the procedures of IPC,22the best IPC protocol for the most beneficial effects,46,48and the amount of muscle that needs to made ischemic to elicit more performance benefits.48,50,73One article in this systematic review focused on these perspectives,23as it was argued in the Discussion section.However,there seems to be an increasing need for this type of article to reach a consensus on the best IPC protocol.
4.6. Limitations
No meta-analysis could be conducted because the heterogeneity of the data was too high, which prevented a valid mathematical combination analysis. Indeed, the heterogeneity analysis, measured with Cochran’s Q test and the I2statistic,76revealed an I2of 73.47%.Among these important clinical heterogeneities and methodologic heterogeneities, we reported statistical, IPC interventions, outcomes, study participants, and study design heterogeneities. In this sense, the included studies were thought to be too different,either statistically,clinically or in methodologic terms,and thus not suitable for a meta-analysis.
5. Conclusion
It was difficult to compare the results between studies because the characteristics of the participants,IPC protocols and exercise tests differed between studies. Overall, the effects of IPC intervention appeared to be more effective in healthy subjects than in athletes. This finding could be due to the protocol not being optimized for this population. Thus, a better knowledge of the mechanisms generated by the IPC intervention would make it possible to optimize the protocols according to the characteristics of the subjects. We invite researchers to further discuss the mechanisms that may be involved in response to IPC intervention in exercise performance to provide the subjects with the best possible experience of IPC intervention.
Authors’contributions
MC and AL conceived of the study and participated in the design and coordination, performed the literature search and study selection from PRISMA statement, interpreted the data,and contributed to the writing of the manuscript; DC conceived of the study and participated in the design and coordination, and contributed to the writing of the manuscript; MC and FL contributed to the writing of the manuscript. All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
 Journal of Sport and Health Science2019年4期
Journal of Sport and Health Science2019年4期
- Journal of Sport and Health Science的其它文章
- Journal of Sport and Health Science Guide for Authors
- Standardization of exercise intensity and consideration of a dose-response is essential.Commentary on“Exercise-linked FNDC5/irisin rescues synaptic plasticity and memory defects in Alzheimer’s models”,by Lourenco et al.,published 2019 in Nature Medicine
- Could sport be part of pediatric obesity prevention and treatment?Expert conclusions from the 28th European Childhood Obesity Group Congress
- Editorial re:Could sport be part.....by Ring-Dimitriou et al.
- Exercise,cognitive function,and the brain:Advancing our understanding of complex relationships
- Author biographies