
Affect and prefrontal hemodynamics during exercise under immersive audiovisual stimulation:Improving the experience of exercise for overweight adults
2019-10-16 02:35:20LeightonJonesPanteleimonEkkekakis
Leighton Jones*,Panteleimon Ekkekakis
a Academy of Sport and Physical Activity,Sheffield Hallam University,Sheffield,S10 2BP,UK b Department of Kinesiology,Iowa State University,Ames,IA 50011,USA
Abstract Objective:Research on methods of improving the affective experience of exercise remains limited,especially for low-active overweight adults.We investigated the effectiveness of a virtual-reality headset and headphones in improving affective responses over conventionally delivered audiovisual stimulation.Methods:Low-active,overweight adults(16 women,5 men;age:34.67±9.62 years;body mass index:28.56±4.95 kg/m2;peak oxygen uptake for men:29.14±6.56 mL/kg/min,for women:22.67±4.52 mL/kg/min,mean±SD)completed 15-min sessions of recumbent cycling at the ventilatory threshold: (a) high immersion (HI, virtual reality headset and headphones),(b) low immersion (LI, television screen and speakers),and(c)Control.During-exercise pleasure and post-exercise enjoyment were self-reported.Oxygenation of the right dorsolateral prefrontal cortex(dlPFC)was assessed with near infrared spectroscopy.Results:Higher pleasure was reported during HI than during LI and Control(Condition×Time interaction;p <0.001,ηp2=0.43).Participants who reported a preference for low exercise intensity showed higher dlPFC oxygenation during Control,but this difference diminished during LI and HI(Condition×Time×Preference interaction;p=0.036,ηp2=0.10).Conclusion:Compared with conventionally delivered audiovisual stimulation,using a virtual-reality headset strengthens the dissociative effect,further improving affective responses to exercise at the ventilatory threshold among overweight, low-active adults. Presumably by competing with interoceptive afferents at the level of sensory input,audiovisual stimulation may lessen reliance on cognitive efforts to attenuate declining affect,as indicated by lower right dlPFC activity,particularly among participants disinclined toward high exercise intensity.2095-2546/© 2019 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords: Affective valence;Enjoyment;Immersion;Music;Video
1. Introduction
The promotion of exercise and physical activity (PA) has traditionally relied on providing people with information(e.g.,about anticipated health benefitsvs.costs, perceived capabilities, and sources of social support). This approach, characterized as the “rational educational model”,1assumes that behavior in general, and health behavior in particular, follow from a fundamentally rational decision-making process. The ultimate objective of rational decision-making is theorized to be the maximization of self-interest,including,above all else,the preservation of health and well-being. Although the rational-educational approach is credited with important successes in the domain of public health, the persistent inability to raise the rate of public participation in exercise and PA is forcing a critical reconsideration of the assumption that humans make behavioral decisions by rationally contemplating relevant information.2For example,according to the Lancet Physical Activity Series Working Group,3“the traditional public health approach based on evidence and exhortation has—to some extent— been unsuccessful so far” (p. 254).In response, an increasing number of researchers are calling for expanded,so-called“dual-process”theoretical models that integrate both rational, information-driven, deliberative pathways to behavior with non-reflective, implicit processes that depend heavily on past affective experiences of pleasure or displeasure.4,5
Prospective correlational6and experimental7studies suggest that affective responses to exercise may indeed play an important role in shaping subsequent exercise and PA behavior.8,9However, research over the past 2 decades has demonstrated that some individuals report declines in pleasure when exercise intensity approximates the ventilatory threshold (VT) and nearly all individuals report decreases at intensities that exceed the VT and preclude the maintenance of a physiological steady state.10Consequently, scholars9have called for the urgent prioritization of “experimental tests that attempt to manipulate the affective experience during exercise” (p. 728). However, very little is presently known about methods of improving the affective response to exercise, especially among individuals who are lowactive and overweight11,12and, therefore, representative of the majority of the adult population in most industrialized countries.
Attentional dissociation or distraction by audiovisual stimulation, aimed at shifting the attentional focus away from the inherently unpleasant interoceptive sensations associated with strenuous exercise, has been shown to ameliorate affective responses even at intensities that slightly exceed the VT.13-15The combination of audio and video typically results in a higher degree of attentional dissociation and more positive affective responses than either modality alone,presumably by saturating sensory channels with exteroceptive stimulation. In the present study, we took the concept of saturating sensory channels with audiovisual stimulation a step further by taking advantage of emerging low-cost technology.We hypothesized that the more immersive audiovisual stimulation delivered through personal devices (virtual-reality headsets and headphones) would attenuate any affective decrease during exercise compared to conventionally delivered audiovisual stimulation (screen and speakers) and a control condition (no audiovisual stimulation).
We also sought to investigate the neural underpinnings of the dissociative effect by assessing the hemodynamic response of the right dorsolateral prefrontal cortex (dlPFC) by using near-infrared spectroscopy (NIRS). The dlPFC is an area involved in top-down cognitive control and selective attention,including situations in which individuals spontaneously or deliberately attempt to shift their focus away from negative affective stimuli.16Consistent with models of hemispheric specialization, the right dlPFC, in particular, is consistently found to be activated during affect-regulation efforts,17,18including coping with pain and discomfort.19,20Higher activation in the right dlPFC (estimated as regional cerebral blood flow summated over a 60-s period via positron emission tomography) has been found to weaken the relationship between activity in the insula(a part of the brain that encodes the intensity of afferent interoceptive cues) and the degree of perceived stimulus intensity and displeasure.21Accordingly,experimental studies involving neuromodulation with transcranial magnetic stimulation or transcranial direct current stimulation have shown that increasing neural activity in the right dlPFC enhances the ability to dissociate from and downregulate negative affect,22-24including acute pain.25
Previous research on the brain hemodynamic responses to distraction from unpleasant stimuli has shown increases in dlPFC activity,both when the distraction consisted of a cognitive activity (mental arithmetic)26and when the distraction consisted of listening to self-selected music.27In contrast,Dunckley et al.28reported that, regardless of whether participants were instructed to focus on or dissociate from painful somatic stimulation, activity in the right dlPFC (assessed by functional magnetic resonance imaging,using an event-related paradigm,with twenty 3-s painful stimuli)was positively associated with activity in the insula and ratings of pain intensity.Thus, Dunckley et al.28speculated that activity in the right dlPFC may reflect attention directed toward the painful stimulus, regardless of instructions to associate or dissociate. In an effort to reconcile their findings with others showing a negative relation between right dlPFC activity and pain, Dunckley et al.28proposed a bidirectional relationship between the intensity of somatic stimulation and activity in the right dlPFC,such that a higher level of pain or displeasure stimulates higher activity in the right dlPFC,and this,in turn,serves to downregulate the pain or displeasure.In the present study,we adapted the hypothesis proposed by Karageorghis et al.29regarding the effects of music on dlPFC activity during exercise, namely,that music might cause a“shift of the entire oxygenation curve toward higher levels of intensity”,thus resulting in “a smaller increase in oxygenation at moderate intensities,presumably due to the lower level of experienced displeasure and therefore reduced need to cognitively control the displeasure” (p. 288). Specifically, we hypothesized that,although the challenging nature of exercise at VT may stimulate an increase in right dlPFC oxygenation (and, therefore,activation),the magnitude of the increase would be attenuated under audiovisual stimulation (presumably more so under immersive stimulation)compared to a control condition.
Finally, we anticipated that the experience of exercise would differ among participants, depending on their scores on the individual-difference variables of exercise intensity preference and tolerance. Preference for exercise intensity is defined as a predisposition to opt for a certain level of exercise intensity if given the opportunity, whereas tolerance of exercise intensity is defined as a trait that influences the tendency of an individual to persevere while exercising at an imposed level of intensity when the experience is uncomfortable or unpleasant.30These constructs were deemed relevant to the present investigation because(a) preference and tolerance have been found to account for 22%-34% of the variance in affective responses to exercise performed at VT30and (b) in a previous study,31young, normal-weight participants scoring in the top and bottom 5% of the distribution of exercise-intensity tolerance were found to differ both in affective responses and in patterns of prefrontal oxygenation at intensities above the VT. We hypothesized that exercise-intensity preference,tolerance, or both, would moderate the effects of our experimental conditions on both affective and prefrontal hemodynamic responses. Specifically, we expected that low-preference or low-tolerance participants (or both)would exhibit worse affective responses to exercise at VT than their high-preference or high-tolerance counterparts, at least while exercising under control conditions (i.e., with any difference likely attenuated under audiovisual stimulation). We also anticipated that, given their worse affective responses, low-preference or low-tolerance participants(or both) would show a larger increase in right dlPFC oxygenation in response to exercise under control conditions,with the difference attenuated under audiovisual stimulation (presumably more so under immersive stimulation).
2. Methods
The study received approval from the Ethics Committee at Sheffield Hallam University, and all participants provided written informed consent.
2.1. Participants
An a priori power analysis focused on affective responses as the primary outcome of interest.A Condition×Time interaction effect14of η2=0.30, an α of 0.05, and intended power of 0.95 indicated that 18 participants would be required. An additional 5 participants (i.e., total of 23) were recruited to account for attrition and outliers.
Recruitment was accomplished through advertisements distributed via university computer networks. Two participants failed to complete all conditions, citing competing time demands as their reason. Thus, the final sample included 21 participants (16 women, 5 men), between the ages of 19 and 58 years(34.67±9.62 years,mean±SD).The inclusion criteria were that they had to have a self-reported level of PA below current recommendations (<150 min of moderateintensity PA or 75 min of vigorous-intensity PA per week)and be overweight (body mass index (BMI) ≥25 kg/m2, 28.56 ±4.95 kg/m2). Peak oxygen uptake (VO2peak) indicated a poor level of aerobic fitness(29.14±6.56 mL/kg/min for men and 22.67±4.52 mL/kg/min for women).
2.2. Measures
2.2.1. Manipulation check:attentional focus
Attentional focus (association vs. dissociation) was assessed using the Attention Scale (AS) proposed by Tammen.32The AS is a single-item bipolar scale ranging from 0,indicating total associative focus (i.e., “internal focus: bodily sensations, heart rate, breathing, etc.”) to 100, indicating total dissociative focus(i.e.,“external focus:daydreaming,external environment, etc.”). Participants were asked to provide a response indicating their attentional focus at the moment immediately preceding the time point at which the scale was presented.
2.2.2. Manipulation check:perceived immersion
The Immersive Experience Questionnaire (IEQ)33was administered immediately after each condition, to assess the degree of perceived immersion in the experience.Because the IEQ was originally developed to measure immersion in computer games, minor modifications were made to the wording of some items (e.g., replacing the word “game” with “music and video”). The original IEQ includes items that tap 5 intercorrelated facets of immersion that all load on an omnibus factor:real world dissociation(7 items;e.g.,“To what extent did you lose track of time?”), emotional involvement (6 items;e.g.,“When interrupted,were you disappointed that the music and video were over?”), cognitive involvement (9 items; e.g.,“To what extent did you feel you were focused on the music and video?”),challenge,and control.The latter 2 facets,challenge and control,refer to perceived properties of video games rather than the immersion experienced by the participants themselves.Therefore,these items were not used in the present investigation. Responses to the IEQ items are entered on a 5-point scale ranging from 1 (not at all) to 5 (a lot). In the present sample, Cronbach’s α coefficient of internal consistency was acceptable (i.e., 0.77 after the control condition,0.92 after the low immersion(LI)condition,and 0.70 after the high immersion (HI) condition). However, it should be noted that only 2 of the 3 experimental conditions(LI, HI) included music and video; the control condition did not. Therefore,although it was necessary to administer the IEQ after all 3 conditions to avoid a confound, items that referred to music and video were treated as “fillers” after the control condition(received “not at all” responses). Therefore, the total IEQ score for the control condition is reported here merely for reference.
2.2.3. Primary outcome:affective valence
Affective valence (pleasure-displeasure) was assessed with the Feeling Scale (FS).34The FS is a single-item,11-point rating scale with anchors ranging from +5 (very good)to-5(very bad).
2.2.4. Secondary outcome:enjoyment
The Physical Activity Enjoyment Scale (PACES)35was administered immediately after each condition to assess enjoyment. The PACES comprises 18 items accompanied by 7-point bipolar response scales (e.g., “I dislike it” vs. “I like it”).Respondents are given the instruction,“Rate how you feel at the moment about the PA you have been doing.”The values of Cronbach’s α coefficient of internal consistency in the original development samples ranged from 0.93 to 0.96.These values are similar to those found in the present study (i.e., 0.97 after the control condition,0.98 after LI,and 0.94 after HI).
2.2.5. Secondary outcome:prefrontal hemodynamics
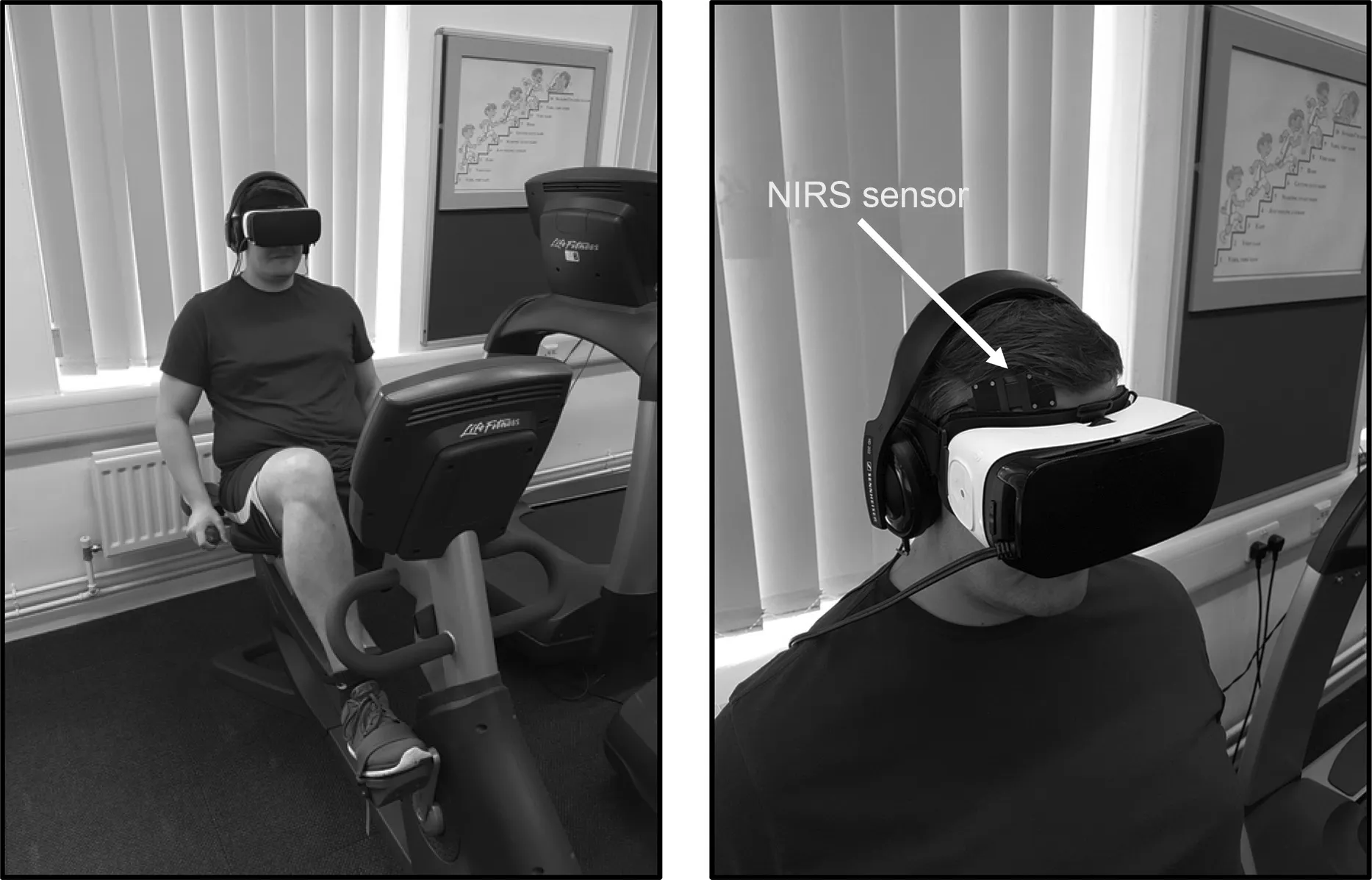
Fig.1. Equipment setup for the high immersion(HI)condition.NIRS=near-infrared spectroscopy.
Oxygenated hemoglobin (O2Hb) and deoxygenated hemoglobin (HHb) in the right dlPFC were recorded using a wireless, continuous-wave NIRS device (PortaLite; Artinis Medical Systems, Elst, the Netherlands). A cranial sensor(58 mm × 28 mm × 6 mm) contained emitters at 760 nm(absorbed primarily by HHb)and 850 nm(absorbed primarily by O2Hb), which were organized in 3 pairs, located at distances of 30 mm, 35 mm, and 40 mm from the detector,respectively.The sensor was positioned at F4 according to the international 10-20 electrode placement system(Fig.1).Data were sampled at 20 Hz continuously from 30 s before the commencement of exercise(i.e.,last 30 s of the warm-up)until the end of 15-min exercise session. The change in the Hb difference ([O2Hb] - [HHb]) compared to the last 30 s of the warm-up (ΔHbDiff) was considered here as an index of cerebral oxygenation.The ΔHbDiff reflects changes in the balance between arterial oxygen delivery and offloading to tissue. As such, this index is considered a surrogate of changes in regional cerebral blood flow and an indication of neuronal activation.
2.2.6. Preference for and tolerance of exercise intensity
The 16-item Preference for and Tolerance of the Intensity of Exercise Questionnaire (PRETIE-Q)30was used to assess the individual difference variables of preference for and tolerance of exercise intensity. The 8-item preference scale includes 4 items that tap preference for high intensity(e.g.,“I would rather have a short, intense workout than a long, lowintensity workout”) and 4 that tap preference for low intensity (e.g., “When I exercise, I usually prefer a slow, steady pace”).Likewise,the 8-item tolerance scale contains 4 items that tap high exercise tolerance(e.g.,“I always push through muscle soreness and fatigue when working out”) and 4 that tap low exercise tolerance (e.g., “During exercise, if my muscles begin to burn excessively or if I find myself breathing very hard, it is time for me to ease off”). Each item is accompanied by a 5-point response scale (ranging from 1(I totally disagree) to 5 (I strongly agree)). In the development samples, Cronbach’s α coefficient of internal consistency ranged from 0.81 to 0.85 for preference and from 0.82 to 0.87 for tolerance.
In our sample, preference and tolerance exhibited noticeably different score ranges, presumably due to the nature of the sample (i.e., low active, overweight adults). Although the range for preference was 27 units (from 12 to 38), extending over 81%of the possible range(i.e.,out of a possible range of 33, from 8 to 40), the range for tolerance was only 15 units(from 16 to 30), extending over 44% of the possible range.This suppression of the range of tolerance scores attenuated the interitem correlations,resulting in unacceptably low internal consistency(α coefficient of 0.62).In contrast,the internal consistency of the preference scale was excellent(α coefficient of 0.94). Therefore, only the preference scores were used in the present study.Preference was used in the analyses as a categorical independent variable based on a median split(low vs.high preference). The median split resulted in 2 groups that differed significantly in preference (t(19)=-5.159,p <0.001,d=2.25)but not tolerance.
2.3. Procedures
2.3.1. Music selection
After being given general guidelines(e.g.,tempo >100 bpm,positive lyrical affirmations),36participants were asked to identify 8-10 tracks and accompanying music videos of their liking that could be used during the experimental exercise session.Participants then rated the musical properties and affective response associated with each track and the accompanying music video,using the Brunel Music Rating Inventory 3 (BMRI-3)36and the Affect Grid (AG),37respectively. Based on a BMRI-3 score >24 (“motivational”) and AG responses indicating that the music video elicited pleasant high activation, an individualized musicvideo playlist lasting for 15 min and comprising 4-5 tracks was created for each participant.
2.3.2. Graded exercise test
Participants completed a graded exercise test on a recumbent cycle ergometer(95R;Life Fitness,Rosemont,IL,USA)to identify the VT and VO2peak. Gas exchange data were collected breath-by-breath with a metabolic cart calibrated before each use (Ultima; MGC Diagnostics Corp., St. Paul, MN,USA). Heart rate (HR) was monitored via telemetry (Polar Electro Oy, Kempele, Finland). The graded exercise test started with a 4-min warm-up,followed by a 14-W/min ramp,beginning from 50 W for women and 71 W for men. The test was continued until volitional termination. The highest 30-s average of VO2was designated as VO2peak. The VT was subsequently identified offline following the 3-method procedure described by Gaskill et al.,38aided by software(WinBreak 3.7;Epistemic Mindworks, Ames, IA, USA).39After recovery from the graded exercise test, participants were familiarized with the experimental protocol, the self-report measures, the experimental setup, and the audiovisual equipment (including the virtual-reality headset) to be used during the experimental sessions.
2.3.3. Experimental exercise sessions
The experimental design was within-subjects, consisting of 3 conditions, scheduled on different days, with a minimum of 48 h separating each condition: (a) LI, (b) HI, and(c)Control.For each condition,participants exercised at the same recumbent cycle ergometer used for the graded exercise test for 15 min (after a 4-min warm-up period) at the same HR that was recorded when the VT occurred during the graded exercise test.Given the low level of cardiorespiratory fitness of the participants, the 15-min exercise duration was chosen, based on pilot testing, to avoid an exaggerated physiological drift over time due to the emergence of a slow component of oxygen uptake. The cycle ergometer was programmed to automatically adjust resistance to maintain this target HR (i.e., HR was held constant both during each condition and across the 3 experimental conditions).
For LI, the audio was delivered via wall-mounted 2-way stereo speakers(Archon 105;FBT,Recanati,Italy)combining a 5-inch woofer and a 1-inch tweeter. Video was shown on a 48-inch (diagonal) television screen (UE48H6400; Samsung,Seoul, Republic of Korea) positioned 4 m away from the participant at eye level. For HI, the audio was delivered via over-the-ear headphones (HD201; Sennheiser, Wedemark,Germany).The video was delivered via a virtual-reality headset (Gear VR; Samsung). This setup is shown in Fig. 1. For both the LI and HI conditions, sound intensity was standardized at 70 dB with a digital sound-level meter smartphone application (Sound Meter; Smart Tools, Daegu, Republic of Korea). For the Control condition, neither audio nor video were provided but, in the interest of ecological validity, the eyes and ears were not occluded.The protocol for all measurements is presented in Fig.2.
The order of the 3 conditions was randomized and counterbalanced to prevent order effects.The sessions were scheduled at the same time of day for each participant to avoid introducing extraneous variance in the dependent variables due to diurnal patterns. Before each condition, participants were instructed to avoid vigorous PA and to follow a similar general pattern of PA and diet.
2.4. Data preprocessing and reduction
Raw optical density data collected with NIRS were converted to estimates of relative concentrations of O2Hb and HHb with the proprietary software Oxysoft Version 3.0.52(Artinis Medical Systems, Elst, the Netherlands) that accompanies the PortaLite device, using the modified Lambert-Beer law. The software uses a differential path length factor of 4.99+0.067(age0.814)based on Duncan et al.40The O2Hb and HHb data were then exported to Matlab (R2018a; The Math-Works,Natick,MA,USA)for further processing(Fig.3).
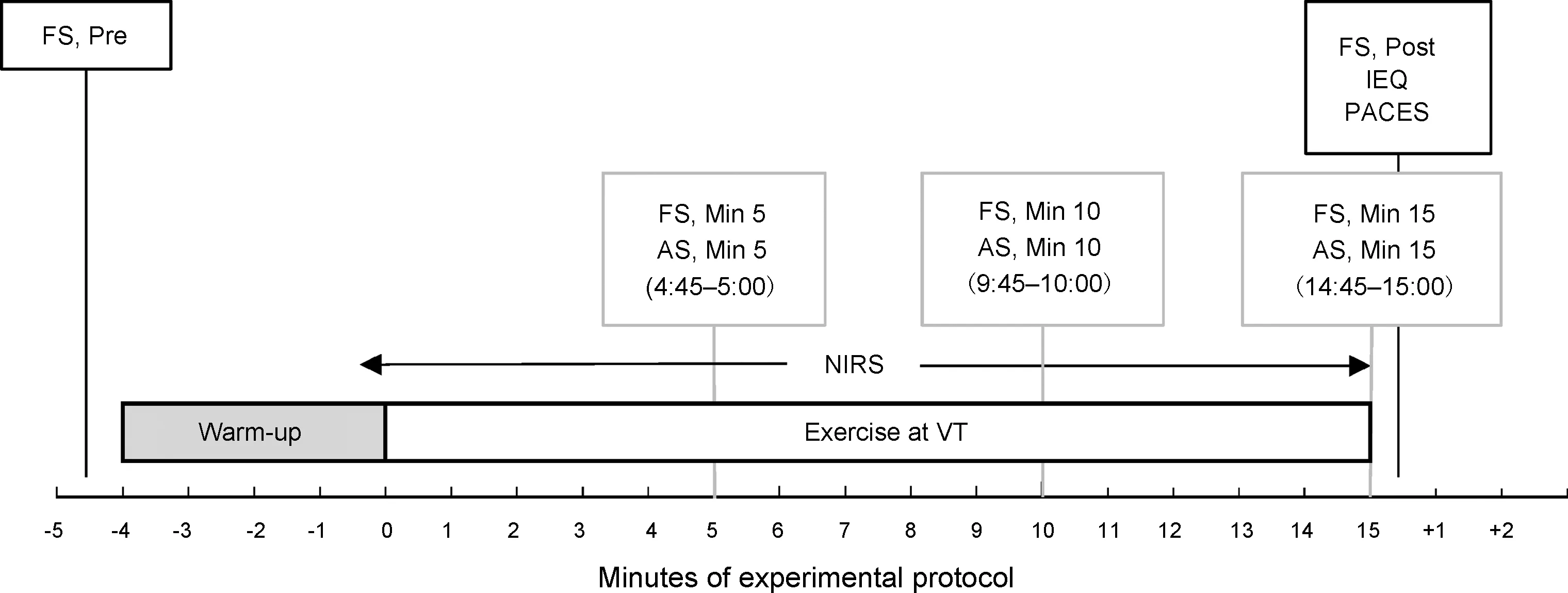
Fig.2. Timing protocol for all measurements. AS=Attention Scale;FS=Feeling Scale;IEQ=Immersive Experience Questionnaire;NIRS=near-infrared spectroscopy;PACES=Physical Activity Enjoyment Scale;VT=ventilatory threshold.
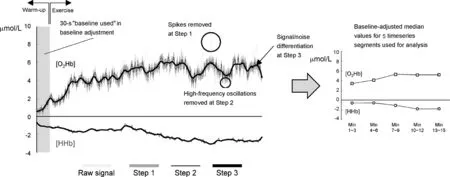
Fig.3. Data preprocessing and reduction steps applied to the hemodynamic data.HHb=deoxygenated hemoglobin;O2Hb=oxygenated hemoglobin.
We first applied the movement artifact removal algorithm from the NIRS Analysis Package (NAP)41to remove spikes (i.e., near-instantaneous signal inflections much larger in amplitude than the typical amplitude of the hemodynamic signal) and correct discontinuities (i.e., baseline shifts). The NAP uses piecewise low-order polynomial interpolation to reconstruct data segments affected by movement artifacts. All 126 timeseries (21 participants ×3 experimental conditions × 2 wavelengths) were visually inspected to ensure that the intended rectifications were properly implemented. Only 3 cases (2.4%) of discontinuities were found.
Second,we removed the low and high parts of the frequency spectrum by applying a third-order Butterworth filter, with bandpass settings of 0.008 and 0.5 Hz. This step was intended to remove oscillations due to heart pulsations(i.e.,≥2 Hz during exercise)and respiration(i.e.,≥0.5 Hz during exercise).
Third, we applied the denoising algorithm of Feuerstein et al.42The goal of this algorithm is to separate the noise from the signal given their differences in amplitude (assuming that the noise has larger amplitude than the underlying hemodynamic signal). The algorithm first calculates the difference between the original signal and a smoothed signal resulting from a quadratic Savitzky-Golay filter and then uses a histogram of this signal difference to iteratively seek the filtering threshold that minimizes the variance overlap between the presumed signal and the presumed noise.
Fourth, for each timeseries, we fit a linear regression through the O2Hb and HHb data representing the last 30 s(600 data points) of the warm-up and considered as the baseline value the estimated value of O2Hb and HHb at the end of the warm-up (600th point). We then expressed all O2Hb and HHb data points as changes from this baseline.
Finally, we divided each timeseries representing exercise periods into five 3-min segments (Min 1-3, 4-6, 7-9,10-12, and 13-15) and calculated the median value of O2Hb and HHb for each segment. These median values were then used to calculate the [O2Hb]-[HHb] difference(ΔHbDiff) that was used in statistical analyses.
2.5. Data analysis
Data were analyzed with repeated-measures analyses of variance (ANOVA), with condition as the within-subjects factor, in the case of variables assessed only once per condition (IEQ,PACES) or with condition (Control, LI, HI) by time repeatedmeasures ANOVAs in the case of variables assessed repeatedly during each condition(AS,FS,ΔHbDiff;Fig.2).In addition,we conducted condition by time ANOVAs for FS and ΔHbDiff with the addition of the between-subjects factor of intensity preference(lowvs.high, based on median split). Violations of sphericity were addressed by using the conservative Greenhouse-Geisser adjustment to the degrees of freedom (decimal degrees of freedom indicate such adjustments). In the case of significant main effects or interactions, follow-upttests were subject to Bonferroni adjustment to prevent the inflation of the Type I error rate due to the multiple comparisons.For convenience,in such cases,the reported probability values represent the observed (uncorrected)pvalue multiplied by the number of comparisons and can, therefore, be judged by the conventional criterion ofp<0.05.Finally,to facilitate the interpretation of hemodynamic changes, correlations between the slope of FS ratings and the slope of ΔHbDiff were examined,both for the entire sample and separately for the low-and high-preference groups.
3. Results
3.1. Manipulation check:attentional focus
A repeated-measures ANOVA of AS data showed only a significant main effect of condition (F(2, 40)=64.765,p=0.000,ηp2=0.76), but no main effect of time (F(2, 40)=0.75,p=0.479, ηp2=0.04), or an interaction (F(4, 80)=0.941,p=0.444, ηp2=0.05) (Fig. 4). Follow-up pairwise comparisons indicated that both LI (p=0.000,d=1.76) and HI (p=0.000,d=2.36) induced more dissociation than the Control. Last, HI induced more dissociation than LI(p=0.025,d=0.54).
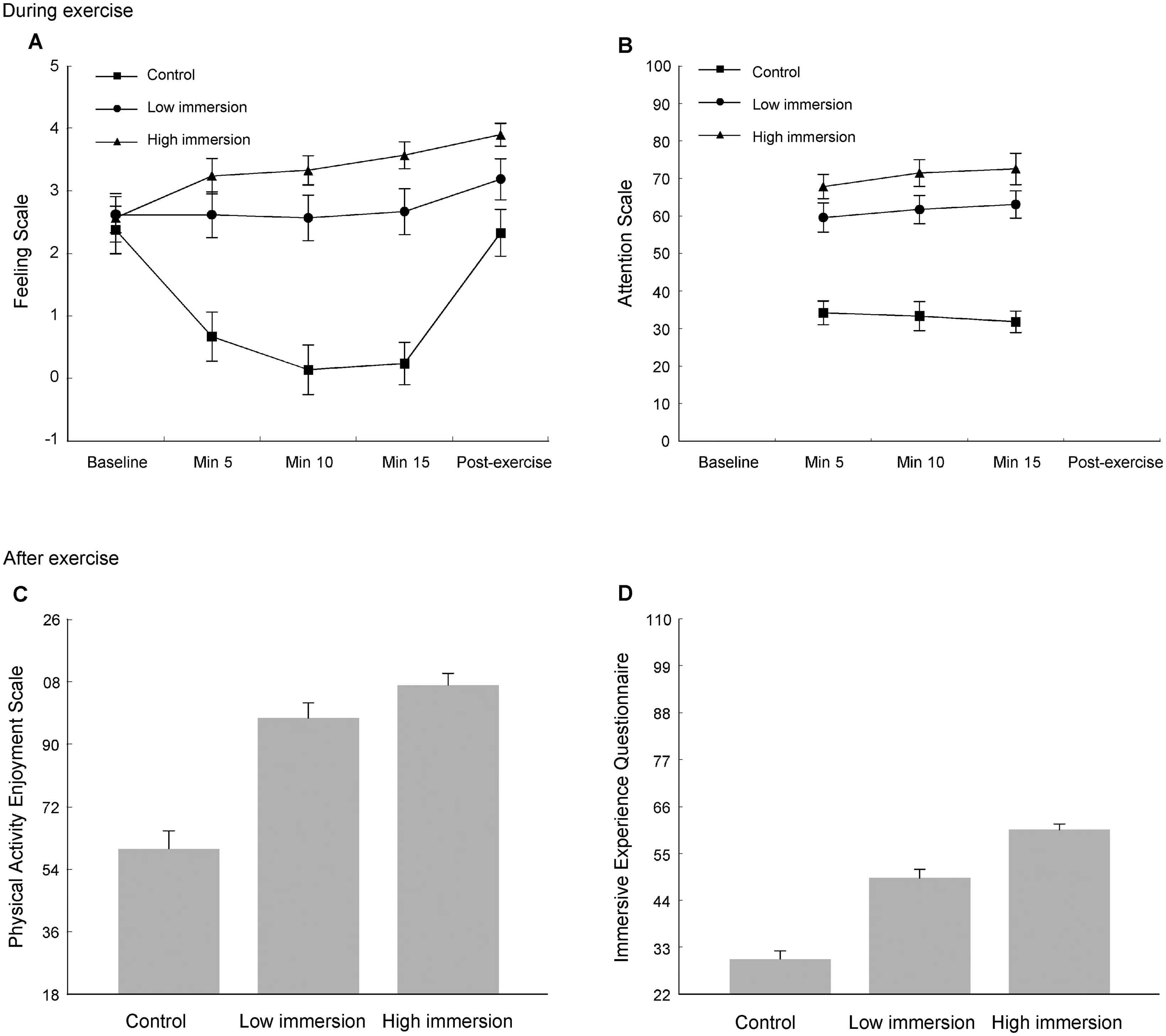
Fig.4. Results of Feeling Scale ratings(A),Attention Scale ratings(B),Physical Activity Enjoyment Scale scores(C),and Immersive Experience Questionnaire scores(D)for the 3 experimental conditions.Note that the Immersive Experience Questionnaire scores for the Control condition partly reflect responses to irrelevant items(i.e.,those referring to music and video)and are shown here merely for reference.The error bars represent standard errors.
3.2. Manipulation check:perceived immersion
The analysis of IEQ data revealed a significant main effect of condition (F(2, 40)=82.423, p=0.000, ηp2=0.81; Fig. 4). Follow-up pairwise comparisons showed differences between all conditions:Control and LI(p=0.000,d=2.10),Control and HI(p=0.001,d=4.07),and LI and HI(p=0.000,d=1.44).
3.3. Primary outcome:affective valence
FS ratings at baseline did not differ between conditions(F(1.540, 30.807)=0.208, p=0.755, ηp2=0.01). The Condition×Time ANOVA showed significant main effects of condition (F(2, 40)=33.774, p=0.000, ηp2=0.63), and time(F(2.134, 42.682)=8.837, p=0.000, ηp2=0.31), as well as a significant interaction (F(3.834, 76.683)=14.786, p=0.000,ηp2=0.43)(Fig.4).During the Control,valence changed over time(F(2.361,47.228)=29.176,p=0.000,ηp2=0.59),exhibiting declines from baseline at Min 5 (p=0.000,d=0.97), Min 10 (p=0.000, d=1.25), and Min 15 (p=0.000, d=1.30). In LI, valence did not change over time (F(2.281,45.620)=1.691, p=0.192, ηp2=0.08). During HI, valence changed over time (F(2.133, 42.663)=4.728, p=0.012,ηp2=0.19), with follow-up comparisons showing a significant increase from baseline to after exercise after Bonferroni correction(p=0.049,d=0.96).
Repeated-measures ANOVAs comparing FS ratings between conditions were significant at all time points after the start of exercise: Min 5 (F(1.516, 30.319)=31.731, p=0.000,ηp2=0.61);Min 10(F(2,40)=52.925,p=0.000,ηp2=0.73);Min 15 (F(2, 40)=54.408, p=0.000, ηp2=0.73); and immediately after exercise (F(2, 40)=8.387, p=0.001, ηp2=0.30). At each time point, the HI resulted in the highest ratings, significantly higher than control at Min 5 (p=0.000,d=1.64), higher than both Control (p=0.000,d=2.14) and LI at Min 10 (p=0.029,d=0.55), higher than both Control (p=0.000,d=2.57) and LI(p=0.014,d=0.65)at Min 15,and higher than Control immediately after exercise(p=0.004,d=1.17).
The Condition × Time analysis with affective valence as the dependent variable was repeated with the addition of the categorical (median split) between-subject factor of exerciseintensity preference. The Preference group factor showed no significant main effect of group or two-way interactions with condition and time. However, the triple Condition × Time ×Preference group interaction closely approached significance(F(8, 152)=1.914,p=0.062, ηp2=0.09; Fig. 5). Notably, the low- and high-preference groups exhibited meaningful (albeit non-significant) differences throughout the Control condition(i.e., at Min 5,d=0.70; at Min 10,d=0.60; at Min 15,d=0.58;and after exercise,d=0.65).
3.4. Secondary outcome:enjoyment
The ANOVA for PACES showed a significant main effect of Condition(F(2,40)=37.150,p=0.000,ηp2=0.65).Followup pairwise comparisons revealed differences between Control and LI (p=0.000,d=1.17) and Control and HI (p=0.000,d=2.36), with higher scores in LI and HI than Control(Fig. 4). The difference between LI and HI (d=0.52) was not significant.
3.5. Secondary outcome:prefrontal oxygenation
The initial Condition×Time analysis for ΔHbDiff showed only a significant main effect of time (F(1.294,25.887)=56.105,p<0.001,ηp2=0.74),but no effect of condition(F(2,40)=0.687,p=0.509, ηp2=0.03), and no Condition× Time interaction (F(2.763, 55.263)=0.842,p=0.469,ηp2=0.04).Repeating the analysis with the addition of the preference group factor showed a significant Condition×Time×Preference group interaction (F(8, 152)=2.130,p=0.036,ηp2=0.10).Follow-up analyses indicated that the low and high preference groups differed only during the Control condition.Specifically,the intergroup differences during the Control condition were (with the low-preference group showing a higher ΔHbDiff)as follows:Min 1-3:p=0.065,d=0.86;Min 4-6:p=0.012,d=1.21;Min 7-9:p=0.009,d=1.27;Min 10-12:p=0.035,d=1.00; and Min 13-15:p=0.057,d=0.88(Fig.5).
3.6. Correlational analyses
The correlations between the slope of FS ratings (Pre to Min 15) and the slope of ΔHbDiff (Min 1-3 to Min 13-15)during exercise were nonsignificant (Control:r=0.050,p=0.829; LI:r=-0.149,p=0.520; HI:r=0.318,p=0.160).Performing the same analyses separately for the low- and high-preference groups revealed 2 distinct patterns, with the low-preference group showing nonsignificant positive correlations and the high-preference group showing significant negative correlations in the Control and LI conditions, and a lack of association in the HI condition (Fig. 6). A statistical comparison of the correlation coefficients derived from the 2 preference groups using Fisher’szmethod showed a significant difference in the Control (z=2.050,p=0.040) and LI conditions (z=2.388,p=0.017), but not in the HI condition(z=1.178,p=0.239).
4. Discussion
The primary purpose of this study was to investigate whether the previously established efficacy of audiovisual stimulation in ameliorating affective responses at exercise intensities proximal to the VT13-15could be further enhanced by the use of low-cost technology that can create a more immersive sensory experience (virtual-reality headset and headphones). We investigated this question in a sample of adults who were low-active and overweight and, therefore,representative of the majority of adults in most industrialized countries.
4.1. Differences in affect and enjoyment:practical implications
Consistent with previous findings on the relation between exercise intensity and affective responses,10we found a large decrease in affective valence during exercise at VT in the absence of audiovisual stimulation. Considering that the VT typically occurs around 50%-60% VO2peakor 60%-70%HRpeak,43namely, close to the commonly recommended“moderate” range of exercise intensity (defined as 46%-63%VO2peakor 64%-76% HRpeak),44this finding may have considerable negative consequences for future PA among lowactive overweight adults.11,12Also in accordance with previous findings,13-15we found that the decrease in affective valence was prevented when audiovisual stimulation was provided through conventional means (i.e., television screen and speakers).Given the dearth of evidence-supported methods for improving the affective experience of exercise for low-active and overweight adults, this finding has meaningful publichealth implications, offering a concrete response to the recently issued challenge9to develop and test methods that can effectively improve the affective response to exercise in different population segments. However, it has been argued that, in order to compete successfully with sedentary alternatives that vie for a portion of discretionary time,it may not be sufficient for exercise to be merely not unpleasant.11,12Instead,it should be pleasure-inducing.
Thus,a novel contribution of the present investigation is the finding that the use of virtual-reality headsets and headphones created a more immersive sensory experience, induced a higher degree of attentional dissociation and ultimately led to an increase in reported pleasure from before to after exercise,as well as a high level of postexercise enjoyment. Compared with the Control condition,the HI condition averaged 3.33 FS units higher at the last Min of exercise.To put this figure into perspective, in a sample with similar characteristics (87%women,low-active,average BMI of 28 kg/m2),a 1-unit higher FS rating during a bout of moderate-intensity walking was cross-sectionally associated with 27-29 additional Min of at least moderate-intensity PA per week and longitudinally associated with 15 additional Min of at least moderate-intensity PA per week 6 months later.6Within the context of recently proposed “dual process” theoretical models, repeated experiences that differ to such a dramatic extent in terms of the pleasure that participants derive, especially at the end of the exercise session,would be predicted to lead to substantial differences in approach-avoidance tendencies, presuming explicit motivational processes (e.g., perceived benefitsvs.barriers,self-efficacy)are held constant.4,5
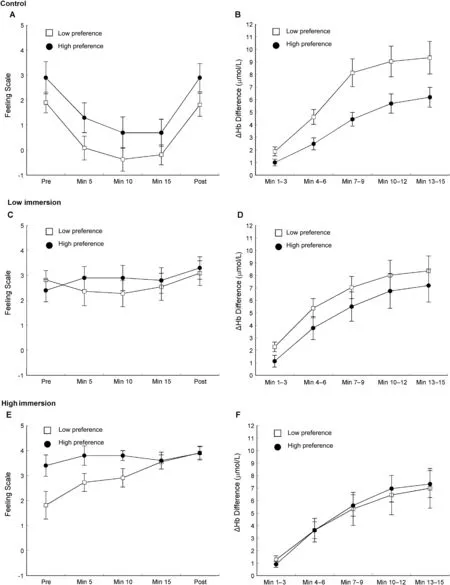
Fig.5. Results of Feeling Scale ratings(A,C,E)and prefrontal oxygenation(ΔHb Difference)changes(B,D,F)of low-and high-preference participants across the 3 experimental conditions.The error bars represent standard errors.
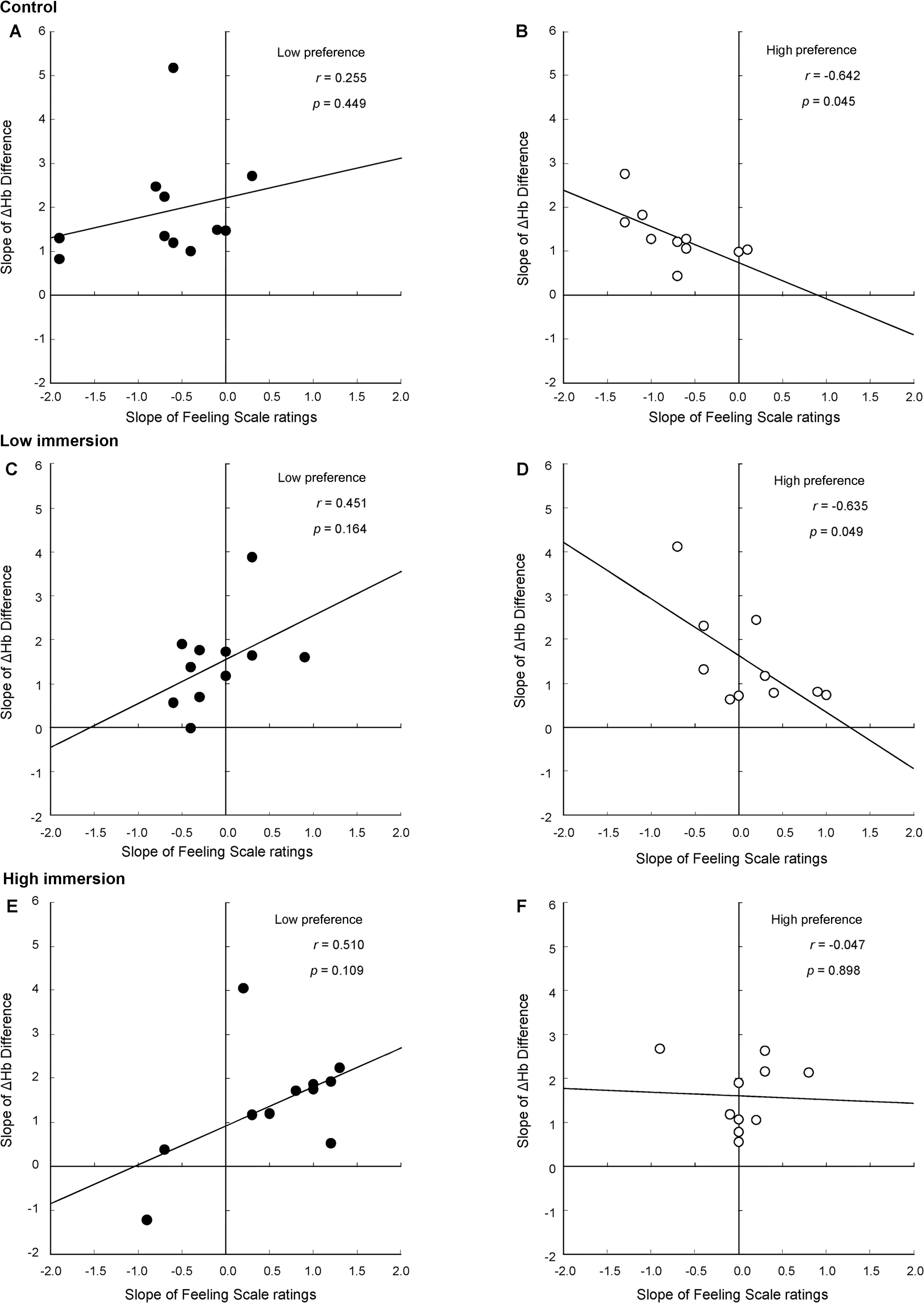
Fig.6. Scatterplots of the correlations between the slopes of Feeling Scale ratings and the slopes of prefrontal oxygenation(ΔHb Difference)during exercise for the low-(A,C,E)and high-preference participants(B,D,F)across the 3 experimental conditions.
Practitioners trying to help participants improve their affective responses to exercise have few evidence-supported options. Besides audiovisual stimulation, these include boosting their self-efficacy through verbal persuasion45and encouraging them to cognitively reframe or reappraise fatigue as a sign of their cardiorespiratory system responding to training.46Compared to such approaches,the use of audiovisual stimulation has several advantages. First, audiovisual stimulation is presumed to improve affect by competing for attentional resources against the salient interoceptive afferents generated by exercise at or above VT.29The crucial factor in this competition seems to be the intensity and engaging nature of sensory stimulation.Therefore,audiovisual stimulation can be applied from the first exercise session,because it does not require special instructions or prior experience. In contrast, intervention approaches that attempt to change cognitive appraisals, such as boosting self-efficacy or reappraising the meaning of the somatic symptoms associated with exercise,target later stages of the information processing pathway and require some degree of training to optimize their effectiveness. Second, the necessary technical infrastructure for audiovisual stimulation already exists in most,if not all,exercise facilities.Third,there is already extensive experimental evidence supporting the use of audiovisual stimulation for enhancing the affective experience of exercise.29,36
Previous work13-15has consistently demonstrated that combining music and video enhances the effectiveness of either modality alone in shifting the attentional focus farther toward dissociation and improving affective responses to exercise performed proximal to the VT. This effect is commonly interpreted as being the result of the combined audio and video engaging 2 senses, thus mounting a more powerful sensory competition against exercise-induced interoceptive afferents.The present work built on this conceptual and empirical foundation. The results reported herein illustrate that the potential of the combined audiovisual stimulation can be further enhanced by taking advantage of emerging low-cost entertainment technologies that create an even more immersive and,therefore, even more dissociative sensory experience. Indeed,we showed that creating such a highly immersive experience can further extend the effectiveness of audiovisual stimulation,making it a meaningful and scalable intervention method for a population that would otherwise typically report declines in pleasure during exercise (i.e., low-active, overweight adults).11,12It should be noted that the integration of smartphones to deliver video images in modern virtual-reality headsets, in conjunction with the ubiquitous availability of headphones and earphones, make the equipment used in the present study relatively inexpensive and thus realistic for large-scale implementation in the field.
4.2. Differences in prefrontal oxygenation:mechanistic implications
Besides highlighting the potential of immersive audiovisual stimulation for practice, the present investigation extended the current understanding of the psychological significance of changes in dlPFC oxygenation during exercise. A previous study that used an energy-and enjoyment-focused mental imagery intervention was successful in improving affective responses during exercise above the VT, but found no difference in left or right dlPFC oxygenation compared to controls.31In the present study,following Karageorghis et al.,29we hypothesized that attentional dissociation by means of audiovisual stimulation would lead to a smaller increase in oxygenation during moderately challenging exercise, presumably because of the “lower level of experienced displeasure and therefore reduced need to cognitively control the displeasure”(p. 288). Despite inducing robust differences in affective responses,our experimental manipulation did not result in a significant Condition×Time interaction for dlPFC oxygenation at the level of the entire sample.Like previous investigations,47,48we found significant increases in dlPFC oxygenation over time,but these did not differ by condition. However, our separate analyses for groups that differed in their preference for exercise intensity (lowvs.high) showed that, in the Control condition,low-preference participants reported substantially lower ratings of affective valence than their high-preference counterparts(even averaging negative ratings at Min 10: -0.364 ± 1.567 and at Min 15: -0.182 ± 1.328) and exhibited significantly higher levels of right dlPFC oxygenation. In contrast, in the 2 audiovisual stimulation conditions,when the ratings of affective valence converged, so did the levels of oxygenation. This pattern seems consistent with our hypothesis29that (a) a lower level of pleasure would be coupled with a higher level of right dlPFC oxygenation, presumably indicative of spontaneous efforts to cognitively regulate the unpleasant experience, and(b) the audiovisual stimulation would attenuate this increase in right dlPFC oxygenation, presumably as an indication of a reduced reliance on prefrontal affect regulation processes.Although these mechanistic suggestions must await direct testing,the finding of the convergence in right dlPFC oxygenation between the low- and high-preference groups from Control to LI,and the eventual elimination of the difference during HI,is intriguing because it parallels the progressive increase in attentional dissociation and perceived immersion across the 3 conditions. It is conceivable that the increasing level of audiovisual stimulation, by shifting the burden of affective regulation from prefrontal-dependent cognitive mechanisms to the earlier (sensory) stages of the information processing pathway, acts as an“equalizer” between individuals who differ in their preference for exercise intensity.
We performed correlational analyses in an effort to investigate the possible mechanistic linkage between changes in prefrontal oxygenation and changes in affect. We did so while being cognizant that the relationship was unlikely to be straightforward. As noted in the Introduction, the relationship is probably bidirectional, such that a higher level of displeasure may stimulate higher activity in the right dlPFC, which,in turn,may facilitate the cognitive downregulation of the displeasure.28We found distinct patterns of oxygenation-affect association in the low- and high-preference groups (Fig. 6).There is a precedent in functional neuroimaging for distinct patterns of activation and cortical-subcortical interactions between groups.For example,studies investigating differences between individuals with and without major depression have shown that, unlike healthy participants, those with depression exhibit increases in prefrontal activity that are uncoupled from activity in the amygdala while viewing negative affectively charged images.49,50Following a similar line of reasoning,we noted that, in the presence of an affective challenge(i.e.,during the Control and LI conditions, in which nearly all or onehalf of the participants,respectively,exhibited negative slopes of affective valence over the duration of the exercise session),only the high-preference participants showed increases in prefrontal oxygenation that were proportional to the severity of the displeasure.This difference may suggest that,when cognitive resources are needed to regulate increasingly unpleasant affective responses, the high-preference participants may be more able to do so than their low-preference counterparts.Therefore, the ability to raise right dlPFC activity in proportion to the degree of affective challenge may be a biological substrate of individual differences in preference for exercise intensity. Once again, during the HI condition, in which there was no affective challenge(i.e.,all but 2 participants exhibited non-negative slopes of affective valence over time), the immersive audiovisual stimulation appears to have acted as an“equalizer”, eliminating the intergroup difference in the association between changes in prefrontal oxygenation and changes in affect.We interpret this finding as being consistent with the suggestion that,under immersive audiovisual stimulation,the regulation of affect does not need to rely on cognitive resources because the effectiveness of the method likely relies in its ability to compete against afferent interoceptive symptoms at the level of sensory input.It is important to remember that,in all 3 conditions,the intensity of exercise was automatically held constant (by the HR-controlled exercise cycle ergometer), and we can therefore assume that the exerciseinduced interoceptive symptoms did not vary between conditions.
Although numerous studies have assessed dlPFC oxygenation changes during exercise,51,52the full implications of these changes have remained enigmatic because it is unclear how the cognitive functions typically attributed to the dlPFC(i.e., error monitoring, executive control, working memory)could be related to exercise experiences or exercise performance. Herein, we have highlighted a function of the dlPFC that is commonly overlooked in the exercise science literature,namely, the inhibitory control over the amygdala and the cognitive downregulation of negative affect.17,18Given that negative affective responses are intrinsically intertwined with exercise performed above the VT,10it is reasonable to postulate that the dlPFC,particularly in the right hemisphere,would also be involved in the regulation of the displeasure and sense of exertional physical fatigue associated with high-intensity exercise.51This finding is arguably an important conceptual contribution of the present study.
4.3. Limitations and future research
A possible alternative explanation for the positive pattern of affective responses in the HI condition is that the use of the virtual-reality headset induced a novelty effect; participants likely had at least some prior experience with exercise without audiovisual stimulation, as well as with audiovisual stimulation provided through a television screen and speakers.In contrast, the virtual-reality headset was a novelty, raising the possibility that the effects observed here may be associated with the initial excitement of trying out a new technological contraption and may, therefore, be ephemeral. Although the possibility of a novelty effect and, therefore, an intervention whose efficacy may wear off over time cannot be fully discounted, it should be pointed out that (a) participants were introduced to the virtual-reality headset during the initial visit to the laboratory,with the express purpose of allowing habituation to occur, and (b) we found strong effects for attentional dissociation and perceived immersion,which are the variables theorized to mediate the effects of the virtual-reality headset.
Although a growing literature linking affective responses to bouts of exercise with long-term PA participation allows us to reasonably infer that the intervention tested here may have implications for behavior in the long run,8,9the present study compared only responses to single sessions of exercise.Therefore, the long-term sustainability of the effects found here remains to be established. Extension of this research to adults with obesity,11,12as well as with samples with balanced representation of the 2 sexes,should also be pursued.
5. Conclusion
Music and video delivered through a virtual-reality headset and headphones induced stronger attentional dissociation and sense of immersion and further improved the efficacy of music and video delivered through a television screen and speakers in ameliorating affective and enjoyment responses to exercise at VT among low active,overweight adults. The examination of prefrontal hemodynamics during exercise using NIRS suggested that immersive audiovisual stimulation may decrease the reliance on prefrontally mediated cognitive resources to regulate affective declines during exercise, particularly among individuals with a low preference for exercise intensity. Overall,the results indicate that using emerging low-cost technology to deliver audiovisual stimulation during exercise may be a viable and effective way to enhance the affective experience of exercise for low-active and overweight individuals.
Acknowledgments
The authors thank the participants,without whose help this project would not have been possible. LJ acknowledges Sheffield Hallam University for financial support that allowed for the purchase of equipment used in this study (NIRS, virtualreality headset).
Authors’contributions
LJ contributed to the conceptualization of the study,designed, pilot-tested, and refined the methods, collected all the data, performed the statistical analyses pertaining to the self-reported outcomes, and developed the first draft of the manuscript; PE contributed to the conceptualization of the study, developed the software used for the determination of the VT, performed the preprocessing and statistical analyses pertaining to the NIRS data,and revised the manuscript.Both authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
Both authors declare that they have no competing interests.
 Journal of Sport and Health Science2019年4期
Journal of Sport and Health Science2019年4期
- Journal of Sport and Health Science的其它文章
- Journal of Sport and Health Science Guide for Authors
- Standardization of exercise intensity and consideration of a dose-response is essential.Commentary on“Exercise-linked FNDC5/irisin rescues synaptic plasticity and memory defects in Alzheimer’s models”,by Lourenco et al.,published 2019 in Nature Medicine
- Could sport be part of pediatric obesity prevention and treatment?Expert conclusions from the 28th European Childhood Obesity Group Congress
- Editorial re:Could sport be part.....by Ring-Dimitriou et al.
- Exercise,cognitive function,and the brain:Advancing our understanding of complex relationships
- Author biographies