
Incidence, distribution of histological subtypes and primary sites of soft tissue sarcoma in China
2019-09-29 06:27:44ZhixunYangRongshouZhengSiweiZhangHongmeiZengHeLiWanqingChen
Cancer Biology & Medicine 2019年3期
Zhixun Yang, Rongshou Zheng, Siwei Zhang, Hongmei Zeng, He Li, Wanqing Chen
National Cancer Center, National Clinical Research Center for Cancer, Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China
ABSTRACT Objective: Soft tissue sarcomas (STSs) are rare malignancies deriving from mesenchyme. In this study, we reported the epidemiology of STS in China using population-based cancer registry data.Methods: In 2017, qualified data from 339 cancer registries were included in the national database. All STS cases were retrieved based on the morphological and topographical codes of International Classification of Diseases for Oncology, and were categorized into different histological subtypes and primary sites accordingly. Nationwide new STS cases were estimated using incidence rate of STS and the national population, and were reported for gastrointestinal stromal tumor (GIST) and STSs other than GIST separately by sex and region. Distribution of histological subtypes and primary sites of STS were calculated, as well as primary sites of GIST.Results: Approximately 39,900 new STS cases occurred nationwide in China in 2014, accounting for 1.05% of overall cancer incidence. The crude incidence rate was 2.91/100,000 and generally increased with age. An overall female predilection was found.GIST was the most common histological subtype, followed by nerve sheath tumor and malignant peripheral nerve sheath tumor,leiomyosarcoma, liposarcoma, and fibrosarcoma. About 67.5% of GIST occurred in stomach while 1.4% were recorded outside the gastrointestinal tract. Connective, subcutaneous and other soft tissues were the most common primary site, of which extremities were the major subsite.Conclusions: The burden of STS is not serious in China relatively. However, due to their histological and topographical complexity, STSs should not be unnoticed, and more basic and clinical studies should focus on STSs.
KEYWORDS Soft tissue sarcoma; incidence; gastrointestinal stromal tumor; epidemiology; China
Introduction
Sarcomas, consisted of soft tissue sarcomas (STSs) and bone sarcomas, are a heterogeneous group of mesenchymal malignancies that can develop at any age, comprising approximately 1% of all adult malignancies and 15% of pediatric malignancies1. Compared with other common cancer types, STSs can develop at almost any anatomical sites2, and are more prone to occur at childhood3. Although the etiology of STSs is still unclear, known risk factors include inherited syndromes, chemical and radiation exposures, viral infections and genetic mutations4,5.
Due to their rarity, STSs are always outnumbered by carcinomas in many primary sites, therefore not reported in most researches categorizing cancers with the International Classification of Diseases6. In United States, it is estimated that 13,040 new cases and 5,150 deaths were caused by STSs in 2018, representing 0.75% of overall cancer incidence and 0.84% of overall cancer mortality7. In Europe, nearly 23,600 new STS cases rose annually and the crude incidence rate was 4.7 per 100,0006. In UK alone 3,300 new cases were diagnosed each year, with about 90 cases in children under 15 years oldd4. So far, most national and subnational epidemiological researches on the burden of STSs were carried out in developed countries3,8-15.
Of all histological subtypes of STSs, gastrointestinal stromal tumor (GIST) was categorized as STS instead of digestive system cancer for the first time in the 2013 World Health Organization (WHO) Classification5,16. Compared with other common cancer types in gastrointestinal tract,GIST starts in different types of cells and needs different types of treatment. Therefore, GIST was either treated as an entity equal to STSs and bone sarcomas6,17, or reported separately from other STS subtypes18-20in some researches.The crude incidence rate of GIST was 1.1-1.4 per 100,000 according to French and Spanish researches20,21. Stomach is the most common site for GIST21while there are some extremely rare tumors that arise outside the gastrointestinal tract but show the features of GIST. These tumors were therefore named extra-GIST22. Similar to the condition of overall STSs, few researches on the epidemiology of GIST and extra-GIST were carried out in developing countries.
With world’s largest population, 23.7% of the global new cancer cases were estimated to occur in China in 201823.However, little is known about the incidence of STS in this country. In order to have a comprehensive understanding on the cancer burden of STS in China, in this study we described the distribution of histological subtypes and primary sites of STS using updated data from 339 population-based cancer registries. Estimation of the incidence of STS in the whole Chinese population was made as well and was reported for GIST and STSs other than GIST (non-GIST STSs) separately.We also described the distribution of GIST and explored the proportion of extra-GIST.
Materials and methods
Cancer registry data source
By 30th August 2017, 449 cancer registries from 31 provinces in China submitted cancer registry data for 2014 to National Central Cancer Registry of China (NCCRC).Local population data were provided along with the cancer data. After quality control based on the criteria of Chinese Guideline for Cancer Registration, data from 339 registries met the criteria and were finally included in this analysis.Among them, 129 were located in urban areas (covering a population of 144,061,915) and 210 were in rural areas(covering a population of 144,181,432). The overall population covered by these 339 cancer registries was 288,243,347 (146,203,891 men and 142,039,456 women),accounting for 21.07% of the national population that year.
All cancer cases were coded according to the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) and the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Of all STS cases, the proportion of morphology verified cases(MV%) was 84.97%. More information on the national cancer registry program and data quality control procedure could be found elsewhere24,25.
Data extraction, classification and statistical analysis
STS cases in the 339 registries were retrieved and categorized into different histological groups according to their ICD-O-3 morphological codes as shown in Table 1 based on a previous study12. The primary site of a case was defined by the ICD-O-3 topographical code. Cases with topographical codes being C40-C41 were deleted to exclude sarcomas in bones, joints and articular cartilages.
Crude incidence rates were calculated by area(urban/rural), sex (male/female) and age group (0, 1-4, 5 to 80 by 5 years, 85+) based on the retrieved cases. To estimate the number of new STS cases in the whole country, incidence rates stratified by area, sex and age group were multiplied by corresponding nationwide population in each stratum.National population data were obtained from Nation Bureau of Statistics. Chinese population in 2000 and World Segi’s population were used for age-standardization.
The estimated nationwide incidence was reported for overall STSs, GIST, and non-GIST STSs separately. The distribution of histological subtypes was reported by sex and age group (0-19, 20-64, and over 65 years old) in order to reveal the sex and age predilection. Primary sites of all STS cases were classified into 14 groups and reported by sex.
Results
Incidence of soft tissue sarcoma
Approximately 39,900 new STS cases (19,200 men and 20,700 women) occurred nationwide China in 2014, as shown in Table 2. The crude incidence rate was 2.91/100,000(2.72/100,000 in men and 3.11/100,000 in women), while the age-standardized rate by Chinese population (ASRcn) and world population (ASRwld) were 2.21 and 2.13 per 100,000,respectively.
There were 5,700 GIST cases (3,200 men and 2,500 women) nationwide in 2014, accounting for about 14.3% of the overall STSs. The crude incidence rate was 0.42/100,000(0.45/100,000 in men and 0.38/100,000 in women). On the other hand, approximately 34,200 non-GIST cases (16,000 men and 18,200 women) were diagnosed, accounting for about 85.7% of the overall STSs. The crude incidence rate was 2.50/100,000 (2.27/100,000 in men and 2.73/100,000 in women). The incidence of overall STSs and non-GIST STSs were higher in women than in men in urban and rural areas,whereas the incidence of GIST was higher in men than in women in both areas.
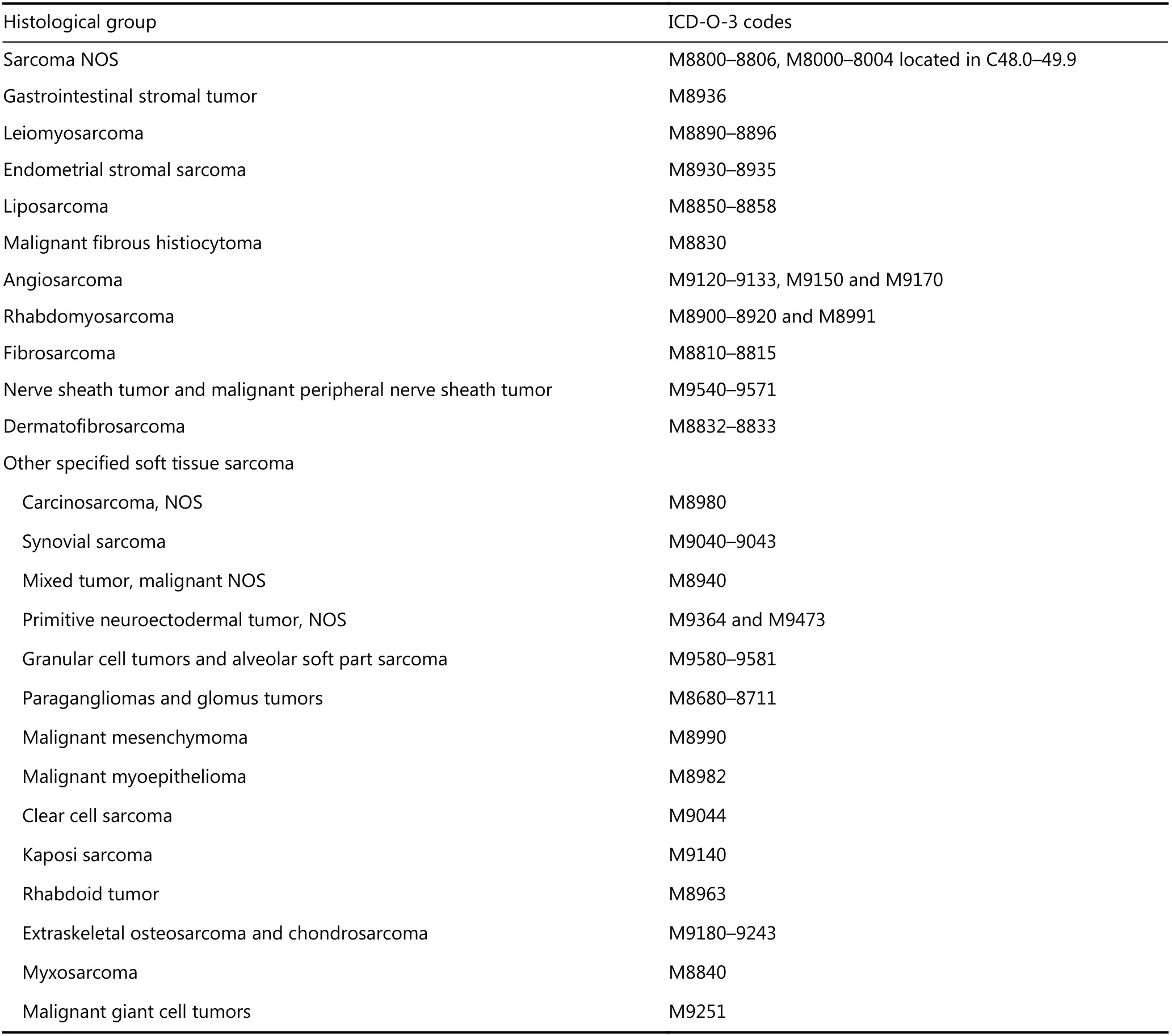
Table 1 Histological subtypes by ICD-O-3 morphological codes
As shown in Figure 1, the age-specific incidence rates of overall STSs and non-GIST STSs were the lowest in children aged 5 to 9 years, increased dramatically after 35 years old and peaked at 75-79 years old in women and 80-84 years old in men for overall STSs, and 80-84 years old in both sexes for non-GIST STSs. As for GIST, the age-specific incidence rate was unstable due to the scarcity in individuals under 25 years old. The rate increased dramatically after 45 years old and peaked at 75-79 years old in women and 70-74 years old in men.
Distribution of histological subtypes
As shown in Table 3, altogether 8,475 new STS cases (4,033 men and 4,442 women) were reported from the 339 cancer registries. The most common histological subtype was GIST(14.38%), followed by nerve sheath tumor and malignant peripheral nerve sheath tumor (MPNST) (12.48%),leiomyosarcoma (5.97%), liposarcoma (5.75%), and fibrosarcoma (5.73%).
Overall male/female ratio was 0.9, indicating a female predilection. Highest ratios were found in malignant myoepithelioma, clear cell sarcoma, malignant fibrous histiocytoma and primitive neuroectodermal tumor NOS,whereas lowest ratios were found in endometrial stromal sarcoma, granular cell tumors and alveolar soft part sarcoma,leiomyosarcoma, carcinosarcoma NOS, and myxosarcoma.
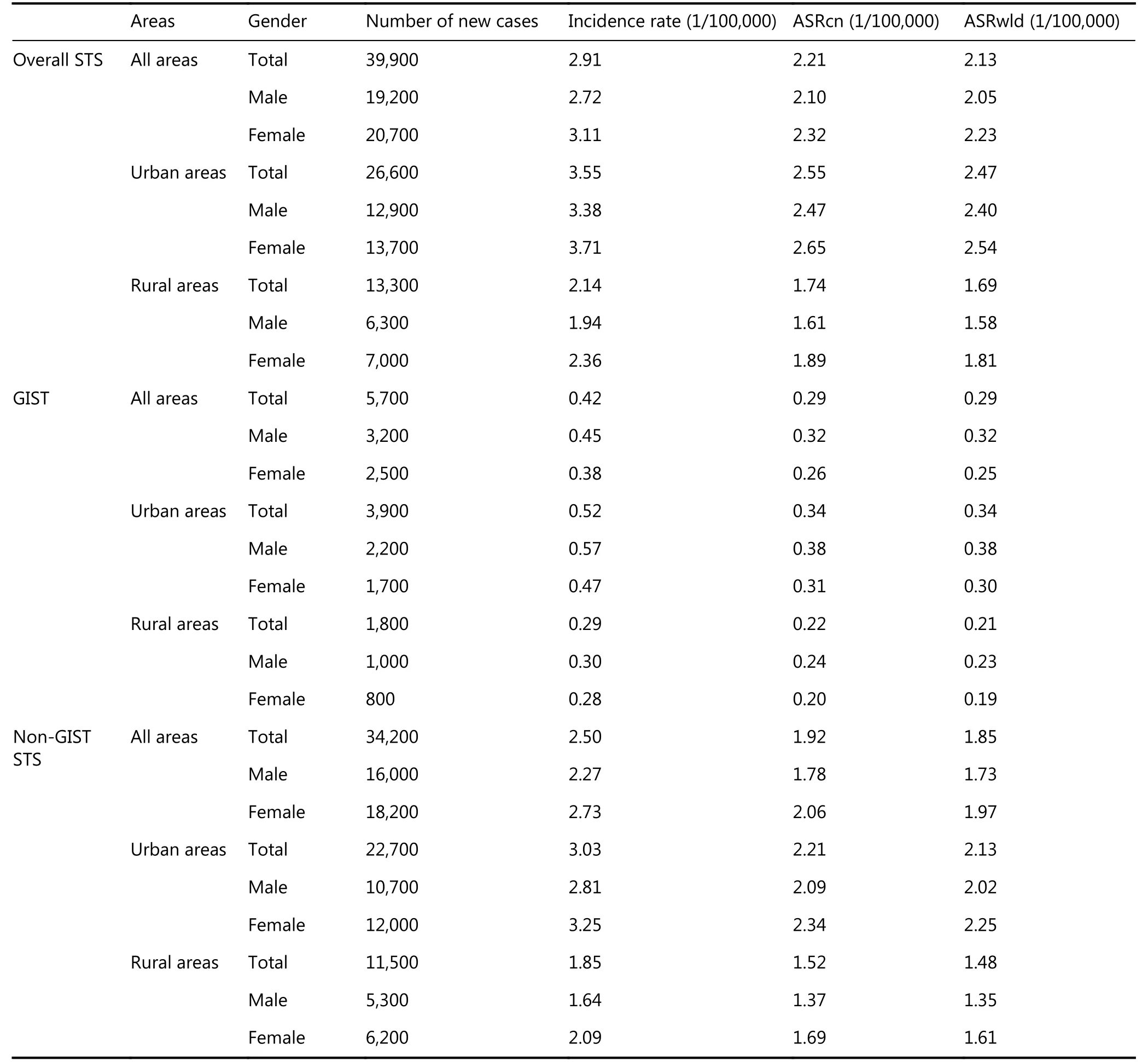
Table 2 Estimated number of nationwide new cases of soft tissue sarcomas in China, 2014
Children and adolescents under 20 years old accounted for 3.12% of all STS cases, while adults aged 20-64 years and over 65 years accounted for 64.64% and 32.24%, respectively. In major histological subtypes, children and adolescents represented 44.63% of all rhabdomyosarcoma cases, whereas endometrial stromal sarcoma (84.13%) and nerve sheath tumor and MPNST (80.72%) occurred mainly in adults aged 20 to 64 years, and proportions of malignant fibrous histiocytoma (47.93%) and GIST (43.07%) were relatively high in elders above 65 years old.
Distribution of primary sites
As shown in Table 4, more than 22% of STSs were located in the connective, subcutaneous and other soft tissues, of which 574 were in lower limb and hip (lower extremities), 234 were in upper limb and shoulder (upper extremities). About one-fifth of STSs occurred in digestive organs, of which 952 were in stomach,294 were in small intestine, and 153 were in liver. Retroperitoneum and peritoneum and eye, brain and other parts of the central nervous system both accounted for nearly 14% of all STSs.
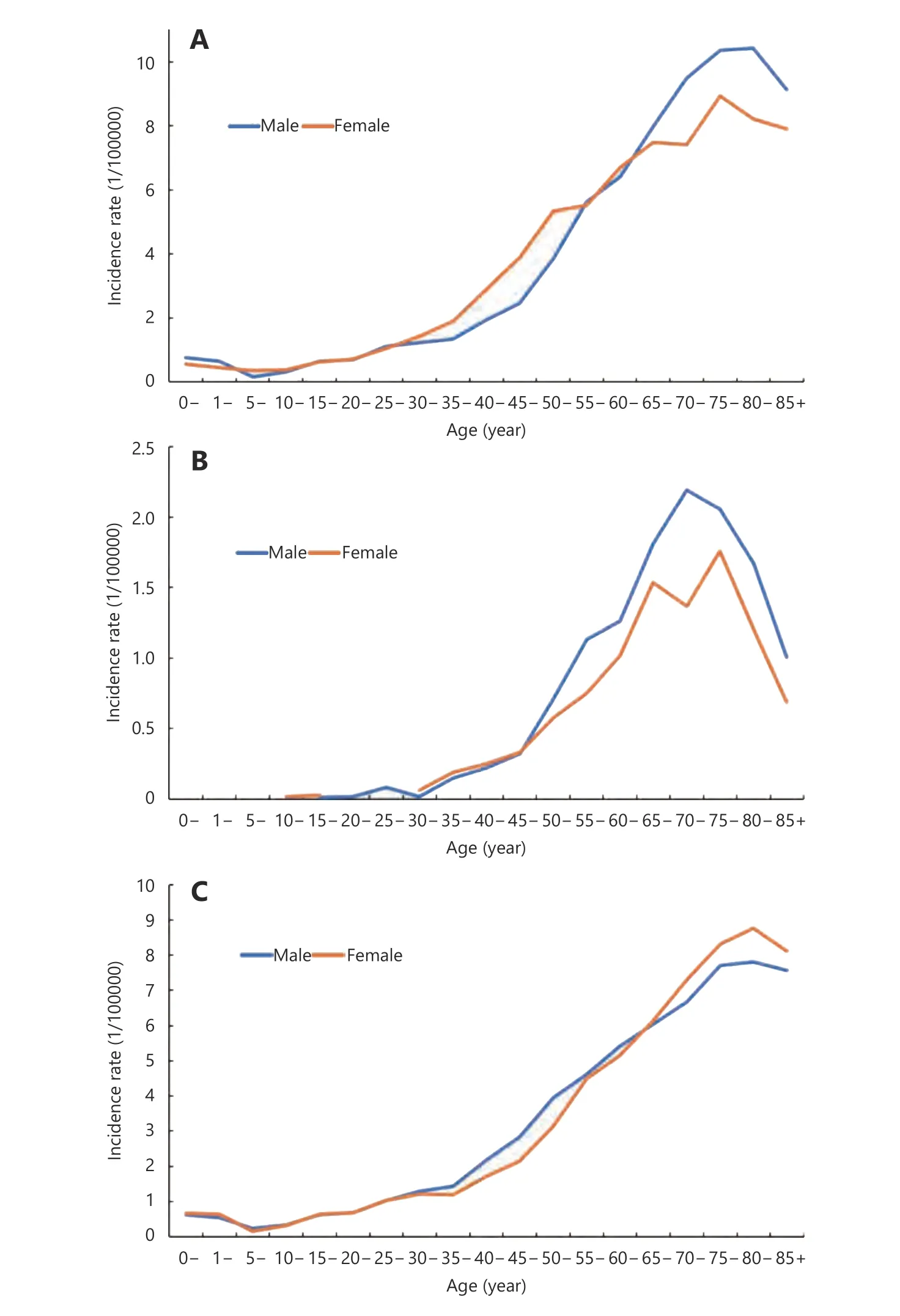
Figure 1 Age-specific incidence for soft tissue sarcoma by sex in China, 2014. (A) All soft tissue sarcoma. (B) Gastrointestinal stromal tumor. (C) All soft tissue sarcoma excluding gastrointestinal stromal tumor.
As shown in Table 5, of all GIST cases, 98.6% arose in digestive organs. Stomach was the most common site(67.51%), followed by small intestine (20.92%), other digestive organs (4.59%) and rectum (3.12%). Extra-GIST was found in retroperitoneum and peritoneum, bronchus and lung, soft tissues, thyroid gland, and other unknown sites, representing 1.4% of all GIST cases.
Discussion
In this study, using population-based cancer registry data, we found that nearly 39,900 new STS cases (5,700 GIST and 34,200 non-GIST) were diagnosed nationwide in China in 2014, representing 1.05% (0.90% in male, 1.23% in female)of all cancer incidence24, larger than the proportion (0.75%)in United States7. Crude incidence rates of STSs and GIST were 2.91 and 0.42 per 100,000 respectively, lower than the corresponding rates in western countries (4.7 and 0.78 per 100,000)6,19.

Table 3 Histological distribution of soft tissue sarcomas by sex and age in China, 2014
Incidence of STS in China generally increased with age.The rate in Austria showed similar trend but peaked and dropped at younger ages14. Unlike carcinomas, STSs comprise a large proportion of pediatric malignancies and are an important cause of death in adolescents and young adults3,4. In our study, 3.1% of all STSs occurred in individuals aged 0 to 19 years, whereas in United States and Japan, corresponding proportions were 5.6% and 6.7%,respectively3,12. Rhabdomyosarcoma was the only entity with a median age < 20 years in United States. It was also the most common subtype in people under 20 years old in these three studies.
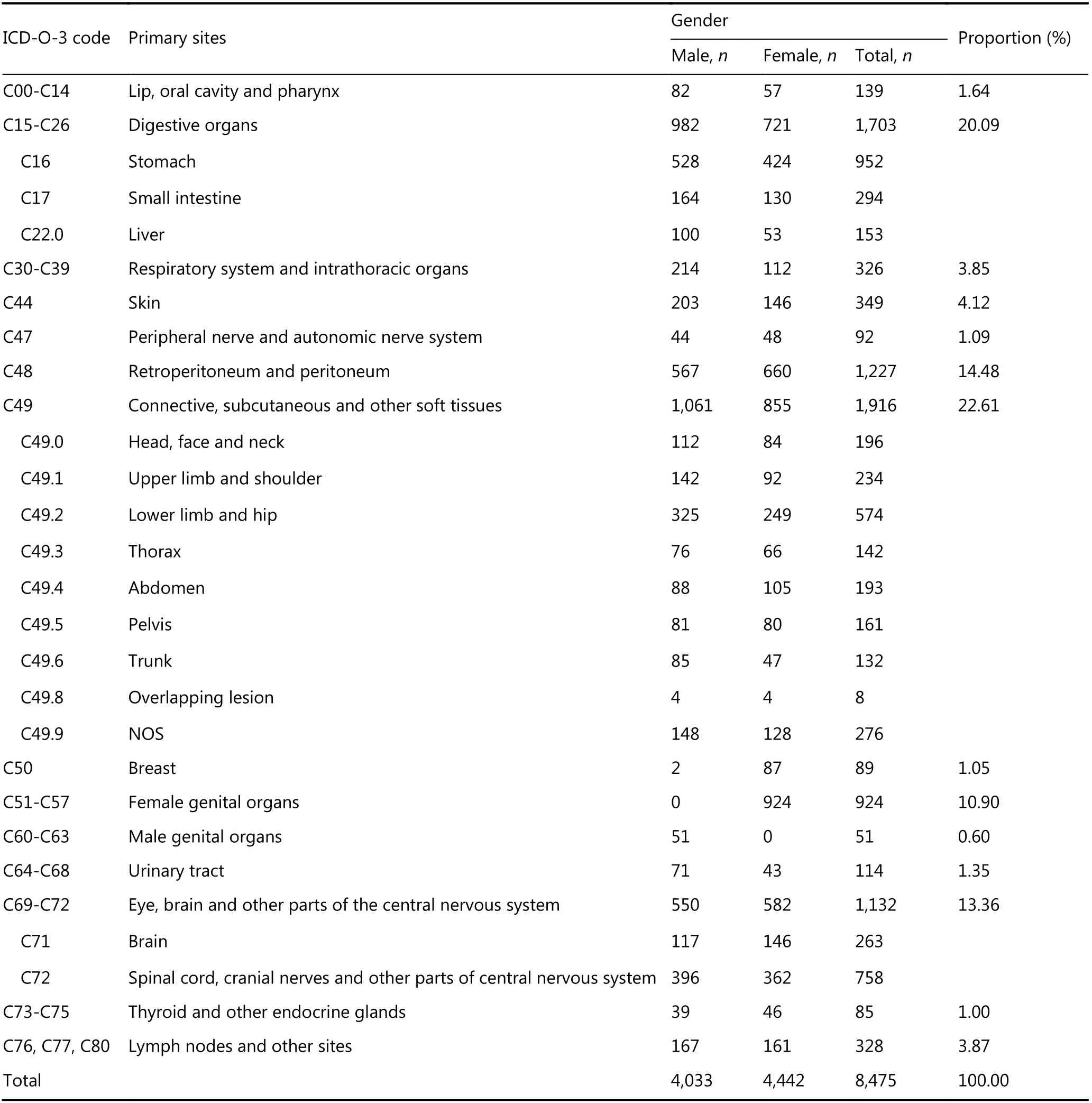
Table 4 Distribution of primary sites of soft tissue sarcomas by gender in China, 2014
Unlike most carcinomas, to which men are prone to develop, contradictions remained as for the major gender of STS patients. In Europe, there were more female patients6,14,while in Korea and Taiwan China, results showed the opposite13,26. Similar to these Asian results, men outnumbered women in most primary sites and histological subtypes in our study. However, there were more female patients due to the numerous cases in breast and female genital organs, and subtypes like leiomyosarcoma, which occurs mainly in genital organs, bladder and uterus.
GIST was the most common histological subtype in Chinese population, as was found in Europe15. In France,16.7% of the identified sarcoma cases were GIST. French distribution of GIST was similar to our study, with 61% and 27% arose in stomach and small intestine, respectively. The proportion of extra-GIST nevertheless was greater because5% of GIST arose in peritoneum. This extravagant percentage can be partly explained by the small sample size21.In contrast to our and American results19, GIST showed a female predilection in France. In United States, there were relatively less GIST in stomach (55.3%) and more in small intestine (28.7%), while the proportion of extra-GIST was 3.0%, also larger than our result19.
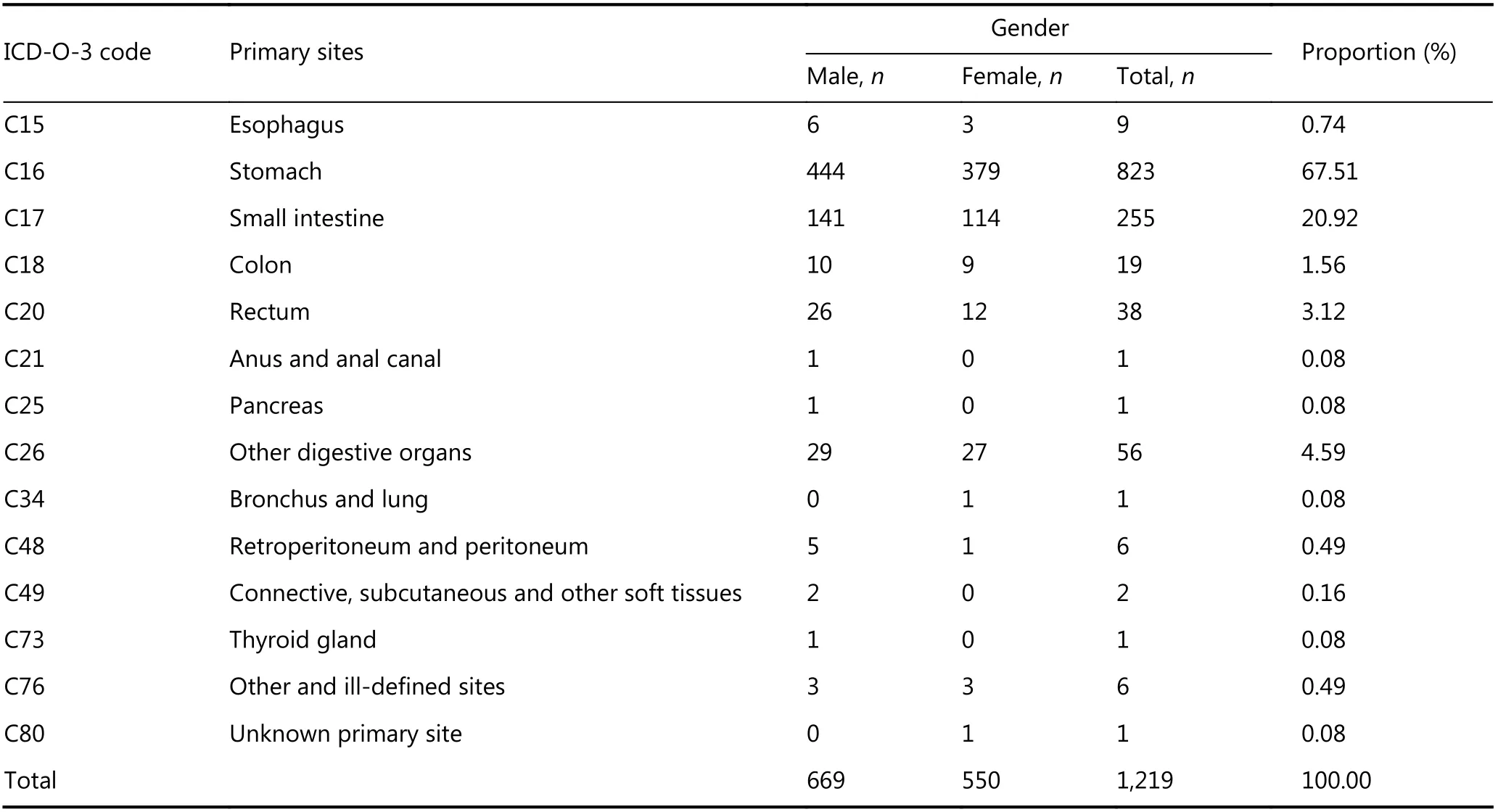
Table 5 Distribution of primary sites of gastrointestinal stromal tumor by sex in China, 2014
Kaposi sarcoma, accounting for less than 0.6% of all STSs,was only a minor subtype in China and even less common(0.2%) in Japan12, whereas it had very high incidence in African countries27. Kaposi sarcoma is also the most common subtype (31.7%) in United States3. This could be explained by the relatively low prevalence of HIV in East Asia because Kaposi sarcoma is strongly related with immune suppression28.
Other than Kaposi sarcoma, common subtypes in United States were fibrohistiocytic tumors (30.4%) and leiomyosarcoma (27.4%)3. Even after the inclusion of GIST into the leiomyosarcoma category, corresponding proportions in our study, which were 5.12% and 20.35%respectively, were still smaller than these results. In Japan,leiomyosarcoma (28.1%) was the most prevalent subtype,followed by liposarcoma (9.6%), and malignant fibrous histiocytoma (9.0%)12. In contrast, nerve sheath tumor and MPNST is far more prevalent in China, representing more than 12% of all STSs in our study, compared with 3.5% in Japan and 4.6% in United States.
In terms of primary sites, according to American Cancer Society, STSs can develop in soft tissues, internal organs as well as retroperitoneum29. However, the WHO classification did not include internal organs as primary sites for STSs and listed only the extremities, trunk wall, and retroperitoneum5.Therefore, STSs were recognized as an entity with a variety of primary sites in some studies10-12,14, while in others, STSs were more confined and sarcomas in internal organs were categorized as visceral sarcoma separately8,15.
In this study, we used the classification of American Cancer Society, and found that connective, subcutaneous and other soft tissues was the most common site. Delving into more specific topographic categories, lower extremity was the most common subsite, and the number of cases in lower extremity was 2-3 times of that in upper extremity. Results in Korea13, Japan12,30and Europe15further proved ours.Digestive organs, which was recognized as visceral sarcomas in some studies, were the second most common site for STSs,of which the majority was GIST. We found 17 extremely rare extra-GIST cases based on this large population-based study.This will provide valuable epidemiological evidence for further researches.
STSs have more than 70 histological subtypes15. Together with the various primary sites, they make up a large number of combinations that vary tremendously in terms of survival and clinical treatment, which means that same histological subtype in different sites may need completely different therapies6,31. The rarity of STSs and the even smaller number of cases in each combination further add to the difficulty faced by researchers and physicians. Although the national survival of STSs in China is still unknown, overall five-year survival rate of STSs in developed countries ranged from 55%to 78%4,8,30, indicating a relatively optimistic prognosis.Nevertheless, survival may vary tremendously (48.0%-99.5%) between different subtypes30, and would worsen along with ageing3. This, together with its scarcity, emphasize that more attention should be paid to this less noticed disease and its patients.
Some limitations of this study should be noticed. First,probable methodology bias remains. We retrieved data based on ICD-O-3 morphological codes in this study because STSs can arise in almost every part in the human body, making topographical codes less useful than in the analysis of carcinomas. Nevertheless, according to a European study,nearly 42% of the first histological diagnoses of STSs were inaccurate. This heterogeneity and discrepancy can lead to misreport on subtype incidence4,32and consequently bias the results on the epidemiology of STSs. Second, proportion of sarcoma NOS was too high compared with Japanese results12,and MV% was lower than that in Europe6, indicating a necessity to strengthen the pathological diagnosis especially in rural China.
Conclusions
This study is the first in China mainland to report the nationwide incidence of STS as well as the distribution of histological subtypes and primary sites. As a group of rare malignancies in China, STSs are more common in children than carcinomas. With numerous histological subtypes and primary sites, tremendous variations remain in STSs, which impose an arduous challenge to both medical researchers and doctors and emphasize more attention.
Acknowledgements
We sincerely appreciate the effort of every cancer registry for the data collection, data sorting, data verification and database creation. This study was supported by CAMS Innovation Fund for Medical Sciences (CIFMS) (Grant No.2016-12M-2-004) and Ministry of Science and Technology(Grant No. 2014FY121100).
Conflict of interest statement
No potential conflicts of interest are disclosed.
 Cancer Biology & Medicine2019年3期
Cancer Biology & Medicine2019年3期
- Cancer Biology & Medicine的其它文章
- TNFα inhibitor C87 sensitizes EGFRvIII transfected glioblastoma cells to gefitinib by a concurrent blockade of TNFα signaling
- A four-gene signature-derived risk score for glioblastoma:prospects for prognostic and response predictive analyses
- Prediction of cervical lymph node metastases in papillary thyroid microcarcinoma by sonographic features of the primary site
- Decrease in the Ki67 index during neoadjuvant chemotherapy predicts favorable relapse-free survival in patients with locally advanced breast cancer
- Prevalence and clinical significance of pathogenic germline BRCA1/2 mutations in Chinese non-small cell lung cancer patients
- Incomplete radiofrequency ablation provokes colorectal cancer liver metastases through heat shock response by PKCα/Fra-1 pathway