
Misinformation on salt water use among Nigerians during 2014 Ebola outbreak and the role of social media
2019-05-13 12:21:58AhmedDahiruBalamiHadizaUmarMeleh
Ahmed Dahiru Balami, Hadiza Umar Meleh
1Ahmed Dahiru Balami, Department of Community Health, Universiti Putra Malaysia, 43400 UPM Serdang, Selangor Darul Ehsan. Malaysia
2Hadiza Umar Meleh, Department of Medical Microbiology, Universiti Putra Malaysia
Keywords:Ebola Social media Salt water Outbreak Nigeria
ABSTRACT Objective: To determine the spread of misinformation on salt water among Nigerians, salt water use for Ebola prophylaxis, and the role played by the social media during the 2014 Ebola outbreak.Methods: Information was collected from the general Nigerian population through online Google forms which were majorly disseminated via Facebook and WhatsApp platforms. The data retrieved was analysed using descriptive statistics, Chi-square test and multivariate logistic regression.Results: A total of 703 questionnaires were included in the final analysis. The respondents’mean age was (30.2±6.7) years, predominantly male (73.2%). Almost all of them (95.0%) had received some message to use salt water, 37.4% of whom received such message on social media. Around a half of them ever made an attempt to verify the health information they received on social media (50.9%), and about a quarter (24.0%) of them had used salt water during the outbreak. Many of them had used salt water because they believed it would not harm them (52.0%). Salt water was less likely to be used by those who had received such message on social media, as well as by those who had received some contrary information to salt use.Conclusions: Social media could serve as an effective tool in propagating health information and should be actively engaged by health agencies, to spread accurate information.
1. Introduction
Ebola virus disease is a serious illness characterized by fever,myalgia, and other non-specific symptoms, with haemorrhagic episodes occurring in 30% to 50% of cases[1]. It also has a very high case fatality of 50% to 90%[2]. Spread of the infection is initiated from wild-life to humans, after which transmission of the virus could continue between humans through body fluids[3]. In West Africa, direct transmission and contaminated staff have generally been the major means of Ebola transmission[4]. Since the first case of Ebola virus disease in 1976, the 2014 outbreak has been the largest in West Africa[5,6], and had even been declared as a Public Health Emergency of International Concern by the World Health Organization[7]. There had initially been no approved options available for Ebola treatment or post-exposure prophylaxis[5], but in order to contain the outbreak, the World Health Organization had later approved convalescent serum for Ebola treatment[8].
Misinformation on the use of salt water for Ebola prevention and treatment had gone viral in Nigeria, and had even led to adverse consequences for some users[9]. Due to high mortality, fear,misinformation and stigma from Ebola infection during the 2014 to 2016 epidemic, the Centre for Disease Control had deployed health communicators to West Africa to support ministries of health in developing and disseminating clear and science-based messages, and promoting science-based behavioral interventions[10].
Social media has the potential for getting health information widely spread, as well as influencing health behaviors[11]. A study among 400 youths in the south-west part of Nigeria revealed that 95% of them were on at least one social media platform, and only 7.3% of them made efforts to verify the authenticity of information they obtained on social media, before sharing them[12]. Despite the challenges associated with the social media, important roles of disseminating correct information through social media platforms like: Twitter, Facebook and WhatsApp, may have also contributed in containing the outbreak[13]. A different study showed that 33.1%of health workers in an infectious disease institute in Romania consulted the internet or social media for information on Ebola during the 2014 to 2016 outbreak[14]. The occurrence of a new case or the entry of a new case into a new geographical location was likely to trigger a surge in the number of tweets using the#ebola[15]. An analysis of tweets during the outbreak, showed that only 38.3% of them contained medically correct information, and tweets with misinformation, were more likely to get retweeted[16]. It was also reported from a longitudinal analysis of tweets during the outbreak that as a result of health information deficiencies, the social media could serve as an obstacle to meeting the health information needs[17]. The aim of this study was to determine the spread of misinformation on salt water among Nigerians, salt water use for Ebola prophylaxis, and the role played by the social media during the 2014 Ebola outbreak. Understanding this would guide health agencies in devising effective strategies for disseminating authentic health information especially during outbreaks, to ensure effective containment of the epidemic.
2. Materials and methods
Nigeria is a country located in West Africa, and comprises of 6 geo-political zones which are the north-east, north-west, northcentral, south-east, south-west and south-south. It is a multi-ethnic country with a population of about 195 million. Nigeria was one of the countries affected by the 2014 Ebola outbreak[18] the source of which was a Liberian diplomat who had been treated in a hospital in Nigeria[19].
A cross-sectional study was conducted among the general Nigerian population who were in Nigeria during the 2014 Ebola outbreak.Around a thousand invitations to the survey (on Google forms) were sent out via 3 social media platforms (WhatsApp, Facebook and e-mail) from the 5th of August, 2017 to the 6th of August, 2018. The survey questionnaire contained 22 items with questions on sociodemography, receipt of information/messages regarding salt water use for Ebola prevention, whether they had used salt water or not and why, and how frequently they believed or shared health information they received on social media. The questionnaire was bilingual(English and Hausa language), which was informed by the fact that literacy among adults in northern Nigeria was predominantly in Hausa language while literacy among adults in Southern Nigeria was predominantly in the English language[20].
The data retrieved from Microsoft Excel spreadsheet was transferred to Statistical Package for Social Sciences version 22(IBM SPSS, Chicago IL, USA) for analysis. Grossly incomplete questionnaires were excluded from the analysis. Categorical data were summarized as frequencies and percentages, and were also presented graphically using pie-charts. Chi-squared tests were performed to determine the bivariate association between salt water use and some of the factors studied. A further multivariate logistic regression analysis was performed to determine predictors of salt water use. The study was approved by the Ethic Review Committee of the State Specialist Hospital Damaturu, Nigeria on 24 July, 2017(YSSH/DTR/GEN/302).
3. Results
Atotal of 760 questionnaires were retrieved, giving a response rate of 76.0%. Fifty seven out of these were grossly incomplete thus,further analyses were restricted to the remaining 703 questionnaires.Their ages were not normally distributed, with median age of 30 years, with 25th and 75th percentiles of 25 and 34 years respectively.As presented in Table 1, 73.2% of them were males, and most were from the north-western part of the country (64.7%). Almost all of them had tertiary education (97.3%).
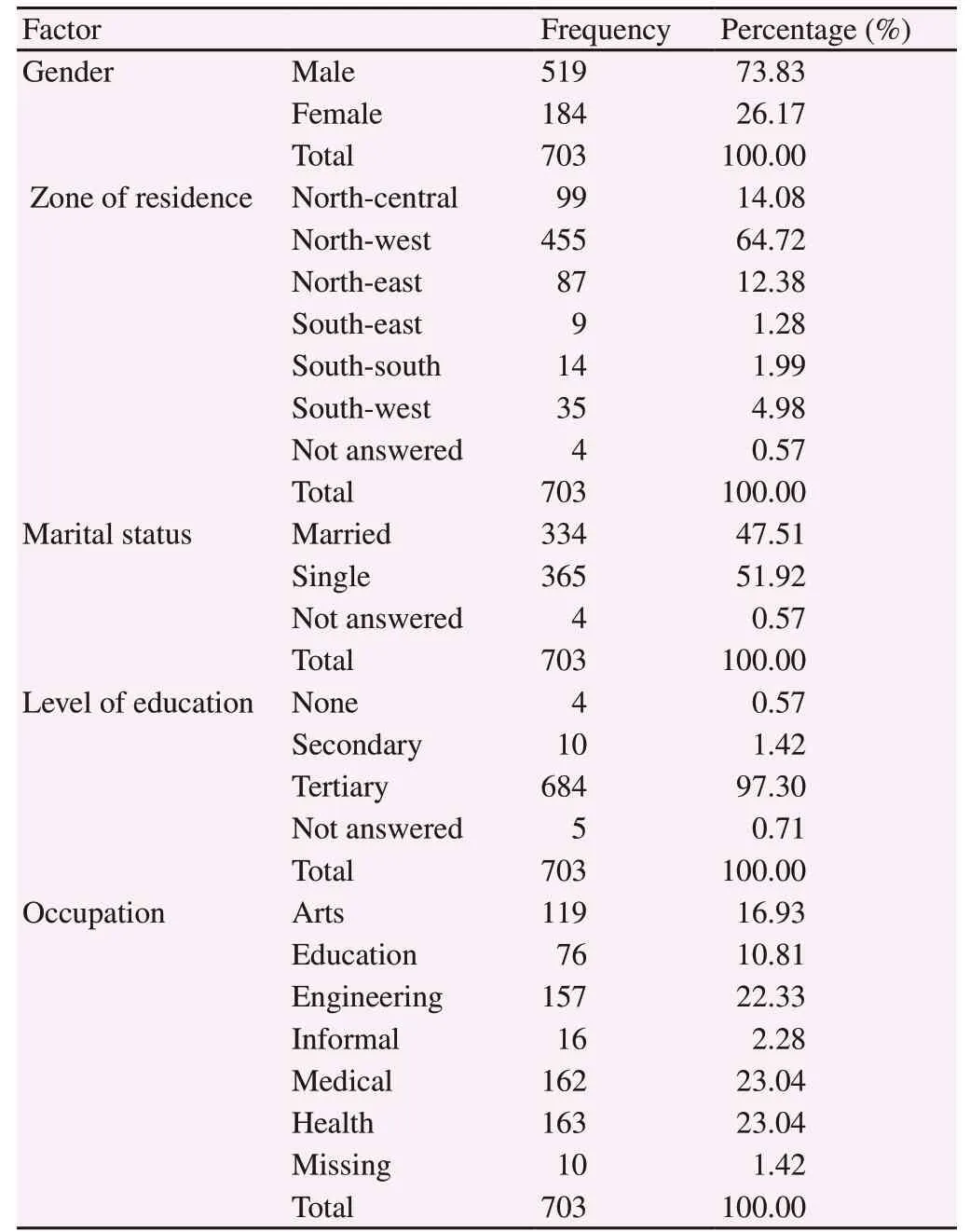
Table 1. Respondents’ socio-demographic characteristics.

Table 2. Information on salt water use for Ebola prevention.
Table 2 shows some details regarding the information on salt water use among the respondents. Almost all of them reported having received some information to use salt water for protection against Ebola during the period of the outbreak (95.02%). The predominant source of this message was the social media (37.41%). About a half of them had also received some contrary message, and around a half had made efforts to verify the authenticity of the message instructing them to use salt water. About a quarter of the respondents had used salt water during the period of the outbreak (24%), which was predominantly through bathing (87%), as illustrated in Figure 1.
Table 3 shows the association between salt water use and respondents’ socio-demographic characteristics. Age group, gender,region of residence, marital status, field of training/occupation,source of information, and receipt of contrary information on the use of salt water were significantly associated with salt water use. There was no significant difference in salt water use between those who had attempted to verify the authenticity of the information they had received and those who had not.
Table 4 shows the position of those respondents who had used salt water. A few among them stated that they would still have done so even if they had been cautioned against it by a health worker(21.56%) or even by the ministry of health (13.77%). Around a quarter (26.95%) believed it was still better that they had used the salt water.
In a multivariate logistic regression analysis to determine the predictors of salt water use, the model was fit, as indicated by a nonsignificant Hosmer and Lemeshow test (P=0.798). The Negelkerke R indicated that 22.1% of variation in salt water use could be explained by the model. As presented in Table 5, females were more than twice more likely to use salt water compared to males, while northerners were about 5 times more likely compared to southerners. Medical doctors were the least likely to have used salt water, while the highest odds of using salt water was among those in informal occupations.Those who had received the information to use salt water from their family members were more likely to do so compared to those who had received the message on social media. In addition, those who had not received any contrary information on salt water use were about twice more likely to do so compared to those who had additionally received contrary information dissuading them against using salt water.
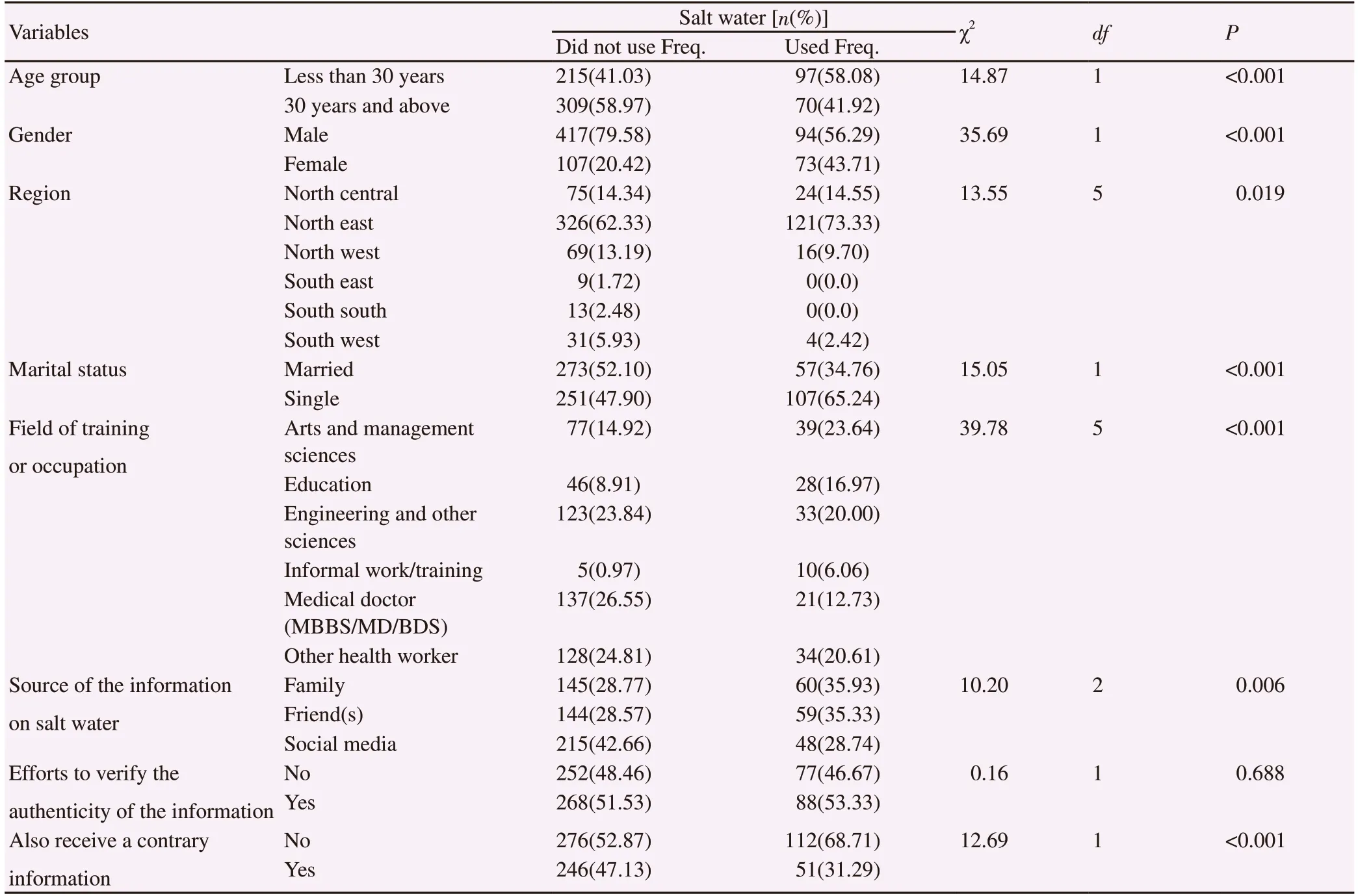
Table 3. Association between salt water use and socio-demographic factors.

Figure 1. Prevalence of salt water use and how it was used among the respondents.
Figure 2 presents the main reasons why those who used salt water had done so. The predominantly stated reason was that they felt salt water would not harm them (52%), while the next most stated reason was that even some health workers had done so (39%).
Figure 3 illustrates how much the respondents generally believed health information on social media. Only a few of them said they almost always believed such messages (11%). About a half (49%)said they sometimes believed some messages, but 32% said they rarely did so.
Figure 4 shows how frequently they shared health information received on social media. A little less than a quarter (22.0%) never shared such information, while the others did so to different degrees,from rarely (38%) to almost always (7%).
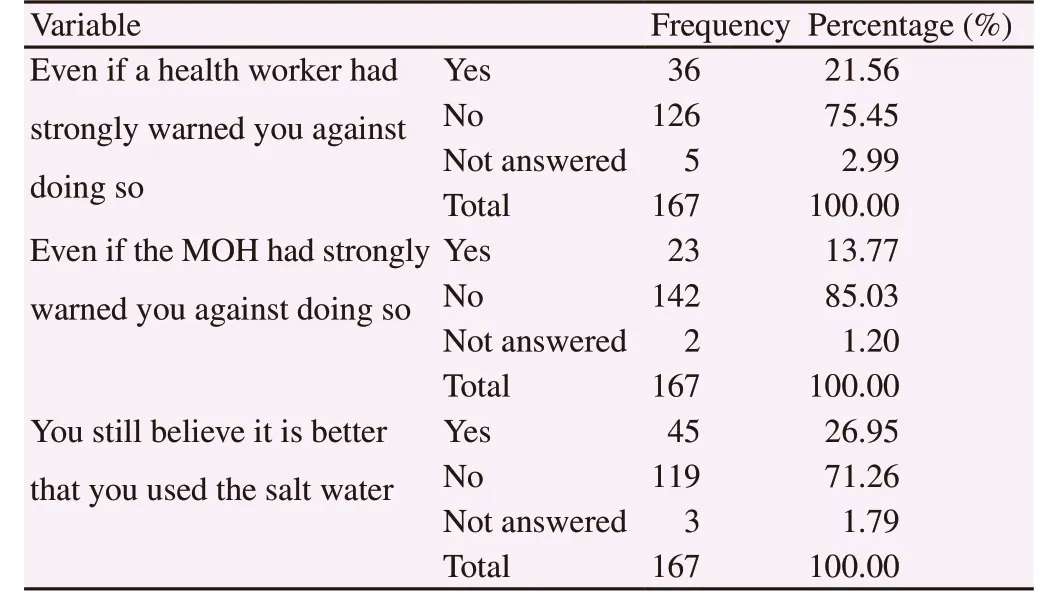
Table 4. Respondents’ position on salt water use (those who had used it,n=167).

Table 5. Predictors of salt water use.

Figure 2. The main reasons for using salt water.
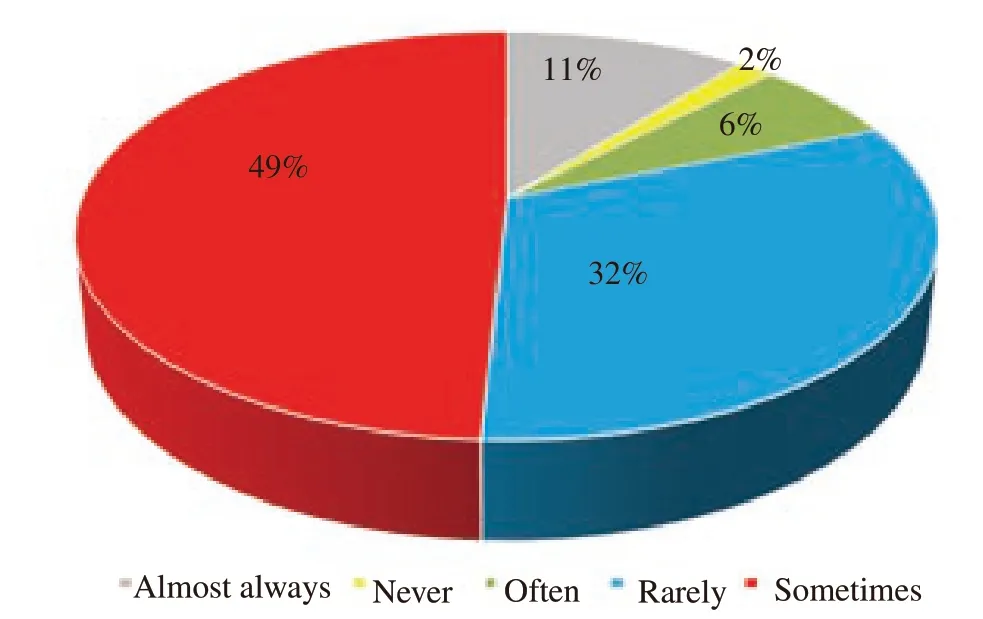
Figure 3. Frequency of believing health information received on social media.
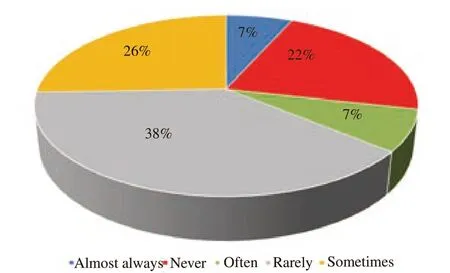
Figure 4. Frequency of sharing health information received on social media.
4. Discussion
Almost all the respondents received the message to use salt water,but less than a half of them had received any information warning against its use, buttressing earlier reports that wrong information has the tendency of spreading faster than correct information[16].The findings also illustrate that in the face of fear, individuals are very likely to subscribe to any re-assuring options provided to them without verifying, and some would still act on such information even if they also receive a strong warning against doing so from an authentic source, exemplifying how perceived susceptibility,perceived severity, and perceived benefits influence health behaviors[21].
Social media was the source of the misinformation on salt water use for over a third of the respondents, who also reported a lower use of salt water compared to those who received the information from family and friends. Compared to a previous study[22], a higher proportion of respondents in this study made efforts to verify the authenticity of the health information they receive on social media(50.92% versus 7.30%). One study also showed that most of the posts by social media users during the period of the outbreak were from direct sharing of information provided by news agencies and health organizations[13] which could explain the low use of salt water among those who obtained their information through this source as it is more likely to be of valid content compared to rumours by family and friends. Furthermore, significantly more of those who received the message on social media were likely to have also received a warning message against doing so.
Motivation is an important factor that influences health behavior[22],and moral support by significant others is an important source of social motivation[23]. This could explain the reason that messages received from family were more likely to be effective in influencing behavior, followed by messages received from friends, and then the social media, whose contacts could be largely virtual and anonymous. About forty percent of those who used salt water did so because some health workers had done the same, indicating that the engagement of health workers in a particular health practice has the tendency of being interpreted as an endorsement of its potency and safety.
Health care practitioners accounted for a sizeable proportion of the participants in this study, and younger participants were significantly more likely to have used salt water, compared to the older ones. These findings are comparable to the results of a previous study among clinicians in Ebonyi state, Nigeria, where the older practitioners demonstrated better knowledge of Ebola reporting compared to their younger colleagues[24]. While those in the arts,education, and informal sector had higher odds of using salt water compared to medical doctors, there was no significant difference between the odds for medical doctors, engineers, and other health workers (non-medical doctors), suggesting that their science background probably empowered them to make more scientific decisions. However, health workers still need more training and exposure on outbreak response and management, as they have high chances of being emulated by lay people during such cases. This is very important, as many of them also seemed vulnerable to trending rumours.
Among the strengths of the study was the anonymity it offered to the respondents, as it would have been unlikely for many of them to confess using salt water during the outbreak if it were in a faceto-face interview. One of its limitations however, was the under representation with regard to region of origin and educational level.There were relatively fewer respondents from the southern regions,and which necessitated collapsing the 6 geo-political zones broadly into north and south for further analyses. Furthermore, since almost all the participants had some tertiary education, the findings may not be generalizable to Nigerians of all educational levels. About a third of the invitations sent out could not be included in the analyses due either to non-response or incomplete response. This could obscure the true picture if the missed respondents happen to be different from those included in the analyses. Since the surveys were mostly sent out to unknown persons, there was no information about the characteristics of those who did not respond, making it impossible to compare the two groups. It is also recommended for future studies to supplement the quantitative methods with a qualitative one in the form of key informant interviews with important stakeholders like community and religious leaders.
In conclusion, wrong information has a great propensity of getting widely disseminated, and of influencing health behaviours during an outbreak. The social media has proven to be an effective tool in propagating health information (both correct and wrong), and the low tendency of such information being subjected to scrutiny by the end users makes it a very important platform for ministries of health and health agencies to engage actively, to spread correct information,while also expelling incorrect rumours.
Conflict of interest statement
The authors declare that they have no conflict of interest.
 Asian Pacific Journal of Tropical Medicine2019年4期
Asian Pacific Journal of Tropical Medicine2019年4期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Disseminated nocardiosis due to Nocardia otitidiscaviarum: A case report and literature review
- Latent tuberculosis infection among medical students in Malaysia
- Wild chive oil is an extremely effective larvicide against malaria mosquito vector Anopheles stephensi
- Characterization of the salivary microbiome in healthy Thai children
- Morphometric discrimination between females of two isomorphic sand fly species, Phlebotomus caucasicus and Phlebotomus mongolensis (Diptera:Phlebotominae) in endemic and non-endemic foci of zoonotic cutaneous leishmaniasis in Iran
- Herbal remedies, vaccines and drugs for dengue fever: Emerging prevention and treatment strategies