
Comparison of p38 MAPK, soluble endoglin and endothelin-1 level in severe preeclampsia and HELLP syndrome patients
2019-04-03 06:37EfendiLukasMaisuriChalidUpikMiskadSyakibBakri
Efendi Lukas, Maisuri T Chalid, Upik A Miskad, Syakib Bakri
1Department of Obstetrics and Gynecology, Faculty of Medicine, Hasanuddin University of Makassar, Indonesia
2Department of Phatology, Faculty of Medicine, Hasanuddin University of Makassar, Indonesia
3Departement of Internal Medicine, Faculty of Medicine, Hasanuddin University of Makassar, Indonesia
Keywords:Preeclampsia HELLP syndrome p38 MAPK Soluble endoglin Endothelin-1
ABSTRACT Objective: To compare the levels of p38 mitogen-activated protein kinase (MAPK), soluble endoglin and endothelin-1 in the serum of patients with severe preeclampsia, hemolysis,elevated liver enzymes, and low platelets (HELLP) syndrome and normal pregnancies.Methods: This study was an observational analytic cross-sectional study performed at Wahidin Sudirohusodo Hospital, Makassar, Indonesia, in the period of 5th February 2016 to 20th January 2017. P38 MAPK, soluble endoglin and endothelin-1 levels of patients with normal pregnancies, severe preeclampsia and HELLP syndrome were measured by enzymelinked immunoabsorbentassay technique, using kits of human soluble endoglin, endothelin-1 and p38 MAPK, Quantikine immunoassay: R&D System Inc.Results: Level of serum p38 MAPK in HELLP syndrome group was higher than in severe preeclampsia and normal pregnancy groups. Soluble endoglin and endothelin-1 levels in pregnancies with severe preeclampsia and HELLP syndrome were higher than normal pregnancy but there was no significant difference between these two groups (P>0.05). Levels of p38 MAPK, soluble endoglin and endothelin-1 also had a positive linear correlation with systolic and diastolic blood pressures (P<0.05).Conclusions: P38 MAPK in serum may be a marker for evidence of the severe hypoxia and its application may be considered for the diagnosis of HELLP syndrome.
1. Introduction
Preeclampsia is a pregnancy-specific syndrome that usually occurs after the 20th week of gestational age, in women with previously normotensive. This condition is characterized by an increase in blood pressure accompanied by proteinuria. Although the etiology of preeclampsia remains unclear, it is widely accepted that a defect in placental trophoblast invasion while implantation has a role in the incompletion of spiral artery remodeling process in patients with preeclampsia[1].
Regulation of trophoblast invasion is allegedly influenced by the balance of pro-angiogenic factors (vascular endothelial growth factors, placental growth factors) and its inhibitor [soluble vascular endothelial growth factors receptor, also known as soluble fms-like tyrosine kinase 1 (sFlt-1)]. In preeclampsia, the failure of trophoblast invasion of the spiral arteries in the pseudovasculogenesis process,is allegedly caused by imbalance of angiogenic and anti-angiogenic factors[2,3]. Incomplete spiral artery remodeling process will cause the walls of the spiral arteries to be inelastic and increase their resistance. Furthermore, this situation causes a decrease in uteroplacental perfusion and it will lead to a placental ischemia. Decrease in placental perfusion, which will be followed by placental hypoxia,is an early important picture in pregnancy with preeclampsia and fetal growth disorders. Placental hypoxia will lead to the release of antiangiogenic factors produced by cytotrophoblast and villous placental tissue in tissue culture[4,5].
Protein kinases are enzymes that covalently bind to phosphate on the side chain of serine, threonine, or tyrosine of specific proteins in cells. Mitogen-activated protein (MAPK) performs specific serine and threonine phosphorylation of target protein substrates and regulates the activity of cellular gene expression, mitosis, movement,metabolism and cell death programming (apoptosis). Since a lot of functions are controlled by the MAPK pathway, many researches have done to determine the role of MAPK in human physiology and disease[6].
P38 MAPK is a key component of the stress response pathways and a target of drugs that suppress inflammatory cytokines. p38 MAPK is activated by a variety of extracellular stimuli such as inflammatory cytokines (interleukin-1β and tumor necrosis factor-α), growth factors such as fibroblast growth factor, and changes in osmolarity,ultraviolet light and chemicals that enhance the stress response.Angiogenesis in the placenta as in the yolk sac and embryo also requires the activity of p38 MAPK. There are 4 MAPK isoforms that have been identified, which are encoded in different gene loci. p38α MAPK plays a role in stress response, and a research has found that p38α MAPK isoform plays an important role in normal embryonic development[7-9]. p38 MAPK pathway is activated by stress, but also plays an important role in immune responses such as cell regulation and differentiation[10-12] It is known that the MAPK pathway is also an important mediator of growth factor signaling in the placenta.
Endoglin is antiangiogenic which is a co-receptor to alterβ1 and β3 growth factors (transforming growth factor-β1 and transforming growth factor-β3), found in significant amounts in the membranes of vascular endothelial cells and syncytiotrophoblast. In patients with preeclampsia, many soluble endoglin are released into the circulation by the placenta[13].
Furthermore, it was reported that endothelin-1 also increased oxidative stress in placental villi, so that endothelin may have an additional impact on maternal cardiovascular system, not only through direct effect on the vascular system, but also indirectly through oxidative stress[14]. The increase of p38 MAPK induced by oxidative stress and placental hypoxic nitrative stress is suggested to lead to increase levels of substances such as soluble endoglin vasoconstrictor which will lead to endothelial dysfunction. Vascular endothelial dysfunction will produce endothelin-1, a potent vasoconstrictor that will cause preeclampsia symptoms, such as hypertension, proteinuria, and edema.
The purpose of this study was to compare the levels of p38 MAPK,soluble endoglin and endothelin-1 in the serum of patients with severe preeclampsia, hemolysis, elevated liver enzymes, and low platelet (HELLP) syndrome and normal pregnancies. Researchers assume that if the level of p38 MAPK may be examined in the serum of pregnant women, it can be one of the markers to assess the severity of complications in pregnancy with preeclampsia.
2. Materials and methods
2.1. Study design
This study is an observational analytic study with cross sectional approach of all patients who met the inclusion criteria.
2.2. Setting
This study was performed at Wahidin Sudirohusodo Hospital,Makassar, in the period of 5th February 2016 to 20th January 2017.
2.3. Participants
Subjects were patients with preeclampsia, HELLP syndrome and normal pregnancies who were: singleton live pregnancies, > 34 weeks in gestational age, no history of hypertension, diabetes mellitus and autoimmune diseases such as systemic lupus erythematosus.
We gathered 80 subjects, who met the inclusion criteria, consist of 45 patients with severe preeclampsia, 13 patients with HELLP syndrome and 22 patients with normal pregnancies.
2.4. Study size
The following formula was used to define sample size:

In this formula, n1and n2was sample size for each group. zα=deviation standard value (1.96), zβ= power (0.842) and then we found that minimal sample size required was 62.
2.5. Variables
Criterion for severe preeclampsia was a pregnancy with systolic blood pressure greater than or equal to 160 mmHg and/or diastolic blood pressure greater than or equal to 110 mmHg at gestational age > 20 weeks along with the presence of proteinuria (++) or more on qualitative examination. HELLP syndrome was determined if there was any: hemolysis, elevated liver enzymes and low platelet count. Level of HELLP syndrome was determined by the degree of Tennese classification. Complete HELLP syndrome (total):platelets <100 000/mL; lactate dehydrogenase 600 000 IU/L or more; aspartate transaminase 70 IU/L or more; bilirubin 1.2 mg/dL or more. HELLP syndrome was incomplete (partial) if there were only 1 or 2 of the above signs.
Blood samples were taken 7 mL, centrifuged 1 000 times in 15 min to separate the serum from its super natan. Serum that had not been checked would be stored in the refrigerator with a temperature of-20 ℃ in the laboratory Prodia Makassar. Laboratory examination was done at Prodia Jakarta. p38 MAPK, soluble endoglin and endothelin-1 levels were examined by enzyme-linked immuno absorbent assay technique using kits human soluble endoglin,endothelin-1 and p38 MAPK, Quantikine immunoassay: R&D System Inc.
2.6. Statistical method
Data were analyzed with SPSS using Mann Whitney, one way ANOVA for normally distributed data, otherwise we would transform data or use Kruskall Wallis test for data that were not normally distributed, and least significant difference tests.
3. Results
Table 1 showed characteristics of the subjects. The age, parity,hemoglobin level and birth weight showed no significant differences(P>0.05) in all three study groups, while systolic, diastolic blood pressure, leukocyte and platelet levels showed a significant difference (P<0.05).
Table 2 showed differences in serum level of p38 MAPK which significantly (P<0.05) differed among the three groups; serum level of p38 MAPK in HELLP syndrome group was higher than in severe preeclampsia and normal pregnancy groups, and there was a significant difference between the groups of HELLP syndrome and severe preeclampsia. In contrary, although serum levels of soluble endoglin and endothelin-1 in patients with severe preeclampsia and HELLP syndrome were significantly higher (P<0.05) than in normal pregnant women, there was no significant difference (P>0.05)between the HELLP syndrome and severe preeclampsia groups.
Table 3 showed that there was a positive linear correlation between levels of P38 MAPK with systolic and diastolic blood pressure,as well as between levels of soluble endoglin and endothelin-1(P=0.000).
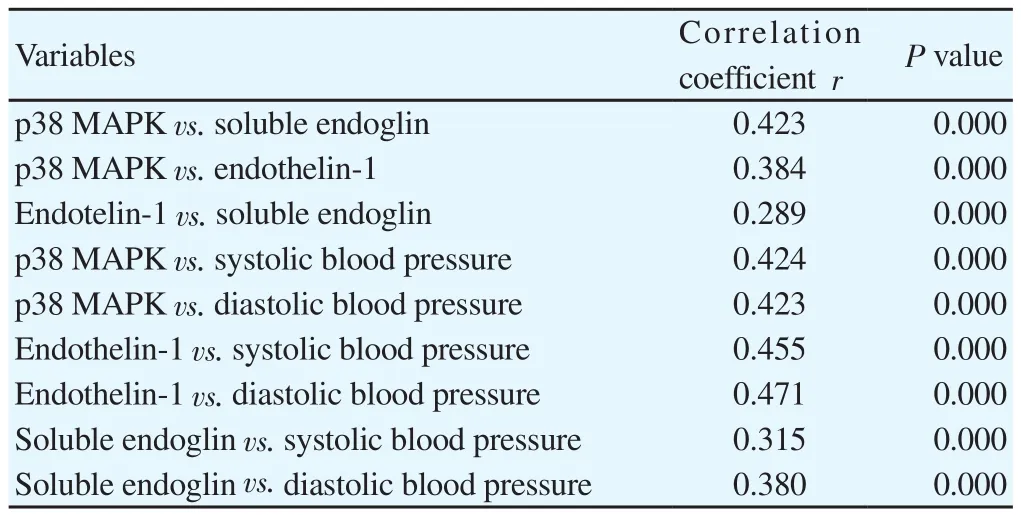
Table 3. Results of correlation analysis (n=80).

Table 1. Characteristic of research variable (mean ± SD).

Table 2. Differences in serum level of soluble endoglin, endothelin-1 and p38 MAPK (mean ± SD).
4. Discussion
In pregnancy with severe preeclampsia there is hypoxia in the placenta which stimulates the release of antiangiogenic factors such as soluble endoglin and soluble vascular endothelial growth factors receptor (sFlt1). In this study, we found increased levels of both soluble endoglin in patients with preeclampsia or HELLP syndrome patients, proving that both severe preeclampsia and HELLP syndrome occur in hypoxic conditions that trigger the release of angiogenic factors. Researchers also found elevated levels of soluble endoglin and sFlt-1 in patients with preeclampsia and HELLP syndrome, but there is no correlation between soluble endoglin and sFlt-1 (r2=0.008, P=0.62).
The imbalance of pro and antiangiogenic factors will cause vascular endothelial dysfunction. Vascular endothelial damage stimulates the release of endothelin-1, which is a vasoconstrictor that will lead to preeclampsia symptoms. In this study, we found elevated level of endothelin-1 in patients with severe preeclampsia and HELLP syndrome, but there were no significant difference in levels of endothelin-1 between patients with severe preeclampsia and HELLP syndrome. This suggested that the two groups have the same level of endothelial dysfunction.
Endothelin-1 also increased oxidative stress in placental villi,so that endothelin may have an additional impact on maternal cardiovascular system, not only through direct effect on the vascular system, but also indirectly through oxidative stress[15]. p38 MAPK also plays a role in modulating angiogenic factors, resulting in hypoxic conditions such as preeclampsia where its level will rise[16].Some researchers, such as Lohmann et al[17] found an increase in p38 MAPK activity in patients with preeclampsia (P=0.022), while in patients with HELLP syndrome it was found to the contrary.
Coradetti et al[18] concluded that p38 MAPK is required for the angiogenic response to environmental hypoxia in patients with HELLP syndrome. They found a decrease in gene expression of p38 MAPK in the placenta of up to 80% compared with normal pregnancy, and HELLP syndrome is suspected in patients with severe hypoxia in the placenta caused by decreased activity of p38 MAPK.
In this study, we found increased level of p38 MAPK in the serum of patients with HELLP syndrome and severe preeclampsia, but the level was significantly higher in patients with HELLP syndrome.There are no previous studies that examined the serum level of p38 MAPK in preeclampsia and HELLP syndrome. The difference in serum level of p38 MAPK in HELLP syndrome and severe preeclampsia suggested that there are different degrees of hypoxia in both groups. Elevated levels of p38 MAPK resulted in increasing vascular endothelial permeability which can aggravate edema including edema in the brain.
p38 MAPK signal proved to act as a “molecular switch” between angiogenesis and hyperpermeability, inhibition of p38 MAPK activity reinforcing effects of vascular endothelial growth factor angiogenesis in both in vitro and in vivo. It was not clear how the relationship between decreased expressions of p38 MAPK in the placenta with increased serum levels of p38 MAPK.
Soluble endoglin, endothelin-1 and p38 MAPK showed a positive correlation with the increase of systolic and diastolic blood pressure.This suggested that any increase in the levels of soluble endoglin,endothelin-1 and p38 MAPK would lead to increased levels of systolic and diastolic blood pressure. From this study, we can conclude that the levels of p38 MAPK in serum may be a marker for the evidence of severe hypoxia and may be considered to be one examination to diagnose HELLP syndrome. We are working on a study to assess the expression of p38 MAPK in the placenta of HELLP syndrome and severe preeclampsia patients and the results will be compared with the levels of p38 MAPK in serum.
In conclusion, elevated levels of p38 MAPK, soluble endoglin and endothelin-1 which are correlated with the increase of systolic and diastolic blood pressure occur in patients with severe preeclampsia and HELLP syndrome. The increase of p38 MAPK serum in HELLP syndrome and severe preeclampsia prove the existence of a process of severe hypoxia. Examination of serum levels of p38 MAPK can be considered to be one of the markers to diagnose HELLP syndrome.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Acknowledgments
Fisrt of all, I would like to express my special thanks and gratitude to all parties involved on this work especially for Prof. Dr. dr. Syakib Bakri, Sp.PD, Dr. dr. Siti Maisuri Chalid, Sp.OG(K), dr. Upik Mariskad, Ph.D, Sp.PA, Prof. Dr. dr. Johanes C Mose, Sp.OG(K)for advising author on this work writing. Secondly, I also gratefully thank to the principal of Wahidin Sudirohusodo Hospital, University of Hasanuddin for its support on this writing. I take full consideration that this work will never completed without help and participation of you all.
 Asian Pacific Journal of Reproduction2019年2期
Asian Pacific Journal of Reproduction2019年2期
- Asian Pacific Journal of Reproduction的其它文章
- Review on canine pyometra, oxidative stress and current trends in diagnostics
- Effect of combination of Gynura procumbens aqueous extract and Trigona spp. honey on fertility and libido of streptozotocin-induced hyperglycaemic male rats
- Effect of Vitex agnus-castus plant extract on polycystic ovary syndrome complications in experimental rat model
- Improvement of Phaseolus vulgaris on breastfeeding in female rats
- Oestrous cycle of Wistar rats altered by sterol and triterpenes rich fraction of Adansonia digitata (Linn) root bark - A scientific rationale for contraceptive use
- Secondary sex ratio of assisted reproductive technology babies