
Effi ciency of community health centers in China during 2013– 2015:A synchronic and diachronic study*
2019-01-23 02:54:12LinZhaoYaoZhangYabingHouGuimingYan
Lin Zhao , Yao Zhang , Yabing Hou , Guiming Yan
1. International Medical School,Tianjin Medical University,Tianjin 300070, China
2. School of Public Health, Tianjin Medical University, Tianjin 300070, China
3. School of Nursing, Tianjin Medical University, Tianjin 300070, China
Abstract Objective: We aimed to explore the eff iciency of community health centers (CHCs) in China from 2013 to 2015, providing policy suggestions for optimizing the allocation of health resources.Methods: Data on the eff iciency of CHCs in 30 provinces/autonomous regions/municipalities in mainland China (except Tibet) from 2013 to 2015 were collected from China’ s Health and Family Planning Statistical Yearbook 2014, China’ s Health and Family Planning Statistical Y earbook 2015,and China’ s Health and Family Planning Statistical Y earbook 2016. Data envelopment analysis and Malmquist index analysis were performed to investigate the eff iciency of sampled CHCs during this period at the national level and the regional level. The applied input indicators include the numbers of CHCs, community health workers, and beds, and the output indicators consist of the numbers of visits and inpatients, the occupancy rate of beds, and the average length of stay.Results: In 2015, the average annual overall technical eff iciency, pure technical eff iciency,and scale eff iciency of CHCs in 30 regions at the national level were 0.715, 0.705, and 0.972,respectively. Eight regions (Guangdong, Guizhou, Hainan, Ningxia, Qinghai, Shanghai, Zhejiang,and Chongqing, accounting for 26.7% of the total) had eff icient CHCs with overall technical eff iciency of 1.000, and the other 22 regions had surpluses of 131 CHCs, 5573 community health workers, and 2086 beds on average. In 2015, the average annual technical change index, pure technical eff iciency change index, total factor productivity, technical eff iciency change index, and scale eff iciency change index of CHCs at the national level were 1.034, 1.002, 1.024, 0.990, and 0.988, respectively. Compared with 2013, the former three increased by 3.4%, 0.2%, and 2.4%,respectively, while the latter two decreased by 1.0% and 1.2%, respectively.Conclusion: On the whole, eff iciency improvements of CHCs were achieved at the national level from 2013 to 2015, but with obvious interregional differences. In regions with ineff icient CHCs identif ied by data envelopment analysis, there was a problem of coexistence of shortage and wastage of community health resources. In view of this, targeted measures should be taken to optimize the allocation of community health resources, and the management of CHCs should be strengthened to improve the eff iciency of these institutions.
Keywords: Community health center; data envelopment analysis; eff iciency; total factor productivity
Introduction
The Opinions of the Central Committee of the CPC a nd t he S tate C ouncil o n D eepening t he Reform of the Pharmaceutical and Healthcare System promulgated in 2009 put forward that,to achieve the goals of the deepening the reform of the pharmaceutical and healthcare system, the principle of the unity of fairness and eff iciency should be adhered to;in particular, importance should be attached to the development and eff iciency evaluation of community health services during improvement of the grassroots healthcare delivery system and promotion of the equalization of the basic public health services. In this way, a long-term mechanism ensuring equity and eff iciency in healthcare will be formed, and the health service sector will gradually fulf ill the responsibilities and duties of the“ gatekeeper” for residents’ health [ 1, 2]. Moreover, the Guiding Opinions of the General Off ce of the State Council on Pushing Forward t he B uilding o f t he Hie rarchical M edical S ystem promulgated in 2015 proposed that, by 2017, a comparatively complete system of supportive policies for the implementation of the hierarchical medical system will have been developed gradually, mechanisms for separation of duties and cooperation of medical institutions will have been developed basically, highquality medical resources will have been orderly and eff iciently allocated to grassroots medical institutions, the building of the primary care workforce, consisting mainly of general practitioners, will have been strengthened, and the utilization eff iciency and overall benef its of medical resources will have been further enhanced. In addition, by 2020, the capabilities of medical institutions delivering hierarchical medical services will have increased comprehensively, the medical insurance system will have gradually improved, a healthcare delivery system characterized by reasonable distribution, appropriate size, optimized hierarchy, clearly def ined responsibilities, fully functioning,and high eff iciency will have been constructed basically, a hierarchical diagnosis and treatment pattern characterized by initial diagnosis and treatment in grassroots medical institutions,bidirectional referral, treatment of acute and chronic diseases separately, and cooperation between upper-level and lowerlevel medical institutions will have been formed in a step-bystep approach, and the construction of the hierarchical medical system based on national conditions will have been completed basically [ 3]. Therefore, evaluating the eff iciency of community health organizations (CHOs) in China contributes to promoting the effective running of the community healthcare delivery system, facilitating the implementation of the hierarchical medical system, and remarkably relieving the problem of “ diff icult and costly access to healthcare services.” To provide evidence-based policy recommendations for optimizing the allocation of health resources, we conducted a synchronic and diachronic study of the eff iciency of community health centers (CHCs) in mainland China (except Tibet) by using data envelopment analysis (DEA)and DEA-based Malmquist index models.
Materials and methods
Data sources
Data concerning the eff iciency of CHCs in 30 provinces/autonomous regions/municipalities in mainland China (Tibet was excluded because of partial data loss) during 2013—2015 were obtained from China’ s Health and Family Planning Statistical Y earbook 20 14, China’ s H ealth a nd F amily Planning Statistical Yearbook 2015, and China ’ s Health and Family Planning Statistical Yearbook 2016 [ 4— 6].
Methods
DEA is a mathematical programming— based method that is used to systematically compare the relative productive eff iciency of different units of the same type by dealing with multiple inputs and outputs. It is considered to be the most mature and advanced approach for measuring the performance of health institutions. By use of the Banker-Charnes-Cooper(BCC) model, a type of DEA model allowing variable returns to scale, scores of pure technical eff iciency (PTE) and scale eff iciency (SE) were obtained; these where then multiplied to obtain the overall technical eff iciency (OTE). If a decisionmaking unit (DMU) achieves an OTE of 1, then it is considered eff icient; otherwise it is ineff icient. For an ineff icient DMU, the target output value was obtained by subtraction of the excess input value from the initial input value; namely, the optimal outputs were achieved by our taking full advantage of the inputs via improvements [ 7]. By use of a DEA-based Malmquist index model, the dynamic eff iciency of the DMU was derived. Eff iciency changes were studied by use of the total factor productivity (TFP), an eff iciency function— based Malmquist index, which was transformed from the distance function— based Malmquist index by use of the reciprocal relationship between the eff iciency function and the distance function. The eff iciency change index (ECI) was def ined as the product of the technical change index (TCI) and the technical eff iciency change index (TECI; which could be decomposed into the pure technical eff iciency change index [PTECI] and the scale eff iciency change index [SECI]). If a DMU achieves an ECI greater than 1, less than 1, or equal to 1, this indicates that it has increasing, decreasing, or constant returns to scale compared with the prior period [ 8].
Evaluation parameters
As DEA-based eff iciency assessment of health institutions is based on input and output data and a specif ied minimum number of inputs and outputs [ 9], reasonable choice of these indicators is of great signif icance. Currently, a widely adopted minimum sample for DEA should be equal to or greater than 2 nm, where n and m represent the number of inputs and outputs, respectively. In a systematic review of studies concerning DEA-based assessment of the eff iciency of medical institutions in China, Wang and Xing [ 9] put forward suggestions for effectively selecting the input and output indicators. On the basis of the suggestions, the aim of our study, and the conditions of domestic CHCs, we developed an assessment system consisting of three input indicators (number of CHCs, number of community health workers, and number of beds) and four output indicators (number of visits, number of inpatients,occupancy rate of beds, and average length of stay). Moreover,we chose 30 Chinese provinces/autonomous regions/municipalities as the DMUs, exceeding the minimum sample size(2 nm = 24; n = 3, m = 4) required for DEA.
Statistical analysis
Data were stored in a database built with Excel 2010 and were analyzed descriptively. DEA-based empirical analysis of the performance of CHCs was conducted with MaxDEA 5.0.
Results
DEA-based effi ciency assessment of the CHCs in China from a synchronic perspective
Input-output indicator values for CHCs in 30 Chinese provinces/autonomous regions/municipalities in 2015:As shown in Table 1, the top three regions with the largest number of CHCs were Guangdong (1078), Jiangsu(548), and Shandong (513), and the three regions with the least number of CHCs were Ningxia (16), Hainan (22), and Qinghai(29). The number of community health workers was greatest in Guangdong (42,837), Jiangsu (37,589), and Zhejiang (33,982),and was least in Ningxia (1229), Qinghai (1937), and Hainan (2490). Jiangsu (19,019), Shanghai (17,099), and Hubei(13,349) were the top three regions having the largest number of beds in CHCs, and Ningxia (94), Qinghai (568), and Hainan(720) were the bottom three. The number of visits in CHCs was greatest in Guangdong (99,604,961), Shanghai (86,740,055),and Zhejiang (84,484,539), and was least in Ningxia (254,589),Qinghai (716,853), and Hainan (1,042,836). In terms of the number of inpatients in CHCs, the three top-ranked regions were Jiangsu (333,650), Hubei (309,576), and Hunan(274,093), and the three bottom-ranked regions were Ningxia(190), Qinghai (8724), and Tianjin (11,852). With regard to the occupancy rate of beds in CHCs, Shanghai (86.0%), Chongqing (74.6%), and Hunan (69.9%) ranked in the top three,while Tianjin (20.6%), Ningxia (22.7%), and Jilin (26.8%)ranked in the bottom three. With regard to the average length of stay in CHCs, the three highest-ranked regions were Shanghai (60.5 days), Beijing (20.7 days), and Ningxia (20.3 days),and the three lowest-ranked regions were Guizhou (4.7 days),Gansu (5.7 days), and Qinghai (6.0 days).
Effi ciency of CHCs in 30 Chinese provinces/autonomous regions/municipalities in 2015:The average annual OTE, PTE, and SE for the CHCs in the 30 Chinese provinces/autonomous regions/municipalities in 2015 were 0.715, 0.705, and 0.972, respectively. The CHCs in eight regions (Guangdong, Guizhou, Hainan, Ningxia, Qinghai,Shanghai, Zhejiang, and Chongqing) scored 1.000 in terms of the average annual OTE, PTE, and SE, indicating their performances were eff icient ( Table 2).
Improvement measures based on input indicators for ineffi cient CHCs at the regional level:Twenty-two regions were found to have ineff icient CHCs: Anhui, Beijing,Fujian, Gansu, Guangxi, Hebei, Henan, Heilongjiang, Hubei,Hunan, Jilin, Jiangsu, Jiangxi, Liaoning, Inner Mongolia,Shandong, Shanxi, Shaanxi, Sichuan, Xinjiang, Yunnan, and Tianjin. To improve the eff iciency of ineff icient CHCs at the regional level under the premise of keeping the outputs constant, there is a need to reduce the input quantity in each of these regions: the numbers of CHCs, community health workers, and beds in these regions need to be reduced by 131, 5573,and 2086, respectively, on average ( Table 3).
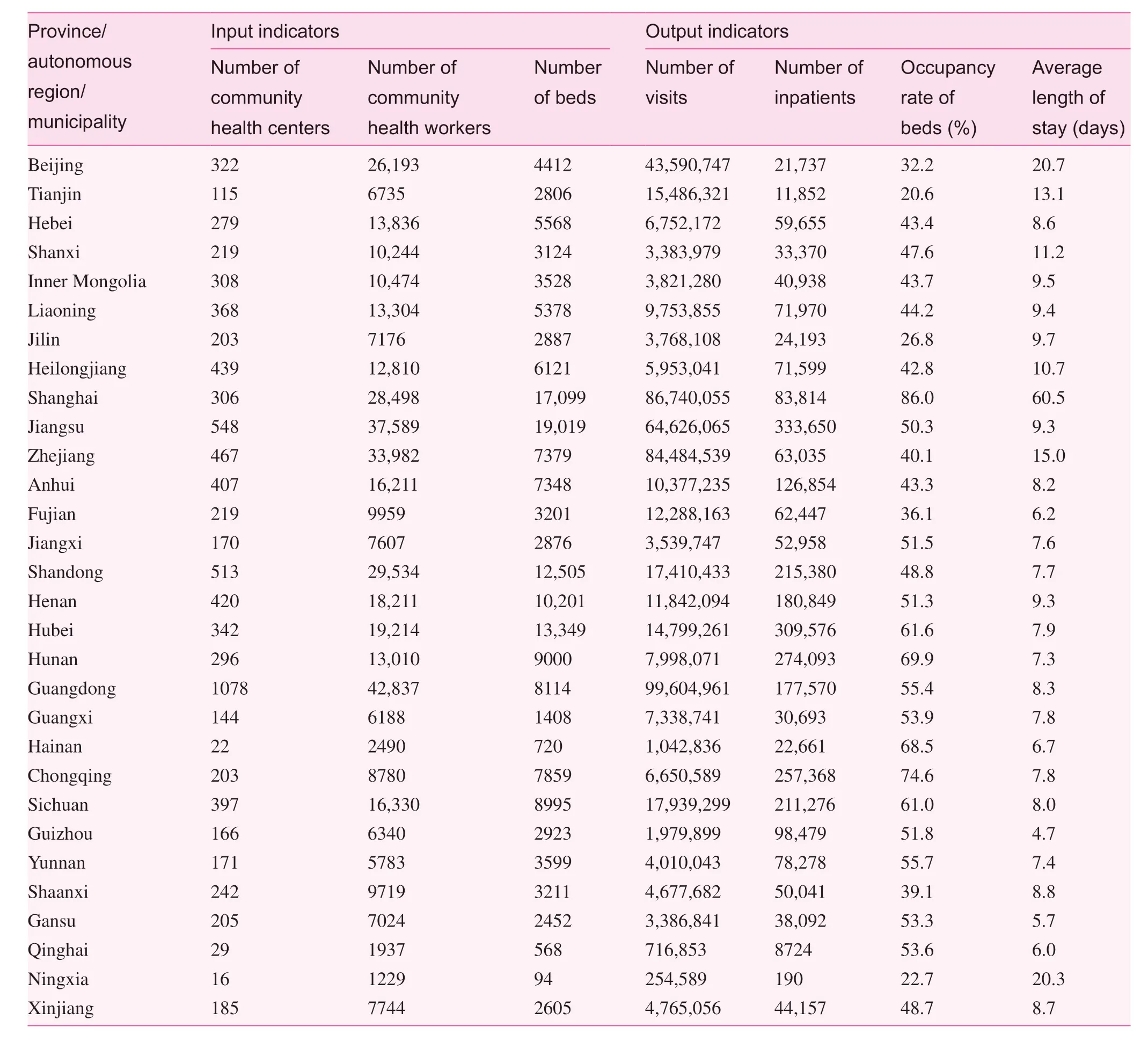
Table 1. Input-output indicator values for community health centers in 30 Chinese provinces/autonomous regions/municipalities in 2015
Effi ciency assessment of the CHCs in China during 2013 – 2015 from a diachronic perspective by use of DEA-based Malmquist index models:In 2015, the average annual TCI, PTECI, TFP, TECI, and SECI of CHCs at the national level were 1.034, 1.002, 1.024, 0.990, and 0.988,respectively. Compared with 2013, the former three grew by 3.4%, 0.2%, and 2.4%, respectively, whereas the latter two declined by 1.0% and 1.2%, respectively. From a regional perspective, compared with 2013, in 2015, the average annual TECI, TCI, PTECI, SECI, and TFP of CHCs increased the most in Tianjin, Qinghai, Shanxi, Jilin, and Qinghai, respectively, increasing by 7.0%, 31.1%, 19.0%, and 4.5%, and 31.1%, respectively, whereas they declined most in Anhui,Beijing, Anhui, Shanxi, and Heilongjiang, respectively, decreasing by 12.8%, 6.2%, 6.4%, 15.9%, and 7.3%, respectively ( Table 4 ).
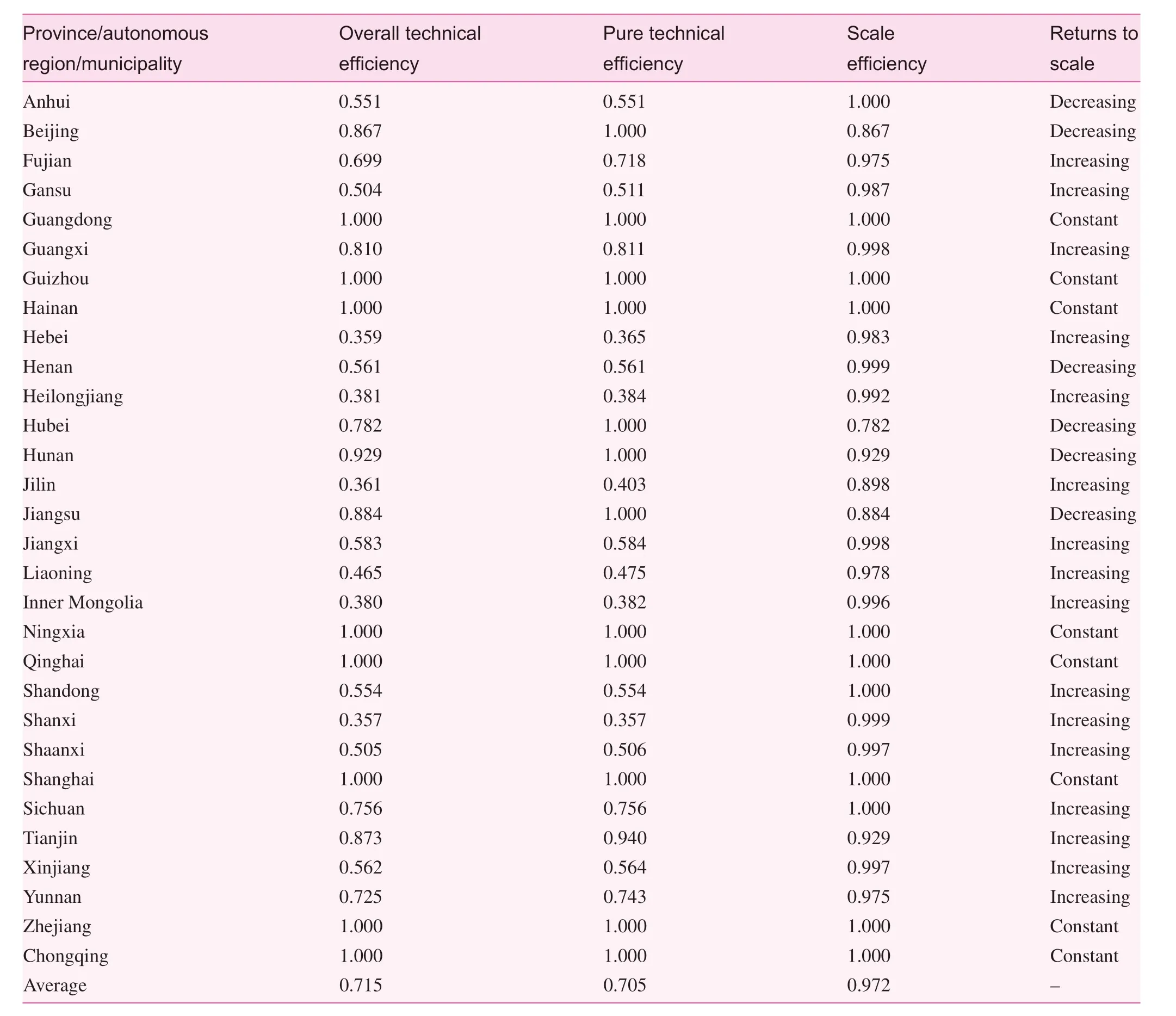
Table 2. Eff iciency of community health centers in 30 Chinese provinces/autonomous regions/municipalities in 2015
Discussion
Static analysis of the effi ciency of CHCs in 30 Chinese provinces/autonomous regions/municipalities
We found that the distribution of community health resources is unbalanced and the workload of CHCs is different across the regions of China. The input/output levels of CHCs were high mainly in Guangdong, Jiangsu, and Shanghai, but were low mainly in Ningxia and Qinghai, which may be due to regional disparities in economic levels and community-based care development. Moreover, the eff iciency of CHCs at the national level is relatively low: only eight regions (26.7% of the total)with eff icient CHCs scored 1 in terms of OTE, PTE, and SE.The CHCs in six regions (Anhui, Beijing, Henan, Hubei,Hunan, and Jiangsu) exhibited decreasing returns to scale, suggesting that health resources in these institutions were wasted during running, while 16 regions (Fujian, Gansu, Guangxi,Hebei, Heilongjiang, Jilin, Jiangxi, Liaoning, Inner Mongolia,Shandong, Shanxi, Shaanxi, Sichuan, Tianjin, Xinjiang, and Yunnan) exhibited increasing returns to scale, indicating that health resources in these institutions became insuff icient because of changes in scale.
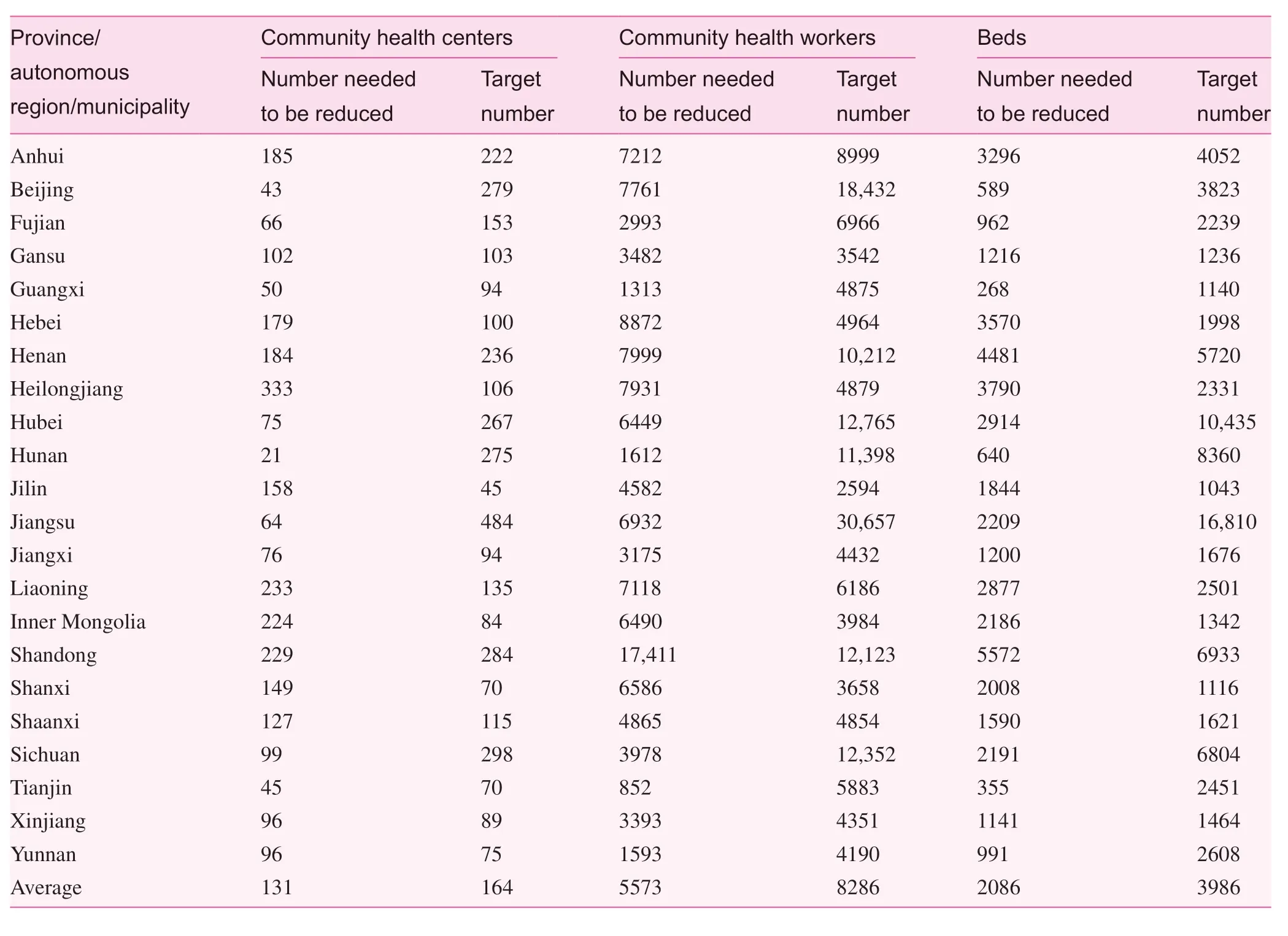
Table 3. Target input quantity and input reductions needed to make ineff icient community health centers eff icient in 22 Chinese provinces/autonomous regions/municipalities
In addition, average surpluses of 131 CHCs, 5573 community health workers, and 2086 beds were found in the 22 regions with ineff icient CHCs, demonstrating that the inputs for the CHCs in these regions were wasted to various degrees or were used insuff iciently. Thus it can be seen that health resources at the national level are manifested by the coexistence of shortage and wastage besides insuff icient amount and imbalanced distribution. In view of this, we suggest that the investment for the construction of public health hardware should be strengthened and equipment available in CHCs should be improved.Moreover, good management and reasonable use of equipment are needed [ 8, 10]. Furthermore, to reduce wastage of health resources, measures for improving the use of the surplus and idle health resources, such as increasing equipment sharing between departments of the CHCs, and loaning equipment to other institutions with payment of a fee, should be taken on the basis of local conditions. In this way, a community-based service delivery system characterized by reasonable distribution, good support, and standardized management will be established.

Table 4. Average annual dynamic changes in the eff iciency of community health centers in 30 Chinese provinces/autonomous regions/municipalities from 2013 to 2015
Dynamic analysis of the effi ciency of CHCs in 30 Chinese provinces/autonomous regions/municipalities by Use of DEA-based Malmquist index models
This study revealed that during 2013— 2015, the CHCs at the national level achieved a TECI of about 1 (0.990) and a TCI of 1.034, suggesting that the improvement of overall production eff iciency in this period was mainly derived from technical innovation. However, since increased PTE and decreased SE are the major driving force of OTE, the low management level of CHCs was mainly caused by decreased scale economies.During the period, the TFP of CHCs across the regions had an average growth rate of 2.4%, which is much lower than that(13.9%) found by Zhao [ 11] concerning the assessment of relative productive eff iciency of medical institutions in 31 regions of China during 2007— 2011. Nevertheless, Zhao proposed that technical innovation rather than an enhanced management level generated the increased eff iciency of medical institutions,which is similar to our f indings.
The TFP of the CHCs in 18 regions (60.0% of the total)improved during 2013— 2015, but there were regional differences. Moreover, the differences were more signif icant between regions with the greatest improvement of TFP of the CHCs and those with the least. Hence, in regions with less improved or decreased TFP of CHCs, reasonable establishment and scientif ic management of CHCs should be strengthened, the integration of the network of CHCs should be achieved as early as possible, registration of general practitioners should be promoted, and the service quality of CHOs should be improved [ 12].
Moreover, governments at the regional level should strongly support social forces to run CHOs to provide diversif ied health services for residents, and in a unif ied way construct the information management system for CHOs to achieve integrated sharing of internal information and big data in healthcare between CHOs as soon as possible. In this way, the diagnostic and therapeutic process (including appointment, registration,diagnosis, treatment, referral, use of public services, payment of medical costs, reimbursement of medical costs though medical insurance, and drug inspection and management) for residents will be more eff icient and convenient, exchange of information between CHOs and physician-patient interaction will be strengthened, the experience of residents in seeking healthcare will be improved, and the overall eff iciency of CHOs will be improved.
Conf lict of interest
The authors declare that they have no conf lict of interest.
Funding
This study was supported by the grants from the National Natural Science Foundation of China (71704130), and the special fund from the China Postdoctoral Science Foundation(2016T90211).
Author contributions
Lin Zhao and Guiming Yan designed and conducted the study,wrote the paper, and are responsible for the content of the paper. Yao Zhang and Yabing Hou helped collect data, perform the study, and interpret the results. Lin Zhao performed quality control and revised the paper.
Signif icance statement
· Evaluation of the eff iciency of CHCs in China at the national level and regional level from synchronic and diachronic perspectives.
· Use of data collected from China’s Health and Family Planning Statistical Yearbook 2014, China’s Health and Family Planning Statistical Yearbook 2015, and China’s Health and Family Planning Statistical Yearbook 2016.
· Use of data envelopment analysis and Malmquist index analysis to analyze the eff iciency of CHCs.
 Family Medicine and Community Health2018年4期
Family Medicine and Community Health2018年4期
- Family Medicine and Community Health的其它文章
- Factors associated with visit-to-visit variability of blood pressure in hypertensive patients at a Primary Health Care Service, Tabanan,Bali, Indonesia
- Nutritional status in adolescent girls: Atte mpt to determine its prevalence and its association with sociodemographic variables
- Predictors of successfully quitting smoking among smokers registered at the quit smoking clinic at a public hospital in northeastern Malaysia
- Relationship between glycemic control and perceived family support among people with type 2 diabetes mellitus seen in a rich kinship network in Southwest Nigeria
- Adherence to clinical guidelines for monitoring diabetes in primary care settings
- Acknowledgement to reviewers