罗哌卡因联合地塞米松对硬膜外分娩镇痛的影响
2019-01-06 03:43林胜仙吴艳琴孔微微
中国现代医生 2019年32期
林胜仙 吴艳琴 孔微微
[摘要] 目的 比较罗哌卡因与罗哌卡因联合地塞米松用于硬膜外分娩镇痛的疗效。 方法 选取2017年8月~2018年8月于我院经阴道分娩的初产妇60例,当产妇宫颈扩张≥4 cm,且变薄50%时被随机分为两组:A组(n=30)予硬膜外0.125%罗哌卡因,总体积为15 mL,B组(n=30)予硬膜外0.125%罗哌卡因联合地塞米松4 mg,总体积15 mL。在首次要求止痛时,通过硬膜外导管给药10 mL 0.125%罗哌卡因,每小时用8 mL 0.125%罗哌卡因进一步镇痛。主要观察指标是硬膜外镇痛时间,次要观察指标包括:阻滞前和阻滞后15 min视觉模拟量表疼痛评分、使用罗哌卡因总量、Apgar评分、脐静脉pH值、产妇满意度和副作用。 结果 B组的平均镇痛时间长于A组,差异有统计学意义(P<0.05)。A组的罗哌卡因总需求量高于B组,差异有统计学意义(P<0.05)。与阻滞前相比,阻滞后 A组和B组的VAS均低于阻滞前,差异有统计学意义(P<0.05)。B组T10平均感觉阻滞起效时间长于A组,差异有统计学意义(P<0.05)。B组的最高感觉阻滞平均时间長于A组,差异有统计学意义(P<0.05)。两组在最高感觉阻滞水平上无统计学差异,两组间无运动阻滞发生率。两组在血流动力学、疼痛评分、新生儿结局、产妇满意度和并发症方面无统计学差异。结论 硬膜外罗哌卡因联合地塞米松在治疗分娩疼痛时延长硬膜外镇痛时间,血流动力学稳定,母婴不良反应有限。
[关键词] 地塞米松;硬膜外镇痛;罗哌卡因;分娩镇痛
[中图分类号] R614 [文献标识码] B [文章编号] 1673-9701(2019)32-0111-04
Effect of ropivacaine combined with dexamethasone on epidural labor analgesia
LIN Shengxian1 WU Yanqin2 KONG Weiwei3
1.Department of Anesthesiology, the First Affiliated Hospital of Wenzhou Medical University, Wenzhou 325000, China;
2.Department of Anesthesiology, Wenzhou People's Hospital in Zhejiang Province, Wenzhou 325000, China; 3.Department of Anesthesiology, the Second Affiliated Hospital of Wenzhou Medical University, Wenzhou 325000, China
[Abstract] Objective To compare the efficacy of ropivacaine and dexamethasone on epidural labor analgesia. Methods 60 primiparas who underwent vaginal delivery in our hospital from August 2017 to August 2018 were enrolled. They were randomly divided into two groups: group A(n=30) was treated with epidural 0.125% ropivacaine, total volume 15 mL and group B(n=30) was treated with epidural 0.125% ropivacaine plus dexamethasone 4 mg, total volume 15 mL. At the first request for analgesia, 10 mL of 0.125% ropivacaine was administered via an epidural catheter and further analgesia was achieved with 8 mL of 0.125% ropivacaine per hour. The primary outcome measure was epidural analgesia time. Secondary observations included visual analog scale pain score, total ropivacaine use, Apgar score, umbilical vein pH, maternal satisfaction and side effects at pre- and post-blocking 15 minutes. Results The mean analgesia time in group B was longer than that in group A, and the difference was statistically significant(P<0.05). The total demand for ropivacaine in group A was higher than that in group B, and the difference was statistically significant(P<0.05). Compared with that before the block, the VAS of group A and group B was lower after block, and the difference was statistically significant(P<0.05). The onset time of T10 mean sensory block in group B was longer than that in group A, and the difference was statistically significant(P<0.05). The mean time of maximum sensory block in group B was longer than that in group A, and the difference was statistically significant(P<0.05). There was no significant difference in the level of maximum sensory block between the two groups, and there was no incidence of motor block in the two groups. There were no statistically significant differences in hemodynamics, pain scores, neonatal outcomes, maternal satisfaction and complications between the two groups. Conclusion Epidural dexamethasone combined with ropivacaine prolongs the time of epidural analgesia in the treatment of labor pain, with hemodynamic stability, and limited maternal and child adverse reactions.
[Key words] Dexamethasone; Epidural analgesia; Ropivacaine; Labor analgesia
随着疼痛生理学和治疗学知识的不断更新以及产科麻醉的不断发展,分娩镇痛的质量得到了显著提高[1]。硬膜外分娩镇痛是目前临床上应用最广泛的分娩镇痛方法,可以充分地减轻疼痛[2]。罗哌卡因是硬膜外分娩镇痛中最常用的局部麻醉药,具有良好的安全性。有研究表明,超声引导下地塞米松联合布比卡因肌间沟臂丛神经阻滞可延长术后镇痛时间[3]。地塞米松通过减少炎症、阻断伤害性C纤维的传导以及阻止神经的异位放电发挥作用[4]。一些研究表明硬膜外注射地塞米松不会出现相关并发症[5,6],其安全性也已得到证实[7]。本实验的目的是比较硬膜外单用罗哌卡因与罗哌卡因联合地塞米松用于分娩镇痛的疗效。
1 资料与方法
1.1 一般资料
选取2017年8月~2018年8月在我院分娩的初产妇60例,随机分为A组和B组(n=30)。纳入标准:①年龄18~35岁;②计划正常阴道分娩者;③美国麻醉师协会(ASA)1或2级;④无椎管麻醉禁忌证。排除标准:①硬膜外失败;②胎儿窘迫;③转为剖宫产;④患者中途拒绝。
1.2 方法
所有产妇入室后均常规建立静脉通道,并滴注乳酸林格氏液作为液体补充。监测产妇无创血压、脉搏血氧、心电图等。麻醉医生在消毒铺巾后,用2%的利多卡因进行局麻后,通过正中入路,用17 g穿刺针(Perfix,Braun,Germany)在L2/3或L3/4椎间隙行硬膜外穿刺,穿刺成功后留置硬膜外导管备用。产妇转为仰卧位,子宫左侧移位,以防止主动脉腔压迫。A组:穿刺成功产妇仰卧位后给予硬膜外0.125%罗哌卡因(AstraZeneca AB,10 mL:75 mg),总体积15 mL(n=30),并用微泵8 mL/h 0.125%罗哌卡因进一步镇痛。在产妇首次要求止痛时,通过硬膜外导管给予10 mL 0.125%罗哌卡因。再次出现疼痛时,通过硬膜外导管给予8 mL 0.125%罗哌卡因。B组:穿刺成功产妇仰卧位后给予硬膜外0.125%罗哌卡因联合地塞米松(天津金耀,H12020515,1 mL:5 mg)4 mg,总体积15 mL(n=30)。并用微泵8 mL/h 0.125%罗哌卡因进一步镇痛。在产妇首次要求止痛时,通过硬膜外导管给予10 mL 0.125%罗哌卡因。再次出现疼痛时,通过硬膜外导管给予8 mL 0.125%罗哌卡因。所有产妇均进行了随访和产程检查,并对疼痛和血流动力学进行评估。当平均动脉血压比基线降低>25%或心率<60用麻黄碱(东北制药,H21022412,1 mL:30 mg)10 mg或阿托品(浙江瑞新,H33020465,1 mL:0.5 mg)0.6 mg静脉推注。产科医生定期监测胎儿心率,并进行相应处理。
1.3 观察指标
观察并比较两组镇痛时间、产妇阻滞前和阻滞后15 min视觉模拟量表(VAS)(0=无疼痛,10=最严重疼痛)疼痛评分、使用罗哌卡因总量、新生儿结局(1、5 min的Apgar评分和脐静脉血pH值)、产妇满意度(非常满意=3,满意=2,一般=1,不满意=0)、T10感觉阻滞起效时间、最高感觉阻滞水平、时间以及并发症。
1.4 统计学方法
采用SPSS22.0软件进行统计分析。计数资料以[n(%)]表示,两组间比较采用χ2检验或Fisher精确检验。计量资料以(x±s)表示,两组间比较采用独立样本t检验或mann-whitney检验,P<0.05为差异具有统计学意义。
2 结果
2.1 两组一般资料比较
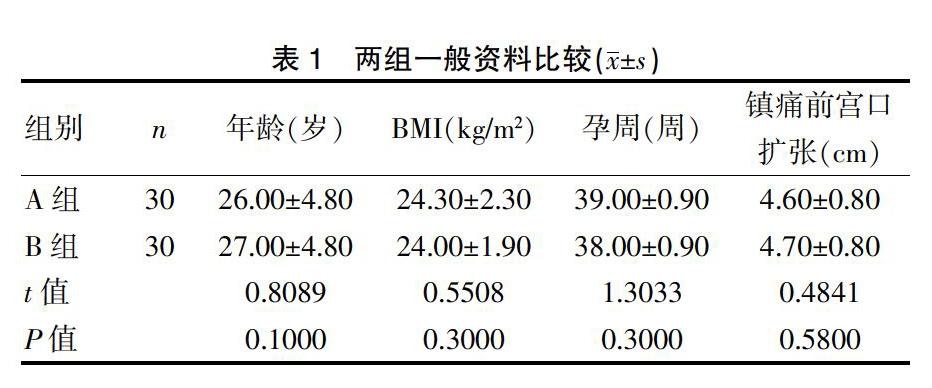
本研究包括60例产妇,分A组和B组(n=30),两组在年龄、孕周、体重指数、镇痛前宫口扩张等方面比较,差异无统计学意义(P>0.05),具有可比性。见表1。
表1 两组一般资料比较(x±s)
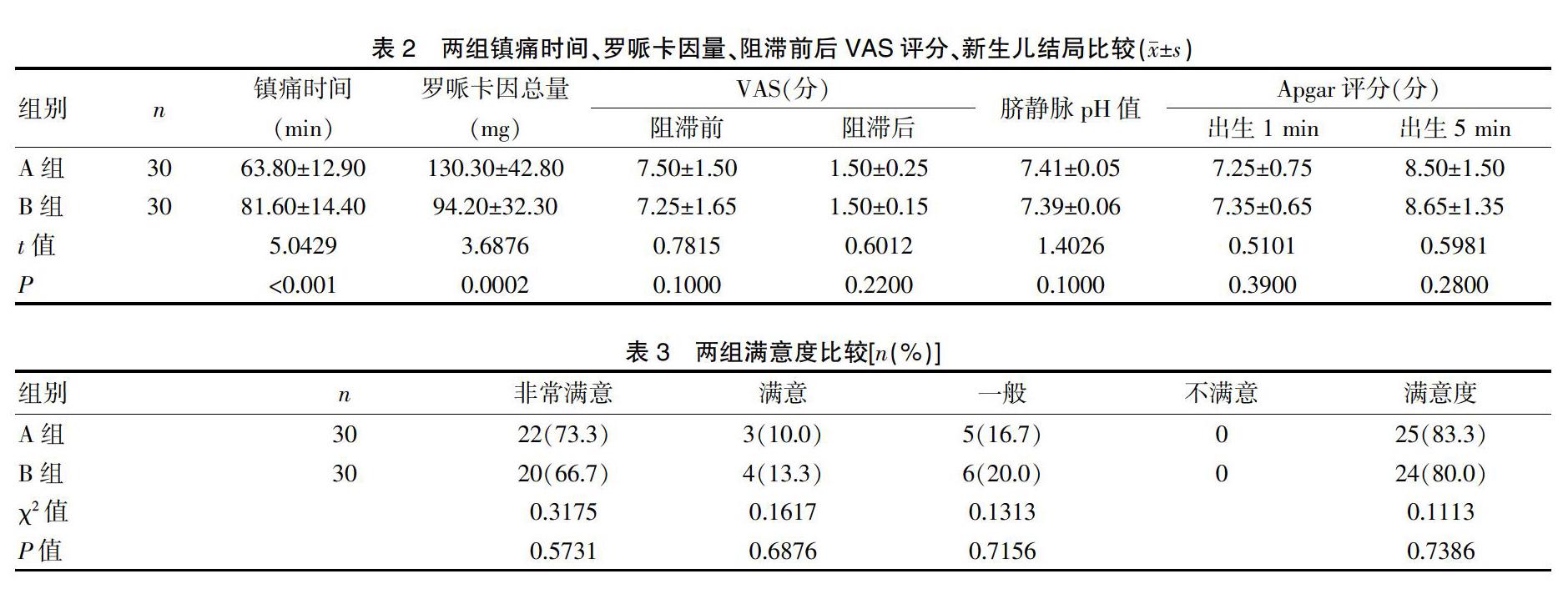
2.2 两组镇痛时间、罗哌卡因量、阻滞前后VAS评分、新生儿结局比较
B组的平均镇痛时间长于A组,差异有统计学意义(P<0.05)。B组的罗哌卡因总需求量低于A组,差异有统计学意义(P<0.05)。与阻滞前相比,阻滞后A组和B组的VAS均低于阻滞前,差异有统计学意义(P<0.05)。两组在脐静脉pH值、Apgar评分方面比较,差异无统计学意义(P>0.05)。见表2。
2.3 两组患者满意度比较
A组和B组在满意度方面比较,差异无统计学意义(P>0.05),见表3。
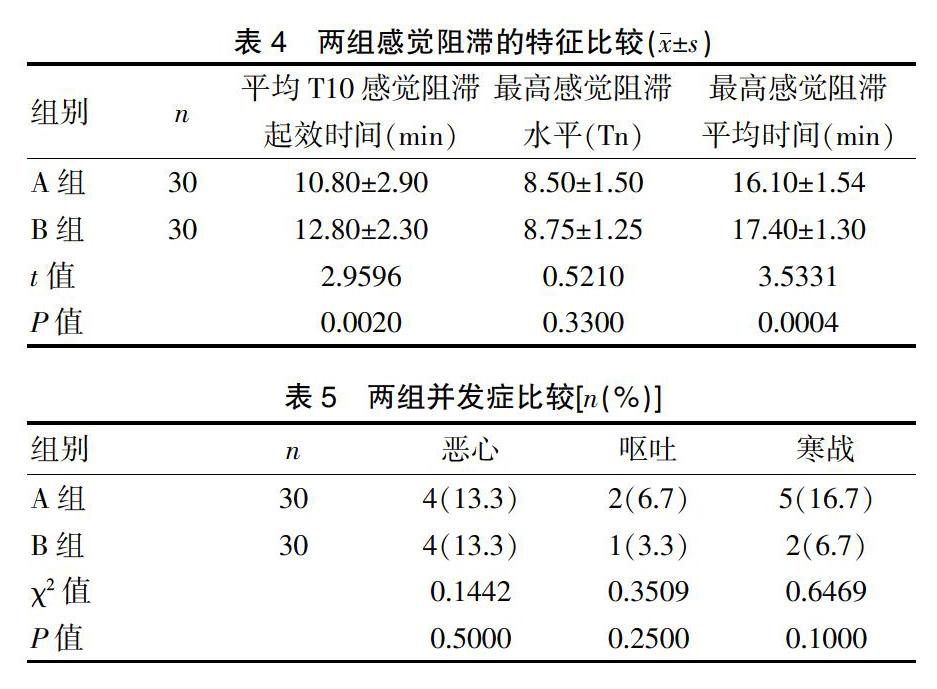
2.4 两组感觉阻滞的特征比较
B组平均T10感觉阻滞起效时间长于A组,差异有统计学意义(P<0.05)。B组的最高感觉阻滞平均时间长于A组,差异有统计学意义(P<0.05)。两组在最高感觉阻滞水平上无统计学差异(P>0.05),两组间无运动阻滞发生率。见表4。
2.5 兩组并发症比较
A组和B组在并发症方面比较,差异无统计学意义(P>0.05),见表5。
3 讨论
分娩时强烈疼痛不仅会使孕产妇出现焦虑、恐惧心理,还可能影响产程进展,增加剖宫产风险,因此,分娩镇痛已经成为临床工作的重点。为了延长镇痛时间,我们通过在局麻药中加入佐剂来延长镇痛持续时间。临床上已经使用几种佐剂,如阿片类药物、可乐定和维拉帕米,但是它们存在效果不确切或明显副作用等问题[8-10]。Mirzai H等[11]研究发现硬膜外皮质类固醇联合布比卡因可增强腰椎间盘手术术后镇痛作用。
目前关于皮质类固醇减轻疼痛的机制尚不十分清楚,当机体受到急性疼痛刺激时,椎管内的前列腺素生成增加,从而产生“痛觉敏化”现象。而皮质类固醇可以通过抑制磷脂酶A2和环加氧酶-2的表达以减少前列腺素的生成,从而减轻“痛觉敏化”[12]。有研究报道,神经外膜注射皮质类固醇能增强术后镇痛效果,它们通过减少炎症和阻断伤害性C纤维的传导以及阻止C纤维神经的异位放电来减轻疼痛[13]。由于这种作用是可逆的,因此类固醇可能对细胞膜有直接作用,类固醇可以通过改变可兴奋细胞中钾通道的功能来引起这种效应[14]。此外,有人认为糖皮质激素可以直接与细胞内糖皮质激素受体结合,通过基因转录直接影响特定蛋白质的合成,从而干扰疼痛信号的传导。
目前尚未有研究確定硬膜外地塞米松用于术后镇痛的最佳剂量。本研究中地塞米松使用的剂量是4 mg,此剂量对成人是相对安全的[15]。本研究结果显示B组的平均镇痛时间长于A组,B组的罗哌卡因总需求量明显少于A组,结果表明硬膜外给予地塞米松可明显增强罗哌卡因的镇痛作用,延长分娩镇痛持续时间,减少罗哌卡因总需求量。本研究结果与Khafagy等[16]的研究结果一致,其研究硬膜外布比卡因中加入地塞米松或芬太尼对术后镇痛效果的影响,结果表明地塞米松组和芬太尼组延长术后镇痛时间,减少阿片类药物的需求。Thomas等[17]的研究表明术前硬膜外给予地塞米松5 mg可减少术后疼痛和阿片类的需求。El-Feky EM等[18]的研究比较了芬太尼、右美托咪定和地塞米松作为布比卡因佐剂用于骶管阻滞镇痛,研究结果表明与单纯局麻药或芬太尼相比,在术后延长疼痛缓解时间上,骶管麻醉布比卡因中加入右美托咪定和地塞米松效果较好,与芬太尼相比,右美托咪定和地塞米松的副作用更小。此外,在Kirksey等[19]的对佐剂相关的随机对照试验和meta分析进行系统回顾的研究中得出结论,一些药物如丁丙诺啡、可乐定、地塞米松、镁等可增强神经阻滞的局部麻醉效果。但是,一些研究结果与前面的发现相反,Lotfinia等[20]研究表明硬膜外注射甲基强的松龙或布比卡因不能缓解腰椎间盘切除术后背部和神经根的疼痛。Abdel-Aleem等[21]研究发现硬膜外8 mg地塞米松联合布比卡因对剖宫产患者VAS评分和术后阿片类药物的消耗没有影响。但是,Hefni AF等[22]研究发现硬膜外给予高剂量的地塞米松比低剂量的地塞米松能更有效地控制中度到重度疼痛。Liu等[23]对7项随机对照试验进行了meta分析,比较低浓度布比卡因硬膜外输注与注射阿片类对产妇剖腹产率的影响,结果表明使用低浓度布比卡因注射硬膜外镇痛没有增加剖腹产的风险,且疼痛缓解效果更好。本研究中两组在新生儿结局、患者满意度以及恶心、呕吐和颤抖等并发症方面差异无统计学意义,表明罗哌卡因联合地塞米松硬膜外分娩镇痛对新生儿和产妇的不良反应有限。
综上所述,本研究结果表明罗哌卡因联合地塞米松硬膜外分娩镇痛能延长镇痛时间,减少罗哌卡因用量,且母婴不良反应有限,值得临床参考和借鉴。
本研究的局限性在于硬膜外地塞米松的剂量及其在分娩过程中的给药时间需要进一步研究,从而在局麻药累积剂量较低的情况下,达到最佳的分娩镇痛。产后镇痛是地塞米松的另一个优势,但这超出了本研究的范围。在未来的研究中,可以对更多的患者进行更加深入的研究。
[参考文献]
[1] Pandya ST. Labour analgesia:Recent advances[J]. Indian J Anaesth,2010,54(5):400-408.
[2] IndraccoloU,Ripanelli A,Di IR,et al. Effectof epidural analgesia on labor times and mode of delivery:A prospective study[J]. Clin Exp Obstet Gynecol,2012,39(3):310-313.
[3] Vieira PA,Pulai I,Tsao GC,et al. Dexamethasone with bupivacaine increases duration of analgesiain ultrasound-guided interscalene brachial plexus blockade[J]. Eur J Anaesthesiol,2010,27(3):285-288.
[4] Dhimar A,Golwala MP,Swadia VN,et al. Pain relief by dexamethasone as an adjuvant to local anesthetics insupraclavicular brachial plexus block[J]. J Anesth Clin Pharmacol,2009,25(3):285-288.
[5] Maleh PA,Bani-Hashem N,Nabavi A,et al. Addition of intrathecal Dexamethasone to Bupivacaine for spinal anesthesia in orthopedic surgery[J]. Saudi Journal of Anaesthesia,2011,5(4):382-386.
[6] Kotani N,Kushikata T,Hashimoto H,et al. Intrathecal methylprednisolone for intractablepostherpetic neuralgia[J].N Engl J Med,2000,343(3):1514-1519.
[7] Price C,Arden N,Coglan L,et al. Cost-effectiveness and safety of epidural steroids in the management of sciatical[J].Health Technol Assess,2005,9(1):1-58.
[8] Wakhlo R,Gupta V,Raina A,et al. Supraclavicularplexus block:Effect of adding tramadol or butorphanol as anadjuncts to local anaesthetic on motor and sensory block andduration of post-operative analgesia[J]. J Anaesth Clin Pharmacol,2009,25(1):17-20.
[9] Gabriella I,Adnane M,Desire-Pascal D,et al.The effects of clonidine added tomepivacaine for paronychia surgery under axillarybrachial plexus block[J]. Anesth Analg,2005, 100(4):1179-1183.
[10] Lalla RL,Anant S,Nanda HS. Verapamil as an adjunct to localanaesthetic forbrachial plexus blocks[J]. MJAFI,2010,66(1):22-24.
[11] Mirzai H,Tekin I,Alincak H. Perioperative use of corticosteroid and bupivacaine combination in lumbar disc surgery:A randomized controlled trial[J]. Spine,2002,27(4):343-346.
[12] Waldron NH,Jones CA,Gan TJ,et al. Impact of perioperative dexamethasone on postoperative analgesia and side-effects:Systematic review and meta-analysis[J]. Br J Anaesth,2010,105(4):506-510.
[13] Benzon HT.Epidural steroids.In:Raj PP,editor.Pain Medicine:A Comprehensive Review[M].Maryland Heights:Mosby,1999:259-263.
[14] Attali B,Latter H,Rachamim N,et al. A corticosteroid-inducedgene expressingan “IsKlike” K+ channel activity in Xenopusoocytes[J]. Proc Natl Acad Sci USA,1995,92(13):6092-6096.
[15] Amr SW,Ahmed IE,Amira RH,et al. Epidural levobupivacaine versus a combination of levobupivacaine and dexamethasone in patients receiving epidural analgesia[J].Journal of Anaesthesiology Clinical Pharmacology,2019, 35(1):109-113.
[16] Khafagy HF,Refaat AI,El-Sabae HH,et al. Efficacy of epidural dexamethasone versus fentanyl on postoperative analgesia[J]. J Anesth,2010,24(4):531-536.
[17] Thomas S,Beevi S. Epidural dexamethasone reduces postoperative pain and analgesic requirements[J]. Can J Anaesth,2006,53(9):899-905.
[18] El-Feky EM,Abd El,Aziz AA. Fentanyl,dexmedetomidine,dexamethasone as adjuvant to local anesthetics in caudal analgesia in pediatrics:A comparative study[J]. Egypt J Anaesth,2015,31(2):175-180.
[19] Kirksey MA,Haskins SC,Cheng J,et al. Local anesthetic peripheral nerve block adjuvants for prolongation of analgesia:A systematic qualitative review[J]. PLoS One,2015,10(9):e0137312.
[20] Lotfinia I,Khallaghi E,Meshkini A,et al. Interaoperative use of epidural methylprednisolone or bupivacaine for postsurgical lumbar discectomy pain relief:A randomized,placebo-controlled trial[J]. Ann Saudi Med,2007, 27(4):279-283.
[21] Abdel-Aleem M,Osman A,Morsy K. Effect of coadministration of dexamethasone with intrathecal morphine on postoperative outcomes after cesarean delivery[J]. Int J Gynaecol Obstet,2012,116(2):158-161.
[22] Hefni AF,Mahmoud MS,Al Alim AA. Epidural dexamethasone for post-operative analgesia in patients undergoing abdominal hysterectomy:A dose ranging and safety evaluation study[J]. Saudi J Anaesth,2014,8(3):323-327.
[23] Liu E,Sia T. Rates of caesarean section and instrumental vaginal delivery innulliparous women after low concentration epidural infusions or opioid analgesia:Systematic review[J]. BMJ,2004,328(7453):1410-1412.
(收稿日期:2019-07-15)
猜你喜欢
中国典型病例大全(2022年10期)2022-05-10
中华养生保健(2020年1期)2020-11-16
特别健康·下半月(2017年3期)2017-04-19
中国卫生标准管理(2015年13期)2016-01-15
中国当代医药(2015年30期)2015-03-01
中国当代医药(2015年20期)2015-03-01
中国当代医药(2015年8期)2015-03-01
中国药业(2014年17期)2014-05-26
河北医科大学学报(2010年9期)2010-03-25