
Speckle Tracking Echocardiography ldentifies lmpaired Longitudinal Strain as a Common Deficit in Various Cardiac Diseases
2018-09-17 08:46:38RandyJeffreyMDPhDRobertHamburgerDOMPHJanelleGoodenEbanksMDandJohnPetersenMDMS
Randy R. Jeffrey, MD, PhD, Robert F. Hamburger, DO, MPH, Janelle Gooden-Ebanks, MD and John W. Petersen, MD, MS
1Division of Cardiovascular Medicine, University of Florida, Gainesville, FL, USA
Abstract The use of speckle-tracking echocardiography (STE) is becoming an increasingly useful tool in the evaluation of myocardial disease. STE software can track the motion of the specular pattern created by the interference of ultrasound with the myofibers of the heart and provide a quantitative means to evaluate subtle changes in ventricular function that often occur before changes in ventricular ejection fraction are observed. STE is most often used to measure the change in shape (strain) of myocardial segments in the circumferential, radial, and longitudinal directions. In various diseases,including coronary artery disease, aortic stenosis, and mitral regurgitation, deficits in longitudinal strain appear to occur earlier than deficits in other measures of strain or in ejection fraction. Consideration of STE measures of left ventricular contraction has the potential to significantly affect clinical management and outcomes of ischemic and valvular heart disease given the ability to separate those with asymptomatic disease who may benefit from earlier interventions than current guidelines may suggest.
Keywords: speckle tracking echocardiography; longitudinal strain; valvular heart disease, ischemic heart disease;echocardiographic imaging
Measures of Left Ventricular Function
Measures of left ventricular (LV) function are essential to the daily care of patients and in the study of cardiovascular disease. The most common measure of LV systolic function is ejection fraction (EF).Unfortunately, EF fails to identify the mechanism of LV systolic dysfunction in nearly half of patients with heart failure [1]. In patients with heart failure and preserved EF, it is common to evaluate Doppler measures of LV diastolic function. Similarly to EF, Doppler measures of diastolic function are often normal in patients with heart failure [2].Fortunately, advances in noninvasive imaging have provided new methods to measure LV mechanics and have improved our ability to identify the LV deficit responsible for symptoms and outcomes.
Interference of ultrasound with the myofibers of the heart creates a specular pattern in the myocardium. Speckle tracking echocardiography(STE) software can track the motion of this specular pattern and therefore track the motion of myocardial segments. STE can quantify the change in shape of a myocardial segment. Typically, STE is used to measure the change in shape of all myocardial segments along three orthogonal axes of the heart (radial, circumferential, and longitudinal)(Figure 1) [3]. Strain is the percent change in shape of a myocardial segment from the end of diastole to peak contraction. STE has been shown to have appropriate interobserver and intraobserver reliability. Additionally, STE measures of myocardial contractility had a reasonable level of agreement and reproducibility when software from different vendors was compared [4, 5].
Normal Left Ventricular Mechanics
STE has expanded our understanding of normal LV mechanics and cardiac physiology. The myofibers of the left ventricle have a helical orientation that contributes to efficient contraction. While myofiber orientation is different at subendocardial and subepicardial levels, the subepicardial fiber orientation determines the overall twisting that occurs in the normal human heart. The twisting of the heart was not easily measured with traditional measures of LV function. STE can quantify the twisting of the heart,and both STE and invasive sonomicrometry have demonstrated a counterclockwise rotation of the LV apex and clockwise rotation of the LV base during systole in healthy hearts when viewed from the LV apex [6].
STE has also expanded our understanding of the timing and magnitude of the shortening of the heart along its long axis, which is calledlongitudinal strain. After depolarization of the LV subendocardium, there is first longitudinal shortening in the LV apex followed by longitudinal shortening in the LV base that results in a descent of the LV base and mitral annulus toward the LV apex. This longitudinal shortening of the left ventricle, which is not measured with routine echocardiography techniques, is controlled predominately by the function of the subendocardial fibers of the left ventricle [7].Longitudinal strain, which is now frequently measured with STE, is most commonly reported as global longitudinal strain (GLS), which is a measure of longitudinal contraction of all LV segments.A negative GLS indicates that the left ventricle shortens during systole. Studies of healthy individuals have reported normal GLS in a range from −16 to −22%. In other words, in healthy individuals the left ventricle shortens during systole by 16–22% of its length at the end of diastole. In a meta- analysis the average GLS for healthy individuals was−20% [8]. Longitudinal strain is not uniform around the circumference of the left ventricle and is typically greatest in the inferior and inferolateral LV segments [9].
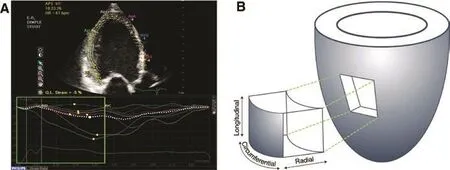
Figure 1 Speckle Tracking Echocardiography (STE) and the Three Orthogonal Axes of the Left Ventricle.
This impressive sequence of events in the various regions of the left ventricle contributes to important blood flow patterns within the left ventricle.The coordinated sequence of LV contraction and relaxation leads to a swirling vortex of blood in the left ventricle. This vortical blood flow that occurs during isovolumic, ejection, and relaxation periods is an efficient flow pattern that optimizes blood ejection [10]. Further, the character of the vortical blood flow pattern changes in patients with abnormal myocardial contraction and relaxation [11].
Abnormal Left Ventricular Mechanics
STE has shown that various cardiac diseases impact LV mechanics in a similar way. The earliest changes in LV mechanics are similar in myocardial ischemia from obstructive coronary artery disease (CAD),pressure overload, and volume overload conditions. All of these conditions appear to first impact longitudinal contraction. STE has the advantage of detecting the abnormal LV longitudinal mechanics that are present in the early stages of these various diseases before abnormalities are seen with standard cardiac ultrasonography.
Myocardial lschemia
Although myocardial ischemia can affect the myocardium in a transmural fashion, the subendocardial myocardial tissue is the most vulnerable to decreases in myocardial perfusion since it is perfused by the most distal part of the coronary circulation [12, 13]. On a macroscopic level, these changes may present as localized wall motion abnormalities seen on standard echocardiography.However, in some instances ischemia may not result in wall motion abnormalities easily seen on standard echocardiographic images. STE can more readily detect subtle changes in myocardial contraction. With the predominant longitudinal orientation of myocardial fibers in the subendocardium, one of the initial functional impacts of ischemia results in a reduction of longitudinal contraction [14–18].Depending on the extent of myocardial ischemia,as demonstrated in animal models, circumferential and radial strain could be maintained or decreased[16, 19]. In some instances, global circumferential strain may actually increase to compensate for the loss in longitudinal contraction [20]. The localization of longitudinal strain to the subendocardial territory is further exemplified by observations that while subendocardial and transmural infarctions both demon strate reduced longitudinal strain, it is only with transmural injury that reductions in circumferential strain are observed [21, 22].
Stress Testing
The ability of STE to measure subtle deficits in contractility caused by myocardial ischemia suggest that it may increase the 78–85% sensitivity to detect obstructive CAD observed with standard stress echocardiography techniques [23, 24]. Longitudinal strain has been shown to be the earliest component of contractility affected by ischemia [15, 16, 18],and thus measurement of regional/segmental longitudinal strain and GLS can help identify myocardial dysfunction caused by ischemia. Although CAD and the resulting ischemia is often more a regional phenomenon, the use of GLS to evaluate patients for evidence of ischemia has been more commonly reported. The reasoning is in part due to the reproducibility of GLS measures on stress echocardiography between readers of differing experience [25],across ultrasound platforms [26], and likely because of ease of use.
The inclusion of STE in stress echocardiography has shown to increase the sensitivity and specificity of detecting obstructive CAD as compared with wall motion analysis alone (Table 1). Ng et al. [27]demonstrated that STE using GLS cutoffs of 20%LV systolic shortening at peak stress in combination with wall motion analysis during dobutamine stress echocardiography increased sensitivity and specificity for detection of significant CAD from 76% and 82.1% to 100% and 96.3%, respectively[27]. Similar incremental improvements in diagnosis of CAD were seen in several other studies that included strain analysis [28, 29, 31, 32, 38–40]. The success of STE has also been shown to be independent of wall motion analysis in dobutamine stress echocardiography. During dobutamine stress testing of patients with moderate to high risk of CAD,a GLS cutoff of 19% LV systolic shortening at peak stress was found to be 94% sensitive and 92% specific in detection of hemodynamically significant coronary lesions [30]. The use of GLS during stress echocardiography has also demonstrated the capacity to detect changes in myocardial function at lower doses of dobutamine (10 μg/kg/min) than are typically required to detect standard wall motion abnormalities [41]. In patients referred for evaluation of angina or suspected non–ST-segment elevation myocardial infarction, use of STE can also establish those patients likely to have significant CAD on the basis of the resting echocardiogram alone without need for stress testing. In a study by Choi et al. [32],the use of a GLS cutoff of 17.9% LV systolic shortening was able to predict those patients with severe CAD (left main or three-vessel disease) on a resting echocardiogram with normal LV EF (LVEF) and no wall motion abnormalities on standard echocardiography with a sensitivity and specificity of 79%.
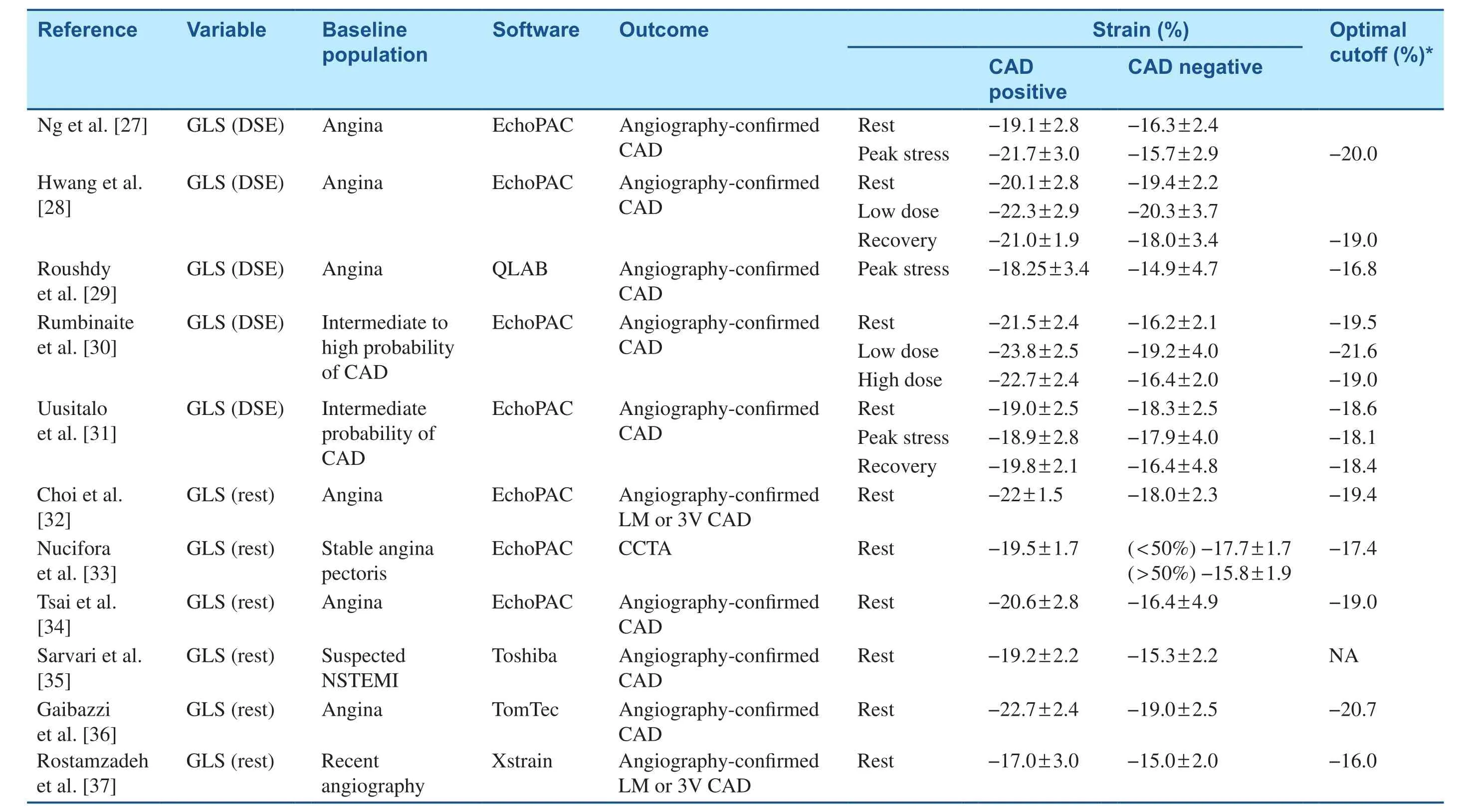
Table 1 Studies of Longitudinal Strain in Patients with Obstructive Coronary Artery Disease (CAD).
Unfortunately, use of STE does pose some problems, which can limit its successful implementation.As with other imaging modalities, interpretation is highly reliant on image quality and reproducibility.Additionally, the lack of clear consensus regarding normal values and what definitively represents positive or ischemic strain findings is still not established. Table 1 displays the various software used to assess STE in patients with suspected ischemic heart disease and demonstrates the variable cutoff points for abnormal LV function suggested by numerous studies. As an example, the difference in the change of GLS in patients identified as having significant CAD during stress echocardiography testing from those without could range from 1.0% to more than 5% [27–29, 31, 38, 42, 43]. Similarly, the cutoffs of minimum GLS measurements determined to represent significant underlying ischemia at rest are also highly variable, and have been reported from 16.0% to 20.7% LV systolic shortening [28, 32–37,44–47].
Aortic Stenosis and Surgical Timing
STE has been shown to be an effective tool to identify subtle changes in myocardial function that can occur in patients with aortic stenosis (AS) before changes in EF [48]. AS leads to maladaptive LV remodeling that includes subendocardial ischemia and fibrosis [49]. Subendocardial myofiber function dictates LV longitudinal contraction. Therefore with advanced AS it is not surprising that longitudinal strain is impaired. GLS differs significantly depending on the severity of valve stenosis, with values of 17.1%, 16.4%, and 14.5% LV systolic shortening for mild, moderate, or severe stenosis, respectively, despite a maintained LVEF [50]. In addition to GLS, endocardial radial strain is also found to be decreased in proportion to the severity of the disease [51]. Interestingly, although circumferential and epicardial radial strain are often found to be preserved in asymptomatic AS [51], in patients with symptomatic disease, it is the circumferential strain indices that are found to be depressed, in addition to significantly greater observed declines in longitudinal strain [52–55]. Of note, in individuals with the variant low-flow low-gradient severe AS, longitudinal strain is found to be even further decreased compared with that in individuals with high- gradient AS (11.6% vs. 14.8% LV shortening),suggesting that progressive longitudinal dysfunction may be a contributing factor to the low-flow AS phenomenon [52]. These observations suggest that in patients with asymptomatic severe AS, decreases in longitudinal strain can identify high-risk candidates for aortic valve replacement (AVR). At present, there is no clear consensus regarding minimum changes or absolute GLS that should warrant earlier intervention for AS treatment. However, it has been shown that in patients with normal or depressed LVEF undergoing transcatheter AVR or surgical AVR, those with impaired GLS had a significantly higher risk of cardiac morbidity and death [56–60].The range of cutoffs observed for GLS that appear to show improved outcome after AVR in normal LVEF patients are broad, and range from 12.1%to 17.8% LV shortening (Table 2) [56, 57, 59–65].At the least, these observations suggest that in patients with severe AS and a declining GLS, early AVR should be considered.
Following definitive procedural intervention,significant reductions in the transaortic gradient are observed with associated improvements in LV strain patterns. Following either surgical or transcatheter AVR, significant increases in longitudinal strain have been observed, with noted increases
in LV systolic shortening on average of 3.2% [54,58, 66–68]. Additionally, studies have shown that increases in circumferential and radial strain also occur following successful procedural intervention[54, 69, 70].

Table 2 Studies of Longitudinal Strain in Aortic Stenosis (AS).
Ultimately, the ability to predict the optimal timing of AVR before onset of irreversible myocardial remodeling remains the goal; however, because of the lack of clear clinical data and variability in the GLS ranges where patients were shown to have clinical benefit, routine implementation of STE for guiding early AS intervention is not yet defined.However, with further study and greater use of STE in evaluation of AS, establishment of consensus data will be available in the future.
Mitral Regurgitation and Surgical Timing
Similarly to AS, surgical intervention for mitral regurgitation (MR) is indicated in the presence of symptoms and in asymptomatic patients who develop LV dysfunction. However, simply “waiting” for LV dysfunction to develop, as defined with standard echocardiographic measures, in an asymptomatic patient is not an appropriate strategy as it is known that increasing LV dysfunction results in worse outcomes after surgery [71]. Owing to favorable loading conditions from decreased afterload and increased preload, LVEF usually remains elevated during the early course of severe MR. But chronic volume overload, increased wall stress, and resultant remodeling lead to myocardial dysfunction and eventually a drop in EF [72]. As certain components of myocardial function become impaired before the development of this drop in EF, the use of STE has been studied as a possible modality for the detection of this early myocardial dysfunction. For example,Kim et al. [73] showed that reduction in longitudinal strain rate occurs earlier than reductions in circumferential and radial strain in patients with severe MR and precedes a drop in more traditional measures of LV function (such as LVEF and dP/dt).Surgical timing in patients with asymptomatic severe MR remains controversial. STE may provide insight into which asymptomatic patients will be at higher risk of developing heart failure and other related adverse cardiac events. In a cohort of patients with severe MR and normal LVEF, patients who required mitral valve surgery during the follow-up period had a lower GLS as compared with those who did not require surgery (19% vs. 21%)[74]. Additionally, the increase in GLS during bicycle exercise testing was lower in those patients who required surgery as compared with those who did not (1.7% vs. 3.4%). Changes in GLS during exercise testing were predictive of changes in LVEF at follow-up. Magne et al. [75] also studied patients with asymptomatic severe primary MR with normal LVEF by performing exercise stress echocardiography, and found that the inability to increase GLS by 2% or more with exercise was superior to LVEF in predicting adverse cardiac events. LV strain evaluated with 3D techniques has also been shown to predict clinical outcomes in patients with severe MR [76]. In asymptomatic patients with severe MR and normal LVEF, 3D GLS was lower in patients with subsequent clinical events as compared with those with no events (15.8% vs. 17.9%),with an optimal cutoff point suggested at 14.3% by receiver operating curve analysis. Interestingly, a novel measure of subendocardial function calledarea strain, which integrates longitudinal and circumferential strain using 3D data, provided the best prediction of event-free survival in multivariate Cox regression.
STE may also be able to predict which patients will have worse outcomes postoperatively.Numerous studies have shown that impaired GLS predicts worsening LVEF after surgery, with cutoffs ranging from 18% to 20.5% LV systolic shortening(Table 3) [74, 76–79]. De Isla et al. [80] showed that longitudinal strain rate at the level of the midventricular septum (<−0.80/s) was the best predictor of a drop in LVEF of more than 10% postoperatively.Alashi et al. [77] found that both GLS and brain natriuretic peptide level when combined with traditional risk factors, such as Society of Thoracic Surgeons score, improved prognostic information regarding postoperative mortality. A preoperative GLS below 20.7% LV systolic shortening in the setting of an elevated brain natriuretic peptide level was predictive of postoperative death. These studies emphasize the importance of incorporating STE measures of longitudinal strain in the decision of surgical timing,and suggest that earlier intervention in patients with asymptomatic severe MR and borderline abnormalities in GLS should be considered.
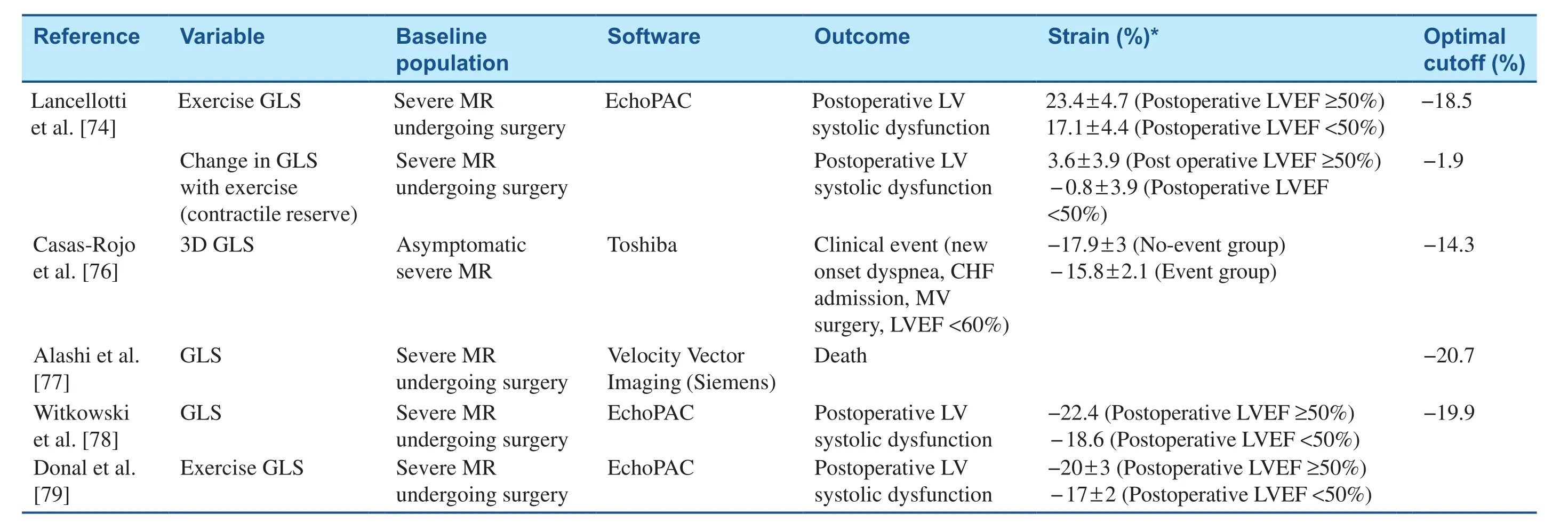
Table 3 Studies of Myocardial Strain in Patients with Severe Mitral Regurgitation (MR).
Percutaneous edge-to-edge repair of the mitral valve is an evolving intervention for the treatment of MR. Multiple studies have been performed using speckle tracking to follow the response of the left ventricle to this intervention. In patients with severe primary MR who receive the mitral valve clip, GLS is initially reduced in the immediate postprocedure setting [81]. Similar reductions were shown in prior studies immediately after operative repair before eventual improvement and have been attributed to immediate changes in loading conditions [82, 83].Multiple authors have shown significant improvements in GLS after mitral valve clip intervention anywhere from 1 month to 6 months after the procedure [84–86].
Left Ventricular Dyssynchrony
Dyssynchrony is typically defined as a difference in the time to peak contraction between different LV segments [87]. LV dyssynchrony is a significant risk factor for adverse cardiac outcomes [88].To address this phenomenon, cardiac resynchronization therapy (CRT) has been used as mainstay treatment with success rates of up to 67% when devices are implanted per standard guidelines [89].This modest degree of CRT efficacy prompted further investigation into the relationship between LV mechanics and CRT outcomes.
STE can define the timing of contraction of all of the LV segments. Dyssynchrony has been measured by comparison of the time to peak of radial, circumferential, and longitudinal strain between LV segments. Dyssynchrony is most commonly measured with radial strain. Studies of radial strain have provided encouraging evidence of its role in identifying likely responders to CRT and in guiding optimal lead placement [90, 91]. Consideration of longitudinal strain appears to also aid in the evaluation of patients with dyssynchrony. Longitudinal dyssynchrony as assessed by the time to peak velocity of two sites with tissue Doppler imaging (≥60 ms) and radial dyssynchrony evaluated by speckle tracking(two sites ≥130 ms) were compared for predictive value [92]. When either longitudinal or radial dyssynchrony was present, there was a 15% or greater increase in EF in 59% of the patients. Conversely,if both longitudinal and radial dyssynchrony were present at the baseline, then there was a 95%response to CRT versus a 10% response if neither was present.
In addition to documenting dyssynchrony that is likely to respond to CRT, longitudinal strain may also help identify those patients with more advanced cardiomyopathy who might not benefit from CRT. D’Andrea et al. [93] studied 45 consecutive patients with ischemic dilated cardiomyopathy and an upcoming CRT procedure. GLS of 12% or less correlated with 84.7% sensitivity and 88.8%specificity in predicting no response to CRT.
In summary, although further investigation is warranted to optimally determine which patients will have the most favorable outcomes, at this time the body of literature suggests that patients with longitudinal and radial dyssynchrony detected on STE incur significant benefit with CRT. Further,longitudinal strain may provide an important predictor of benefit in patients with more advanced cardiomyopathies.
Conclusions and Future Directions
Standard measures of LV systolic function, such as EF, fail to identify LV dysfunction and guide management in various cardiac diseases. STE software can track the motion of the myocardium throughout the cardiac cycle and quantify the shortening of the myocardium along the long axis of the left ventricle during systole. Impairment of longitudinal systolic shortening of the left ventricle appears to be an early mechanical deficit in multiple cardiac diseases and is not measured with standard echocardiographic analysis. The level of impairment in longitudinal strain that indicates the need for change in patient management has been variable across studies and different software programs, and thus ongoing evaluation of the optimal cutoff point of GLS in guiding therapy for various conditions is required.The available studies have suggested that a GLS below 16–20% LV systolic shortening at peak stress improves our identification of angiographyconfirmed obstructive CAD. The optimal GLS cutoff that predicts preoperative events in patients with asymptomatic severe AS has had a significant range across studies, but many have suggested that a GLS below 15% LV systolic shortening is predictive of poor outcome. Further, a GLS below approximately 15–18% LV systolic shortening predicts preoperative events and postoperative LV systolic dysfunction in patients with asymptomatic severe MR.
Efforts at ensuring that standardized measures of GLS and other parameters of strain are reliably available across various echocardiographic systems are necessary. Additional studies confirming that use of standardized measures of GLS can appropriately guide the timing of valvular intervention are required. In addition to GLS, more advanced measures of LV function may enhance our evaluation of cardiac function, and preliminary study encourages ongoing investigation. For example, STE can not only determine GLS for the entire left ventricle but can also quantify longitudinal contraction in the subendocardial and subepicardial layers of the myocardium. Initial studies suggest that impairment of longitudinal contraction in the subendocardial layer has the best correlation with AS severity and may therefore provide the best measure to determine optimal surgical timing [94]. Consideration of loading conditions when one is interpreting STE-determined measures of strain may also be important as this may better approximate the power of the ventricle. Longitudinal strain adjusted for both systolic and diastolic blood pressure has been shown to be a powerful predictor of cardiovascular events in patients without known cardiovascular disease [95].Further study could help determine if longitudinal strain adjusted for blood pressure could better predict outcomes in patients with CAD or valvular heart disease.
Conflict of lnterest
The authors declare that they have no conflicts of interest.
 Cardiovascular Innovations and Applications2018年3期
Cardiovascular Innovations and Applications2018年3期
- Cardiovascular Innovations and Applications的其它文章
- Cardiovascular Innovations and Applications
- The Contemporary Role of Femoral Artery Access
- Persisting Angina after Successful Surgical Removal of a Large Coronary Artery Aneurysm Attached to the Proximal Portion of the Left Circumflex Artery: Role of Coronary Artery Spasm
- Bioresorbable Vascular Scaffold in the Midportion of the Left Anterior Descending Artery for Cardiac Allograft Vasculopathy in a Cardiac Transplant Patient
- The Use of Direct Oral Anticoagulants for Prevention of Stroke and Systemic Embolic Events in East Asian Patients with Nonvalvular Atrial Fibrillation
- Current Status of Coronary Atherectomy