
Implementation and assessment of diverse strategies for physical activity promotion in Vietnam—A case report
2018-04-26 07:39GbriellBekviHenrikssonThuHoiNguyenJuliKilheAgnesNorstrSofieSvenssonThiThnhHuongTrnIngeborgVnDerPloegCrlJohnSunberg
Gbriell Bekvi-Henriksson*,Thu Hoi Nguyen,Juli Kilhe,Agnes Norström,Sofie Svensson,Thi Thnh Huong Trn,Ingeborg Vn Der Ploeg,Crl John Sunberg,e,*
aDepartment of Physiology&Pharmacology,Karolinska Institutet,Stockholm 17177,Sweden
bDepartment of Neurobiology,Care Sciences and Society,Division of Physiotherapy,Karolinska Institutet,Huddinge 14183,Sweden
cNational Geriatric Hospital,Hà Nô·i 100000,Vietnam
dDepartment of Ethics&Social Medicine,Hanoi Medical University,Hà Nô·i 100000,Vietnam
eUnit for Bioentrepreneurship,Department of Learning,Informatics,Management and Ethics,Karolinska Institutet,Stockholm 17177,Sweden
1.Introduction
Physical activity(PA)is effective in the prevention and treatment of many non-communicable diseases(NCDs)such as cardiovascular diseases,type 2 diabetes,certain types of cancer,dementia,and depression.1The World Health Organization(WHO)has recognized physical inactivity as the fourth leading underlying risk factor for premature death,causing over 5 million deaths per year,worldwide.2,3Despite these facts,a more sedentary lifestyle is spreading,not only in high-income,but also in middle-and low-income countries.2
To address this negative trend,it is imperative to study and implement contextualized methods to increase PA both in the public at large and in specific patient groups.Several methods have shown to increase PA among patients in health care and community settings.4In Sweden,the method Physical Activity on Prescription(PAP)has been used for almost 2 decades and is recognized as an effective method to increase PA among patients in health care settings.The self-reported adherence to PAP is shown to be 50%-65%,which is comparable to the adherence rates found in studies of drug prescriptions.5In addition,self assessed quality of life is improved following PAP.6The guidelines for disease preventing methods,issued by the National Board of Health and Welfare in Sweden,states that“health care services should offer counseling as well as written prescriptions or pedometers and special follow-ups to individuals with insufficient levels of PA”.Official documents on national,regional,and local level support the use of the PAP method.6The evidence-based handbookPhysical Activity in the Prevention and Treatment of Diseasethat accompanies PAP(referred to as FYSS in Swedish)describes the evidence for the use of PA in prevention and treatment of more than 30 conditions and diseases.7FYSS is a tool for health care professionals to use when prescribing PA,as it provides recommendations for the most effective type and dose(intensity,frequency,and duration)of PA for each condition.8
The Swedish version of PAP consists of 5 components:(1)patient-centered counseling,(2)use of the evidence-based handbook FYSS,(3)individualized written prescription,(4)collaboration between health care and societal organizations,such as sports clubs,and(5)follow-up.5Similar methods for health care-based PA promotion are used elsewhere in the Nordic region as well as in other parts of the world.Unique for the Swedish version however,is that the counseling and written prescription are individualized and can be prescribed by any licensed health care professional with sufficient knowledge about PAP.The method PAP,which can be used for prevention or treatment of more than 30 conditions or diseases,is implemented in the Swedish health care system and is most widespread within primary care.6The number of patients issued PAP have increased during the last 10 years;however,little is known about the number of professional health care workers who use PAP in Sweden.Because the Swedish method of PAP can be used for a variety of diseases,is cost-effective,and lacks considerable side effects,6it is suitable for low-and middle-income countries in the prevention and treatment of NCDs.
Community settings for PA promotion include public health approaches that have a wide reach and can be implemented with minimal resources.Mass-media campaigns are considered cost-effective and have an impact on people’s awareness of health behaviors such as PA.9The effect of mass-media campaigns may be enhanced if conducted in combination with other strategies,such as policies or environmental changes.9Another approach is to develop national PA guidelines that can provide a basis for public health efforts to increase PA as well as provide a basis for future research.10In 2010,WHO releasedGlobal Recommendations on Physical Activity for Health.1Following that,many countries have developed their own national recommendations or guidelines,which may differ slightly due to cultural and contextual variances.In many low-and middle income countries,such as Vietnam,national recommendations or guidelines on PA are still lacking.Hence,developing guidelines for PA in Vietnam should be a priority activity.
Sweden and Vietnam share a long history of development cooperation within various fields,such as infrastructure,poverty reduction,and health care.11Since the 1980s,Vietnam has developed from one of the world’s poorest low-income countries to a lower middle-income country,with a rapidly growing economy.11During 2010-2013 a partner-driven cooperation project was conducted in Vietnam,with the overall aim to increase the awareness of the role of PA in prevention and treatment of disease.This was done by introducing and exploring 4 strategies:
1.Development of an education and training program on the method PAP for health care professionals,followed by an evaluation process;
2.Translation and dissemination of the evidence-based handbook(FYSS);
3.Implementation of a mass-media campaign to influence the awareness of PA in the Vietnamese society;
4.Initiation of the process of developing national guidelines on PA.
The partners involved in this project were(1)Karolinska Institutet,a large medical university in Stockholm,Sweden,(2)Professional Associations for Physical Activity in Sweden,a sub-association within the Swedish Society of Medicine,and(3)Hanoi Medical University(HMU),a leading Vietnamese university in collaboration with the Ministry of Health and the WHO office in Hanoi,Vietnam.The project was funded by the Swedish International Development Cooperation Agency(Sida in Swedish).Experiences and lessons learned from this partnerdriven cooperation project,where the PAP method was translated and disseminated from a high-income country to a lower middle-income country,a mass-media PA campaign was launched,and Vietnamese PA Guidelines were initiated are described in this case report.
2.Case report
This case report focuses on the above mentioned 4 strategies(1-4)used to implement and disseminate the PAP method and to develop national guidelines for PA in Vietnam.However,within the scope of this project only the first strategy could be accurately evaluated.
2.1.Development of an education and training program on the method PAP for health care professionals,followed by an evaluation process
The first strategy involved designing courses on the PAP method.Two different courses were designed:(1)a 5-day,in-depth course held in Sweden for key persons from the Vietnamese health care system,called the “Training of Trainers”(TOT)course and(2)a 2-day training course on PAP held in Vietnam,for several groups of health care professionals.
2.1.1.TOT course
The purpose of theTO T course was to educate trainers,who in turn,assisted as trainers of the PAP courses held in Vietnam.Their mission also was to continue to spread the method PAP after the project had ended.The curriculum for the TOT course included understanding the relationship between PA and health benefits and the underlying physiological mechanisms for these relationships,general recommendations for PA,and implementation of PAP in the Vietnamese health care system.In total,13 key persons from the Vietnamese health care system participated in 1 of the 2 TOT courses held in Sweden in August and September 2011 and in February 2012.

Fig.1.Project timeline.FYSS is the Swedish abbreviation of the evidence-based handbook Physical Activity in the Prevention and Treatment of Disease that accompanies PAP.Int.=international;PA=physical activity;PAP=Physical Activity on Prescription;TOT=Training of Trainers.
2.1.2.PAP course
The purpose of the PAP course was to educate health care professionals to use the method PAP,i.e.,to recommend or prescribe PA to their patients,when relevant.This course had a more practical approach with workshops and case-studies and the learning objectives included assessment of lifestyle risk factors,evidence-based methods for promotion of PA,and public health benefits of PA.The training material was written in English by the Swedish lecturers and translated into Vietnamese before the courses.The courses were held in English and were simultaneously translated into Vietnamese by a Vietnamese interpreter.The project timeline is shown in Fig.1.
During two 1-week periods(November 2011 and April 2012),251 persons took part in 5 separate 2-day PAP training courses.The course participants were mainly staff(physicians,nurses,and other medical collaborators)from 3 major hospitals in Hanoi as well as 1 hospital and 1 medical clinic in Phu Tho,a rural province outside Hanoi.Also,19 journalists took part in the courses as well as some medical students.The Vietnamese project partner was responsible for the recruitment of the course participants.In addition,a short introductory PAP course(half day)was held for 24 health care professionals at the Hospital of Post and Telecom in Hanoi in November 2012,in conjunction with an international conference on PAP,which was also part of the project.
The PAP training courses were evaluated by using(1)a general course evaluation distributed and returned right after the courses and(2)an on-site follow-up evaluation,6-14 months after the courses.
1.The general course evaluation comprised 9 questions(6 closed-and 3 open-ended questions)with the closedended responses presented on a 5-category scale anchored from most positive to least positive descriptors.The open-ended questions were posed about the general perceptions of the training course,the PAP curriculum,and perceived strengths and limitations as well as suggestions for improvements.Appendix 1 contains the wording of the course evaluation.
2.An on-site follow-up was performed in Hanoi during September-November 2012,6-14 months after the courses.At this time,a 14-item self-report questionnaire(Appendix2),was administered to health care professionals to capture participants’demographic characteristics and perceptions of PAP.The questionnaire contained items about general characteristics of the course participants(Q1-8),attitudes to the PAP method(Q9),self-reported knowledge and confidence to use PAP(Q10-12),and self-reported usage of PAP after the short training(Q13-14).Responses were tallied into frequencies and for items 9-12,responses were compared between persons attending the TOT courses in Sweden and the PAP courses in Vietnam using χ2tests.Data were analyzed using IBM SPSS Statistics Version 21.0(IBM Corp.,Armonk,NY,USA).The level of significance was set top<0.05.
The 14-item questionnaire was complemented by a qualitative evaluation to obtain a deeper understanding of how the participants perceived their experiences.Eight semi-structured interviews with training course participants were conducted in English and interpreted into Vietnamese by an experienced interpreter.An interview guide was used(Appendix 3),and the interviews were recorded,transcribed verbatim into text documents in English and analyzed using manifest content analyses.Informed consent was provided by the participants prior to the study.Results from the qualitative evaluation are outside the scope of this study.
2.2.Translation and dissemination of the evidence-based FYSS handbook
The second strategy included translation and dissemination of the handbook used for the PAP program.Based on criteria relevant for the Vietnamese context,such as particularly common NCDs in Vietnam,a selection of chapters from the FYSS handbook were translated from English into Vietnamese.The translation process involved many authors and was divided into the following steps.
1.Selection of chapters(35 out of 47 chapters);
2.Translation from English to Vietnamese by a group of 9 medical doctors;
3.Editorial work by 12 medical specialists;
4.Linguistic review(by an independent linguistic group);
5.Review by medical specialists;
6.Second review of all chapters by editors.
During the translation process,Swedish and Vietnamese experts frequently discussed difficulties that occurred(i.e.,words that were difficult to translate).A brief quality control of samples of the book was carried out by a group of experts prior to printing.A more extensive quality control was performed after the book was printed by a group of doctors and medical students at HMU(www.ipapo.org/en/lets-study-together.html).
2.3.Mass-media campaign
The third strategy involved disseminating PA materials to target groups.As communication played an important role in achieving the project objectives,a professional media bureau from Hanoi was involved in the project from the start.The communication strategy focused on 4 target groups:health care professionals,journalists,policy makers,and the public.In addition to general information on national television,specific tools were used to reach each of the 4 target groups such as websites,social media,and publications in the health and medicine area and national key publications of lifestyle.Nineteen journalists from different media outlets,organizations,and companies participated in the training course on PAP in Hanoi in April 2012 to improve knowledge and ability to report on the subject.
During the period May-October 2012,a campaign for raising PA awareness was prepared.The campaign activities included the establishment of an official website linked to social media,TV talk shows broadcast on national television,promotional material(such as posters displayed at different places in Hanoi,such as hospitals,clinics,and at HMU),media exposure,and advertisements.After the formal end of the project,the website www.ipapo.org became a type of e-archive for the project as well as an interactive e-resource for the development of PAP.In addition to the Vietnamese website,there is a Swedish website hosted by the Swedish Professional Associations for Physical Activity on the theme of PA for global health(www.pa4gh.org).The Swedish website provides information about the project in English and links to the Vietnamese website.The mass-media campaign was “kicked-off” in November 2012,just before an international conference on PAP in Hanoi,and ran until February 2013.The international conference on PAP,whose main goal was to raise the awareness of PA and PAP on the political agenda and in health care,gathered about 140 people,mainly medical specialists from various fields,policy makers,journalists,and medical students.The conference was organized by the Vietnamese partner,HMU.
2.4.National guidelines on PA
The fourth strategy involved setting the framework for the development of national guidelines for PA in Vietnam.The process of developing national guidelines and policy documents on PA was initiated through several awareness and advocacy activities during the 3-year project.The process started with a 1-week “study visit”to Sweden in March-April 2011,by a delegation of 4 people;from the WHO-office,HMU,HMU hospital,and a journalist.The schedule for the visit included meetings with Swedish experts in the field of PA and discussions on how to implement PA effectively and how to advocate policy changesetc.In addition,several physical meetings took place in Vietnam during the 3-year project,with various Vietnamese ministries,e.g.,the Ministry of Health,the Ministry of Education and Training,and the Ministry of Culture,Sports and Tourism as well as the WHO-office in Hanoi,with whom Swedish experts shared their experiences from the process of developing national recommendations on PA in Sweden.On November 7th 2012,a workshop on PA in the prevention and treatment of NCDs,targeting policy makers,was organized in Hanoi in conjunction with the international conference on PAP.The objectives were to share experiences on the international guidelines for enhancing PA and to discuss the development of national guidelines for enhancing PA in Vietnam.
3.Results
3.1.Study participants and demographic characteristics
In total 251 adults participated in the training courses and 123 completed the course evaluation.Of those not completing the evaluation,86 were omitted because they did not provide patient care(i.e.,students and journalists)and 6 were unable to attend the evaluation session(i.e.,they lived too far from Hanoi to participate in the evaluation).Of the remaining 159 participants in the project,36 dropped out from the study because they could not be reached during the period of the data collection(due to maternity leave,change of workplace or gone for business trip).Of the remaining 123 health care professionals completing the 6-to 14-month follow-up evaluation,most were between 21 and 50 years,female,PAP course participants,physicians,or nurses,and had worked in the health care field for over 15 years(Table 1).
3.1.1.Development of an education and training program for health care professionals on PAP,followed by an evaluation process
General perceptions of the PAP training course were evaluated with 42 of 58(72%)participants completing the evaluations after the course(Table 2).Based on the quantitative questions,most had a positive general impression of the course,rating it as either good or excellent,and agreed that it met their expectations,was useful,and was appropriate.The lectures were rated as either good or excellent.
Responses from the open-ended questions revealed the course provided a positive learning environment,with teachers’attitudes and a supportive classroom atmosphere as strengths of the course.A weakness mentioned by many participants was the limited time allocated for the course.Also,some participants had complaints about the written material, finding it unclear at times.With regard to improvements to the course,more thanhalf proposed increasing the length of the course(from 2 to 4 or 5 days)as well as increasing the time for practical instructions and discussions(qualitative data not shown).
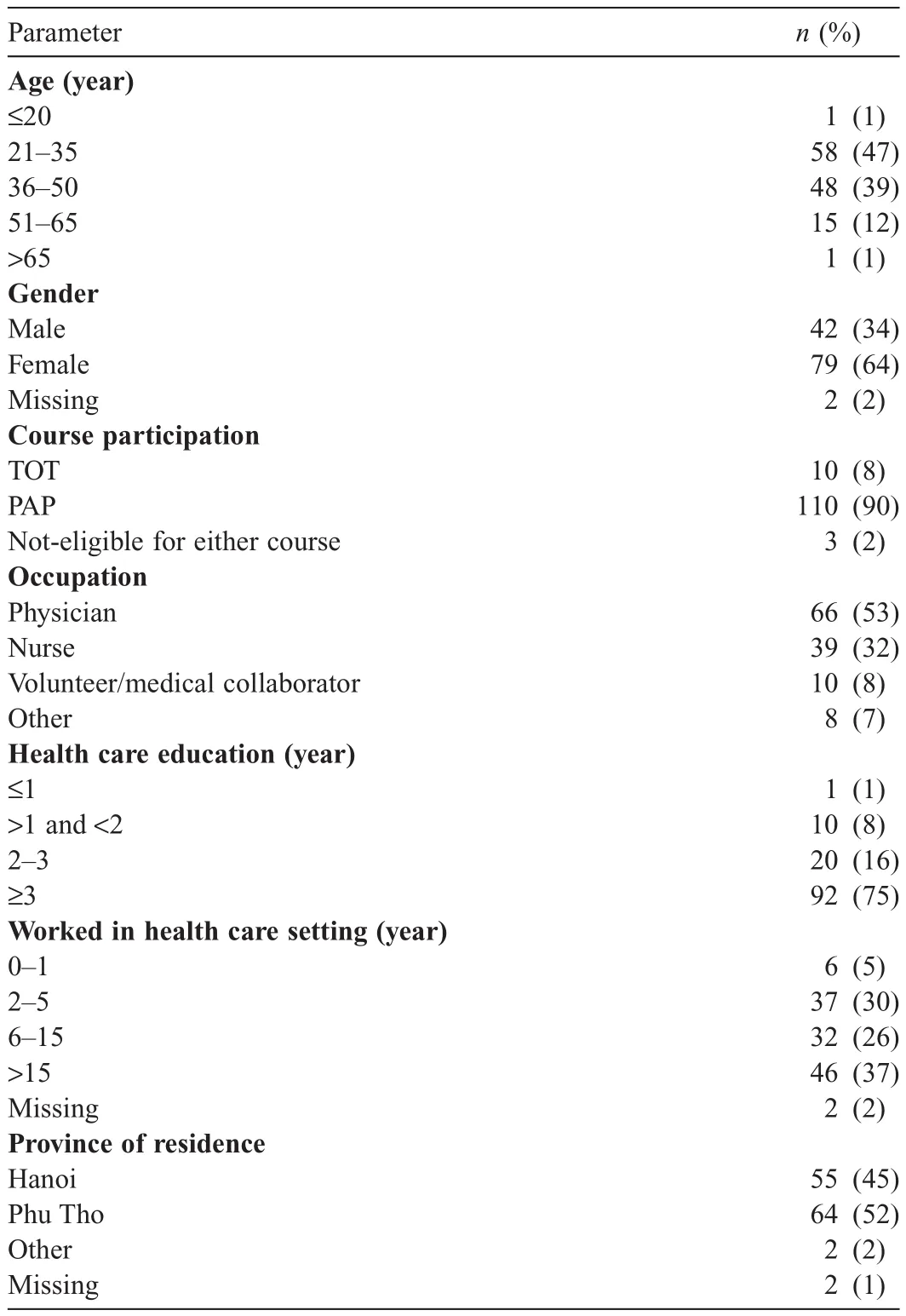
Table 1Demographic characteristics of course participants completing the 6-14 months follow-up PAP course evaluation(n=123).
Items 9-14 from the follow-up questionnaire completed 6-14 months after the short training course focused on the perceived importance of PA in the health care setting and the respondents’perceptions of the PAP method.Respondents ranked PA as somewhat-to-very important within the health care system;yet more than half(56%)reported uncertainty(neither poor nor good)when it came to knowledge about how to use PAP and 10%reported poor or very poor knowledge.Around half(54%)felt confident to recommend or prescribe PA.No differences in responses were observed between participants who attended the TOT courses in Sweden(n=10)and PAP courses in Vietnam(n=110)(p>0.05)(Table 3).
As presented in Table 4,about a third of the course participants(29%)reported an increase in prescriptions for PA after the short training course;however,there were also some participants(13%)who reported prescribing PA less often after the course.
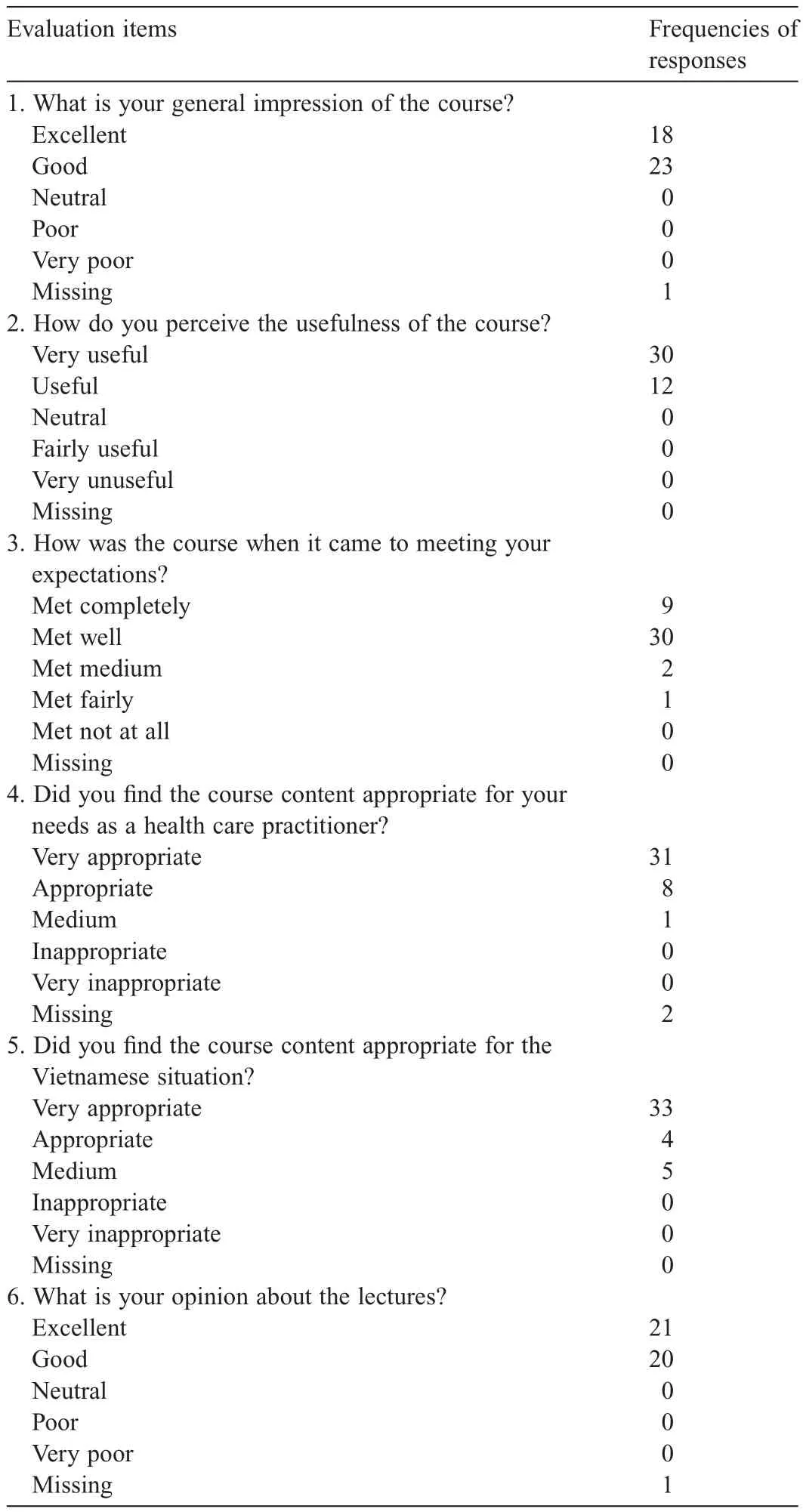
Table 2Frequencies of responses from the Physical Activity on Prescription course evaluation administered after the course(n=42).
3.1.2.Translation and dissemination of the evidence-based FYSS handbook
Five hundred copies of the FYSS handbook were printed,and the book was launched at the international conference on PAP in Hanoi in November 2012.All participants at the conference(140 people)received a free copy of the book.A pdfversion of the FYSS book can be downloaded for free from the project website in Vietnam(http://ipapo.org/fyss-books).The book has been provided at training courses in Vietnam after the project ended.
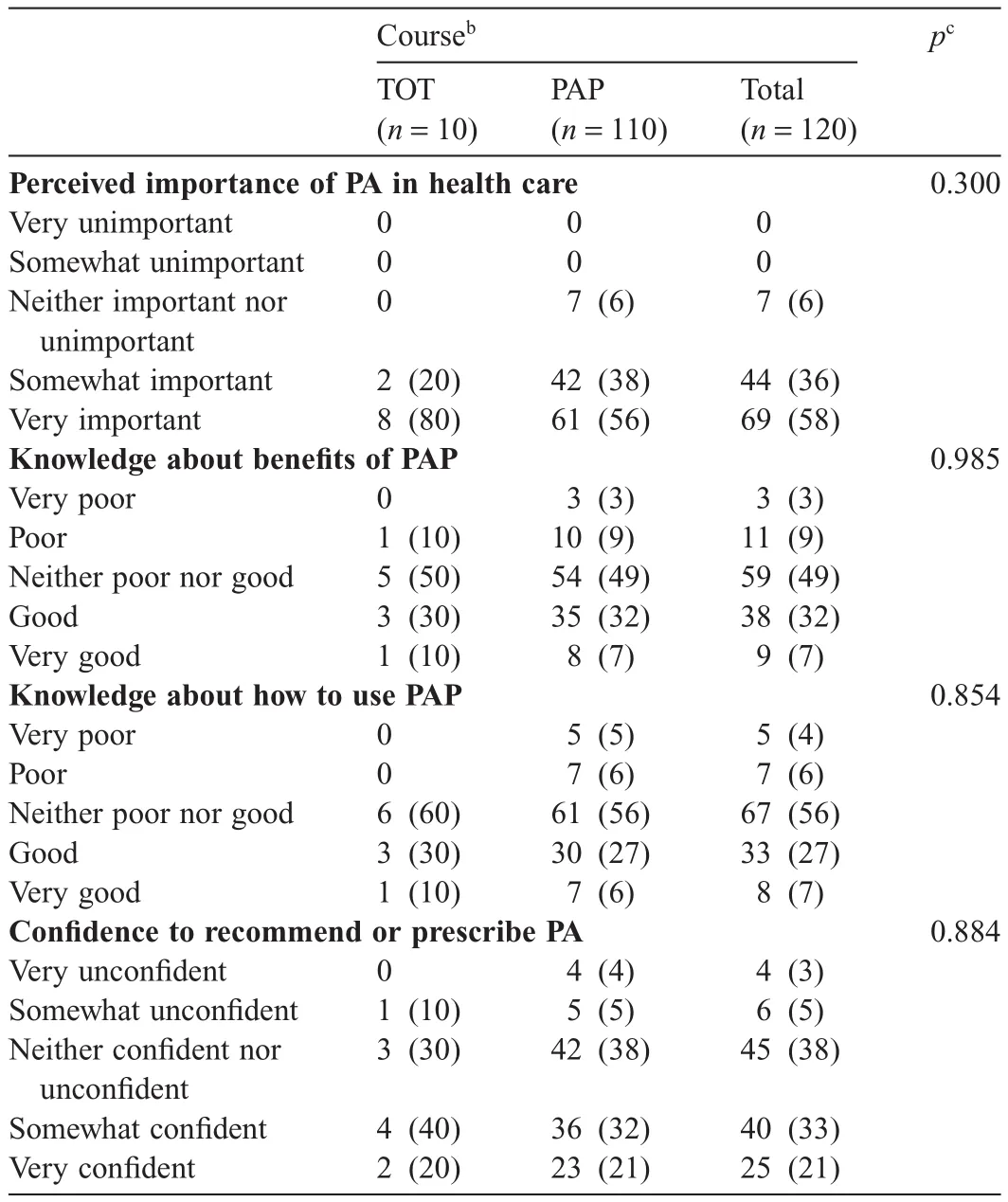
Table 3Responses to the 6-14 months follow-up evaluation of the PAP course and comparison of responses between the course participants in the PAP only and the TOT courses(n=123)a.
3.1.3.Mass-media campaign
Vietnamese mass-media covered the study visit to Sweden in March-April 2011,the training courses in November 2011 and in April 2012,as well as the international conference on PAP in November 2012 and the succeeding workshop.During the 3-year project,the communication team working in close collaboration with a media bureau resulted in 69 published articles,4 TV-news features,and 2 national TV-talk show broadcasts.12The 2 most popular TV-channels were contacted for the features,with suitable formats and evening time slots.Estimates from the Vietnamese branch of Taylor Nelson Sofre showed that 83%of the Vietnamese population was watching television daily during 2012.
3.1.4.National guidelines on PA
The workshop in conjunction with the international conference on PAP in November 2012,which brought together some 20 policy makers from several ministries and non-governmental organizations in Vietnam,received attention both on national television,via 2TV-news features,13,14and in Vietnamese newspapers via 6 articles.12In November 2013,1 year after the workshop,a follow-up discussion was held in Hanoi which revealed that national guidelines on PA for primary school children were developed by the Ministry of Health in collaboration with the Ministry of Education and Training in Vietnam and approved in late 2013.15These guidelines will be followed by guidelines on nutrition and PA for high risk populations.PA is a main part of the national strategy for NCDs control and prevention during 2015-2020,which has been approved by the Prime Minister in Vietnam.16The Vietnamese partners have stated that the project was instrumental for the Vietnamese ministries,in taking the first action for developing national guidelines.It is,however,difficult to definitely discern if and how the present project influenced this process.
4.Discussion
The overall purpose of this pilot project was to increase the awareness among health care professionals,and other target groups in Vietnam,about the beneficial effects of PA in the prevention and treatment of disease.PAP has been shown to not only increase the level of PA,but also to improve self-assessed quality of life among Swedish persons.6Because this project was not designed as an intervention study,it is not possible to draw any conclusions about the efficacy of the project.The results indicate that the project led to enhanced awareness and a positive attitude to PAP in the prevention and treatment of disease.Overall,the experiences and lessons learned from this partner-driven cooperation project are valuable for future projects.

Table 4Health care professionals self-reported number of PA recommendations given before and after the training course on PAP(n=103)a.
This project addressed a relatively new challenge for lowand middle-income countries,provided new ways of thinking about PA in the health care setting and instilled great enthusiasm in the Swedish and Vietnamese research and clinical groups.The comprehensive mass-media campaign conducted during the 3-year project,gained impact and awareness about PA both nationally and regionally.Furthermore,the development of these national guidelines for primary school children,accepted 1 year after the end of the project,is very promising as a method for increasing PA in Vietnam.The extent that this project affected the development is unknown.
Several new initiatives from the Vietnamese project partner have been launched,which include training courses on PA for health care professionals and patients;decisions about and advanced planning for the establishment of lifestyle clinics;and plans for further national guidelines on PA as well as new research projects in the field of PA.These examples further illustrate that several Vietnamese colleagues have been influenced by the project to a degree where they dare to start up entirely new organizations and activities.Initially,there was a concern that introducing a “ready-made”concept such as PAP from a high-income country would adversely affect the long tradition of various types of traditional PA in Vietnam.Historically,there has been a genuine knowledge about preventive medicine and the importance of PA in Vietnam,long before the Western world recognized this link.17,18Also in modern time,after the Cultural Revolution in 1945,preventive health education was prioritized in the Vietnamese society.17,18However,this concern was not justified,since the project was well received and new initiatives have been started.
Despite the accomplishments of the project,some limitations can be mentioned.First,follow-up questionnaires were initially sent by e-mail.However,many people were unfamiliar with receiving and responding to questionnaires via e-mail,therefore the initial plan had to be changed.The on-site follow-up was performed instead,where the questionnaires were distributed via the hospitals where the course participants worked.Unfortunately,the response rate was low.Second,following translation of the questionnaires into Vietnamese,the questionnaires were not back-translated to English due to time constraints and a lack of resources.When using questionnaires in cross-cultural research,it is recommended that both the questionnaires and the answers are back-translated to assure the quality of the results.19Third,even though the written material was translated and the lectures were simultaneously interpreted from English to Vietnamese,language barriers existed which were perceived as a limitation by some of the participants.Accordingly,efforts should be taken to minimize language barriers in projects abroad.Fourth,to make the course assessable to as many people as possible,2 days were allocated for the course.According to the course evaluations and the qualitative evaluation,many participants stated that they would have preferred a longer course.This,and the other limitations mentioned,might explain why more than half of the participants in the study reported their knowledge on how to use PAP as being “neither poor nor good”and “neither confident nor unconfident”to recommend or prescribe PA.
5.Conclusion
The intent of this project was to raise the awareness of the importance of PA in prevention and the treatment of disease and that the method PAP could be adapted in a way that was suitable for the Vietnamese context.There was shared responsibility for the program between Swedish and Vietnamese leaders,which showed a partner-driven cooperative project could be highly valuable,beneficial,and empowering to both partners.This project can provide others who are about to design and undertake similar initiatives in low-and middle-income countries with useful information and inspiration.
This project was funded by the Swedish International Development Cooperation Agency(Sida),Department for Development Partnership(No.AKT-2010-045).The authors would like to thank all the course participants for their committed participation, filling out the questionnaires,and participating in the interviews.The authors are sincerely thankful to all the people who in various ways contributed to the project,both in Vietnam and in Sweden,in particular all the teachers who conducted the training courses.A warm thanks to Danson Media,Hanoi,for highly appreciated cooperation during the project and to bachelor student Matilda Jansson,Linnæus University,Sweden,for helping with background research and references.The authors are grateful to Professors Eva Jansson and Mai-Lis Hellénius,Karolinska Institutet,for close cooperation and valuable contributions along the way and to Dr.Nguyen Thi Thanh Huong,Hanoi Medical University,for her initial cooperation.Finally,a special thanks to Helena Wallin,Karolinska Institutet,project assistant in the first phase of the collaboration.
Authors’contributions
CJS and TTHT designed the study;JK,AN,and SS carried out the data collection and performed the statistical analyses in collaboration with TTHT and THN;GBH coordinated the analysis of the project,supported the follow-up evaluations,and wrote the original manuscript in collaboration with CJS and IVDP;all authors critically reviewed and revised the draft.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Appendix:Supplementary material
Supplementary data to this article can be found online at doi:10.1016/j.jshs.2017.11.004.
1.World Health Organization.Global recommendations on physical activity for health.Geneva.Available at:http://whqlibdoc.who.int/publications/2010/9789241599979_eng.pdf;2010[accessed 24.07.2017].
2.World Health Organization.Global health risks.Mortality and burden of disease attributable to selected major risks.Geneva.Available at:http://whqlibdoc.who.int/publications/2009/9789241563871_eng.pdf;2009[accessed 24.07.2017].
3.Lee IM,Shiroma EJ,Lobelo F,Puska P,Blair SN,Katzmarzyk PT,et al.Effect of physical inactivity on major non-communicable diseases worldwide:an analysis of burden of disease and life expectancy.The Lancet2012;380:219-29.
4.Swedish Agency for Health Technology Assessment and Assessment of Social Services.Methods for physical activity:an systematic literature review.(Metoderföratt främjafysiskaktivitet.Ensystematisk litteraturöversikt). Stockholm. Available at: http://www.sbu.se/contentassets/c2cb6581355047b48367f19e1c9e3700/fysisk_aktivitet.pdf;2007[accessed 24.07.2017].[in Swedish].
5.Kallings LV,Leijon ME,Kowalski J,Hellénius ML,Ståhle A.Self-reported adherence:a method for evaluating prescribed physical activity in primary healthcare patients.J Phys Act Health2009;6:483-92.
6.Public Health Agency of Sweden.Personalized written ordination of physical activity.(FaR Individanpassad skriftlig ordination av fysisk aktivitet).Östersund.Available at:https://www.folkhalsomyndigheten.se/far/;2011[accessed 24.07.2017].[in Swedish].
7.Swedish National Institute of Public Health.FYSS 2008.Physical activity in the prevention and treatment of disease.Stockholm.Available at:http://www.fyss.se/fyss-in-english/chapters-in-fyss/;2008[accessed 24.07.2017].
8.Börjesson M,Sundberg CJ.FYSS(physical activity book for prevention and treatment):behavioural change also for the physician?Br J Sports Med2013;47:937-8.
9.Cavill N,Bauman A.Changing the way people think about healthenhancing physical activity:do mass media campaigns have a role?J Sports Sci2004;22:771-90.
10.Bouchard C,Blair SN,Haskell WL.Physical activity and health.Campaign,IL:Human Kinetics;2012.
11.The Swedish International Development Cooperation Agency(Sida).Evaluationstudyof long-termdevelopment co-operationbetweenVietnam and Sweden.Available at:http://www.sida.se/globalassets/global/about-sida/sida-utvarderingar/c721722_sida61468en_se_2012-2_vietnam_inlaga_c3.pdf/;2012[accessed 24.07.2017].
12.Danson Media.Making the move by aligning communication efforts in Vietnam.Available at:http://www.pa4gh.org/wp-content/uploads/2013/06/Vietnam-PAPTD-Final-report-on-communication-activities.pdf;2013[accessed 24.07.2017].
13.PAPTD.VTC News.YouTube.Available at:https://www.youtube.com/watch?v=ZuIq1aPkf9c;2012[accessed 24.07.2017].
14.PAPTD.O2TV.O2 Diary.2013.YouTube.Available at:https://www.youtube.com/watch?v=S0ZvdAR6Dok&feature=youtu.be;2013[accessed 24.07.2017].
15.National recommendations on physical activity for primary school children in Vietnam.Available at:http://vncdc.gov.vn/vi/phong-chongbenh-khong-lay-nhiem/444/huong-dan-thuc-hanh-dinh-duong-hop-ly-vatang-cuong-hoat-dong-the-luc-cho-hoc-sinh-tieu-hoc-trong-nha-truong;2013[accessed 16.12.2017].[in Viatnamese].
16.National Strategy for prevention of cancer,cardiovascular disease,diabetes,chronic obstructive pulmonary disease,asthma and other non-communicablediseases,theperiod2015-2025.Available at:http://vncdc.gov.vn/vi/he-thong-van-ban/1/5/32/376qdttg;2015[accessed 16.12.2017].[in Viatnamese].
17.Craig D.Familiar medicine.Everyday health knowledge and practice in today’s Vietnam.Honolulu:University of Hawaii Press;2002.Available at: http://muse.jhu.edu/books/9780824862473?auth=0; [accessed 24.07.2017].
18.Jansson M.Physical activity gives health benefits,but is this new to the Vietnamese?An analysis of articles from Vietnamese newspapers[BA thesis].Kalmar:Linnæus University,School of Social Sciences;2012.Available at:http://www.pa4gh.org/wp-content/uploads/2013/02/MATILDA-JANSSON-uppsats1.pdf;[accessed 24.07.2017].
19.Brislin RW.Back-translation for cross-cultural research.J Cross Cult Psychol1970;1:185-216.
 Journal of Sport and Health Science2018年1期
Journal of Sport and Health Science2018年1期
- Journal of Sport and Health Science的其它文章
- Research highlights from the Status report for step it up!The surgeon general’s call to action to promote walking and walkable communities
- Environments favorable to healthy lifestyles:A systematic review of initiatives in Canada
- The built environment correlates of objectively measured physical activity in Norwegian adults:A cross-sectional study
- The association of various social capital indicators and physical activity participation among Turkish adolescents
- Feasibility of using pedometers in a state-based surveillance system:2014 Arizona Behavioral Risk Factor Surveillance System
- Matched or nonmatched interventions based on the transtheoretical model to promote physical activity.A meta-analysis of randomized controlled trials