
The association of various social capital indicators and physical activity participation among Turkish adolescents
2018-04-26 07:39nayzerEmreBilginEzelNurKorurDarioNovakyasettinDemirhan
Günay Yılızer*,Emre Bilgin,Ezel Nur Korur,Dario Novak,Gıyasettin Demirhan
aDepartment of Physical Education and Sports Teaching,Anadolu University,Eskis¸ehir 26555,Turkey
bDepartment of Physical Education and Sports Teaching,Hacettepe University,Ankara 06800,Turkey
cDepartment of Physical Education and Sports Teaching,Ordu University,Ordu 52200,Turkey
dDepartment of General and Applied Kinesiology,University of Zagreb,Zagreb 10110,Croatia
1.Introduction
Physical activity participation(PAP)is one of the determining factors for optimal growth and development of children and adolescents.1,2There is also evidence to suggest that physical inactivity during early periods of life may track into adulthood and affect quality of life.3However,the majority of children and adolescents do not meet the current international guidelines for physical activity(PA),and 4 out of 5 adolescents do not participate in PA at the recommended level.4,5Physical inactivity is one of the major causes of various non-communicable diseases and premature deaths.6
Prevention and control of physical inactivity related noncommunicable diseases,such as cardiovascular disease,cancer,and diabetes,are a major challenge in developing countries.7Turkey is a developing country on the verge of a physical inactivity crisis.4The World Health Organization reported that 77.1%of male adolescents and 86.9%of female adolescents in Turkey are inactive.8As a consequence of an inactive lifestyle and in line with global World Health Organization reports,the Turkish Statistical Institution9reported that the majority of deaths in Turkey are caused by cardiovascular diseases and various types of cancers.Therefore,eliminating physical inactivity among Turkish adolescents is vitally important to decrease non-communicable diseases and their associated deaths.6
Social factors are highlighted as important determinants of individual health along with positive and risky health-related behaviors such as unhealthy diet,smoking,and physical inactivity.10Providing a positive social environment is emphasized as a possible mediator of PAP.11Recent attention has focused on social capital(SC)as a factor contributing to health outcomes such as PA behavior.12,13SC is defined as“social networks and the associated norms of reciprocity and trustworthiness”14and it is different from other social determinants of health as it is based on an individual’s direct choices and behaviors.15Measures such as cooperation,interpersonal trust and reciprocity,and exchange of social support within a group are determinants of SC.16Higher levels of SC perceptions have been linked to higher levels of PA among adults.17However little is known about SC and PAP in adolescents.How an SC mechanism may affect PAP in adolescents is explained as(1)informal social control decreases juvenile delinquency,therefore encouraging residents to exercise in outdoors,(2)collective efficacy improves access to PA opportunities,and(3)social norms related to healthy behaviors promote PA.18
Although PAP is important for the health and development of adolescents,19most of the studies exploring the relationship between SC and PAP have focused on adult populations.In addition,most studies examining the associations between SC and health outcomes have been conducted in high-income countries resulting in a lack of information related to populations from middle-and low-income countries and those from different cultures.Exploring these associations may help to reverse the physical inactivity trend among Turkish adolescents and to increase health quality among the Turkish population.The aim of this study was to examine the association between various SC indicators and PAP among high school-aged Turkish adolescents.
2.Materials and methods
A cross-sectional study design was implemented in 2016 among high school students from urban areas in 4Turkish cities(Ankara,Eskis¸ehir,I˙stanbul,and Ordu).I˙stanbul and Ankara are large size urban cities with a population of 15,000,000 and 5,000,000 people,respectively.Eskis¸ehir with a population of 850,000 people and Ordu with a population of 750,000 people are mid-size urban cities.Schools were randomly selected from a list of all public schools.All participants,school principals,and participants’parents were informed about the aim,procedure,and the data collection tools of the study.Participants and their parents signed informed consent forms.Only students who volunteered to participate in the study completed the data collection tool.The study was approved by Ethical Board Committee of the Hacettepe University and Turkish Ministry of Education.The data collection tool was administered to 19 high schools out of 1935 high schools in the referenced cities.Researchers selected 20 adolescents from each grade of each school for a total of 1520 adolescents invited to participate in this study.The participation rate was 81.25%.A total of 506 female(54.9±8.5 kg,163.8±6.5 cm,20.4±2.8 kg/m2)and 729 male(64.7±11.1 kg,174.0±7.7 cm,21.3±3.0 kg/m2)high school students from Grades 9-12(aged 14-18 years)participated in this study.
The outcome,PAP,was assessed by the short form of International Physical Activity Questionnaire(IPAQ)that provides total PA in the last 7 days as metabolic equivalent hours per week(MET-hours per week).20The short form of IPAQ was previously adapted into Turkish and validated.21The validation study reported moderate and significant relationship between the short form of the Turkish IPAQ and energy expenditure measured with an accelerometer.The IPAQ consists of 3 PA sections:vigorous,moderate,and walking PA.Based on PA recommendations calling for 60 min/day of PA in adolescents,22the PA score was dichotomized into “yes”or“no”for at least 60 min daily participation for overall PAP.Self-reported average PA min/day was multiplied by days/week and divided by 7 to determine the cut-point for dichotomized PAP as active or non-active.23
In addition to the IPAQ,participants answered survey questions about their perceptions of SC in the school,neighborhood,and family settings.24The survey consists of 6 questions about SC perceptions(Fig.1).School SC was composed of 3 indicators:interpersonal trust between teachers and students,interpersonal trust among students,and collaboration between students.Neighborhood SC was composed of 2 indicators:trust in the neighborhood and informal social control.Family SC was assessed by a single indicator.Participants answered questions using a 5-item Likert scale ranging fromstrongly agree(5)tostrongly disagree(1).Each SC indicator was transformed into dichotomous variables as high(strongly agree,agree)and low(neither agree nor disagree,disagree,andstrongly disagree).The survey was adapted into Turkish according to recommendations related to intercultural inventory adaptations.25All questions were analyzed as independent variables.
Study covariates were body mass index(BMI)and self-rated health.Self-rated health was assessed by a single question(How do you perceive your overall health?)with responses ranging fromvery poor,poor,regular,good,orexcellent.The responses were also dichotomized as poor(very poor,poor,andregular)and good(good,excellent)health status.BMI was included as a categorical variable in the statistics,calculated as self-reported weight in kilograms divided by self-reported height in meters squared.Overweight cut points ranged from 22.6 to 25.0 in males and from 23.3 to 25.0 in females.Obesity cut points ranged from 27.6 to 30.0 in males and 28.6 to 30.0 in females.Methods used to calculate gender and age-specific cut points are presented elsewhere.26
Before data analyses,multiple imputation analyses were conducted for missing data.27The variables with the highest missing data were PA variables(22.7%)and BMI(3.8%).The SC indicator with the most missing data was collaboration between students(1.7%).Descriptive statistics were calculated to explain features of the study population.Chi-square(χ2)tests were used to compare all categorical variables between genders.Finally,multiple binomial logistic regression was used to identify the associations of SC indicators and PAP adjusting for BMI and self-reported health.Models for PAP were first analyzed for the total sample then separately by gender.Ninetyfive percent confidence intervals were calculated for the odds ratios.The data were analyzed using SPSS Statistics Version 20.0(IBM Corp.,Armonk,NY,USA)and the significance level was set asp<0.05.
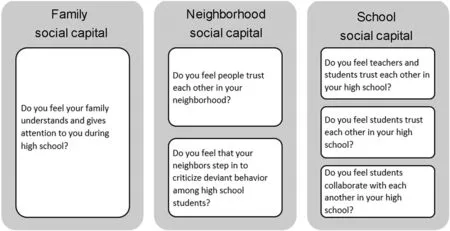
Fig.1.Social capital indicators.
3.Results
Descriptive percentages of the SC indicators,covariates,and PAP scores by gender are shown in Table 1.The majority of students reported high family support in school and low informal social control.Most had a normal BMI and were classified as active.Compared with females,χ2tests indicated that male high school students reported higher levels of students’interpersonal trust,good self-rated health,an overweight condition or obesity,and PAP.
The odds ratios of PAP for SC perceptions and covariates are shown in Table 2.Overall PAP was significantly associated with gender(p<0.05).Informal social control(p<0.05)andteacher-student interpersonal trust(p<0.001)were inversely associated with PAP among male high school students.Students interpersonal trust was positively associated with PAP among male high school students and inversely associated with PAP among female high school students(p<0.001).Good self-rated health was also positively associated with PAP among male high school students(p<0.001).
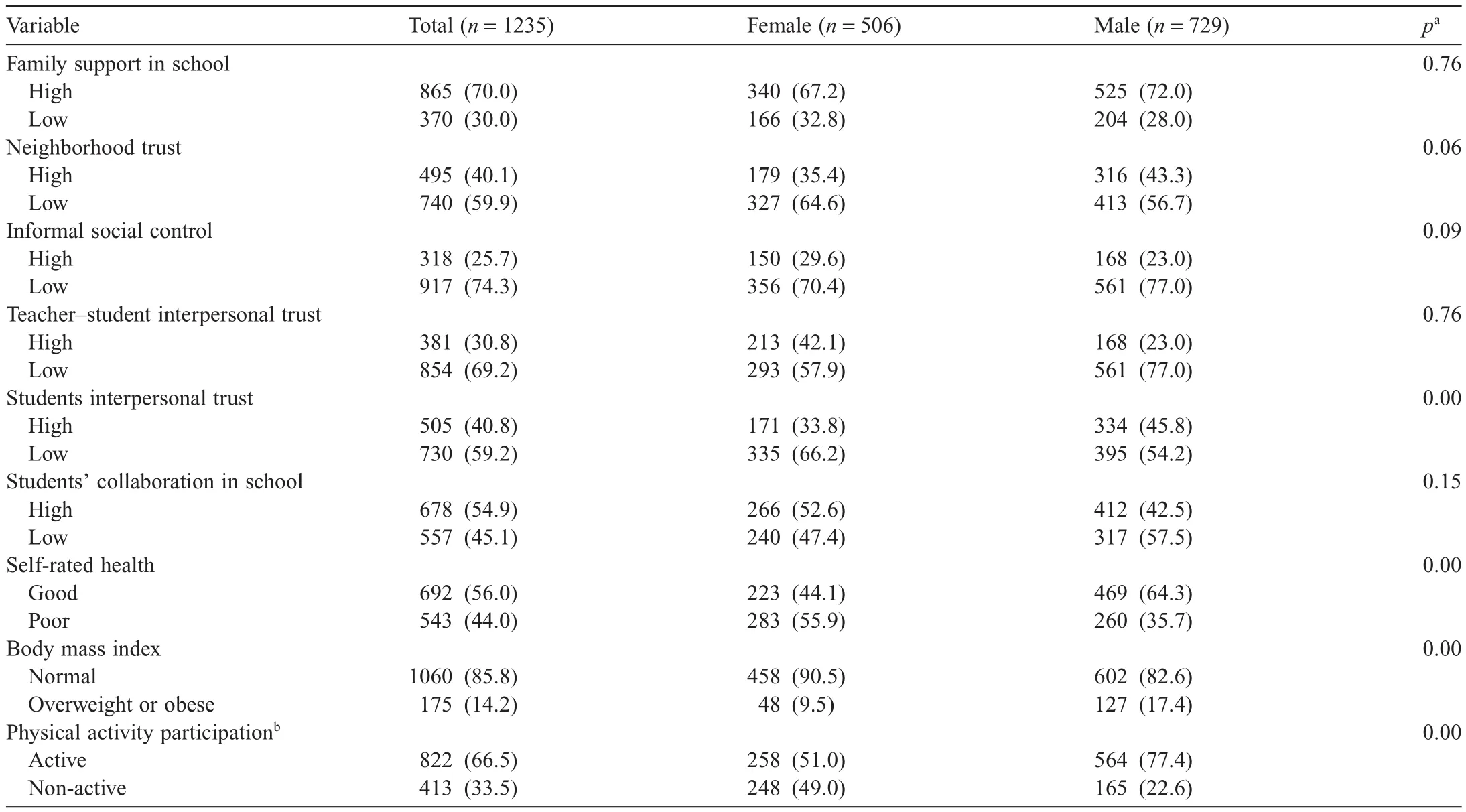
Table 1Comparison of perception of social capital indicators and covariates by gender in Turkish high school students,2016(n(%)).
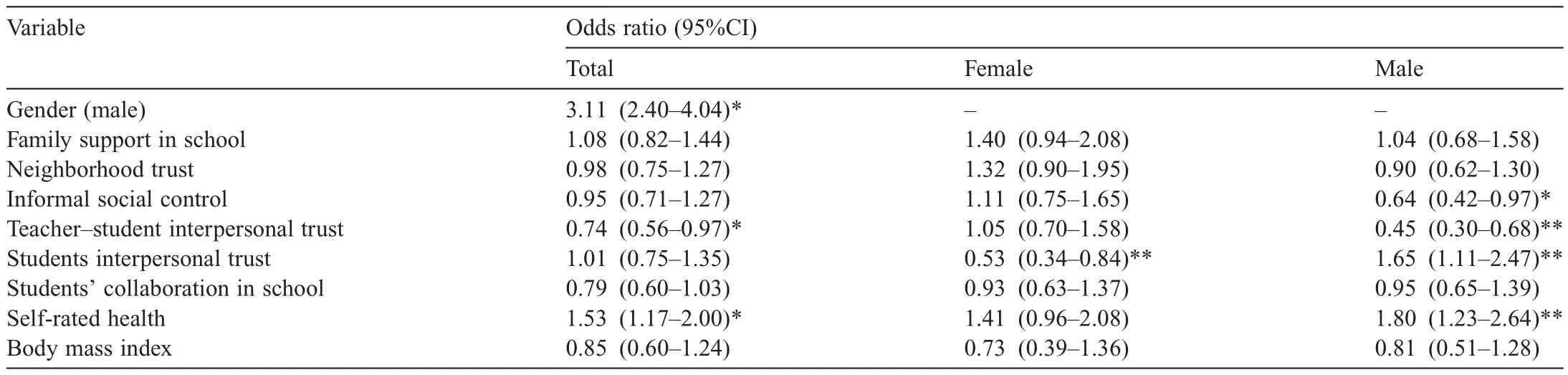
Table 2Odds ratios for overall physical activity participation by social capital indicators,self-rated health,and body mass index among Turkish high school students,2016.
4.Discussion
This study reports the association between various SC indicators and PAP among Turkish high school-aged adolescents.Males reported significantly higher students interpersonal trust in school than females.PAP was 3 times higher in males than in females.Only a few SC perceptions were associated with PAP among Turkish adolescents.Males with higher students interpersonal trust were 65%more likely to report higher PAP than males with low interpersonal trust.On the other hand,males with higher teacher-student interpersonal trust and higher informal social control and females with higher students interpersonal trust were less likely to report PAP than those with lower ratings.
Higher teacher-student interpersonal trust was associated with 55%lower odds for PAP among males while no association was observed in females.Similar to our findings,Novak et al.23demonstrated an inverse association between teacher student trust and PAP among Croatian male high school students.The low percentage of Croatian male students with high trust(32.6%)was similar to values observed in our study(23.0%).Hamid and Lok28demonstrated that male adolescents were less trusting of authority figures such as teachers and they also indicated that male adolescent relationships were less satisfying in terms of trust.Trust is a necessary component of a teacher-student relationship and it increases with teacher assertiveness and responsiveness to students.29Encouragement and perceived support from teachers are thought to be important mediators of PA.30Accordingly,perceived support from teachers has the potential to increase PAP among male adolescents,especially if teachers are assertive and responsive in promoting PA.
The positive link between SC,measured by teacher-student interpersonal trust,school belonging,and PAP was demonstrated in a study among Canadian adolescents.31The authors showed that the average weekly volume of moderate-to-vigorous PA performed by students with the highest school SC was about 40 min/week higher than for students with the lowest school SC score.As well,teacher-student relationships characterized by trust is an important factor for the social and emotional competence needed by students to achieve various outcomes in school.32In this context,teachers are role models for positive health behaviors in schools.33,34For example,physical education teachers with more favorable role modeling attitudes are themselves more active and have lower BMIs.35The inverse association between teacher-student interpersonal trust and PAP among males and the absence of an association among females suggests a need to better understand teachers’role modeling behaviors,motivational approaches,and aspirations as well as the school environment related to PA.It is also important to understand how male and female high school students perceive trust toward teachers and translate that trust into positive health-related behaviors.
Interpersonal trust among students was positively associated with PAP in males,yet inversely associated with PAP among females.This finding is consistent with Laird et al.36who reported peer social support was not a strong predictor of PAP among female adolescents.Instead,they suggested that being supported by various people in diverse ways was important for PAP.Stevens et al.37explicated that the sense of trust between youth may promote health by encouraging feelings of acceptance,support,and safety.They observed that attending a school with a high quality environment and where youths perceive school as a safe place was associated with fewer behavioral,emotional,and mental problems.Several studies worldwide also support the findings about interpersonal trust observed in our study.For example,studies conducted in Balkan countries reported no significant associations between students interpersonal trust with PAP23nor with self-rated health after adjustment for PAP among high school-aged adolescents.38,39A study among Swedish adults reported significantly higher odds ratios for low PA and with low trust,but only in the group who felt that they needed support to participate in PA.40Another Swedish study suggested low levels of PA may be partly due to a lack of generalized trust of other people in social networks.41In the current study,a high proportion of female adolescents rated interpersonal trust among students as low(66.2%).Reasons for this are unknown.Additional studies are needed to understand how interpersonal trust among students is related to PAP.
In this study,the odds for PAP were nearly 40%lower among male adolescents with higher informal social control in the neighborhood context than their peers with opposite ratings.Informal social control describes the role of adults stepping in to prevent the occurrence of crime,vandalism,litter in the streets,and deviant health behaviors such as drug abuse and smoking within a community.Studies conducted in the USA,Western Europe,and Eastern Europe have demonstrated that informal social control was associated with higher self perceived health and PA.23,39,42A Japanese study indicated that informal social control promoted neighborhood safety by preventing juvenile delinquency and was associated with outdoor PA.18Moreover,neighborhood informal social control can affect parents’perceptions of safety and allow them to encourage their youth to be physically active outdoors.43A Dutch study noted that correcting deviant behaviors in an early stage of childhood development may be related directly to adolescents refraining from acting up badly and indirectly by providing them with self-confidence.44
Our results were consistent with other studies that measured informal social control with the same question and that also reported no association between informal social control and higher levels of health-related behaviors.38,45Although informal social control promotes outdoor PA in the neighborhood context by providing a sense of safety,strict maintenance of social order also may be interpreted as a regulation of adolescent behavior.Novak and Kawachi45suggest that strict maintenance of social order may have a downside of having too strong SC.For example,restrictions on individual freedom and downward leveling of norms are identified as negative consequences of too strong SC.46A comparison of informal social control in neighborhoods in Turkish and Dutch cities showed informal social control was higher in Turkish cities than in Dutch cities.47Therefore,it would be expected that in Turkish adolescents,informal social control would be positively associated with PAP.However,this was not observed in the current study.Therefore,PA related social norms may be a possible cofounder of SC and the downside of having too strong SC in Turkey.This possibility should be researched in future studies within a Turkish context.
Results of present study revealed no association between perceived family support and PAP,despite the fact that role modeling,providing psychological support,and logistical support are considered to be important examples of social support provided by parents and are associated with PAP among adolescents.48Although family involvement in PA is important for creating a supportive environment,parental participation in PA is not the most important factor in promoting PA among youth.49In the Turkish context,Kelecioğlu and Bilge50reported that families may actually interfere their adolescent’s life and expose their expectations on adolescents in the context of supporting their needs.For example,families often send their children to extra classes and hire private tutors to advance their school performance.This may lead to an excessive school workload and depression.While this possibility may explain the absence of a relationship between family SC and PAP among Turkish adolescents,more studies are needed to fully understand this association.
Self-rated health was associated with PAP for males and females in the current study.Studies have shown that perceived health is positively associated with PA regardless of physical health status.51,52Active Canadian adolescents reported higher self-rated physical and mental health as compared with less active peers.53Swedish adolescents reported that participation in PA was important to maintain optimal body weight and self-rated health.54PA also was positively associated with very good self-rated health in high school-aged Finnish adolescents.55Moreover,in Spanish adolescents,increasing frequency of PA was associated with better self-rated health.56These findings are plausible as PA engenders reduced depression levels,improved hormonal response to stress,and increased positive physical self-concept,which may be a possible explanations for the association between perceived health and PAP.57,58
While the results present significant associations between SC and PAP,this study has some methodological limitations.Reverse causation cannot be ruled out due to the cross-sectional design used in the study.Although the assessment of PAP with the IPAQ has the advantage of collecting data easily,selfadministered instruments produce data with a validity and reliability that varies in different populations.59Finally,the school site was not included in this study as a cofounder,but it might influence the SC perceptions among students,and future studies should consider this variable.
5.Conclusion
Our study presents findings between perceptions of SC indicators and PAP among adolescent male and female high school students in a developing country.The perceived SC indicator of students interpersonal trust was positively related with PAP in males but inversely related to PAP in females.Teacher-student interpersonal trust and informal social control were inversely associated with PAP among male adolescents.Other SC indicators were not related to PAP.Additional studies are recommended to understand the influences of perceptions of SC and PAP participation in Turkish adolescents.
The authors would like to thank all high school students who participated in this study and their families.The authors also would like to thank school principals and physical education teachers for their tremendous collaboration in collecting data.This study was conducted as pilot research for the Ph.D.thesis of Günay Yıldızer.This research did not receive any specific grant from funding agencies in the public,commercial,or notfor-profit sectors.
Authors’contributions
GY,EB,and ENK were responsible for collecting data;GY and DN conducted statistical analyses;GD was responsible for all legal permissions;all authors drafted the paper.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
1.Strong WB,Malina RM,Blimkie CJR,Daniels SR,Dishman RK,Gutin B,et al.Evidence based physical activity for school-age youth.J Pediatr2005;146:732-7.
2.Eime RM,Young JA,Harvey JT,Charity MJ,Payne WR.A systematic review of the psychological and social benefits of participation in sport for children and adolescents:informing development of a conceptual model of health through sport.Int J Behav Nutr Phys Act2013;10:98.doi:10.1186/1479-5868-10-98
3.Telama R.Tracking of physical activity from childhood to adulthood:a review.Obes Facts2009;2:187-95.
4.Hallal PC,Andersen BL,Bull FC,Guthold R,Haskell W,Ekelund U,et al.Global physical activity levels:surveillance progress,pitfalls,and prospects.The Lancet2012;380:247-57.
5.Kann L,McManus T,Harris WA,Shanklin SL,Flint KH,Hawkins J,et al.Youth risk behavior surveillance—United States,2015.CDC MMWR Surveill Summ2014;65:1-178.
6.Lee IM,Shiroma EJ,Lobelo F,Puska P,Blair SN,Katzmarzyk PT,et al.Effect of physical inactivity on major non-communicable diseases worldwide:an analysis of burden of disease and life expectancy.The Lancet2012;380:219-29.
7.Bauman A,Schoeppe S,Lewicka M,Armstrong T,Candeias V,Richards J.Review of best practice in interventions to promote physical activity in developing countries.Geneva:WHO Press.Available at:http://www.who.int/dietphysicalactivity/bestpracticePA2008.pdf; 2005 [accessed 22.04.2017].
8.World Health Organization.Global status report on noncommunicable diseases 2014.Geneva.Available at:http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf?ua=1; 2014 [accessed 22.04.2017].
9.Turkish Statistical Institution.Cause of death statistics(Ölüm Nedeni I˙statistikleri).Available at:http://www.tuik.gov.tr/PreHaberBultenleri.do?id=24572;2016[accessed 24.05.2017].[in Turkish].
10.Currie C,Zanotti C,Morgan A,Currie D,de Looze M,Roberts C,et al.Social determinants of health and well-being among young people.Health Behaviour in School-aged Children(HBSC)study:international report from the 2009/2010 survey.Copenhagen:WHO Regional Office for Europe;2012.
11.Voorhees CC,Murray D,Welk G,Birnbaum A,Ribisl KM,Johnson CC,et al.The role of peer social network factors and physical activity in adolescent girls.Am J Health Behav2005;29:183-90.
12.Lomas J.Social capital and health:implications for public health and epidemiology.Soc Sci Med1998;47:1181-8.
13.Fisher KJ,Li F,Michael Y,Cleveland M.Neighborhood-level influences on physical activity among older adults:a multilevel analysis.JAging Phys Act2004;12:45-63.
14.Putnam RD.E pluribus unum:diversity and community in the twenty- first century The 2006 Johan Skytte Prize Lecture.Scan Polit Stud2007;30:137-74.
15.Kawachi I,Kennedy BP,Lochner K,Prothrow-Stith D.Social capital,income inequality,and mortality.Am J Public Health1997;87:1491-8.
16.van der Gaag MPJ,Webber M.Measurement of individual social capital.In:Kawachi I,Subramanian SV,Kim D,editors.Social capital and health.New York,NY:Springer;2008.p.29-49.
17.Lindström M,Hanson BS,Östergren PO.Socioeconomic differences in leisure-time physical activity:the role of social participation and social capital in shaping health related behaviour.Soc Sci Med2001;52:441-51.
18.Ueshima K,Fujiwara T,Takao S,Suzuki E,Iwase T,Doi H,et al.Does social capital promote physical activity?A population-based study in Japan.PLoS One2010;5:e12135.doi:10.1371/journal.pone.0012135
19.Ortega F,Ruiz J,Castillo M,Sjöström M.Physical fitness in childhood and adolescence:a powerful marker of health.Int J Obes2008;32:1-11.
20.Craig CL,Marshall AL,Sjöström M,Bauman AE,Booth ML,Ainsworth BE,et al.International Physical Activity Questionnaire:12-country reliability and validity.Med Sci Sports Exerc2003;35:1381-95.
21.Saglam M,Arikan H,Savci S,Inal-Ince D,Bosnak-Guclu M,Karabulut E,et al.International Physical Activity Questionnaire:reliability and validity of the Turkish version.Percept Mot Skills2010;11:278-84.
22.U.S.Department of Health and Human Services.Physical Activity GuidelinesforAmericans. Available at: www.health.gov/paguidelines;2008[accessed 24.05.2017].
23.Novak D,Doubova SV,Kawachi I.Social capital and physical activity among Croatian high school students.Public Health2016;135:48-55.
24.Furuta M,Ekuni D,Takao S,Suzuki E,Morita M,Kawachi I.Social capital and self-rated oral health among young people.Community Dent Oral Epidemiol2012;40:97-104.
25.Hambleton RK,Patsula L.Adapting tests for use in multiple languages and cultures.Soc Indic Res1998;45:153-71.
26.Cole TJ,Bellizzi MC,Flegal KM,Dietz WH.Establishing a standard definition for child overweight and obesity worldwide:international survey.BMJ2000;320:1-6.
27.Graham JW,Olchowski AE,Gilreath TD.How many imputations are really needed?Some practical clarifications of multiple imputation theory.Prev Sci2007;8:206-13.
28.Hamid PN,Lok DPP.Loneliness in Chinese adolescents:a comparison of social support and interpersonal trust in 13 to 19 year olds.Int J Adolesc Youth2000;8:45-63.
29.Wooten AG,McCroskey JC.Student trust of teacher as a function of socio-communicative style of teacher and socio-communicative orientation of student.Commun Res Rep1996;13:94-100.
30.Haerens L,Cerin E,Maes L,Cardon G,Deforche B,De Bourdeaudhuij I.Explaining the effect of a 1-year intervention promoting physical activity in middle schools:a mediation analysis.Public Health Nutr2008;11:501-12.
31.Button B,Trites S,Janssen I.Relations between the school physical environment and school social capital with student physical activity levels.BMC Public Health2013;13:1191.doi:10.1186/1471-2458-13-1191
32.Jennings PA,Greenberg MT.The prosocial classroom:teacher social and emotional competence in relation to student and classroom outcomes.Rev Educ Res2009;79:491-525.
33.World Health Organization.School policy framework:implementation of the WHO global strategy on diet,physical activity and health.Geneva:WHO Press;2008.
34.U.S.Centers for Disease Control and Prevention.Guidelines for school and community programs to promote lifelong physical activity among young people.Morb Mortal Wkly Rep1997;50:1-36.
35.Cardinal BJ.Role modeling attitudes and physical activity and fitness promoting behaviors of HPERD professionals and preprofessionals.Res Q Exerc Sport2001;72:84-90.
36.Laird Y,Fawkner S,Kelly P,McNamee L,Niven A.The role of social support on physical activity behaviour in adolescent girls:a systematic review and meta-analysis.Int J Behav Nutr Phys Act2016;13:79.doi:10.1186/s12966-016-0405-7
37.Stevens P,Lupton R,Mujtaba T,Feinstein L.The development and impact of young people’s social capital in secondary schools.London:Institute of Education,2007.(Centre for Research on the Wider Benefits of Learning Research Report).
38.Novak D,Ivana M,Snezana RJ,Štefan L,Tomislav K.The influence of social capital domains on self-rated health among Serbian high-school students?A school-based cross-sectional study.Monten J Sport Sci Med2016;5:33-8.
39.Novak D,Suzuki E,Kawachi I.Are family,neighbourhood and school social capital associated with higher self-rated health among Croatian high school students?A population-based study.BMJ Open2015;5:e007184.doi:10.1136/bmjopen-2014-007184
40.Lindström M.Social capital,desire to increase physical activity and leisure-time physical activity:a population-based study.Public Health2011;125:442-7.
41.Lindström M,Hanson BS,Stergren P-O.Socioeconomic differences in leisure-time physical activity:the role of social participation and social capital in shaping health related behaviour.Soc Sci Med2001;52:441-51.
42.Drukker M,Buka SL,Kaplan C,McKenzie K,van Os J.Social capital and young adolescents’perceived health in different sociocultural settings.Soc Sci Med2005;61:185-98.
43.Cerin E,Suen YN,Barnett A,Huang WYJ,Mellecker RR.Validity of a scale of neighbourhood informal social control relevant to pre-schoolers’physical activity:a cross-sectional study.SSM—Popul Health2017;3:57-65.
44.Drukker M,Kaplan C,Feron F,van Os J.Children’s health-related quality of life,neighbourhood socio-economic deprivation and social capital.A contextual analysis.Soc Sci Med2003;57:825-41.
45.Novak D,Kawachi I.Influence of different domains of social capital on psychological distress among Croatian high school students.Int J Ment Health Syst2015;9:18.doi:10.1186/s13033-015-0010-1
46.Kawachi I,Subramanian SV,Kim D.Social capital and health.NewYork,NY:Springer Science;2010.p.215-28.
47.Binbay T,Drukker M,Alptekin K,Elbi H,AksuTanık F,Özkınay F,et al.Evidence that the wider social environment moderates the association between familial liability and psychosis spectrum outcome.Psychol Med2012;42:2499-510.
48.Sterdt E,Liersch S,Walter U.Correlates of physical activity of children and adolescents:a systematic review of reviews.Health Educ J2014;73:72-89.
49.Salmon J,Booth ML,Phongsavan P,Murphy N,Timperio A.Promoting physical activity participation among children and adolescents.Epidemiol Rev2007;29:144-59.
50.Kelecioğlu H,Bilge F.Adaptation of academic expectations stress inventory:validity and reliability study.Hacettepe Univ J Educ2009;148-57.
51.McHugh JE,Lawlor BA.Perceived health status is associated with hours of exercise per week in older adults independent of physical health.J PhysAct Heal2013;10:1102-8.
52.Abu-Omar K,Rütten A,Robine JM.Self-rated health and physical activity in the European Union.Soz Praventivmed2004;49:235-42.
53.Herman KM,Hopman WM,Sabiston CM.Physical activity,screen time and self-rated health and mental health in Canadian adolescents.Prev Med2015;73:112-6.
54.Elinder LS,Sundblom E,Rosendahl KI.Low physical activity is a predictor of thinness and low self-rated health:gender differences in a Swedish cohort.J Adolesc Health2011;48:481-6.
55.Kantomaa MT,Tammelin T,Ebeling H,Stamatakis E,Taanila A.High levels of physical activity and cardiorespiratory fitness are associated with good self-rated health in adolescents.J Phys Act Health2015;12:266-72.
56.Galan I,Boix R,Medrano MJ,Ramos P,Rivera F,Pastor-Barriuso R,et al.Physical activity and self-reported health status among adolescents:a cross-sectional population-based study.BMJ Open2013;3.doi:10.1136/bmjopen-2013-002644
57.Dishman RK,Hales DP,Pfeiffer KA,Felton GA,Saunders R,Ward DS,et al.Physical self-concept and self-esteem mediate cross-sectional relations of physical activity and sport participation with depression symptoms among adolescent girls.Health Psychol2006;25:396-407.
58.Rothon C,Edwards P,Bhui K,Viner RM,Taylor S,Stansfeld SA.Physical activity and depressive symptoms in adolescents:a prospective study.BMC Med2010;8:32.doi:10.1186/1741-7015-8-32
59.Biddle SJH,Gorely T,Pearson N,Bull FC.An assessment of self-reported physical activity instruments in young people for population surveillance:project ALPHA.Int J Behav Nutr Phys Act2011;8:1.doi:10.1186/1479-5868-8-1
 Journal of Sport and Health Science2018年1期
Journal of Sport and Health Science2018年1期
- Journal of Sport and Health Science的其它文章
- Research highlights from the Status report for step it up!The surgeon general’s call to action to promote walking and walkable communities
- Environments favorable to healthy lifestyles:A systematic review of initiatives in Canada
- The built environment correlates of objectively measured physical activity in Norwegian adults:A cross-sectional study
- Feasibility of using pedometers in a state-based surveillance system:2014 Arizona Behavioral Risk Factor Surveillance System
- Matched or nonmatched interventions based on the transtheoretical model to promote physical activity.A meta-analysis of randomized controlled trials
- Collegiate athletes’mental health services utilization:A systematic review of conceptualizations,operationalizations,facilitators,and barriers