
Predictive power of abnormal electroencephalogram for post-cerebral infarction depression
2018-03-14 07:38YanpingZhengFuxiWangDeqiangZhaoYanqingWangZiweiZhaoZhanwenWangJunLiuJunWangPingLuan
中国神经再生研究(英文版) 2018年2期
Yan-ping Zheng, Fu-xi Wang, De-qiang Zhao, Yan-qing Wang, Zi-wei Zhao Zhan-wen Wang Jun Liu, Jun Wang, Ping Luan
1 Health Science Center, Shenzhen University, Shenzhen, Guangdong Province, China
2 Department of Dermatology, Shenzhen Second People’s Hospital, Shenzhen, Guangdong Province, China
3 Department of Neurology, Nanfang Hospital of Southern Medical University, Guangzhou, Guangdong Province, China
4 Department of Neurology, Shenzhen Second People’s Hospital, Shenzhen, Guangdong Province, China
5 Department of Neurology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, Guangdong Province, China
6 Cognitive Impairment Ward, Department of Neurology, Third Affiliated Hospital of Shenzhen University, Shenzhen, Guangdong Province, China
Introduction
Post-cerebral infarction depression (PCID) is the main form of post-stroke depression (PSD) and encompasses the majority of stroke. PCID is a common neuropsychiatric complication that affects the life quality of patients, and with symptoms involving consciousness and language, and mental retardation. The earliest study of PSD was in 1924 (Burvill et al., 1997). Burvill et al. (1997) performed experiments that found stroke patients were prone to behavioral and psychological disorders after brain injury. PSD was further confirmed as a persistent state in 1951, although the results were not widely noticed by medical academics. Folstein et al. (1977) performed clinical studies showing that PSD is a common complication of stroke patients, with an incidence rate of up to 45%. This attracted the attention of the medical profession, and PSD research became a ‘hot’ topic.
As a common psychiatric complication after ischemic stroke,PCID is a neurological disorder associated with depression.It refers to patients in a depressed state and includes a variety of neurological diseases or diseases. PCID symptoms include low mood and loss of interest, physical symptoms (such as sleep disorders, appetite disorders, and non-specific somatic symptoms), and psychological symptoms (such as anxiety,depression, mood, self-guilt, and self-reproach). Patients with a severe form of the illness even have tendencies of delusion and suicide. Therefore, detailed disease information cannot be obtained by clinicians, which is coupled to a lack of specific laboratory examinations and treatments for patients, as well as high rates of misdiagnosis and missed diagnosis within PCID patients (Shen, 2015). The prevalence of depression is up to 80% among cerebral infarction patients under conservative treatments (Li and Ma, 2015). Invasive treatment strategies may show some improvement for this unfavorable prognosis.
Related factors and mechanisms for PSD onset are not yet fully clear. It is generally believed that PSD is caused by interaction between biological, social, and psychological factors. PSD is an organic change in brain tissue involving the limbic-cerebral hemisphere system (specifically, prefrontal cortex, striatum, globus pallidus, and thalamus), and thereby affects regulation of circulatory dysfunction related to emotional disorders (Finnigan et al., 2004), accompanied by changes in states of consciousness. Studies have shown that cerebral blood flow is blocked for 30 seconds with cerebral infarction. Further, nerve cell membrane potential activity is abnormal, and the resulting changes can be observed by electroencephalography (EEG). Hence, EEG activity is viable for understanding changes in PSD pathogenesis, auxiliary diagnoses, and monitoring evaluation of its therapeutic effect, which support the theoretical foundation.
Changes in regional brain pathology function influenced by ischemic stroke can be analyzedviawell-established,sensitive EEG. EEG is a low-cost, noninvasive imaging technique that can measure nerve electrophysiology in the brain with excellent temporal resolution. Moreover, EEG has been explored for prognosis in acute stroke for over 40 years (Kaste and Waltimo, 1976). There studies on whether further courses of depression can be predicted using EEG changes (Peltz et al., 2010; Assenza et al., 2013). Independent prediction of PCID is assessed by presence of abnormal EEG features, with the aim of early identification of depression and enabling interventional treatment strategies during a ‘window of opportunity’. Here, our study sought to identify predictive factors for PCID by analyzing abnormal EEG signals in patients.
Subjects and Methods
Subjects
In total, 321 cerebral infarction patients were selected from the Neurology Clinic of Shenzhen Second People’s Hospital in Guangdong Province of China from July 2015 to February 2016. Inclusion criteria were: patients in Guangdong Province of China who had brain imaging tests, either computerized tomography (CT) or magnetic resonance imaging (MRI), combined with diagnostic criteria for stroke that conform to the fourth National Cerebrovascular Disease Conference in 1995 (Chinese Society of Neuroscience and Chinese Neurosurgical Society, 1996), and who were consequently diagnosed with cerebral infarction. Patients had stroke onset within 7 days, with vital signs of stability and sanity, did not suffer from obvious speech disorders(including partial motor aphasia without sensory aphasia),and cooperated with examination. Exclusion criteria were:initial involvement of additional vascular territories; taking any sedatives; or a history of other mental illnesses, such as depression. Cerebral infarction patients were classified into two categories, irrespective of sex, for direct comparison:middle-aged < 60 years old and elderly > 60 years old (Additional file 1). Subjects were further divided into two subgroups: PCID group (score results ≥ 8 scores) and non-PCID group (score results < 8 scores) (Additional file 2), based on Hamilton Depression Rating Scale (HAMD) scale score (Assenza et al., 2013).Figure 1shows a flow chart of the study.All subjects provided informed consent.
Data on demographics (sex and age), time after stroke, and frequency of stroke were collected from hospital electronic medical records. EEG examination within 7 days after onset is a standard procedure for incidence of cerebral infarction,and was generally performed in the hospital.
According to the formula for estimating sample size,n=400 × (q/p), where p is the prevalence rate and q = 1 − p. In this study, p = 72.6%, with a resultingn= 156. The number of patients used for the study was 321, which is more than 156, and therefore meets the estimated sample size.
HAMD scale assessment
HAMD factors include anxiety, weight loss, cognitive disorders (e.g., guilt, suicide, and agitation), day and night changes, changes in job interest symptom retardation, sleep disturbances, and hopelessness. These factors accurately reflect a patient’s psychopathology, and the target group’s clinical symptoms. Classification of evaluation results: total score <8 points is normal; total score 8–20 points may have depression; total score 20–35 points represents depression; total score > 35 points represents severe depression. The highest HAMD scale score is 133 points. Low HAMD scale scores reflect mild depression (Tang and Zhang, 1984).
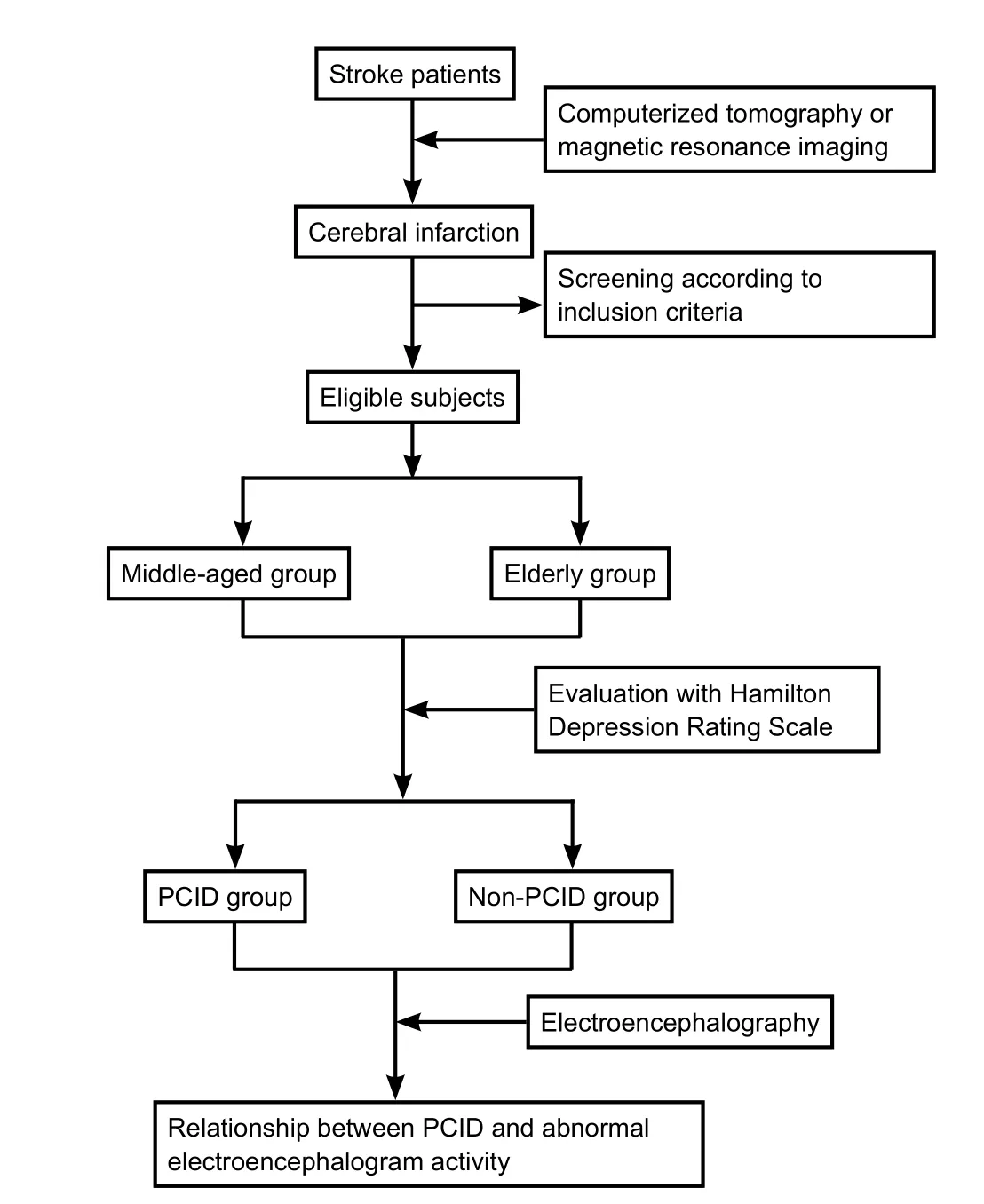
Figure 1 Flow chart of the study.
EEG recordings
The Natus Nicolet digital video EEG recording system was used with a 19-channel analogue recorder (Natus Neurology Incorporated, Middleton, WI, USA). Additionally, the International 10-20 system was used with Ag/AgCl electrodes.Impedance was maintained at < 5,000 Ω, amplifier sampling at a rate of 512 Hz, and frequency of filter settings ranged from 0.5–70 Hz. EEG recordings were at a speed of 30 mm/s, with sensitivity of 7–10 mV/mm. Notching filter at a frequency of 50 Hz was used when artifacts appeared. Bipolar montages were used (longitudinal: Fp1-F3, Fp2-F4, F3-C3, F4-C4, C3-P3, C4-P4, P3-O1, P4-O2, Fp1-F7, Fp2-F8, F7-T3, F8-T4,T4-T6, T5-O1, T6-O2, Fz-Cz, and Cz-Pz; transversal: Fp1-Fp2, F7-F3, F3-Fz, Fz-F4, F4-F8, A1-T3, T3-C3, C3-Cz, Cz-C4, C4-T4, T4-A2, T5-P3, P3-Pz, Pz-P4, P4-T6, and O1-O2),counterpart with reference montages (reference electrodes:Cz, A1, and A2). Ischemic stroke patients were examined within 7 days of incidence. EEG data were recorded under observation to ensure the patient’s eyes were closed. In addition, flash stimulation was performed following eye opening and closing. EEG was performed for 30–60 minutes. Test time depended on patient cooperation. The test time was extended if subjects suffered from forehead sweating, opened their eyes, or electromyography artifacts. Simultaneously,patients were regarded to lift those interferences. Alpha band activity weakens and disintegrates, and should be absent during sleeping. Reasonable EEG spectroscopy of 20–30 minutes was used in the sober and non-interference stages.EEG features were usually based on power ratios of alpha,beta, theta, and delta bands (Finnigan et al., 2004). Spectral analysis of EEG signals were performed by a certified EEG examiner (Li-jie Ren and Yan-qing Wang), who had understanding of stroke without knowledge of the clinical course.
EEG analysis
Raw EEG recording data from ischemic stroke patients were analyzed. The following parameters were considered: (1)involvement of occipital background frequencies to determine whether they are equal to, greater, or less than 8 Hz; (2)slowing activity influencing the entire hemisphere; (3) characteristic parameters within the spectrum (e.g., amplitude,activity, persistence, and reactivity of focal or lateralized slowing) (Ahmed, 1988); (4) slowing activity outside the ischemic lesion; and (5) regional attenuation without delta(RAWOD) (Schneider and Jordan, 2005).
Statistical analysis
Differences of continuous and categorical variables were separately evaluated by independent samplest-test and chi-square test. Odds ratios (OR) and 95% confidence intervals (95%CI)were estimated by binary logistic analysis for abnormal EEG features in the PCID and non-PCID groups. The groups and models were unadjusted and adjusted for age, gender, and EEG recordings (frequency of strokes). All data were analyzed using IBM SPSS19.0 software (IBM, Armonk, NY, USA). Statistical significance was set at two-tailedP< 0.05.
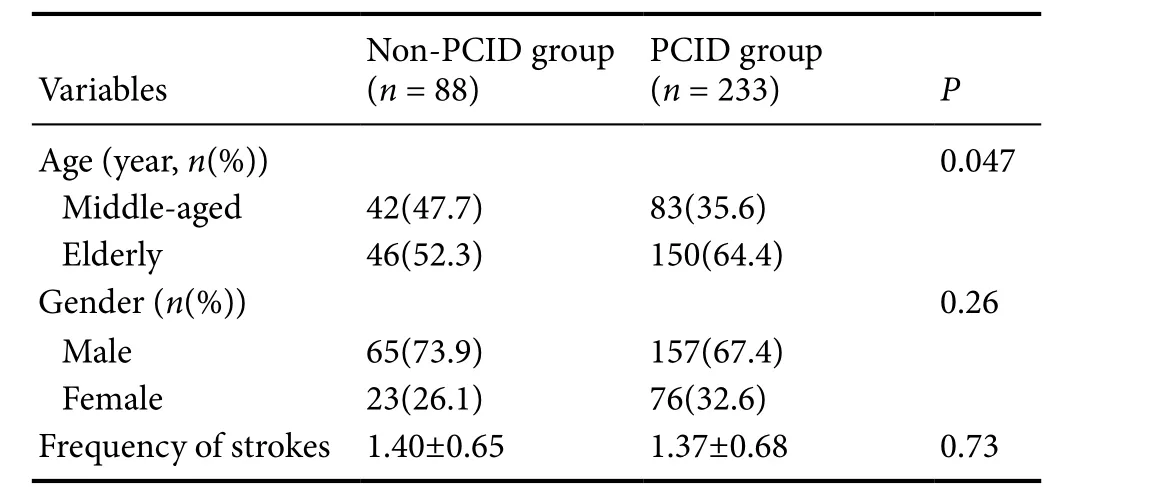
Table 1 Baseline characteristics and abnormal electroencephalogram
Results
Baseline characteristics and abnormal EEG analysis in patients with or without depression
Baseline characteristics of 321 patients are shown inTable 1. The number of subjects was greater in the depression group than that in non-depression group. Stroke frequency before EEG was lower in the depression group than that in the non-depression group. The variables, middle-aged and elderly, were significantly associated with depression after cerebral infarction. However, they were not significantly associated with depression for age variables when estimated by 95%CIin logistic regression models.

Table 2 Abnormal EEG characteristics
Analysis of abnormal EEG characteristics
Data for independent prediction of PCID, andOR(95%CI)by abnormal EEG features are shown inTable 2. Prevalence for low-amplitude alpha activity and slow theta activity were higher in the depression group than that in the non-depression group, whereas data for fast beta activity and delta activity were lower. Cerebral infarction patients suffered from depression predominant with low-amplitude alpha activity(adjustedOR1.85 [1.11–3.06]) and slow theta activity (adjustedOR1.76 [1.06–2.92]). Neither group was significantly associated with fast beta activity and slow delta activity.
Discussion
In our 321 cerebral infarction patients, EEG recordings can be considered independent predictors of clinical course.Similarly, EEG recordings provide useful information for identifying cerebral infarction patients who may develop depression. Our findings indicate that cerebral infarction patients predominantly experience depression with low-amplitude alpha activity and slow theta activity. In contrast, beta activity and slow delta activity were not significantly associated with development of depression in cerebral infarction patients. These results are in accordance with previous studies (Peltz et al., 2010; Assenza et al., 2013).
Detection of EEG is user-friendly, relatively simpler than imaging patterns, and can be quickly accessed. EEG is sensitive to disturbed neuronal functioning caused by energy depletion, such as cerebral infarction. EEG changes in cerebral infarction can be observed within minutes. Meanwhile,EEG can also measure developments of pyramidal neurons in response to decreased cerebral blood flow and hypoxia.There are relationships between reduced cerebral blood flow,degree of neuronal damage, and changes in EEG morphology (Faught, 1993; van Putten and Tavy, 2004). Serial EEG recordings have been investigated for their potential utility in predicting clinical course during recovery. Nerve cell function declines and relative amplitude of neural activity weakens in cerebral infarction patients with hypoperfusion,which results in low-amplitude alpha activity (Pollock and Schneider, 1990). Previous studies have found that slow theta activity is a predominant sign in PCID patients (Cillessen et al., 1994; Jordan, 2004). The 121 symptoms of major depressive disorder subjects indicate the appearance of theta activity and alpha activity in longer haulviaQEEG (Deslandes et al., 2004; Leuchter et al., 2012).
Our results indicate that patients are regarded as having depression when EEG morphologies of low-amplitude alpha activity and slow theta activity appear. In our study, the presence of beta activity and slow delta activity after infarction suggested the patients were at low risk of depression. Continuous slow theta activity appears to be the most sensitive parameter in progression of depression by means of focal signs. Predominant low-amplitude alpha activity is a risk for PCID. Absence of slow activity and slight depression of alpha activity are excellent EEG predictive factors. Unfavorable predictor outcomes were low-alpha volatility activity and delta activity (Peltz et al., 2010; Assenza et al., 2013). We found that low-amplitude alpha activity together with continuous slow theta activity is predictors of PCID. Contradictory findings may be due to differences in living habits, for example, having a light diet and taking a break after lunch.
EEG, with an additional field, comes into the picture that it can predict the progress of depression following onset of stroke. This may be a progressive process in ischemic tissue,along with a possible reversible window for neuronal injury(Khodayari-Rostamabad et al., 2011). Whether neuronal injury leading to depression is reversible is not distinguishable in the clinic (Jordan, 2004). Even depression scales do not necessarily reflect depression course. EEG findings are relevant to good long-term prognosis, for example, absence of low-amplitude alpha activity and slow theta activity are considered predictive factors of a reversible state (Begić et al., 2011). Thus, for this indication, EEG might be included in future guidelines. Potential applications for PCID include early detection and follow-up courses, although diagnostic values must be established.
Our study is novel in identifying abnormal EEG characteristics as an independent risk factor for PCID in Chinese people of the Guangdong Province. The HAMD scale is used for depression diagnosis under normal conditions. It is assessed by a family member through recording medical history and observing clinical symptoms of the patient. The HAMD scale is relatively objective compared with other scales. Furthermore,rigorous quality control and face to face interviews are used by hospital employees for the HAMD scale. Consequently,HAMD score data are statistically significant in the study.
Subjects in our findings were chosen from the Shenzhen Second People’s Hospital of China. The sample size and representativeness might be limited, and all of those might influence the statistical results for HAMD scores. EEG signals were analyzed by certified examiners (instead of Matlab software) to acquire sampling rates, and performed in signal analysis, which might over- and underestimate the relationship. In addition, there are not any uniform international standards in use of Matlab software for EEG diagnosis. Observational bias might exist when depression is assessed by HAMD scale and clinical features. Hence, attention should be paid to explaining and comparing findings. Based on these findings, future research is needed to select different cerebrovascular disease types, adopt scales combined with the Self-Rating Depression Scale and HAMD, and use Matlab software for spectral analysis of EEG signals.
In summary, conventional EEG has been applied for cerebral infarction patients. Sole use of scales to diagnose depression might be susceptible to subjective assessment. EEG generated information may forecast depression onset after cerebral infarction and contribute to identifying intrusive treatment strategies within the window of probability. Therefore, the influence of depression may be minimized as well as permanent neurological weaknesses decreased. Presence of low-amplitude alpha activity and slow theta activity are independent predictors of PCID. Intensive interventions should be targeted to reduce deaths due to depression in cerebral infarction patients.
Author contributions:YPZ and FXW performed statistical analysis and wrote the paper. ZWZ and ZWW were responsible for data collection.YQW, DQZ and JL analyzed EEG signals. PL and JW gave the guidance of study design. All authors approved the final version of the paper.
Conflicts of interest:None declared.
Financial support:This study was supported by the National Natural Science Foundation of China, No. 81372919; the Natural Science Foundation of Guangdong Province of China, No. 2014A030313016;the Basic Key Research Project Fund of Shenzhen City of China, No.JCYJ20150324140036853; the Science and Technology Program Fund of Shenzhen City of China, No. JCYJ20140418181958477. Funders had no involvement in the study design; data collection, management, analysis,and interpretation; paper writing; or decision to submit the paper for publication.
Research ethics:The study was performed in accordance with the Declaration of Helsinki and relevant ethical principles.
Data sharing statement:Datasets analyzed during the current study are available from the corresponding author on reasonable request.
Plagiarism check:Checked twice by iThenticate.
Peer review:Externally peer reviewed.
Open access statement:This is an open access article distributed underthe terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under identical terms.
Additional files:
Additional file 1:Single sample test for Hamilton Depression Scale(HAMD) score.
Additional file 2:Logistic regression models analysis for age group.
Ahmed I (1988) Predictive value of the electroencephalogram in acute hemispheric lesions. Clin Electroencephalogr 19:205-209.
Assenza G, Zappasodi F, Pasqualetti P, Vernieri F, Tecchio F (2013) A contralesional EEG power increase mediated by interhemispheric disconnection provides negative prognosis in acute stroke. Restor Neurol Neurosci 31:177-188.
Begić D, Popović-Knapić V, Grubišin J, Kosanović-Rajačić B, Filipčić I,Telarović I, Jakovljević M (2011) Quantitative electroencephalography in schizophrenia and depression. Psychiatr Danub 23:355-362.
Burvill P, Johnson G, Jamrozik K, Anderson C, Stewart-Wynne E (1997)Risk factors for post-stroke depression. Int J Geriatr Psychiatry 12:219-226.
Chinese Society of Neuroscience and Chinese Neurosurgical Society(1996) Diagnosis of various cerebrovascular diseases. Zhonghua Shenjingke Zazhi 29:379-380.
Cillessen JP, van Huffelen AC, Kappelle LJ, Algra A, van Gijn J (1994)Electroencephalography improves the prediction of functional outcome in the acute stage of cerebral ischemia. Stroke 25:1968-1972.
Deslandes A, Veiga H, Cagy M, Fiszman A, Piedade R, Ribeiro P (2004)Quantitative electroencephalography (qEEG) to discriminate primary degenerative dementia from major depressive disorder (depression). Arq Neuropsiquiatr 62:44-50.
Faught E (1993) Current role of electroencephalography in cerebral ischemia. Stroke 24:609-613.
Finnigan SP, Rose SE, Walsh M, Griffin M, Janke AL, McMahon KL,Gillies R, Strudwick MW, Pettigrew CM, Semple J, Brown J, Brown P, Chalk JB (2004) Correlation of quantitative EEG in acute ischemic stroke with 30-day NIHSS score: comparison with diffusion and perfusion MRI. Stroke 35:899-903.
Folstein MF, Maiberger R, McHugh PR (1977) Mood disorder as a specific complication of stroke. J Neurol Neurosurg Psychiatry 40:1018-1020.
Jordan KG (2004) Emergency EEG and continuous EEG monitoring in acute ischemic stroke. J Clin Neurophysiol 21:341-352.
Kaste M, Waltimo O (1976) Prognosis of patients with middle cerebral artery occlusion. Stroke 7:482-485.
Khodayari-Rostamabad A, Reilly JP, Hasey GM, deBruin H, MacCrimmon D (2011) Using pre-treatment electroencephalography data to predict response to transcranial magnetic stimulation therapy for major depression. Conf Proc IEEE Eng Med Biol Soc 2011:6418-6421.
Leuchter AF, Cook IA, Hunter AM, Cai C, Horvath S (2012) Resting-state quantitative electroencephalography reveals increased neurophysiologic connectivity in depression. PLoS One 7:e32508.
Li LJ, Ma X (2015) A Guide to the Prevention and Treatment of Depression in China (II). Beijing: Chinese Medical Multimedia Press Co., Ltd.
Peltz CB, Kim HL, Kawas CH (2010) Abnormal EEGs in cognitively and physically healthy oldest old: findings from the 90+study. J Clin Neurophysiol 27:292-295.
Pollock VE, Schneider LS (1990) Quantitative, waking EEG research on depression. Biol Psychiatry 27:757-780.
Schneider AL, Jordan KG (2005) Regional attenuation without delta(RAWOD): a distinctive EEG pattern that can aid in the diagnosis and management of severe acute ischemic stroke. Am J Electroneurodiagnostic Technol 45:102-117.
Shen LX (2015) The clinical significance of SEP and plasma serotonin in patients with post-stroke depression. Yanji: Yanbian University.
Tang YH, Zhang MY (1984) Hamilton Depression Scale (HAMD).Shanghai Jingshen Yixue:61-64.
van Putten MJ, Tavy DL (2004) Continuous quantitative EEG monitoring in hemispheric stroke patients using the brain symmetry index.Stroke 35:2489-2492.

- 中国神经再生研究(英文版)的其它文章
- Neuroprotective effects of statins against amyloid βinduced neurotoxicity
- Detection of thinned corticospinal tract and corticoreticular pathway in a patient with a calf circumference discrepancy
- Dyslipidemia modulates Müller glial sensing and transduction of ambient information
- Mitochondrial transplantation strategies as potential therapeutics for central nervous system trauma
- A new direction for Alzheimer’s research
- DNA plasticity and damage in amyotrophic lateral sclerosis