表皮生长因子受体少见突变型非小细胞肺癌临床病理特征及治疗分析
2017-12-11 09:03张峤刘翔李建军曹燕珍张健单莉
中国肿瘤临床 2017年21期
张峤 刘翔 李建军 曹燕珍 张健 单莉
表皮生长因子受体少见突变型非小细胞肺癌临床病理特征及治疗分析
张峤①刘翔②李建军①曹燕珍③张健④单莉①
目的:分析非小细胞肺癌患者表皮生长因子受体(epidermal growth factor receptor,EGFR)少见突变型的临床病理参数及EGFR-TKIs治疗的初步疗效。方法收集2012年1月至2016年4月新疆医科大学附属肿瘤医院经病理证实的29例非小细胞肺癌携带少见EGFR突变患者临床病理资料,分析少见突变型的临床病理特征及与EGFR-TKIs疗效之间的关系。结果在29例少见突变患者中,最常见的远处转移器官依次为同侧/对侧肺组织、骨、脑、肝、肾上腺,最常见的淋巴结转移依次为肺门淋巴结、锁骨上/下淋巴结、颈根部淋巴结及纵隔淋巴结。少见突变中单突变16例,L861Q 5例,G719X 5例,20ins 4例,S768I 2例。双突变型11例,S768I及20ins突变4例,L858R及S768I双突变1例,19Del及T790M双突变1例,L861Q及G719X双突变2例,19Del及S768I突变1例,20ins及G719X突变1例,T790M及G719X突变1例。三突变2例,L858R、L861Q及G719X突变1例,S768I、20ins及G719X突变1例。一线EGFR-TKIs治疗客观缓解率(objective response rate,ORR)43.75%,疾病控制率(disease control rate,DCR)50.00%,中位无疾病进展生存期(median progression-free survival,mPFS)5.50个月。二线EGFR-TKIs治疗ORR为28.57%,DCR为42.85%,mPFS为4.00个月。三线EGFR-TKIs治疗ORR为33.33%,DCR为50.00%,mPFS为2.67个月。结论EGFR少见突变对EGFRTKIs治疗的有效率及生存时间存在较大个体差异,EGFR少见突变患者的ORR及PFS均较经典突变患者低,部分高于野生型。对少见突变患者,EGFR-TKIs治疗一线疗效略优于二、三线,但无显著性差异。
非小细胞肺癌 表皮生长因子受体 靶向治疗 少见突变
表皮生长因子受体(epidermal growth factor re⁃ceptor,EGFR)是表皮生长因子受体(HER)家族成员之一,表达于正常上皮细胞表面,在部分肿瘤细胞中过表达,EGFR的过表达和肿瘤细胞的迁移、浸润及预后相关[1]。在高加索人群中肺腺癌EGFR敏感突变患者的发生率为10%~20%,肺鳞状细胞癌约为3%,而在亚裔肺腺癌人群中发生率约70%,肺鳞状细胞癌中约为10%[2-4]。之前的研究显示EGFR突变与人种,性别,腺癌,不吸烟等因素密切关系[5-7]。随着测序及PCR技术的应用,目前EGFR突变已成为EG⁃FR-TKIs靶向治疗是否有效的主要预测因子。EG⁃FR-TKIs治疗客观缓解率(objective response rate,ORR)达到70%~80%,中位PFS达到9~12个月,总生存期(overall survival,OS)达到20~32个月,成为EGFR突变型非小细胞肺癌一线治疗方案[7]。
EGFR突变主要存在于18、19、20、21外显子中,其中19外显子框内缺失突变和21外显子L858R点突变,20外显子T790M突变最常见,占EGFR总突变的50%~90%,称为经典突变[6,8-9]。其他的敏感突变均称为少见突变,临床上较常见的有18外显子的G719X,21外显子的L816Q、G719C等[9-10]。既往研究显示少见突变患者经EGFR-TKIs治疗后其PFS及ORR较常见突变患者低,但由于少见突变发生比例低,部分重叠出现,在不同人种及不同突变种类中EGFR-TKIs治疗疗效差异大,故目前无统一共识。
本研究收集了本中心近年来出现的29例携带EGFR少见突变的非小细胞肺癌患者,观测其病理特征与EGFR-TKIs疗效之间的关系,以期为EGFR少见突变患者的临床治疗提供相应的数据支撑。
1 材料与方法
1.1 研究对象
收集2012年1月至2016年4月新疆医科大学附属肿瘤医院经病理证实的携带少见确诊EGFR突变的晚期非小细胞肺癌患者29例的临床病理资料。所有患者均符合以下条件:1)病理学为肺腺癌的Ⅲb期/Ⅳ期患者;2)年龄≥18岁;3)治疗前组织标本均经EGFR基因检测;4)EGFR-TKIs治疗患者定义为至少接受30天吉非替尼、厄洛替尼、埃克替尼的标准治疗;5)至少有一个可测量病灶,根据实体瘤的疗效评价标准(Response Evaluation Criteria in Solid Tumors, RECIST)1.1定义的可测量病灶为靶病灶;6)临床分期根据美国癌症联合委员会第七版(AJCC)TNM分类决定;7)规律随访,有完整的病理资料。
1.2 方法
1.2.1 临床资料收集 包括年龄、性别、吸烟情况、民族、TNM分期、病理类型、原发灶位置、转移脏器数目、淋巴结转移部位、EGFR突变类型、靶向治疗药物最佳疗效、疾病进展时间、末次随访时间和死亡时间等。
1.2.2 ARMS(ADx)法 采用厦门艾德生物医药科技有限公司研发的人类EGFR基因突变检测试剂盒[荧光PCR法(ADx-EGFR29)]。具体操作步骤按试剂盒说明书进行。
1.2.3 疗效评价指标 根据实体瘤的疗效评价标准评价疗效,分为完全缓解(complete response,CR)、部分缓解(partial response,PR)、疾病稳定(stable disease,SD)和疾病进展(progressive disease,PD)。客观缓解率(ORR)=(CR+PR)/全部病例数×100%。疾病控制率(disease control rate,DCR)=(CR+PR+SD)/全部病例数× 100%。
1.3 统计学分析
采用SPSS 20.0软件进行统计学分析。各组间临床特征的比较采用χ2检验,采用Kaplan-Meier法计算患者的PFS并绘制生存曲线。P<0.05为差异具有统计学意义。
2 结果
2.1 少见突变患者临床特征
在29例少见突变患者中,男性19例,女性10例,平均年龄63.14(38~82)岁,有吸烟史12例,无吸烟史17例,17例有吸烟史的患者吸烟支数平均值为495.8(100~900)。肺鳞状细胞癌3例(10.3%),腺癌26例(89.7%)。其中汉族25例(86.2%),其他民族(包括维吾尔族1例、回族2例、俄罗斯族1例)4例,占3.8%。根据第AJCC七版TNM分期其中Ⅳ期21例,8例ⅢB期,原发病灶位于左肺13例(44.8%),右肺16例(55.2%)。最常见转移是同侧/对侧肺内转移14例,其余依次为骨转移10例、脑转移9例、肝转移5例、肾上腺转移4例、胸膜转移3例、肾转移1例,最常见转移淋巴结为肺门淋巴结8例、颈部3例、锁骨上/下淋巴结5例、纵隔1例、其他部位2例。患者临床病理特征,见表1。
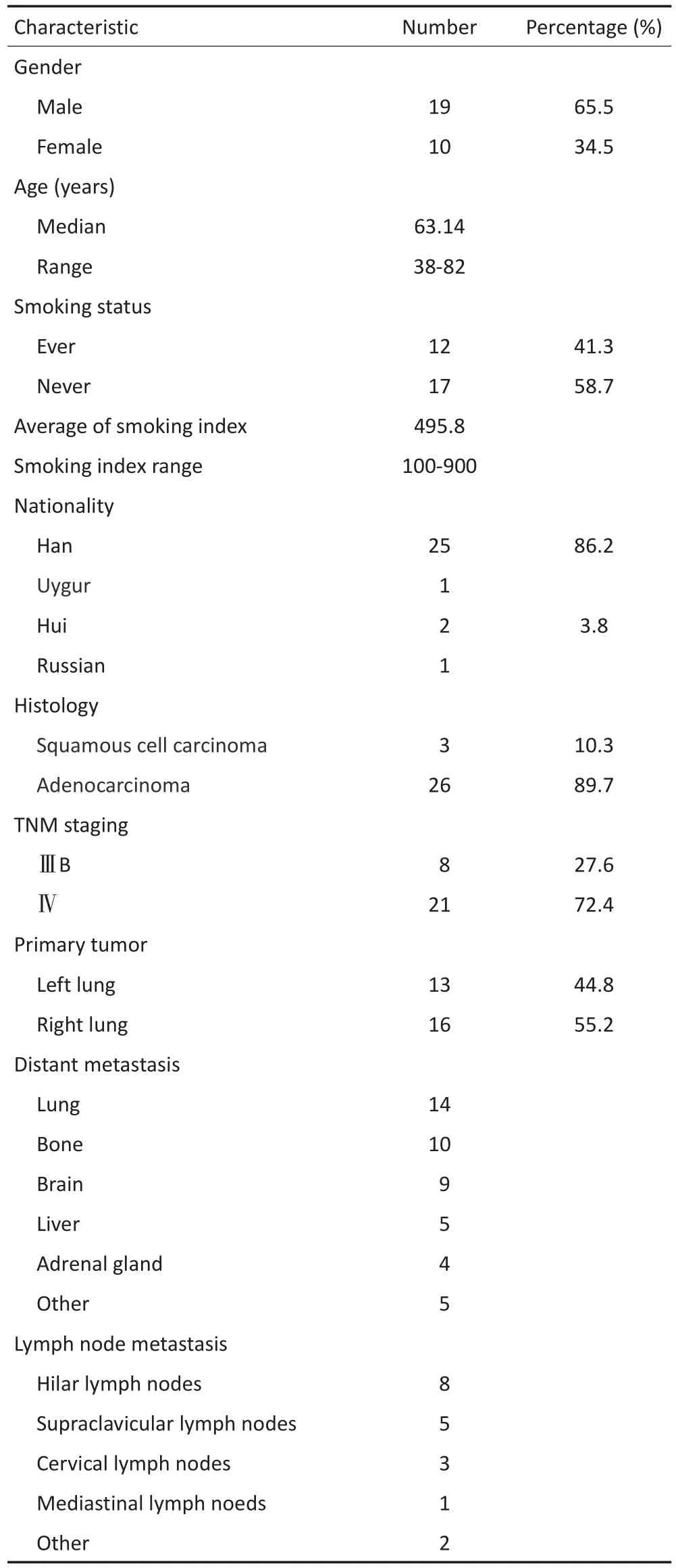
表1 少见EGFR突变患者临床病理特征Table 1 Clinicopathologic features of patients with uncommon mutations of EGFR
2.2 少见突变病理类型分析
29例少见突变患者中,单突变16例,L861Q 5例,G719X 5例,20外显子插入突变4例,S768I 2例。双突变11例,S768I及20ins突变4例,L858R及S768I双突变1例,19Del及T790M双突变1例,L861Q及G719X双突变2例,19Del及S768I突变1例,20ins及G719X突变1例,T790M及G719X突变1例。三突变2例,L858R、L861Q及G719X突变1例,S768I、20ins及G719X突变1例(表2)。
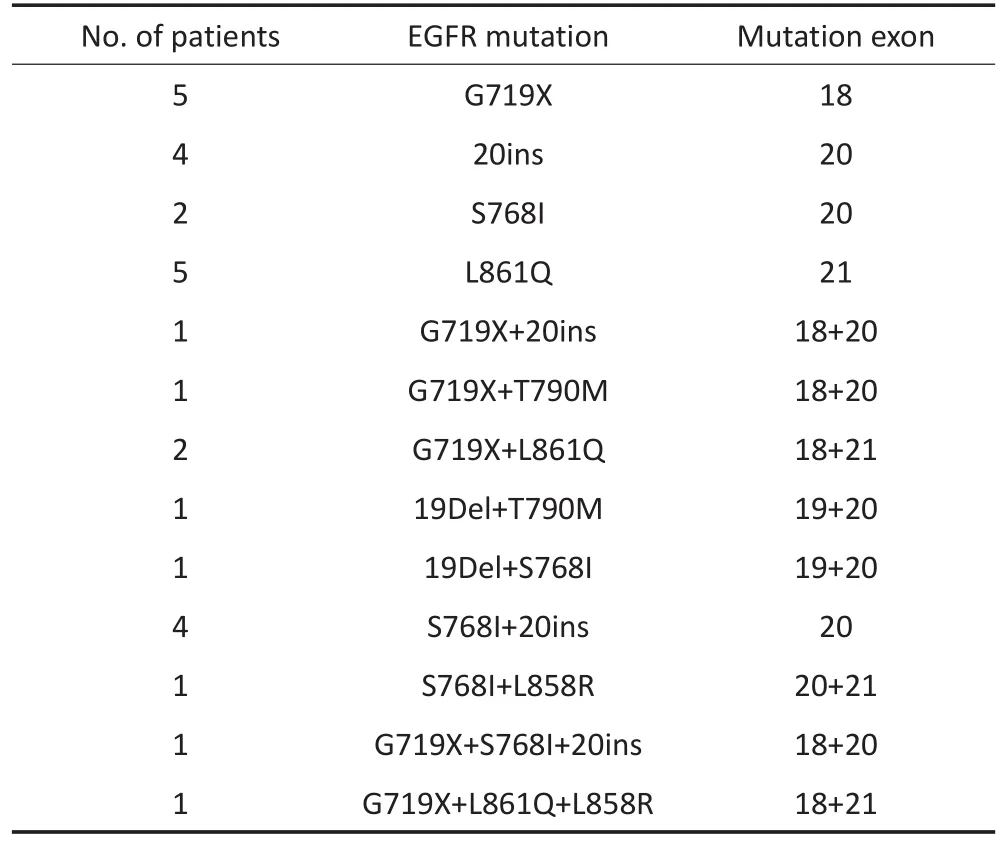
表2 EGFR突变的类型分布Table 2 Types of EGFR uncommon mutation
2.3 少见突变TKI治疗分析
29例患者均接受EGFR-TKIs治疗,其中吉非替尼16例,厄洛替尼12例,埃克替尼1例。一线EGFRTKIs治疗客观缓解率(ORR)43.75%,疾病控制率(DCR)50.00%,中位无疾病进展生存期(mPFS)5.50个月。二线EGFR-TKIs治疗客观缓解率(ORR)28.57%,疾病控制率(DCR)42.85%,中位无疾病进展生存期(mPFS)4.00个月。三线EGFR-TKIs治疗客观缓解率(ORR)33.33%,疾病控制率(DCR)50.00%,中位无疾病进展生存期(mPFS)2.67个月(表3~6)。

表3 一线接受EGFR-TKIs治疗的16例患者临床病理特征及疗效Table 3 Summary of clinical information of 16 patients treated with first-line EGFR-TKIs
对于少见突变患者,无论是ORR、DCR还是mPFS,一线EGFR-TKIs治疗似乎略优于二线及三线治疗,但其mPFS无显著性差异(P>0.05,图1)。

表3 一线接受EGFR-TKI治疗的16例患者临床病理特征及疗效(续表3)Table 3 Summary of clinical information of 16 patients treated with first-line EGFR-TKIs
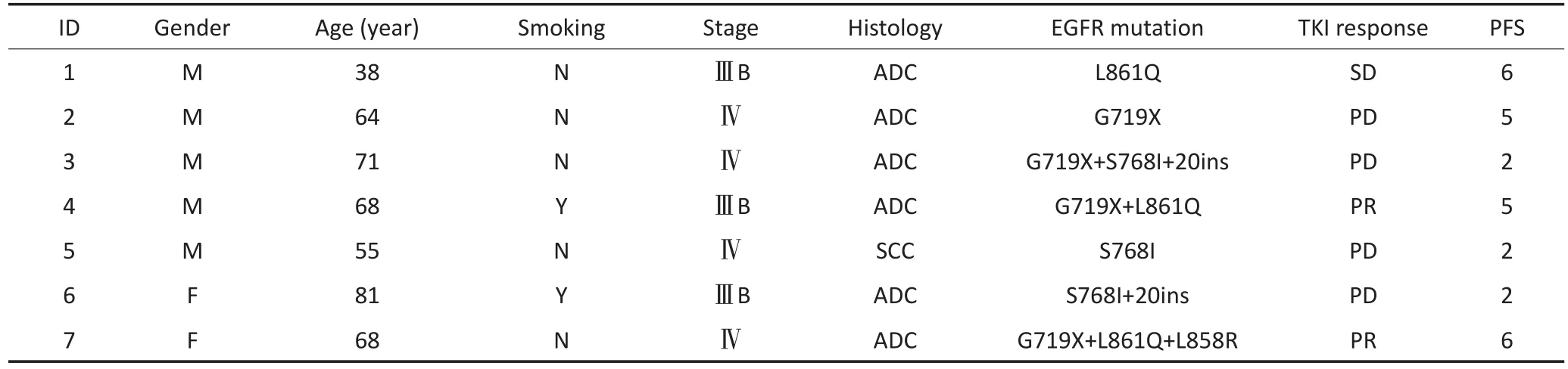
表4 二线接受EGFR-TKIs治疗的7例患者临床病理特征及疗效Table 4 Summary of clinical information of seven patients treated with second-line EGFR-TKIs

表5 三线接受EGFR-TKIs治疗的7例患者临床病理特征及疗效Table 5 Summary of clinical information of seven patients treated with third-line EGFR-TKIs

表6 29例少见突变患者经EGFR-TKIs治疗近期疗效汇总Table 6 Summary of short-term effects of 29 cases with EGFR uncommon mutation treated with EGFR-TKIs
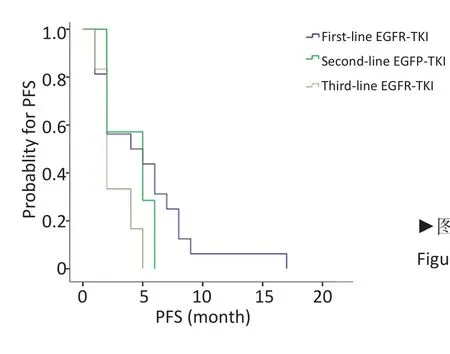
▶图1 EGFR少见突变患者接受EGFR-TKI治疗的PFSFigure 1 The PFS analysis of patients with EGFR uncommon mutations treated with EGFR-TKIs
3 讨论
EGFR是表皮生长因子受体,属于酪氨酸激酶型受体,在恶性肿瘤中常过表达,与配体结合参与细胞的增殖,分化,血管形成,肿瘤转移及抗凋亡等过程。EGFR靶向治疗开启了肺癌治疗的新时代,但治疗敏感性与EGFR突变状态明显相关。其中最常见的突变位19号外显子缺失突变(19Del)和21号外显子点突变(L858R),占所有突变的80%~90%[8,11-12]。
少见突变因发生比例低,目前循证医学证据仅见一些小样本的回顾性研究及个案报道,有研究显示一线接受EGFR-TKIs治疗的少见敏感突变患者有效率可达85.7%,其中少见突变合并19Del及L858R复合突变患者获益比例高,部分复合突变患者ORR及中位PFS、OS与常见突变相似[13]。在本研究回顾分析了ⅢB期/Ⅳ期非小细胞肺癌少见突变病例29例,发现EGFR少见突变发生比例与患者的性别,吸烟与否无显著性差异。最常见的远处转移器官依次为肺、骨、脑、肝、肾上腺,最常见的转移淋巴结依次为肺门淋巴结、锁骨上/下淋巴结、颈根部淋巴结及纵隔淋巴结。本研究比较患者EGFR-TKIs的疗效可以发现一线接受EGFR-TKIs治疗客观缓解率(ORR)43.75%,疾病控制率(DCR)50.00%,中位无疾病进展生存期(mPFS)5.50个月。二线EGFR-TKIs治疗ORR为28.57%,DCR为42.85%,mPFS为4.00个月。三线EGFR-TKIs治疗ORR为33.33%,DCR 50.00%,mPFS为2.67个月。结果显示随着EGFR-TKIs治疗的后移,其疗效呈逐渐减弱的趋势,中位无疾病进展生存时间缩短,但因病例数较少,无显著性差异。这可能与患者体力状态,药物耐受性及EGFR突变峰度变化及继发性耐药相关。
本研究少见突变位点中最常见为G719X,在29例患者中G719X突变5例,复合突变6例。G719位于18外显子的点突变包括第719位点的甘氨酸被丝氨酸、丙氨酸或半胱氨酸(G719S/A/C)所取代。既往研究显示G719突变型与ATP亲和力介于野生型EGFR及L858R之间[14],G719X单突变ORR为36.8%,但也有报道显示G719突变无论是单突变还是双突变,ORR均可达53.3%,中位PFS为8.1个月[15]。本研究中5例G719X突变患者ORR达80%,mPFS为6个月。6例复合突变患者ORR达50%,mPFS为3.5个月。其最佳疗效为部分缓解(PR),单突变ORR及PFS均优于复合突变患者,但低于经典突变。可能原因为部分复合突变患者同时携带了耐药突变,其与ATP的亲和能力较G719单突变低,同时不排除旁路干扰可能。
L861Q为本研究另一常见突变位点,是EGFR第 20号外显子上861位密码子点突变,在本研究29例患者中L861Q单突变有5例,合并G719X为1例,合并G719X、L858R为1例。既往报道显示L861Q在EGFR突变的2%[16],提示一代EGFR-TKIs对L861Q耐药。也有报道提示部分EGFR-TKIs对L816Q有效,但有效率低于L858R及G719[10]。NEJ002研究回顾性分析了7例G719X、3例L8861Q,吉非替尼治疗组少见敏感突变NSCLC患者中位OS明显低于常见敏感突变组,而化疗组少见敏感突变患者的中位OS与常见敏感突变组差异无统计学意义[17]。本研究中5例L861Q患者使用一代EGFR-TKIs治疗后ORR为40%,mPFS为6.2个月。
综上所述,EGFR少见突变因包含不同类型及亚型,其对EGFR-TKIs治疗的有效率及生存时间存在较大个体差异,可能与其参与了不同的信号转导途径相关。总体来说EGFR少见突变患者ORR及PFS均较经典突变者低,部分高于野生型。一线EGFRTKIs治疗略优于二、三线的优势,面对常见突变合并少见敏感突变或耐药突变的患者建议考虑一线使用EGFR-TKIs药物,少见敏感突变合并少见耐药突变的患者EGFR-TKIs疗效有待进一步研究。因此在临床治疗方案选择上应区别对待不同的少见突变患者,其具体的作用机制还需进一步研究。
[1]Paez JG,Janne PA,Lee JC,et al.EGFR mutations in lung cancer:correlation with clinical response to gefitinib therapy[J].Science,2004, 304(5676):1497-1500.
[2]Mok TS,Wu YL,Thongprasert S,et al.Gefitinib or carboplatin-paclitaxel in pulmonary adenocracinoma[J].N Engl J Med,2009,361 (10):947-957.
[3]Mitsudomi T,Morita S,Yatabe Y,et al.Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor(WJTOG3405):an open label,randomised phase 3 trial[J].Lancet Oncol,2010,11(2):121-128.
[4]Zhou C,Wu YL,Chen G,et al.Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-smallcell lung cancer(OPTIMAL,CTONG-0802):a multicentre,open-label,randomised,phase 3 study[J].Lancet Oncol, 2011,12(8):735-742.
[5]Arrieta O,Campos-Parra AD,Zuloaga C,et al.Clinical and pathological characteristics,outcome and mutational profiles regarding nonsmall-cell lung cancer related to wood-smoke exposure[J].J Thorac Oncol,2012,8:1228-1234.
[6]Arrieta O,Cardona AF,Federico Bramuglia G,et al.Genotyping nonsmall cell lung cancer(NSCLC)in Latin America[J].J Thorac Oncol, 2011,6:1955-1959.
[7]Lee HJ,Kim YT,Kang CH,et al.Epidermal growth factor receptor mutation in lung adenocarcinomas:relationship with CT characteristics and histologic subtypes[J].Radiology,2013,268:254-264.
[8]Koyama N,Watanabe Y,Iwai Y,et al.Distinct Benefit of Overall survival between patients with non-small-cell lung cancer harboring EGFR exon 19 deletion and exon 21 L858R Substitution[J].Chemotherapy,2017,62(3):151-158.
[9]O'Kane GM,Bradbury PA,Feld R,et al.Uncommon EGFR mutations in advanced non-small cell lung cancer[J].Lung Cancer,2017,109: 137-144.
[10]Frega S,Lorenzi M,Fassan M,et al.Clinical features and treatment outcome of non-small cell lung cancer(NSCLC)patients with uncommon or complex epidermal growth factor receptor(EGFR)mutations[J].Oncotarget,2017,8(20):32626-32638.
[11]Lynch TJ,Bell DW,Sordella R,et al.Activating mutations in the epidermal growth factor receptor underlying responsiveness of nonsmall-cell lung cancer to gefitinib[J].N Engl J Med,2004,350(21): 2129-2139.
[12]Sharma SV,Bell DW,Settleman J,et al.Epidermal growth factor receptor mutations in lung cancer[J].Nat Rev Cancer,2007,7(3): 169-181.
[13]Kobayashi S,Canepa HM,Bailey AS,et al.Compound EGFR mutations and response to EGFR tyrosine kinase inhibitors[J].J Thorac Oncol, 2013,8(1):45-51.
[14]Li K,Yang M,Liang N,et al.Determining EGFR-TKI sensitivity of G719X and other uncommon EGFR mutations in non-small cell lung cancer:Perplexity and solution(Review)[J].Oncol Rep,2017, 37(3):1347-1358.
[15]Wu JY,Yu CJ,Chang YC,et al.Effectiveness of tyrosine kinase inhibitors onquot;uncommonquot;epidermal growth factor receptor mutations of unknown clinical significance in non-small cell lung cancer[J]. Clin Cancer Res,2011,17(11):3812-3821.
[16]Mitsudomi T,Yatabe Y.Epidermal growth factor receptor in relation to tumor development:EGFR gene and cancer[J].FEBS J,2010,277 (2):301-308.
[17]Watanabe S,Minegish Y,Yoshizawa H,et al.Effectiveness of gefitinib against non-small-cell lung cancer with the uncommon EGFR mutations G719X and 816Q[J].J Thorac Oncol,2014,9(2):189-194.
(2017-03-17收稿)
(2017-06-16修回)
(编辑:杨红欣 校对:周晓颖)
Clinicopathologic characteristics of non-small cell lung cancer patients with seldom mutation types of epidermal growth factor receptor and treatment analysis
Qiao ZHANG1,Xiang LIU2,Jianjun LI1,Yanzhen CAO3,Jian ZHANG4,Li SHAN1
1Lung Cancer No.1 Ward;2Medical Department;3Department of Pathology,Tumor Hospital Affiliated to Xinjiang Medical University,Urumqi 830011,China;4Medical Team of 69260 Troops,Chinese People's Liberation Army,Urumqi 830017,China
Objective:To compare clinicopathologic parameters of uncommon mutations of epidermal growth factor receptor(EGFR) and preliminary therapeutic effects of EGFR-TKI treatment in patients with non-small cell lung cancer.MethodsWe collected clinicopathological data from 29 patients with non-small cell lung cancer who carry uncommon mutations of EGFR,which were pathologically confirmed in the Tumor Hospital Affiliated to Xinjiang Medical University,from January 2012 to April 2016.Then we analyzed the relationship between the clinicopathologic characteristics of uncommon mutations and therapeutic effects of EGFR-TKIs.Results:Among the 29 cases of patients with uncommon mutations,the most common distant metastasis organs were ipsilateral/contralateral lung tissue,bone,brain,liver,and adrenal gland;the most common metastatic lymph nodes were hilar lymph node,supraclavicular/ subclavian lymph node,neck-root lymph node,and mediastinal lymph node.In seldom mutations,16 cases of single mutation were found:5 cases of L861Q,5 cases of G719X,4 cases of 20ins,and 2 cases of S768I.By contrast,11 cases of double mutations were found:4 cases of S768I and 20ins,1 case of double mutation of L858R and S768I,1 case of double mutation of 19Del and T790M,2 cases of double mutations of L861Q and G719X,1 case of 19Del and S768I,1 case of 20ins and G719X,and 1 case of T790M and G719X.Moreover,2 cases of triple mutation were found:1 case of L858R,L861Q,and G719X;1 case of S768I,20ins,and G719X.The objective response rate(ORR)of the first-line EGFR-TKI therapy was 43.75%,the disease control rate(DCR)was 50%,and the median progression-free survival(mPFS)was 5.5 months.Furthermore,the ORR of the second-line EGFR-TKI therapy was 28.57%,the DCR was 42.85%,and the mPFS was 4 months.Moreover,the ORR of the third-line EGFR-TKI therapy was 33.33%,the DCR was 50.00%,and the mPFS was 2.67 months.Conclusion:Great individual differences were found on EGFR uncommon mutations for effective rate and survival time of EGFR-TKI treatment;in general,ORR and mPFS of EGFR seldom mutations were lower than classical mutations and partly higher than wild types.The first-line therapeutic effects of EGFR-TKI therapy was slightly better than the second-line or third-line therapeutic effects;however,no significant statistical difference was observed.
non-small cell lung cancer,EGFR,target therapy,uncommon mutation
①新疆医科大学附属肿瘤医院肺内科一病区(乌鲁木齐市830011);②医务部;③病理科;④中国人民解放军69260部队卫生队
单莉 teen825@sohu.corn
10.3969/j.issn.1000-8179.2017.21.313

张峤 专业方向为胸部肿瘤的基础及临床研究。E-mail:962923466@qq.com
猜你喜欢
电子科技大学学报(2022年5期)2022-10-29
中国生殖健康(2020年4期)2021-01-18
中华养生保健(2020年7期)2020-11-16
房地产导刊(2020年10期)2020-11-16
中外文摘(2020年13期)2020-08-01
福建基础教育研究(2020年4期)2020-05-28
时代英语·高三(2019年4期)2019-09-03
中国生殖健康(2018年4期)2018-11-06
幸福·悦读(2016年11期)2016-12-21
中学生理科应试(2014年12期)2015-01-15