低角与均角安氏Ⅱ类1分类错肌激动器治疗前后软硬组织变化
2017-11-13 01:48:30张延晓,陈瑛,徐庆
实用口腔医学杂志 2017年5期

目的探讨肌激动器对不同骨面型的安氏Ⅱ类1分类患者矫治前后软硬组织变化的影响。方法纳入22 例骨性安氏II类1分类患者[(男12 例,女10 例,平均年龄(11.5±0.67) 岁],根据其骨面型分为低角组(n=15)和均角组(n=7)。肌激动器矫治前后拍摄头颅侧位定位片,头影测量分析治疗前后软硬组织的变化。用SPSS 13.0软件,t检验分析治疗结果差异。结果所有患者治疗前后Co-Pg、ANB、Wits、NA-Pg、L1-APg和L6-MP值差异具有统计学意义(P<0.05)。骨组织项目中低角组和均角组治疗前后Wits值变化分别为1.34°±1.82°和3.50°±1.77°,NA-Pg值变化分别为(3.06±2.00) mm和(5.80±3.17) mm,牙齿项目中L1-APg变化值分别为(-1.16±1.74) mm和(-2.83±1.48) mm,组间差异均具有显著统计学意义(P<0.05)。低角与均角组软组织测量项目比较差异无统计学意义(P>0.05)。结论肌激动器矫治低角和均角骨性安氏II类1分类患者均能取得较理想的治疗效果,均角患者对矫治器的反映效果好于低角患者。
垂直骨面型; 肌激动器; 功能矫治器; 头影测量; 安氏Ⅱ1

1 材料与方法
1.1 研究对象
1.2 矫治方法
1.3 X线头影测量项目
1.3.4 软组织测量项目 UL-Eline,上唇突点到审美平面的距离;LL-Eline,下唇突点到审美平面的距离;∠N'-A'-FH,软组织鼻根点和上唇凹点的连线与眶耳平面之交角;∠N'-Pg'-FH,软组织鼻根点和软组织颏前点连线与眶耳平面之交角;∠N'-Sn-Pg',软组织鼻根点,软组织颏前点分别与鼻底点连线,两线相交成角;ZAngle,软组织颏前点和相对位置靠前的上下唇突点的连线的延长线与FH平面的后下之交角。
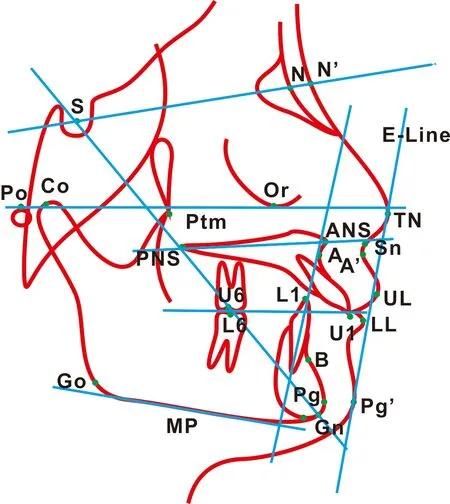
图 1 测量标志点及参考平面
1.4 统计学分析
采用SPSS 13.0统计软件进行统计分析,对所有测量数据进行t检验,P<0.05具有显著统计学意义。
2 结 果
另外,SNB 2 组治疗后比治疗前均有所增大,均角组增大值多于低角组,但低角组治疗前后比较差异有统计学意义。ANS-Ptm均有所增大,但均角组治疗前后比较差异有统计学意义。U6-PP 2 组治疗前后比较均有所增大,其中低角组治疗前后比较差异有统计学意义。∠L1-NB值2 组治疗后比治疗前均稍有增大,其中均角组治疗前后比较差异有统计学意义。
3 讨 论
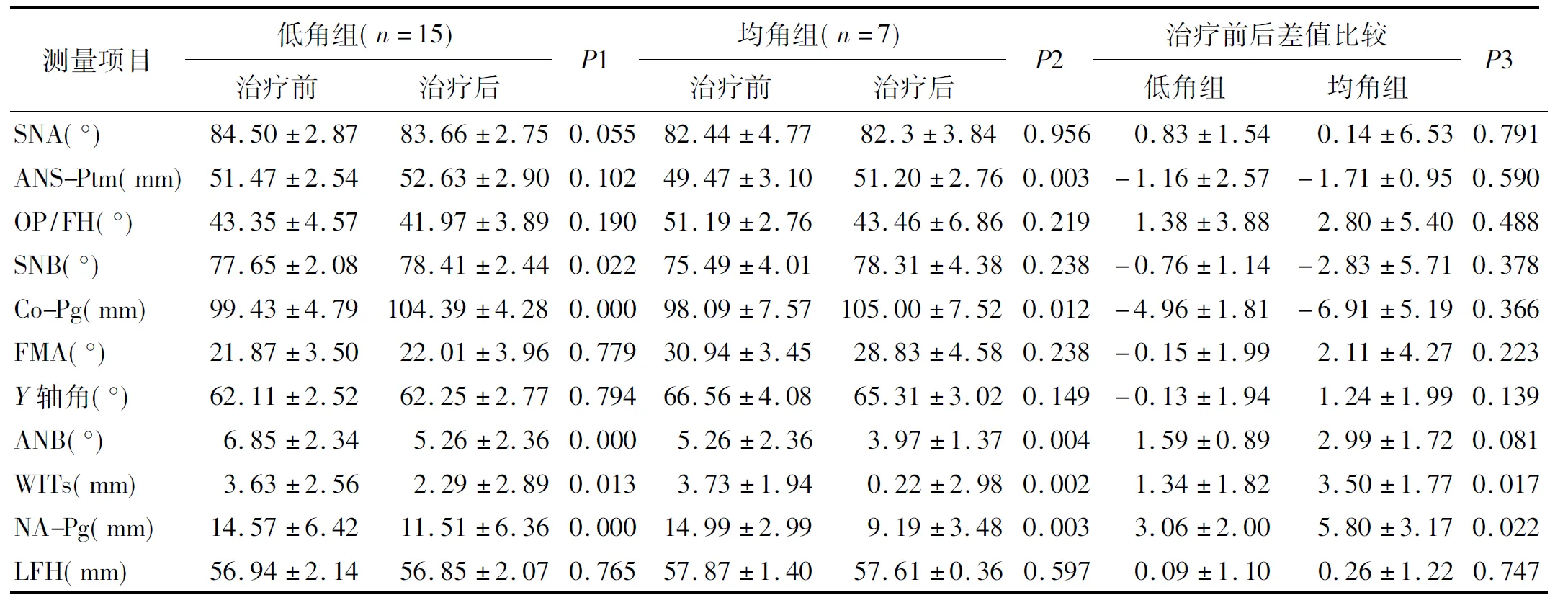
表 1 骨组织测量项目
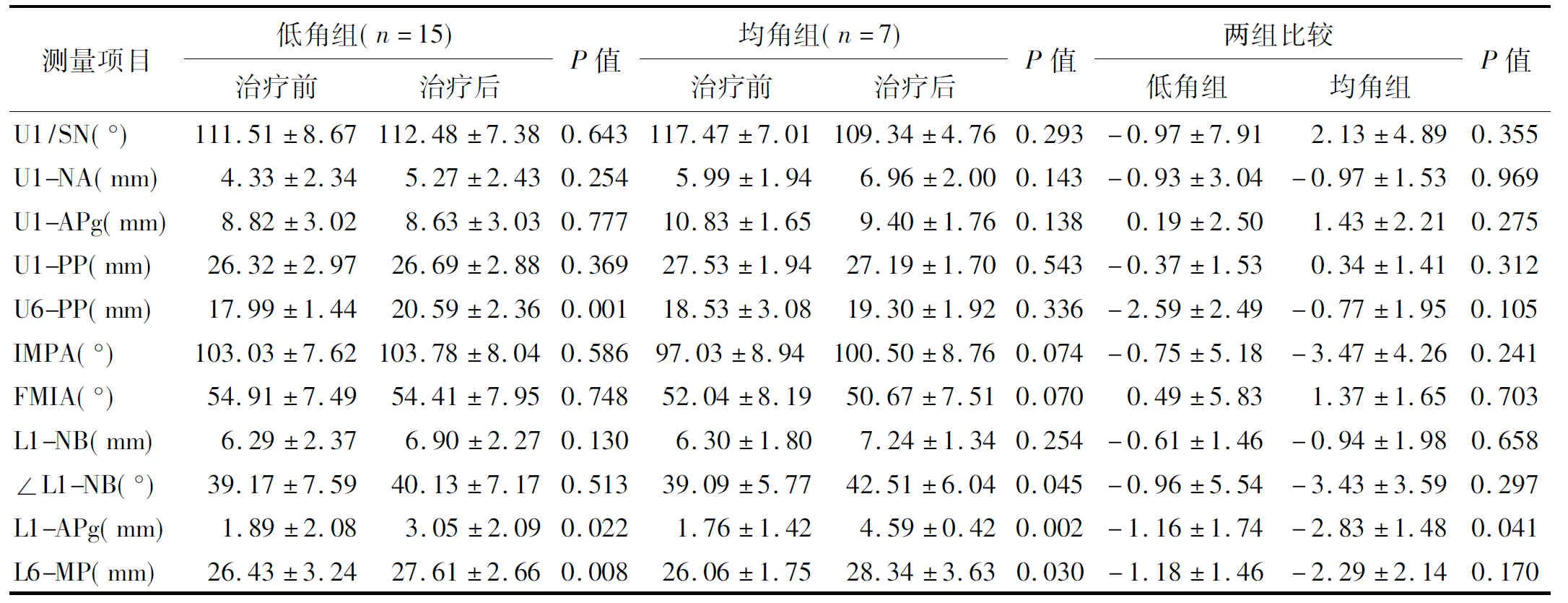
表 2 牙齿测量项目
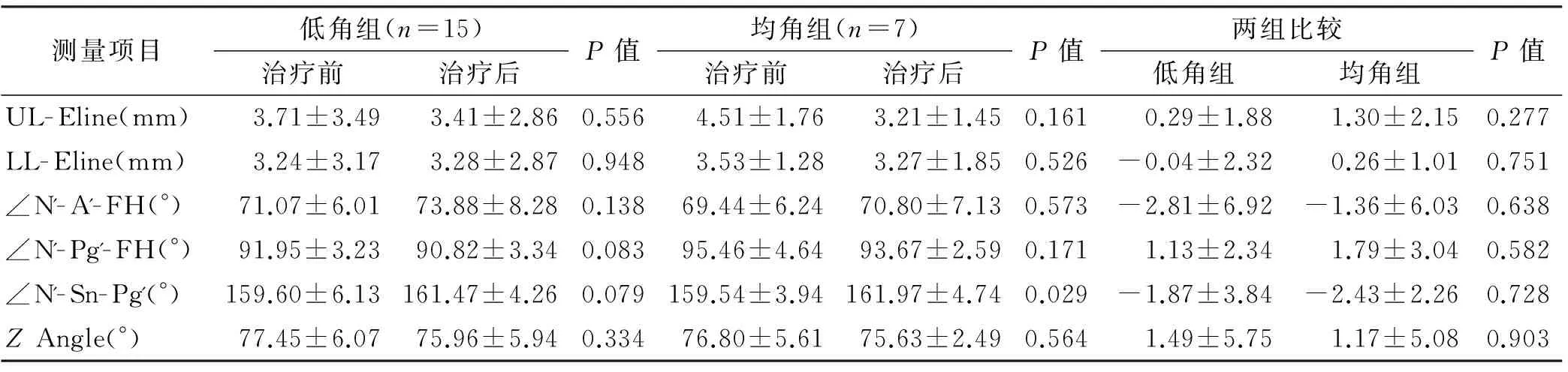
表 3 软组织测量项目
3.1 上、下颌骨变化情况
结果显示2 组SNA和OP/FH治疗后均略有减少,但变化不明显;均角患者治疗后上颌骨长度增加,治疗前后差异有统计学意义,可能是生长发育的原因;2 组SNA、ANS-Ptm和OP/FH比较无明显差别。对于肌激动器是否能抑制上颌骨的生长,学者们有不同的看法。Cozza等[4]用肌激动器矫治了40 例替牙列患者,发现治疗后SNA减少了0.5°;Maran等[5]用肌激动器联合头帽治疗了28 例混合牙列患者治疗后SNA减少了2°,而Lerstøl 等[6]发现肌激动器联合头帽治疗后SNA变化不大。Van[7]认为单纯的肌激动器对上颌复合体的作用并不明确,但它与口外牵引联合使用时,可以抑制上颌骨的向前与向下生长,并阻止腭部下降。
所有患者SNB治疗后均有所增加,低角组治疗前后有差异;下颌平面角(FMA)和Y轴角治疗前后没有明显变化;2 组患者下颌骨长度(Co-Pg)治疗后比治疗前均有明显增加;测量的4 个下颌指标2 组之间比较无明显差别。以上说明肌激动器治疗后,B点前移,下颌长度有所增加。曹凌[8]以未做功能矫治的下颌后缩Ⅱ类患者为对照,发现对照组治疗后SNB角增大了0.2°,下颌长度增加1.3 mm,而肌激动器治疗组SNB增大1.8°,下颌长度增加了2.2 mm, 明显多于对照组,因此认为肌激动器可以促进下颌的生长发育。下颌前伸对下颌骨的生长及改建是否产生实质性的影响尚存在争论。McNamara[9]认为下颌前伸能刺激髁突的改建,从而能刺激整个下颌骨的生长;Ma等[10]发现肌激动器治疗后关节窝变浅,髁突高度增加,矢状向髁突轻微前移,关节盘明显后移,关节盘没有改建。Luder[11]则把下颌前伸引起的下颌骨位置变化归于牙槽骨及下切牙位置的补偿性改变,否定有任何实质性的骨改建。Jakobsson等[12]指出用肌激动器治疗后下颌平面角与治疗前比较有显著性差异,他认为下颌平面角的增长是治疗中下颌骨的向前下旋转所致,而与下后牙的萌出无关;在正常生长发育的儿童中,随着下面高的增长,颏点顺时针向后旋转,但由于下颌长度的增长,使颏部相对于头颅位置以每年1 mm的速度向前生长。本研究中2 组患者治疗后下颌平面角没有显著变化,表明由于下颌功能性后缩的消除,抵消了下面高增加所致的不利影响,使下颌平面角保持不变,与曹凌[8]的研究基本一致。
3.2 牙齿变化情况
3.3 软组织变化情况
各项指标治疗前后无明显差别,2 组之间也无差别,可能与样本量小有关系。但从侧貌上看治疗后比治疗前还是有明显改善的。软组织形态是人们评价颜面外形的最直接指标, 是正畸患者就诊的主要原因之一,要达到良好的正畸疗效,必然要考虑到患者的软组织形态。Türkkahraman等[16]观察到肌激动器治疗后下唇的突出,认为肌激动器能成功的改变下唇位置,改善软组织凸度。Mara等[5]发现治疗后软组织面角(G'-Sn-Pg' )增大了2.3°,颏唇沟深度减少了0.8 mm;曹凌[8]发现与未治疗的对照组相比,实验组的G'-Sn-Pg'增大1.9°;本实验中低角和均角组G'-Sn-Pg' 分别增大了1.87°±3.84°和2.43°±2.26°。Varlik等[17]认为安氏Ⅱ类错患者经过肌激动器矫治后,额突角和下唇基角都有增大,使得下领后缩面型得到改善。基于现在的文献,肌激动器等功能矫治器对软组织的改变还是存在争议的,需要长期的双盲的前瞻型的随机研究证实,三维定量测量可以帮助我们解决头颅侧位定位片分析带来的局限[18-19]。
[2] Fisk RO, Wilson RE. Selection of patients amenable to simple orthodontic procedure using a malocclusion treatment severity index[J]. J Can Dent Assoc(Tor), 1973, 39(7): 468-471.
[3] James A, McNamara JA Jr. Components of class Ⅱ malocclusion in children 8-10 years of age[J]. Angle J Orthod, 1981, 51(3): 177-202.
[4] Cozza P, De Toffol L, Colagrossi S. Dentoskeletal effects and facial profile changes during activator therapy[J]. Eur J Orthod, 2004, 26(3): 293-302.
[6] Lerstøl M, Torget O, Vandevska-Radunovic V. Long-term stability of dentoalveolar and skeletal changes after activator-headgear treatment[J]. Eur J Orthod, 2010, 32(1): 28-35.
[7] Van Beek H. Overjet correction by a combined headgear and activator.[J]. Eur JOrthod, 1982, 4(4): 279-290.
[8] 曹凌. 肌激动器对下颌生长发育影响的对比研究[D]. 西安: 第四军医大学, 2001.
[9] McNamara JA Jr, Bryan FA.Long-term mandibular adaptations to protrusive function: An experimental study in Macaca mulatta[J]. Am J Orthod Dentofacial Orthop, 1987, 92(2): 98-108.
[10]Ma X, Fang B, Dai Q, et al. Temporomandibular joint changes after activator appliance therapy: A prospective magnetic resonance imaging study.[J]. J Craniofac Surg, 2013, 24(4): 1184-1189.
[11]Luder HU. Effects of activator treatment-evidence for the occurrence of two different types of reaction.[J]. Eur J Orthod, 1981, 3(3): 205-222.
[12]Jakobsson SO. Cephalometric evaluation of treatment effect on Class II, division I malocclusions.[J]. Am J Orthod, 1967, 53(6): 446-457.
[13]Lavergne J, Gasson N. The influence of jaw rotation on the morphogenesis of malocclusion[J]. American Journal of Orthodontics, 1978, 73(6):658-666.
[14]Greco M, Fichera G, Caltabiano M, et al. Short-term effects of the activator in skeletal Class II division 1 patients with different vertical skeletal pattern. A retrospective study[J]. Minerva Stomatol, 2010, 59(3):61-74.
[15]Pancherz H. A cephalometric analysis of skeletal and dental changes contributing to Class II correction in activator treatment[J]. Am J Orthod, 1984, 85(2): 125-134.
[16]Türkkahraman H, Sayin MO. Effects of activator and activator headgear treatment: Comparison with untreated Class II subjects[J]. Eur J Orthod, 2006, 28(1): 27-34.
[17]Varlik SK, Gültan A, Tümer N. Comparison of the effects of Twin Block and activator treatment on the soft tissue profile.[J]. Eur J Orthod, 2008, 30(2): 128-134.
[18]Flores-Mir C, Major PW. A systematic review of cephalometric facial soft tissue changes with the activator and bionator appliances in Class II division 1 subjects[J]. Eur J Orthod, 2006, 28(6): 586-593.
[19]Landázuri DR, Raveli DB, dos Santos-Pinto A, et al. Changes on facial profile in the mixed dentition, from natural growth and induced by Balters' bionator appliance[J]. Dental Press J Orthod, 2013, 18(2): 108-115.
[20]肖珲. 安氏Ⅰ类高、低角型正畸病例牙齿移动速度的比较研究[J]. 实用医学杂志, 2005, 21(14): 1519-1520.
[21]Yüksel S, Kaygisiz E, Ulusoy C, et al. Post-treatment evaluation of a magnetic activator device in Class II high-angle malocclusions[J]. Eur J Orthod, 2010, 32(4): 425-429.
[22]Dolce C, Schader RE, McGorray SP, et al. Centrographic analysis of 1-phase versus 2-phase treatment for Class II malocclusion[J]. Am J Orthod Dentofacial Orthop, 2005, 128(2): 195-200.
[23]Dolce C, McGorray SP, Brazeau L, et al. Timing of class II treatment: Skeletal changes comparing 1-phase and 2-phase treatment[J]. Am J Orthod Dentofacial Orthop, 2007 ,132(4): 481-489.
[26]Thiruvenkatachari B, Harrison JE, Worthington HV, et al. Orthodontic treatment for prominent upper front teeth(Class II malocclusion) in children[J]. Cochrane Database Syst Rev, 2013, 11: CD003452.
[27]Malta LA, Baccetti T, Franchi L, et al. Long-term dentoskeletal effects and facial profile changes induced by bionator therapy[J]. Angle Orthod, 2010, 80(1): 10-17.
[28]Dalci O, Altug AT, Memikoglu UT. Treatment effects of a twin-force bite corrector versus an activator in comparison with an untreated Class II sample: A preliminary report[J]. Aust Orthod J, 2014, 30(1): 45-53.
Theeffectsofactivatortreatmentonthehardandsofttissueprofileofdifferentskeletalpatterns
ZHANGYanxiao,CHENYing,XUQing.
214001,DepartmentofOrthodontics,WuxiStomatologyHospital,China
Objective: To evaluate skeletal, dentoalveolar and soft tissue profile changes by activator therapy in patients with different skeletal patterns of Class II 1 malocclusions.Methods22 subjects(10 girls, 12 boys, mean age 11.5±0.67 years) in the mixed or early permanent dentition , were included and divided into low angle(n=15) and average angle(n=7) groups on the basis of skeletal pattern. All patients were treated with a traditional activator. The skeletal, dentoalveolar and soft tissue profile changes were compared on lateral cephalograms before and after treatment. Statistical analysis was performed witht-test of SPSS 13.0 at a level of significance ofP<0.05.ResultsActivator treatment in these growing patients resulted in a correction of the skeletal Class II relationship(decrease of ANB , Wits and NA-Pg), an advancement of the mandibular structures(increase of Co-Pg and L1-APg), and changes of the teeth(increase of L6-MP). The changes of Wits, NA-Pg and L1-APg value of low and average angle groups were 1.34°±1.82° and 3.50°±1.77°,( 3.06±2.00) mm and (5.80±3.17) mm,(-1.16±1.74) mm and (-2.83±1.48) mm respectively(P<0.05). No statistical significance was found in the soft tissue profile changes whether intra-class or inter-group comparison.ConclusionThe activator appliance is effective in treating growing patients with mandibular deficiency, and mandibular reconstruction, in patients with average angle it is more effective than in those with low angle.
Verticalskeletalpattern;Activator;Functionalappliance;Cephalometricmeasurement;AngleⅡ1
214001, 无锡牙病防治所
陈瑛 E-mail: chenyin234@126.com
R783.5
A
10.3969/j.issn.1001-3733.2017.05.025
(收稿: 2017-03-22 修回: 2017-04-25)
猜你喜欢
昆明医科大学学报(2021年1期)2021-02-07 01:06:48
课外生活(小学1-3年级)(2019年10期)2019-11-29 01:56:02
中国医药指南(2019年3期)2019-01-07 05:12:03
中华老年口腔医学杂志(2016年5期)2016-03-01 02:24:23
西南医科大学学报(2016年4期)2016-01-03 01:26:25
中国医疗美容(2015年1期)2015-07-12 10:06:52
中国医疗美容(2015年1期)2015-07-12 10:06:37
中国医疗美容(2015年1期)2015-07-12 10:06:37
安徽医药(2014年9期)2014-03-20 13:14:02
好孩子画报(2014年2期)2014-03-07 22:17:24