
Potential predictive factors for pathologic complete response after the neoadjuvant treatment of rectal adenocarcinoma: a single center experience
2017-08-27 03:24:25FeryelLetaiefMeherNasriMounaAyadiKhedijaMeddebAminaMokraniYosraYahyaouiNesrineChraietHendaRaiesAmelMezlini
Cancer Biology & Medicine 2017年3期
Feryel Letaief, Meher Nasri, Mouna Ayadi, Khedija Meddeb, Amina Mokrani, Yosra Yahyaoui, Nesrine Chraiet, Henda Raies, Amel Mezlini
Department of Medical Oncology, Salah Azaïz Cancer Institute, Tunis 1006, Tunisia
Potential predictive factors for pathologic complete response after the neoadjuvant treatment of rectal adenocarcinoma: a single center experience
Feryel Letaief, Meher Nasri, Mouna Ayadi, Khedija Meddeb, Amina Mokrani, Yosra Yahyaoui, Nesrine Chraiet, Henda Raies, Amel Mezlini
Department of Medical Oncology, Salah Azaïz Cancer Institute, Tunis 1006, Tunisia
Objective: To assess the response rate of patients with rectal adenocarcinoma to neoadjuvant therapy and to identify the predictors of histological regression after neoadjuvant radiotherapy (RT) or concurrent chemoradiotherapy (CCRT). Methods: This study recruited 64 patients. The patients had resectable cancer of the lower and the middle rectum (T3/T4 and/or N+) without distant metastasis and
Rectal tumor; chemotherapy; neoadjuvant radiotherapy; pathologic complete response
Introduction
Colorectal cancer is the third most commonly diagnosed cancer worldwide following pulmonary and breast cancer1. Rectal cancer is a cancer of the digestive tract with the second highest increasing incidence; the American Cancer Society (ACS) estimates that approximately 39,220 new cases of rectal cancer occurred in 20162. It commonly occurs during the 5th and 6th decades of life1. Adenocarcinoma is the most common histological subtype of rectal cancer3. During the last two decades, a deeper understanding of the rectal anatomy and the development of novel therapeutic strategies have helped improve the prognosis of rectal cancer patients4. Furthermore, the recurrence of rectal cancer has been controlled or decreased by the introduction of total mesorectal excision (TME) as a treatment strategy for this cancer5. Surgical treatment is the gold standard treatment for early-stage rectal cancers without lymph node involvement (T1/T2 and N0)6. However, for advanced rectal cancer (T3/T4 and/or N+), surgical treatment alone is associated with a high risk of loco-regional recurrence7. Combining radiotherapy with surgery has transformed the therapeutic management of rectal cancer, decreasing the local recurrence of cancer and increasing the overall survival rate of patients8. Furthermore, certain studies have reported that the association of chemotherapy and radiotherapy with surgery intensifies these positive effects and allows successful tumor downstaging9,10. Compared with surgical resection alone or postoperative concurrent chemoradiotherapy (CCRT), preoperative CCRT improves local control and increases therate of sphincter conservation11. The response to neoadjuvant CCRT varies among different individuals. Most patients respond to neoadjuvant CCRT, and approximately 20% of patients achieve a pathologic complete response (pCR). Thus, they lack any viable tumor cells in the final surgical specimen12. Tumor response to radiochemotherapy is the main reason behind the development of novel surgical strategies for managing patients classified as good responders to neoadjuvant treatment. Therefore, certain cases only receive minimally invasive surgical procedures, such as anal sphincter conservation and local resection, or even only surveillance13. Given that patients with pCR have a better prognosis, and the treatment strategy for these patients may differ from that for patients without pCR, the ability to predict response to neoadjuvant CCRT is of great clinical importance. In addition, patients with pCR have a better long-term outcomes than those without pCR5. Certain retrospective studies have identified some clinical factors that are predictors of tumor response to preoperative CCRT, including tumor size and carcinoembryonic antigen (CEA) level14. However, these studies were limited by the small sample sizes of patients with pCR. Consequently, predicting pCR after neoadjuvant CCRT for rectal cancer patients remains a great challenge for clinicians. Therefore, this retrospective study was designed with the aim to evaluate the clinical and pathological responses of patients with rectal cancer to neoadjuvant treatments. In addition, this study aimed to help identify the potential predictive factors for pCR after neoadjuvant treatment in patients with locally advanced, middle, and low rectal cancer.
Patients and methods
Patient selection
This study was performed at Salah Azaïz Cancer Institute. Data were collected for 64 rectal cancer patients who were referred to the institution from 2006 to 2011 for preoperative chemotherapy. All patients had histologically confirmed rectal adenocarcinoma. All patients underwent MRI at initial staging and after neoadjuvant treatment. Only patients with T3 or T4 stage, with or without lymph node involvement and without distant metastases were eligible. All patients received neoadjuvant radiotherapy with or without chemotherapy followed by surgery. Patients were excluded if they had distant metastasis. Resected specimens were subjected to histological examination, and histological response was defined in accordance with Dworak classification. In this study, 3 groups of patients were categorized on the basis of histological response: complete response group (grade 4), partial response group (grades 1, 2, and 3), and no response group (grade 0). This study was approved by the ethics committee of Salah Azaïz Cancer Institute.
Treatments
Statistical analysis
Univariate analysis was performed using Fisher’s exact test. Survival curves were constructed using Kaplan-Meier methods. Survival analysis was performed with the log rank test. Factors with significant prognostic values were evaluated using the multivariate Cox regression model to explore the independent effects of potential predictors on pCR rate. A P<0.05 was considered statistically significant. All analyses were performed using IBM SPSS ver. 20.0 (IBM, Armonk, NY, USA). The predictive factors studied in the univariate analysis were age, sex, TNM stage, differentiation, nodal involvement, CEA level, hemoglobin level, lymphocyte level, and the association of chemotherapy with radiotherapy.
Results
The median age of the patients was 57 years (ranging from 22 to 85 years). The majority of rectal cancer patients was males and represented 56% of cases. All patients exhibited good performance status of 0 or 1. Of the patients, 48% had moderately differentiated histology. The median initial CEA concentration was 8.23 ng/dL (ranging from 1 ng/dL to 52ng/dL). The median initial Hb concentration was 11.7 g/dL (ranging from 7.9 g/dL to 17.2 g/dL). Of the 64 patients, 14 patients had T2 stage, 38 had T3 stage, and 12 patients had T4 stage tumors. The vast majority of patients (73%) presented lymph node involvement. The characteristics of the patients are summarized in Table 1.
A total of 24 patients (38%) received neoadjuvant CCRT, whereas 62% patients received neoadjuvant radiotherapyalone. All the patients received a radiotherapy dose of 45 Gy. The characteristics of neoadjuvant treatment are summarized in Table 2. All of the patients underwent surgery: 1 patient underwent local excision, 29 patients underwent Miles’surgery, and 34 patients underwent lower and anterior resection. Most of the patients underwent surgery with a delay of 6 to 8 weeks after neoadjuvant treatment (37 patients). The postoperative pCR rate was 19% (n=2), and the partial response rate was 56.3% (n=36). A total of four patients who underwent abdominoperineal resection exhibited pCR.
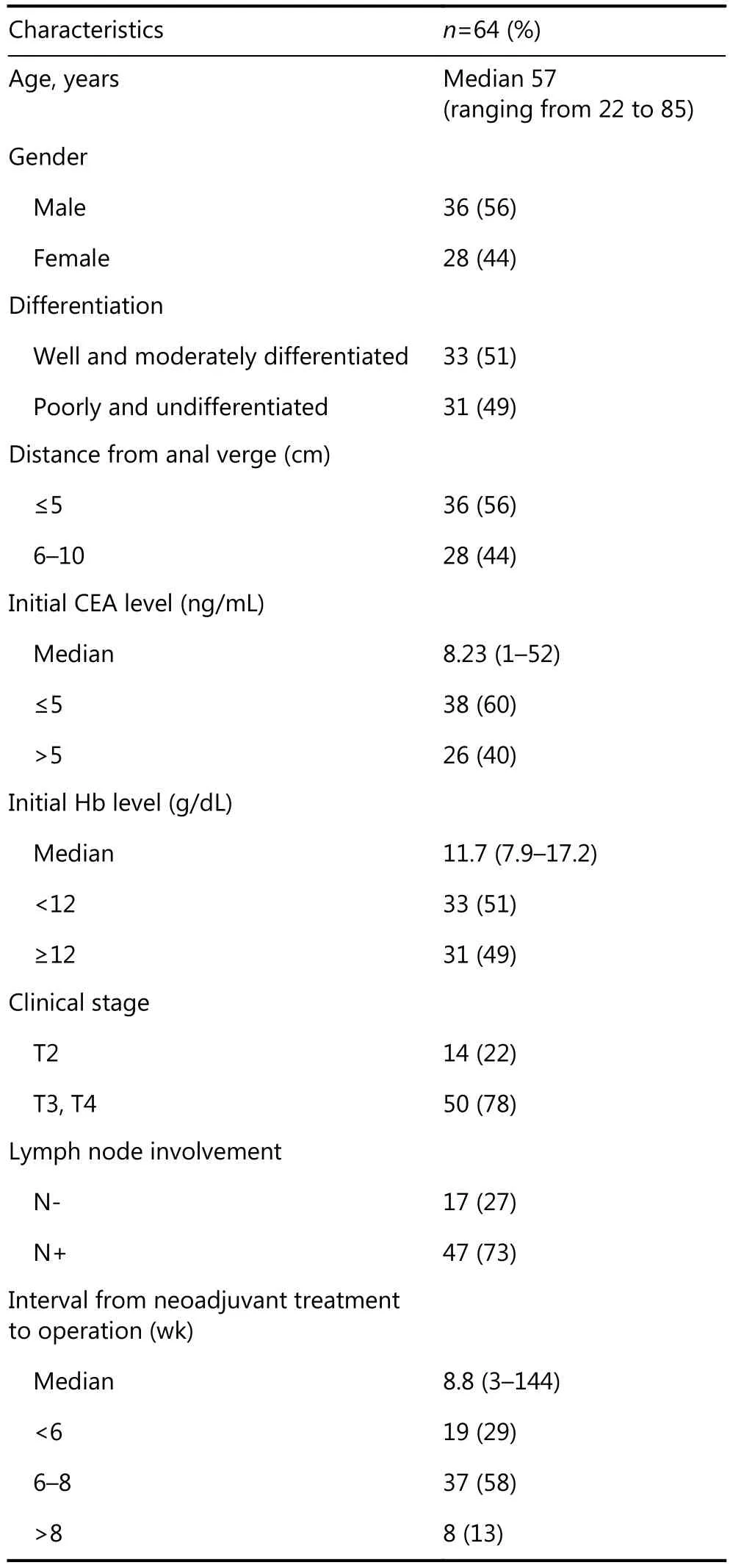
Table 1 Patient characteristics
The univariate and multivariate analyses of predictive factors for pCR are listed in Tables 3 and 4. In univariate analyses, patients with well- or moderate-differentiated histology had a higher, pCR rate than patients with poorly differentiated or undifferentiated histology (P=0.01). An interval of more than 8 weeks between neoadjuvant treatment and surgery was not a significant predictive factor (P=0.294) of pCR. pCR rate was higher in males (22%) than in females (14%). An initial CEA concentration of <5.0 ng/mL was associated with a higher pCR rate (31% vs. 0%; P=0.01), and pCR rate was also higher in patients with T2 stage cancer (43%) than in patients with T3 (18%) or T4 (8%) stage cancers (P=0.031). The differences in pCR rates between both genders and interval between surgery greater than 8 weeks were marginally significant. Univariate analyses revealed that initial Hb concentration and CEA level, absent lymph node involvement (cN0), T stage, CCRT, and well- or moderate-differentiated tumors were significantly associated with pCR. In our series, 28 patients presented radiological tumoral downstaging. ycT was significantly associated with increased pCR (P<0.001, OR=24, 95% CI 20–29). Statistical analysis, however, showed no association between ycN and pCR (P=0.241, OR=0.556, 95% CI 0.464–1.512) (Table 5).
Variables with P<0.05 were investigated in multivariate analysis. cN0 (P=0.03), neoadjuvant CCRT (P=0.01), andradiological tumor downstaging (P=0.02) were associated with pCR. Initial CEA (P=0.5), tumor differentiation (P=0.293), clinical T stage (P=0.329), and initial Hb level (P=0.462) were not independent predictive markers of pCR in multivariate analysis. Gastrointestinal (GI) diseases were the most commonly observed complication after neoadjuvant treatment. A total of 16 patients had grade 1 GI complications. Ten patients had grade 2 GI complications,which required pharmacotherapy. Six patients had grade 1 genitourinary (GU) complications. Three patients had grade 2 GU complications. No grades 3 or 4 complications were observed. Most of the patients tolerated surgical treatment. Two patients had grade 2 GI complications, including bowel obstruction, that required supportive management. No grades 3 or 4 complications occurred after surgery.
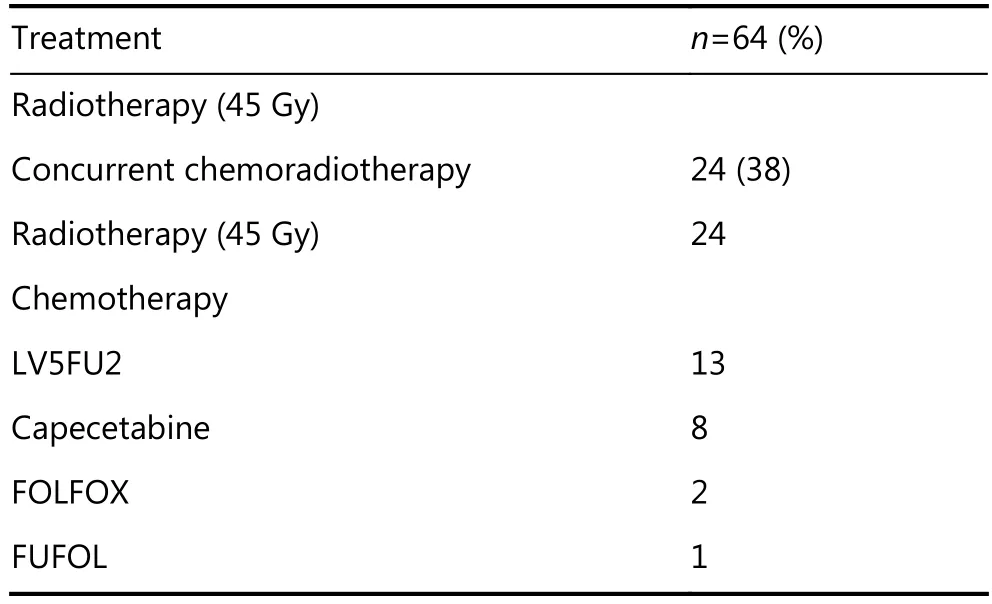
Table 2 Characteristics of neoadjuvant treatment

Table 3 Univariate analysis of predictors for pathologic complete response
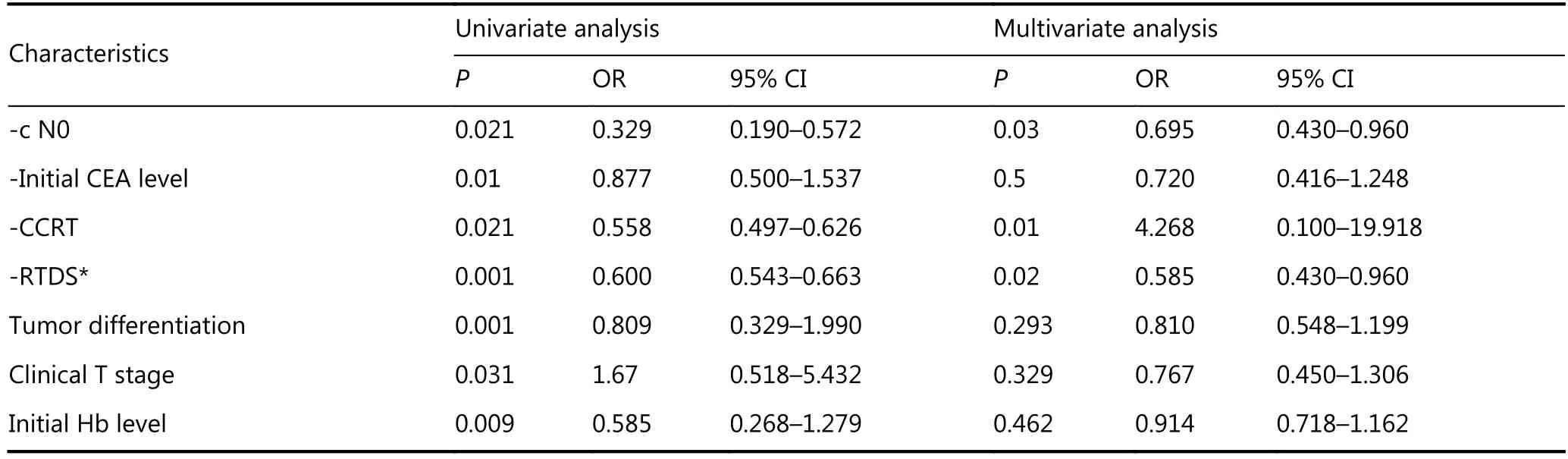
Table 4 Multivariate analysis of predictors for pathologic complete response
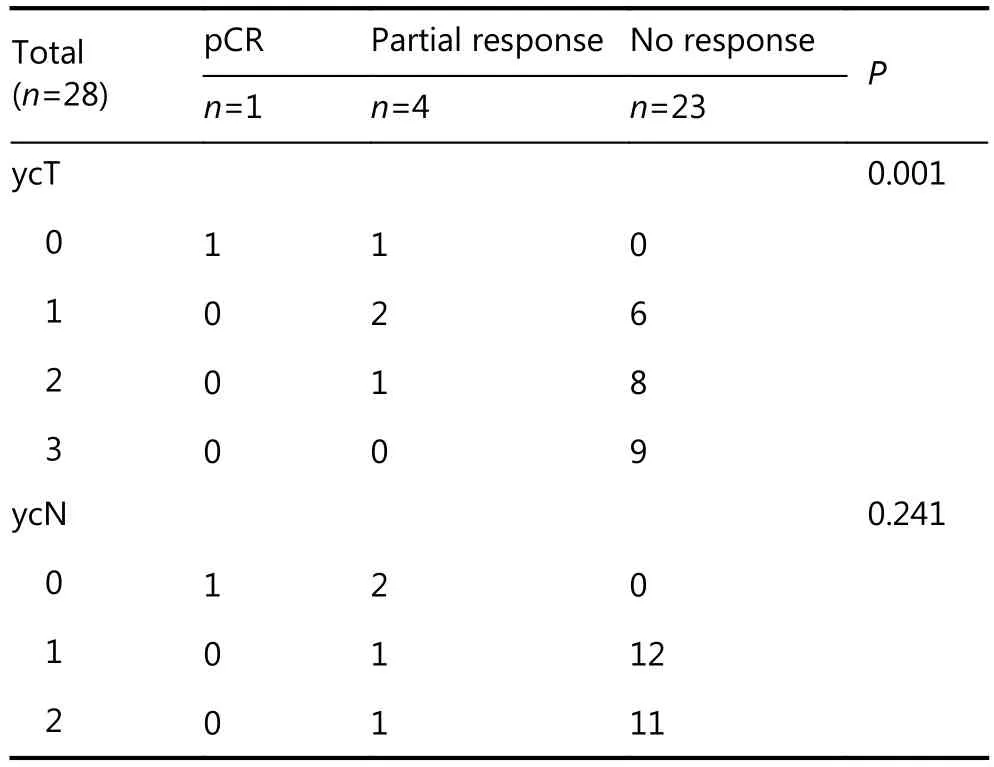
Table 5 Clinical significance of ycT staging and ycN staging to pCR in patients with downstaging effect
Discussion
A regional disparity in the worldwide incidence of rectal cancer has been reported. According to the International Agency for Research on Cancer (IARC), colorectal cancer is the third most frequently diagnosed cancer in men (9.4%) and the second most frequently diagnosed cancer in women (10%). Furthermore, the rates of colorectal cancer in developed countries (60% of cases) are higher than those in other countries1. According to the North Tunisia Cancer Registry 2004/2006, rectal cancer represents 39.3% of the diagnosed colorectal cancers in Tunisia15. From 1994 to 2006, the incidence of rectal cancer decreased considerably in men with a reported annual augmentation of 4%15. Adenocarcinoma remains by far the most frequently diagnosed histological type of rectal cancer, representing 83% and 84% of rectal tumors diagnosed in men and women, respectively15.
During the last two decades, the management of locally advanced rectal cancer has shown considerable progress due to three major revolutions in treatment strategies: TME, neoadjuvant radiotherapy, and neoadjuvant chemotherapy. These treatment methods have improved the local control of the disease and thus increased patients’ overall survival. In fact, before the development of TME and the emergence of neoadjuvant treatments, the recurrence rate of rectal cancer ranged from 20% to 30%16. In this study, 19% of cases presented pCR, as identified on the basis of Dworak classification17. A partial response was observed in 27% of cases. According to many publications, low-lying rectal cancer is associated with poor prognosis, which could explain the poor histological response associated with this localization. Das et al.18conducted a study with 562 patients who received neoadjuvant radiochemotherapy for nonmetastatic rectal adenocarcinoma. Multivariate analysis revealed that a 5 cm distance from the AV superior is significantly associated with poor histological response (P=0.035)18. However, in our series, distance from the AV was unassociated with pCR. We also found that pCR rate was significantly higher in patients with well-differentiated tumors and in the T2 stage; these results corresponded with those reported in the literature19.
We also investigated the predictive value of biologicalmarkers. Univariate analyses showed that an initial CEA concentration of <5 ng/mL was significantly associated with pCR (P=0.010). Related studies have reported that an initial CEA concentration of <5 ng/mL before neoadjuvant radiochemotherapy is a significant independent predictive factor of pCR18-20. Park et al.21reported that initial CEA concentration is associated with histological response, and that higher initial CEA concentrations are associated with higher risks of poor histological response [CEA (ng/mL) ≤3: 36.4% of tumor regression/CEA 3–6 ng/mL: 23.6% of tumor regression/CEA 6–9 ng/mL: 15.6% of tumor regression and CEA >9 ng/mL: 7.8% of tumor regression (P=0.001)]. Although Choi et al.16reported that an initial hemoglobin lever greater than 12 g/dL is predictive of histological response, we did not find that hemoglobin level is predictive of histological response in multivariate analysis. We also demonstrated that cN0 in rectal cancer patients was associated with high rates of pCR in univariate (P=0.021) and multivariate analyses (P=0.03). In previous studies, both Yoon et al.19and Choi et al.16identified that cN0 as an independent predictive factor of pCR and that the use of TME decreased the recurrence rate in rectal cancer patients (<10%)19.
Neoadjuvant radiotherapy decreases the two-year recurrence rate (2% recurrence rate for the neoadjuvant radiotherapy group)22. In addition, combining neoadjuvant chemotherapy and radiotherapy increases pCR rate and decreases local recurrence compared with the neoadjuvant radiotherapy alone but does not affect overall survival and disease-free survival9,10,23,24. In this study, the recruited patients received a 5FU-based neoadjuvant chemotherapy regimen9. Furthermore, certain studies have indicated that the combination of oxaliplatin with 5FU is not superior to 5FU alone, is not well tolerated, and is associated with increased toxicity grades of 3 to 425. Another attractive treatment strategy for patients with advanced rectal cancer is neoadjuvant chemotherapy followed by chemoradiation. Numerous clinical trials have reported a favorable outcome, such as higher pCR rate, higher progression, and disease-free survival along with a better overall survival among included patients26-30. PRODIGE 23 is an ongoing phase 3 trial evaluating the benefits of neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy compared with preoperative chemoradiotherapy alone in patients with resectable, locally advanced rectal cancer. The primary outcome of this trial is expected by next year (NCT01804790). Similarly, the preliminary results of the completed phase 2 trial of COPERNICUS in the UK reported the promising efficacy of 4 cycles of neoadjuvant oxaliplatin and fluorouracil followed by short-course preoperative radiotherapy and immediate surgery for resectable rectal cancer (NCT01263171)31.
Another reported predictive factor for pCR is the delay between neoadjuvant treatment and surgery. Usually, surgery is performed six to eight weeks after neoadjuvant chemoradiotherapy with a mean rate of pCR of 12%. In the GRECCAR-6 trial, the treatment response of 264 patients with T3–T4 N0 or Tx N+ adenocarcinoma of the mid/lower rectum after neoadjuvant radiochemotherapy is evaluated. The results showed that waiting 11 weeks after CCRT does not increase the rate of pCR after surgical resection. A longer waiting period may be associated with higher morbidity and more difficult surgical resection32. In the present study, the patients received surgical treatment after a median delay of 8.8 weeks after neoadjuvant treatment; however, the surgical treatment was not predictive of pCR.
Conclusions
We investigated the potential predictive factors for the pCR of rectal cancer in 64 patients who underwent neoadjuvant treatment followed by surgery. cN0, CCRT rather than radiotherapy alone, and radiological tumor downstaging are independent predictive factors for pCR in this cohort of patients. However, this study was limited by the small cohort size and its retrospective design. The identification of potential predictors for pCR will aid the selection of patients who will achieve pCR. Patients with non-response factors may receive local treatment instead of surgical intervention or to opt out of radical surgery. Further randomized studies for the identification of other potential predictive factors of pCR, including biological markers in rectal cancer, are warranted.
Conflict of interest statement
No potential conflicts of interest are disclosed.
1.Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015; 136: E359-86.
2.American Cancer Society. Cancer facts and figures 2016. Atlanta: American Cancer Society; 2016.
3.Mogoantă SS, Vasile I, Totolici B, Neamţu C, Streba L, Busuioc CJ, et al. Colorectal cancer-clinical and morphological aspects. Rom JMorphol Embryol. 2014; 55: 103-10.
4.Brenner H, Bouvier AM, Foschi R, Hackl M, Larsen IK, Lemmens V, et al. Progress in colorectal cancer survival in Europe from the late 1980s to the early 21st century: the EUROCARE study. Int J Cancer. 2012; 131: 1649-58.
5.Van De Velde CJH, Boelens PG, Borras JM, Coebergh JW, Cervantes A, Blomqvist L, et al. EURECCA colorectal: multidisciplinary management: European consensus conference colon & rectum. Eur J Cancer. 2014; 50: 1.e1-1.e34.
6.Carlson RW, Jonasch E. NCCN evidence blocks. J Natl Compr Canc Netw. 2016; 14: 616-9.
7.Swedish Rectal Cancer Trial. Improved survival with preoperative radiotherapy in resectable rectal cancer. N Engl J Med. 1997; 336: 980-7.
8.Den Dulk M, Krijnen P, Marijnen CA, Rutten HJ, Van De Poll-Franse LV, Putter H, et al. Improved overall survival for patients with rectal cancer since 1990: the effects of TME surgery and preoperative radiotherapy. Eur J Cancer. 2008; 44: 1710-6.
9.Ceelen W, Fierens K, Van Nieuwenhove Y, Pattyn P. Preoperative chemoradiation versus radiation alone for stage II and III resectable rectal cancer: a systematic review and meta-analysis. Int J Cancer. 2009; 124: 2966-72.
10.Braendengen M, Tveit KM, Berglund A, Birkemeyer E, Frykholm G, Påhlman L, et al. Randomized phase III study comparing preoperative radiotherapy with chemoradiotherapy in nonresectable rectal cancer. J Clin Oncol. 2008; 26: 3687-94.
11.Sauer R, Liersch T, Merkel S, Fietkau R, Hohenberger W, Hess C, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012; 30: 1926-33.
12.Martin ST, Heneghan HM, Winter DC. Systematic review and meta-analysis of outcomes following pathological complete response to neoadjuvant chemoradiotherapy for rectal cancer. Br J Surg. 2012; 99: 918-28.
13.Rouanet P. Réponse tumorale complète des cancers du rectum après traitement néoadjuvant: faut-il opérer? Point de vue du chirurgien Bull Cancer. 2011; 98: 25-9.
14.Moureau-Zabotto L, Farnault B, De Chaisemartin C, Esterni B, Lelong B, Viret F, et al. Predictive factors of tumor response after neoadjuvant chemoradiation for locally advanced rectal cancer. Int J Radiat Oncol Biol Phys. 2011; 80: 483-91.
15.National Institute of Public Health. Division of cancer epidemiology in Tunisia. Cancer Registry of north Tunisia. 2004-2006; Tunis: INSP, 2007.
16.Choi CH, Kim WD, Lee SJ, Park WY. Clinical predictive factors of pathologic tumor response after preoperative chemoradiotherapy in rectal cancer. Radiat Oncol J. 2012; 30: 99-107.
17.Dworak O, Keilholz L, Hoffmann A. Pathological features of rectal cancer after preoperative radiochemotherapy. Int J Colorectal Dis. 1997; 12: 19-23.
18.Das P, Skibber JM, Rodriguez-Bigas MA, Feig BW, Chang GJ, Wolff RA, et al. Predictors of tumor response and downstaging in patients who receive preoperative chemoradiation for rectal cancer. Cancer. 2007; 109: 1750-5.
19.Yoon SM, Kim DY, Kim TH, Jung KH, Chang HJ, Koom WS, et al. Clinical parameters predicting pathologic tumor response after preoperative chemoradiotherapy for rectal cancer. Int J Radiat Oncol Biol Phys. 2007; 69: 1167-72.
20.Moureau-Zabotto L, Farnault B, De Chaisemartin C, Esterni B, Lelong B, Viret F, et al. Predictive factors of tumor response after neoadjuvant chemoradiation for locally advanced rectal cancer. Int J Radiat Oncol Biol Phys. 2011; 80: 483-91.
21.Park JW, Lim SB, Kim DW, Jung KH, Hong YS, Chang HJ, et al. Carcinoembryonic antigen as predictor of pathologic response and a prognostic factor in locally advanced rectal cancer patients treated with preoperative chemoradiotherapy and surgery. Int J Radiat Oncol Biol Phys. 2009; 74: 810-7.
22.Van Gijn W, Marijnen CAM, Nagtegaal ID, Kranenbarg EMK, Putter H, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011; 12: 575-82.
23.Bosset JF, Collette L, Calais G, Mineur L, Maingon P, Radosevic-Jelic L, et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med. 2006; 355: 1114-23.
24.Gérard JP, Conroy T, Bonnetain F, Bouché O, Chapet O, Closon-Dejardin MT, et al. Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: results of FFCD 9203. J Clin Oncol. 2006; 24: 4620-5.
25.Gérard JP, Azria D, Gourgou-Bourgade S, Martel-Lafay I, Hennequin C, Etienne PL, et al. Clinical outcome of the ACCORD 12/0405 PRODIGE 2 randomized trial in rectal cancer. J Clin Oncol. 2012; 30: 4558-65.
26.Tournigand C, André T, Achille E, Lledo G, Flesh M, Mery-Mignard D, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol. 2004; 22: 229-37.
27.Chau I, Brown G, Cunningham D, Tait D, Wotherspoon A, Norman AR, et al. Neoadjuvant capecitabine and oxaliplatin followed by synchronous chemoradiation and total mesorectal excision in magnetic resonance imaging-defined poor-risk rectal cancer. J Clin Oncol. 2006; 24: 668-74.
28.Fernández-Martos C, Pericay C, Aparicio J, Salud A, Safont M, Massuti B, et al. Phase II, randomized study of concomitant chemoradiotherapy followed by surgery and adjuvant capecitabine plus oxaliplatin (CAPOX) compared with induction CAPOX followed by concomitant chemoradiotherapy and surgery in magnetic resonance imaging-defined, locally advanced rectal cancer: Grupo cáncer de recto 3 study. J Clin Oncol. 2010; 28:859-65.
29.Perez K, Safran H, Sikov W, Vrees M, Klipfel A, Shah N, et al. Complete neoadjuvant treatment for rectal cancer: the brown university oncology group CONTRE study. Am J Clin Oncol. 2014; 40: 283-7.
30.Schou JV, Larsen FO, Rasch L, Linnemann D, Langhoff J, Høgdall E, et al. Induction chemotherapy with capecitabine and oxaliplatin followed by chemoradiotherapy before total mesorectal excision in patients with locally advanced rectal cancer. Ann Oncol. 2012; 23: 2627-33.
31.Gollins S, Sebag-Montefiore D, Adams R, Saunders MP, Grieve R, Scott N, et al. A phase II single arm feasibility trial of neoadjuvant chemotherapy (NAC) with oxaliplatin/fluorouracil (OxMdG) then short-course preoperative radiotherapy (SCPRT) then immediate surgery in operable rectal cancer (ORC): COPERNICUS (NCT01263171). J Clin Oncol. 2015; 33: 3609
32.Lefevre JH, Mineur L, Kotti S, Rullier E, Rouanet P, de Chaisemartin C, et al. Effect of interval (7 or 11 weeks) between neoadjuvant radiochemotherapy and surgery on complete pathologic response in rectal cancer: A Multicenter, Randomized, Controlled Trial (GRECCAR-6). J Clin Oncol. 2016; 34: 3773-80.
Cite this article as: Letaief F, Nasri M, Ayadi M, Meddeb K, Mokrani A, Yahyaoui Y, et al. Potential predictive factors for pathologic complete response after the neoadjuvant treatment of rectal adenocarcinoma: a single center experience. Cancer Biol Med. 2017; 14: 327-34. doi: 10.20892/j.issn.2095-3941.2017.0037
e patients received conventional radiotherapy with a mean total dose of 45 Gy (ranging from 44 to 46 Gy). Of these patients, only 37% (n=24) had chemotherapyassociated radiotherapy. The patients received 5-fluorouracil (5FU)-based chemotherapy orally or via continuous infusion. Xeloda was administered 5 days a week for 5 weeks. LV5FU2 associated with 5FU and folinic acid was administered via continuous infusion for 46 h every 15 days during radiotherapy. The first cycle of FUFOL was administered from days 1 to 5 during the first week of radiotherapy. The second cycle of FUFOL was administered from days 29 to 33 during the fifth week of radiotherapy. Finally, FOLFOX 4 was administered via continuous infusion with LV5FU2 for 2 hours every 15 days during radiotherapy. Patients received surgical treatment 6 to 8 weeks after neoadjuvant treatment. Surgical intervention consisted of low anterior resection surgery or abdominoperineal resection surgery.
Meher Nasri
E-mail: mehernasri352@yahoo.fr
Received April 9, 2017; accepted May 23, 2017.
Available at www.cancerbiomed.org
Copyright © 2017 by Cancer Biology & Medicine
neoadjuvant RT or CCRT followed by radical surgery with total mesorectal excision (TME) between January 2006 and December 2011. The patients were classified into non-response (NR), partial response (PR), and pathologic complete response (pCR) based on the Dworak tumor regression grading system. Results: The median age of patients was 57 years (ranging from 22 to 85). A total of 24 patients were treated with neoadjuvant CCRT, whereas 40 patients were treated with RT alone. Abdominoperineal resection (APR) was performed on 29 patients (45%). Anterior resection with TME was performed on 34 patients (53%). One patient had local resection. Histologically, 12 (19%), 24 (73%), and 28 (44%) patients exhibited pCR, PR, and NR, respectively. Univariate analysis revealed that the predictors of tumor regression were as follows: the absence of lymph node involvement from initial imaging (cN0) (P=0.021); normal initial carcinoembryonic antigen (CEA) level (P=0.01); hemoglobin level ≥12 g/dl (P=0.009); CCRT (P=0.021); and tumor downstaging in imaging (P=0.001). Multivariate analysis showed that the main predictors of pCR were CT combined with neoadjuvant RT, cN0 stage, and tumor regression on imaging. Conclusions: Identifying the predictors of pCR following neoadjuvant therapy aids the selection of responsive patients for nonaggressive surgical treatment and possible surveillance.
 Cancer Biology & Medicine2017年3期
Cancer Biology & Medicine2017年3期
- Cancer Biology & Medicine的其它文章
- Survival after pulmonary metastasectomy in colorectal cancer patients: does a history of resected liver metastases worsen the prognosis? A literature review
- Expression levels of β-catenin and galectin-3 in meningioma and their effect on brain invasion and recurrence: a tissue microarray study
- Inhibition of IKK-NFκB pathway sensitizes lung cancer cell lines to radiation
- BsmI (rs1544410) and FokI (rs2228570) vitamin D receptor polymorphisms, smoking, and body mass index as risk factors of cutaneous malignant melanoma in northeast Italy
- Preclinical and clinical applications of specific molecular imaging for HER2-positive breast cancer
- Natural and artificial small RNAs: a promising avenue of nucleic acid therapeutics for cancer