
Chewing gum for postoperative ileus after colorectal surgery: A systematic review of overlapping meta-analyses
2017-08-12 00:02:19HuiZhngYongHongDengTingShuiGuoMinSong
Frontiers of Nursing 2017年2期
Hui Zhng,Yong-Hong Deng,Ting Shui,Guo-Min Song
aGraduate College,Tianjin University of Traditional Chinese Medicine,Tianjin 300193,China
bDepartment of Nursing,Tianjin Hospital,Tianjin 300211,China
Chewing gum for postoperative ileus after colorectal surgery: A systematic review of overlapping meta-analyses
Hui Zhanga,Yong-Hong Denga,Ting Shuaia,Guo-Min Songb,*
aGraduate College,Tianjin University of Traditional Chinese Medicine,Tianjin 300193,China
bDepartment of Nursing,Tianjin Hospital,Tianjin 300211,China
A R T I C L EI N F O
Article history:
18 February 2017
Accepted 21 April 2017
Available online 8 June 2017
Chewing gum
Colorectal surgery
Ileus
Meta-analysis
Jadad algorithm
Background:Many meta-analyses investigating gum chewing for postoperative recovery after colorectal surgery have been published with inconsistent fi ndings.Therefore,we performed this study to systematically review these overlapping meta-analyses and offer clinical recommendations based on the current best evidence for decision makers.
Methods:Multiple databases,including PubMed,EMBASE,Cochrane Library,Chinese BioMedical Literature on disc(CBMdisc),China National Knowledge Infrastructure(CNKI),Chinese Wanfang and Chinese VIP,were searched through October 2016.We included meta-analyses investigating the effectiveness of chewing gum for postoperative ileus after colorectal resection.Two investigators independently scanned and evaluated eligible meta-analyses,extracted essential information,assessed the methodological quality with the Assessment of Multiple Systematic Reviews(AMSTAR)tool and Oxford Levels of Evidence,and used the Jadad decision algorithm at each step for all procedures.Heterogeneity≤50%was accepted.
Results:Ten meta-analyses were included in our study.The AMSTAR scores varied from 5 to 9,with a median of 7.7.Most heterogeneity fell into the acceptable range.After implementing the Jadad decision algorithm,two meta-analyses of RCTs were selected based on search strategies and the implications of selection.The available best evidence indicated that gum chewing signi fi cantly reduced time to fi rst fl atus,time to fi rst bowel movement,time to fi rst bowel sounds and length of hospital stay.However, these two meta-analyses reached inconsistent conclusions as to the complications and economic bene fi ts.
Conclusions:With the current best available evidence,we suggest gum chewing is bene fi cial for gastrointestinal function and reducing postoperative ileus.
©2017 Shanxi Medical Periodical Press.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1.Introduction
Traditionally,physicians prohibit oral feeding until normal intestinal function returns after colorectal surgery.However,this procedure may result in postoperative ileus(POI),which can cause abdominal distension,abdominal pain,nausea,vomiting and delayed return of gastrointestinal motility.1These problems can delay postoperative recovery,prolong length of hospital stay(LOS) and increase fi nancial burden.2,3In the United States,postoperative ileus has been found to cost between$750 million and$1 billion annually.4Therefore,preventing or reducing POI after colorectal surgery is extremely important.
Many interventions and strategies,such as prokinetic agents and epidural anesthesia,have been used to manage POI.5-7However,these methods have a limited effect,and there is still a relatively high incidence of POI.As an alternative,gum chewing promotes the recovery of gastrointestinal peristalsis for postoperative patients without generating the side-effects associated with early feeding.However,several systematic,meta-analytic reviews have been published investigating chewing gum for postoperative recovery of gastrointestinal function after colorectal surgery,and the results are con fl icting.A uni fi ed and consistent conclusion has not yet been drawn,which creates an obstacle for informed decision-making.Thus,a systematic review of overlapping meta-analyses was executed to evaluate the effect of gum chewing for postoperative ileus.
The aims of this systematic review of all meta-analyses were to provide clinical suggestions and guide clinical workers in makingthe right decision based on the currently inconsistent available evidence.
2.Materials and methods
We relied on the Cochrane Handbook for Systematic Review of Interventions8and Preferred Reporting Items for Systematic Reviews and Meta-analysis(PRISMA)9to choose dependable and available systematic reviews and meta-analyses.All procedures were performed with Microsoft®Word(Microsoft Corporation, Redmond,Washington,USA).Due to the procedures being conductedwith previously published information,ethical approval and informed consent of the patients was not needed.
2.1.Literature search
All systematic reviews and meta-analyses comparing gum chewing to other groups of patients with postoperative ileus were included.Two investigators independently searched the PubMed, Cochrane Library,EMBASE,Chinese BioMedical Literature on disc (CBMdisc),China National Knowledge Infrastructure(CNKI),Chinese Wanfang and Chinese VIP databases up to October 2016.The search terms used were as follows:gum chewing,chewing gum, gum*,ileus,colectomy,colorectal surgery,systematic review and meta-analysis.A manual check of the reference lists was also conducted to identify other eligible studies.These searches were limited to publications in English and Chinese.The electronic supplementary material(ESM)was gathered to summarize all search information.
2.2.Selection criteria
The aim of implementing the systematic review of overlapping meta-analyses was to explain the inconsistent conclusions among meta-analyses evaluating gum chewing for patients with postoperative ileus.Therefore,letters to the editor,correspondence, meeting abstracts,meta-analyses excluding RCTs and systematic reviews without meta-analyses were not included in this study.
2.3.Selection of meta-analyses
Two investigators independently screened studies from all relevant meta-analyses according to the title and abstract of all the articles and checked the full-texts based on the selection criteria in the original checking stage.The discrepancies between the two investigators were settled by consulting a third investigator or discussion until an agreement was reached.
2.4.Information extraction
We assigned two investigators to independently extract the elementary information from eligible meta-analyses for our study. The data abstracted from the included meta-analyses included the fi rst author name,publication year,author state,electronic database,search time,search item,search restriction,and all outcomes of interest.Disagreements between the two investigators were settled by appealing to a third investigator.
2.5.Quality assessment
Two investigators were assigned to independently evaluate the search strategy of all eligible studies,including the publication language and status of the original research.Moreover,two investigators were also chosen to independently assess the methodological quality of each potential systematic review with a metaanalysis.ThemethodincludedtheAssessmentofMultiple Systematic Reviews(AMSTAR)Instrument and Oxford Levels of Evidence.10AMSTAR,with good reliability and validity,is a methodological quality assessment tool of systematic reviews and(or) meta-analyses.11-13Anydisagreementbetweenthetwoinvestigators was resolved by discussion.
2.6.Assessing heterogeneity
We abstracted information from all eligible research to assess heterogeneity.The purpose of a heterogeneity assessment is to discover whether the systematic reviewer appropriately and correctly used the heterogeneity assessment tool and whether they performed subgroup analysis or(and)sensitivity analysis.We de fi ned an I2of less than 50%as acceptable based on the judgment criteria in the Cochrane Handbook for Systematic Review of Interventions.8
2.7.Implementing the Jadad decision algorithm
The Jadad decision algorithm is a guideline for interpreting disagreement in systematic reviews within a meta-analysis.14When the expert experiences and results of trials are inconsistent,Jadad provides six reasons for the inconsistent systematic reviews within meta-analyses to help decision-makers(including researchers, policy-makers,clinical medical personnel,and patients)choose the best health care interventions.The six reasons included the speci fi c clinical question,de fi nite studyinclusionandexclusion criteria,data extraction,methodological quality assessment,ability to pool studies,and summary of the information.14Three investigators performed the Jadad decision algorithm to identify the reasons for the discordant meta-analyses until an agreement was reached.
3.Results
3.1.Search results and basic information on eligible meta-analyses
The literature search revealed 30 abstracts,and no additional sources were found.After using the speci fi ed study search terms,10 systematic reviews with meta-analyses4,15-23ful fi lled the inclusion and exclusion criteria and were selected for the study.We used the EndNote(version X7.1)literature management software to screen and manage the potential studies.These eligible meta-analyses were published between 2007 and 2016.Fig.1 summarizes the fl ow of selection and con fi rmation of references from the bibliography.Table 1 and Table 2,respectively,present the basic information on all of the studies included and number of original studies.1,24-59
3.2.Search methodology
To reduce the publication and time-lag bias,a comprehensive literature search was conducted.We evaluated the search methodology quality of all included studies.Every meta-analysis includedinthisstudysearchedtheMEDLINE,PubMedor Cochrane databases as part of the literature search.With the exception of two studies,19,22the others used the EMBASE database. However,there was a distinct variability in the use of other databases,including CINAHL,Scopus,CNKI,CBM,Wanfang,Web of Science and others.Table 3 describes the details of the searches. Five meta-analyses4,17,20,21,23did not impose language restrictions.
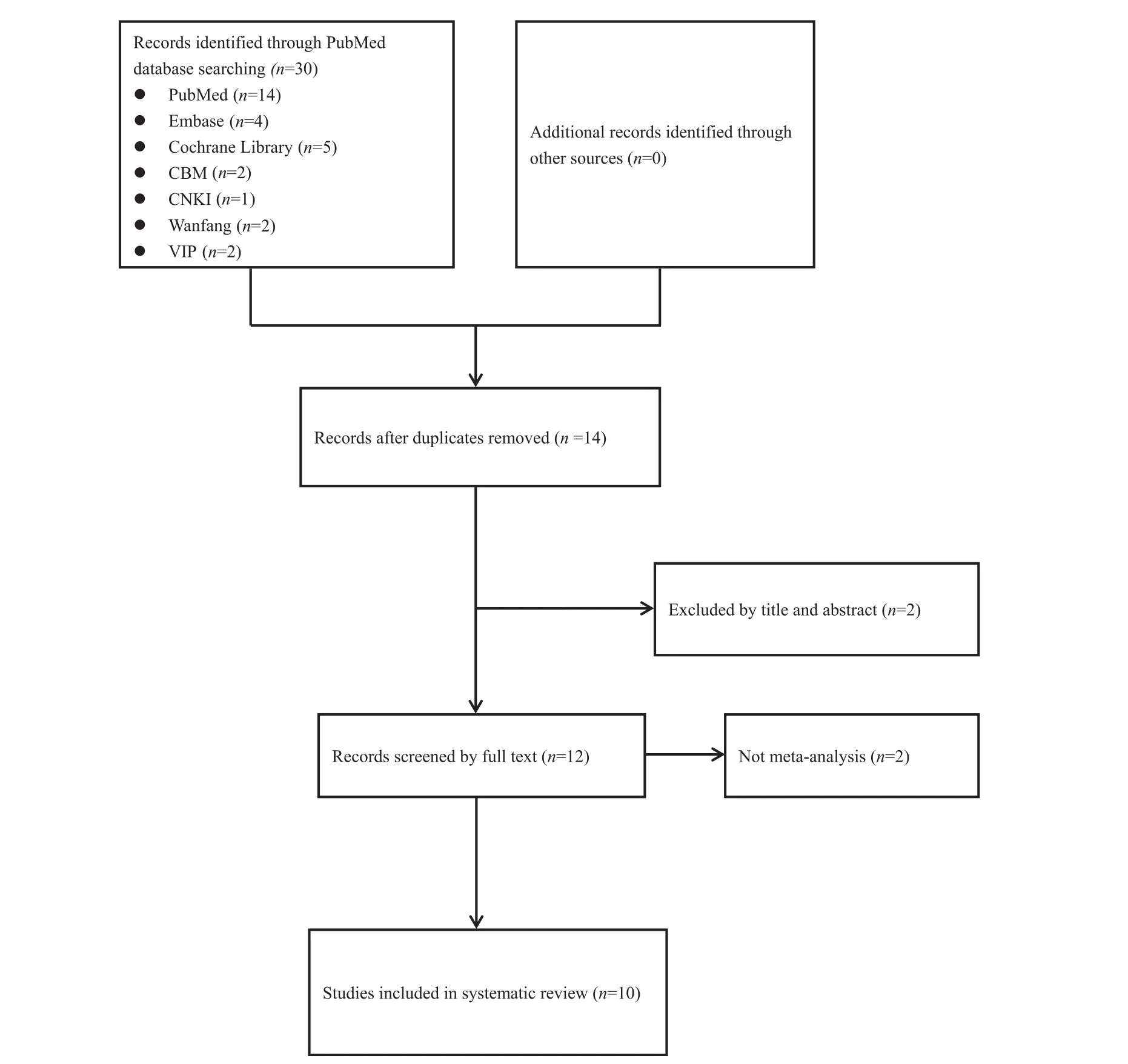
Fig.1.Flow diagram for the identi fi cation and selection of meta-analyses:30 potential records were initially screened.

Table 1 Basic information of each eligible meta-analysis.
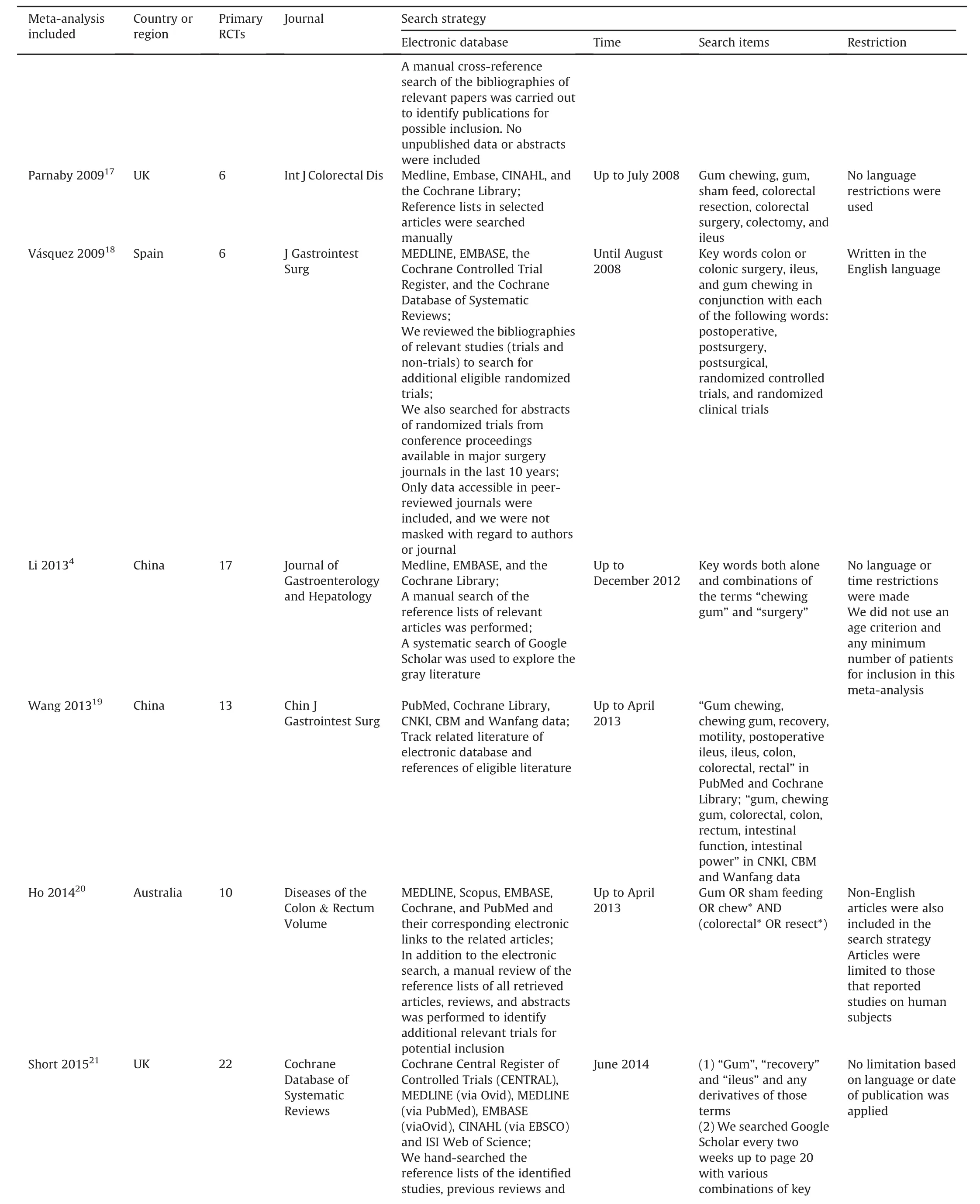
Table 1 (continued)
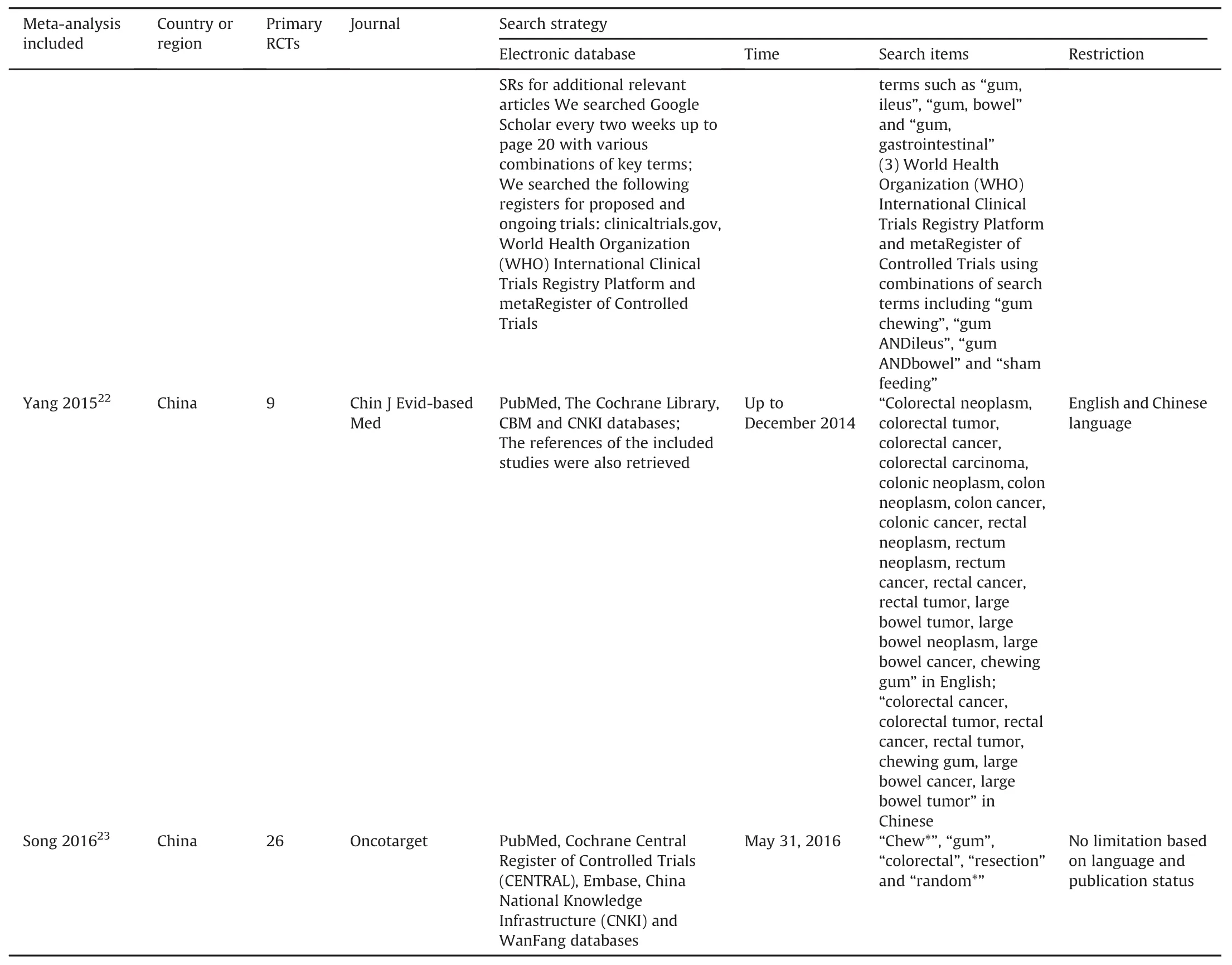
Table 1 (continued)
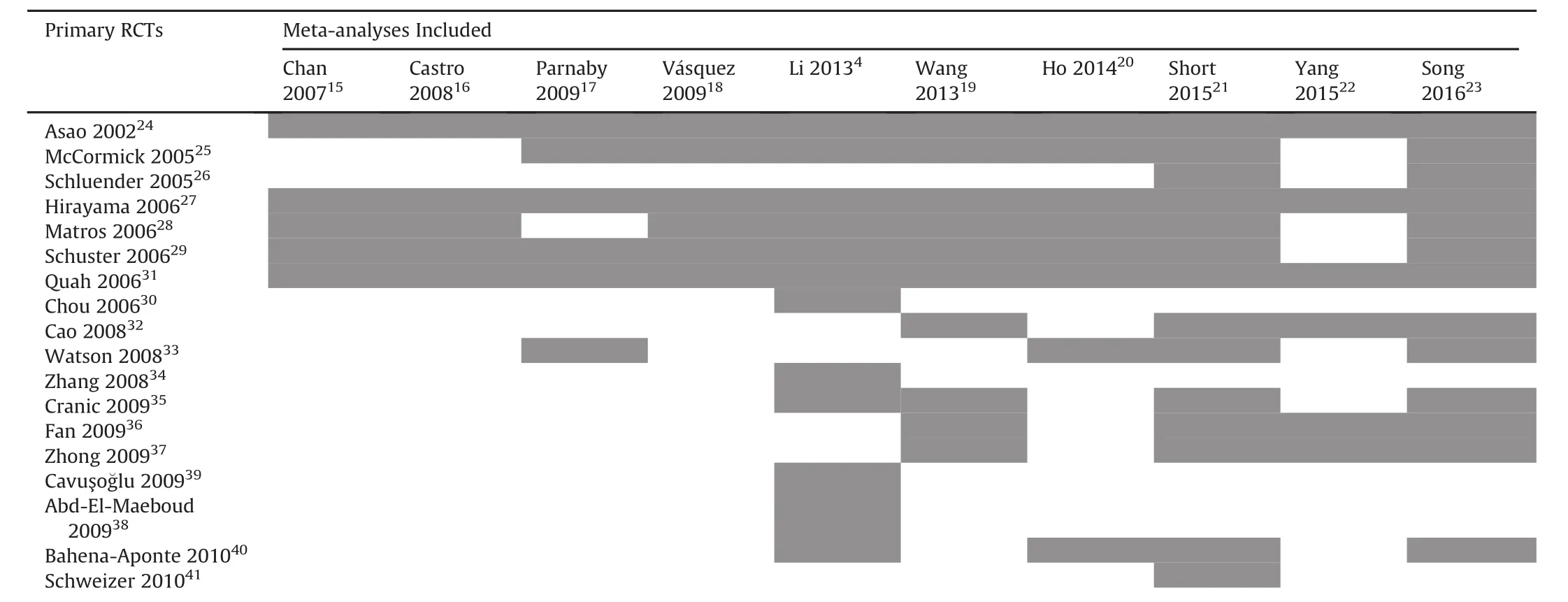
Table 2 Primary RCTs incorporated into each eligible meta-analysis.
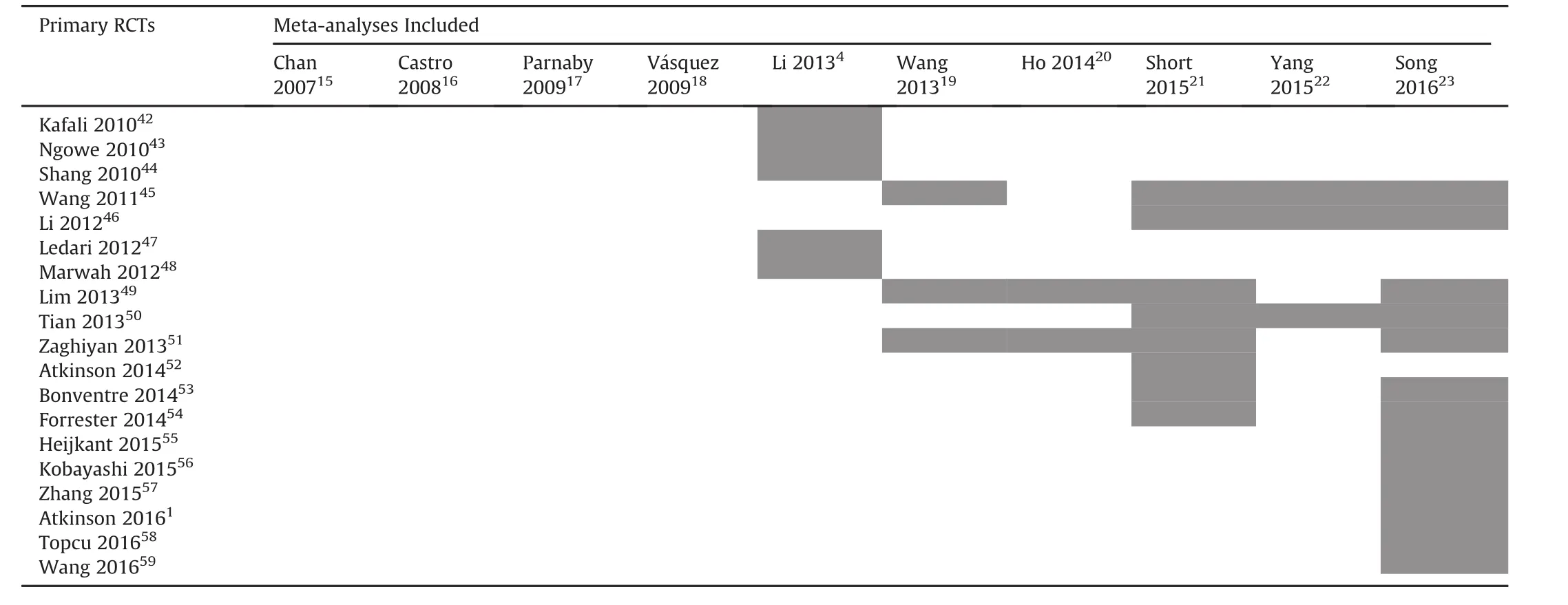
Table 2 (continued)
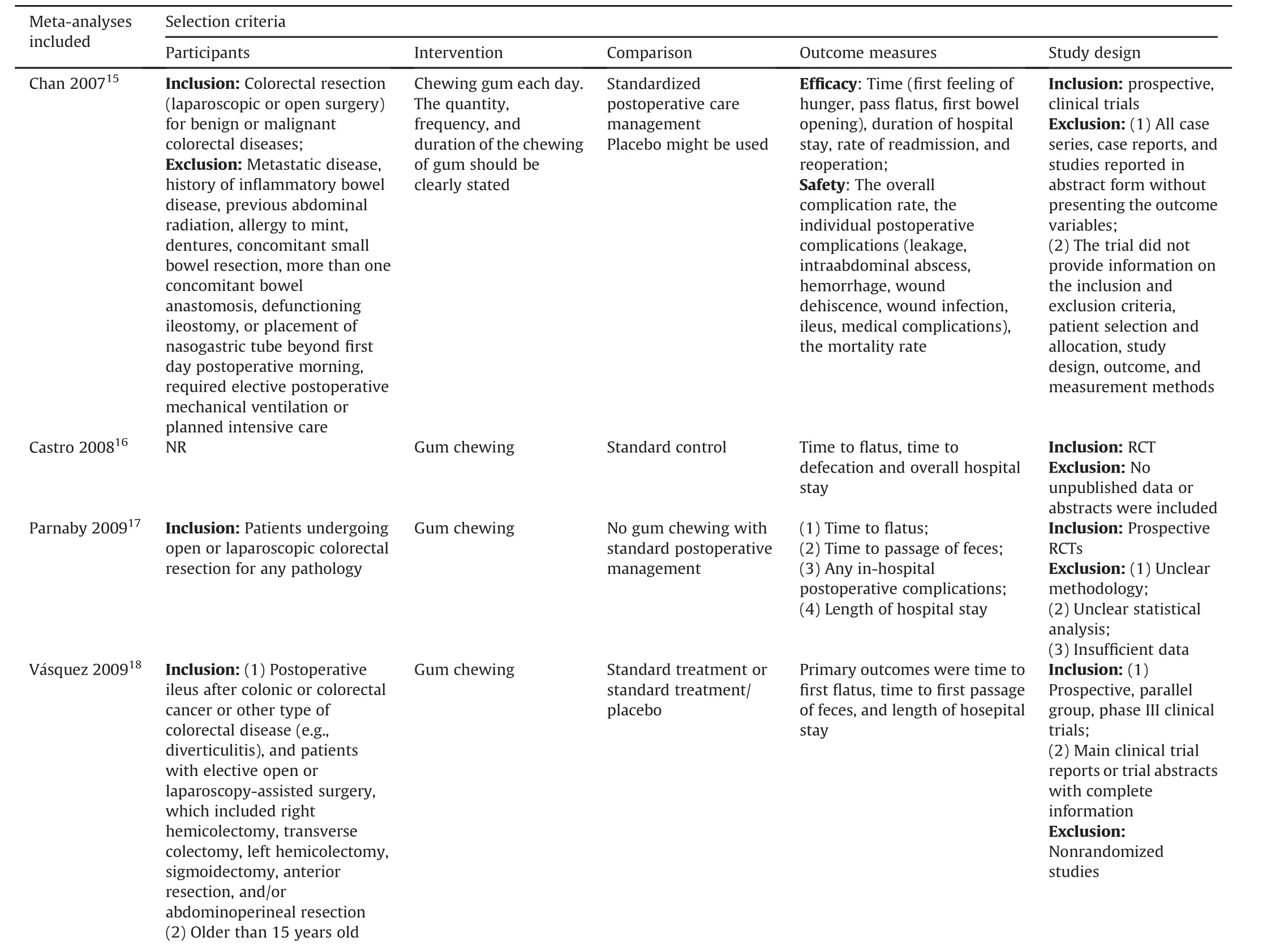
Table 3 Search methodology used by each meta-analysis.
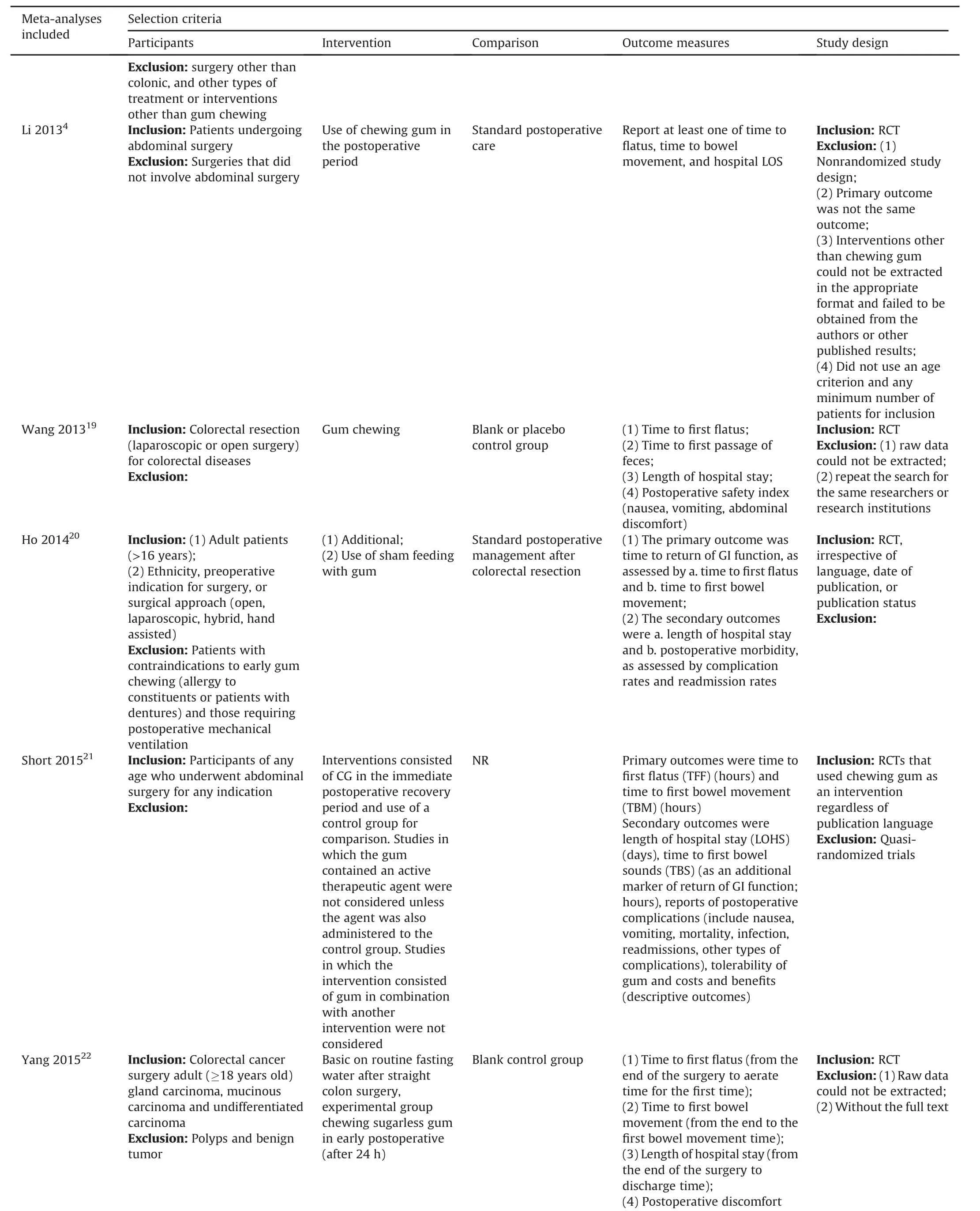
Table 3 (continued)
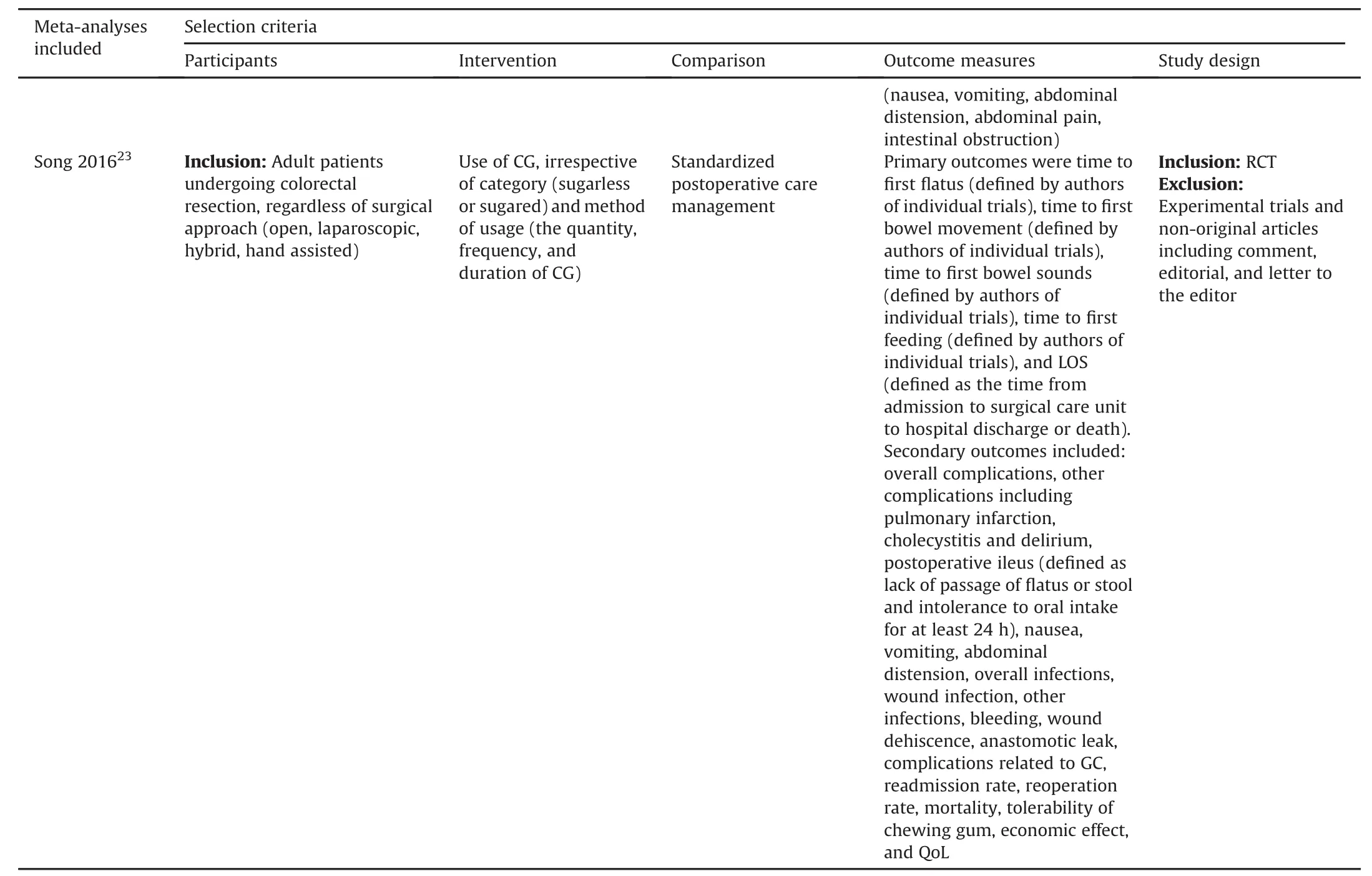
Table 3 (continued)
Three meta-analyses15,16,18limited the publication language to English.The remaining two meta-analyses19,22restricted the writtenlanguagetoEnglishandChinese.Threemeta-analyses15,16,20were limited to human subjects.
3.3.Methodological quality
High quality research is generated from reliable evidence and standard reporting.The Oxford Levels of Evidence10and AMSTAR12tools were used to assess and rate the evidence and methodological quality,respectively,of all of the included meta-analyses.
Based on the Oxford Levels of Evidence,all of the meta-analyses included provided Level II evidence.Most of the meta-analyses15,16,18,19,21-23were performed with Review Manager statistical software to pool data.The meta-analysis conducted by Chan and colleagues15also followed the Quality of Reporting of Meta-analysis (QUOROM)guidelines.Only one meta-analysis17was implemented usingtheComprehensiveMeta-analysis(Biostat,Engelwood,CA,USA) software package.Two meta-analyses4,20used the STATA statistical software.Subgroup and sensitivity analyses were used in four and three meta-analyses,respectively.Table 4 and Table 5,respectively, show the methodology quality and AMSTAR data for each study included.The AMSTAR scores varied from 5 to 9,with a median of 7.7.
3.4.Assessing heterogeneity
Several methods were used to assess the heterogeneity of each meta-analysis,and all 10 studies used a statistical heterogeneity analysis.
In Table 6,we summarized the heterogeneity level,subgroup analysis and sensitivity analysis for each study.The heterogeneity of most outcomes(≤50%)was in the acceptable range used by the Cochrane Collaboration.8
3.5.Results of Jadad decision algorithm
Table 7 lists the outcomes of all of the eligible meta-analyses. The Jadad decision algorithm was executed to con fi rm which of the 10 meta-analyses that provided the currently best available evidence to develop clinical treatment recommendations.Three authors(S.T,Z.H and X.T)independently elected the same route for the Jadad decision algorithm.Because(1)all of the meta-analyses addressed the same question,(2)none of the meta-analyses included the same primary trials,and(3)the reviewed studies did not restrict the same selection criteria,the Jadad decision algorithm recommends that the highest-quality studies can be elected based on the different criteria,including the methodologic quality,language of publication,publication status and availability of data on individual patients in the primary trials.The last criterion did not apply to our study.After application of the aforementioned criteria,we ultimately selected two meta-analyses written by Short et al21and Song et al23(Fig.2).
The two meta-analyses both concluded that gum chewing signi fi cantly reduced time to fi rst fl atus,time to fi rst bowel movement,time to fi rst bowel sounds and length of hospital stay.Song et al23also found no signi fi cant difference in time to fi rst feeding between the gum chewing group and control group.However,these twometa-analysesreachedinconsistentconclusionsoncomplications and economic bene fi ts.Short et al21reported that there were little differences in mortality,infection risk,readmission rate or cost.The patients tolerated the chewing gum well.Song et al23found that there were no signi fi cant differences between the groups in overall complications,nausea,vomiting,bloating,wound infection,bleeding,dehiscence,readmission,reoperation,or mortality.The gum chewing group had a lower risk of postoperative ileus as well as a lower net bene fi t and quality of life.
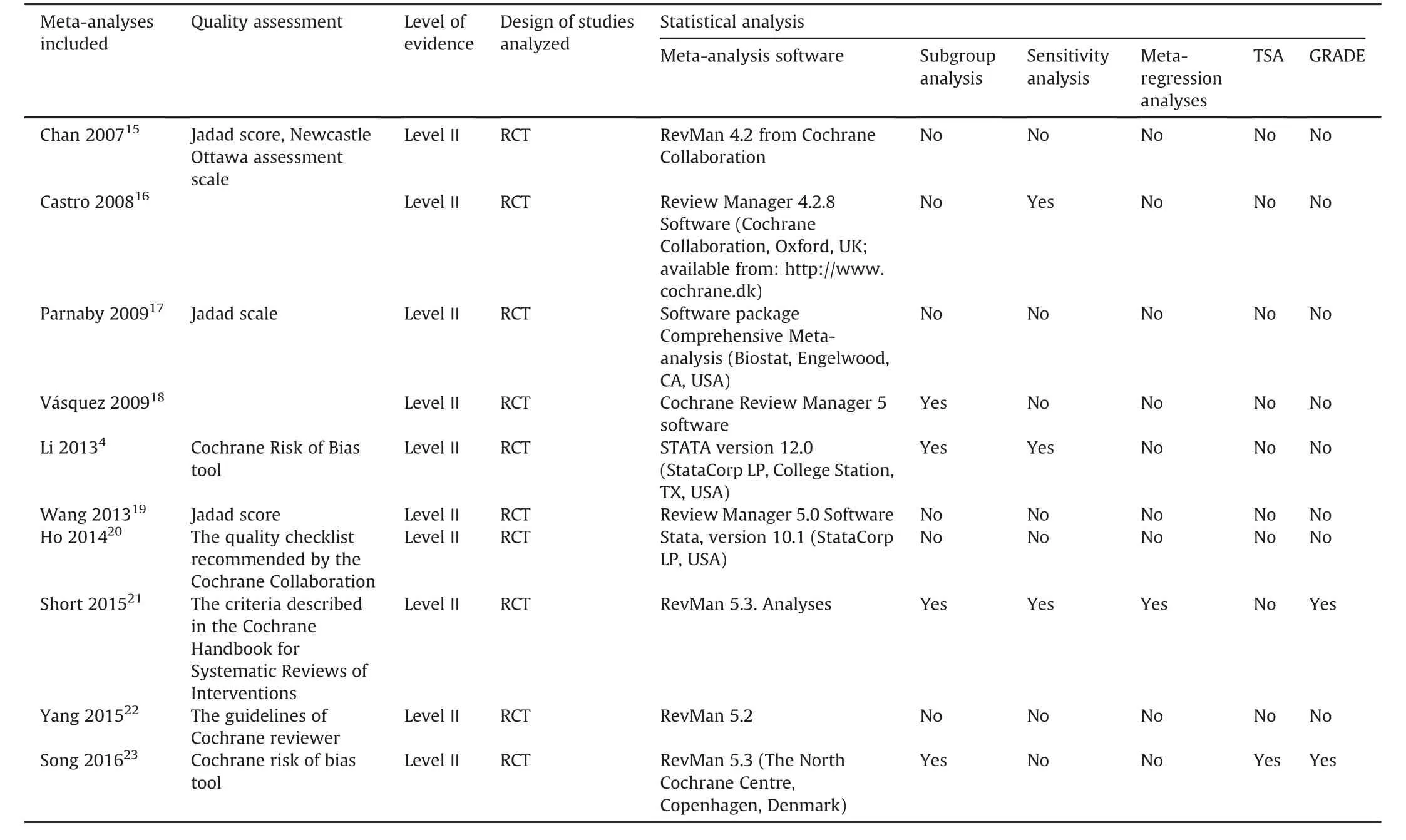
Table 4 Methodological information for each included study.
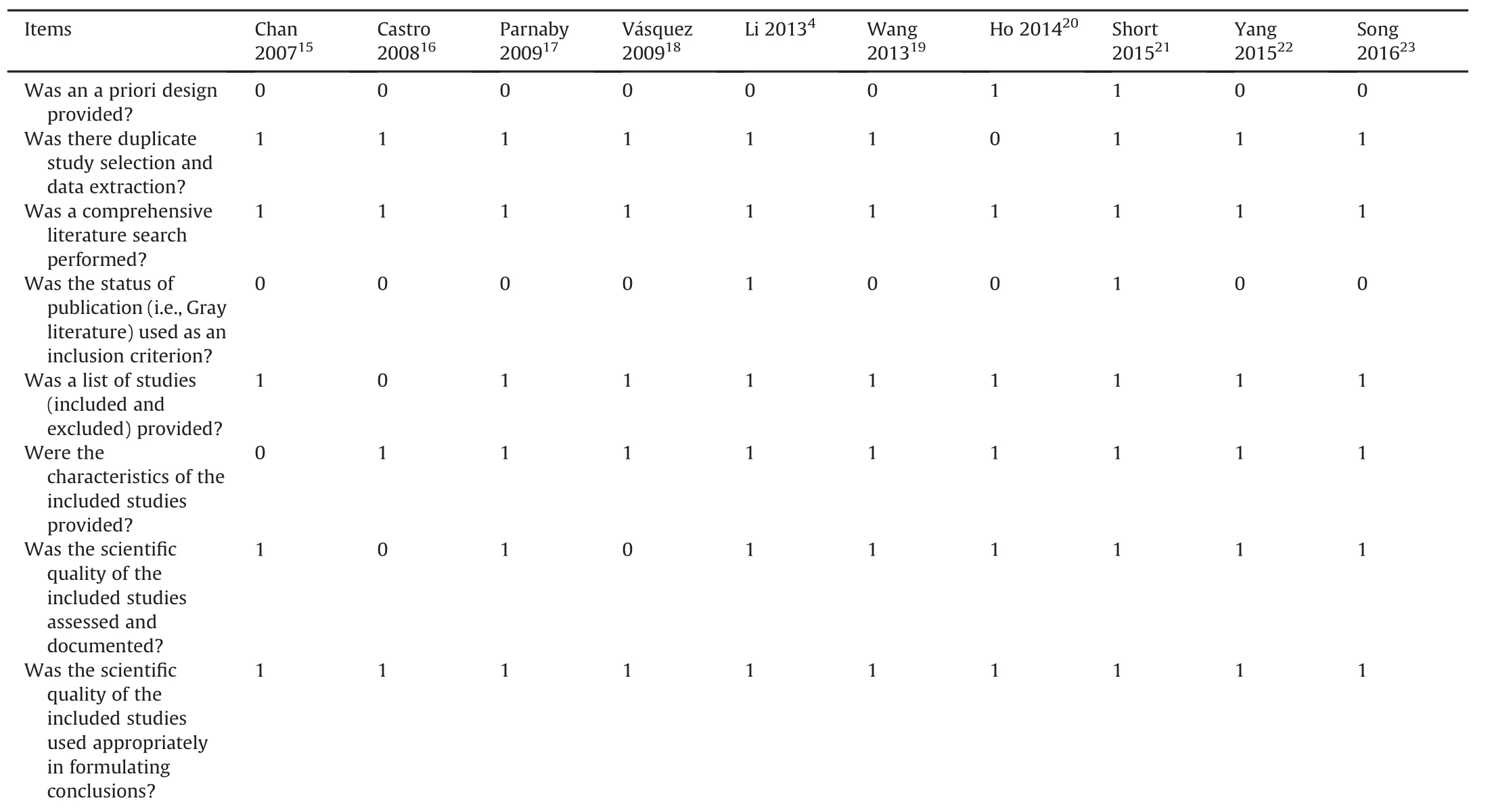
Table 5 AMSTAR criteria for each included study.
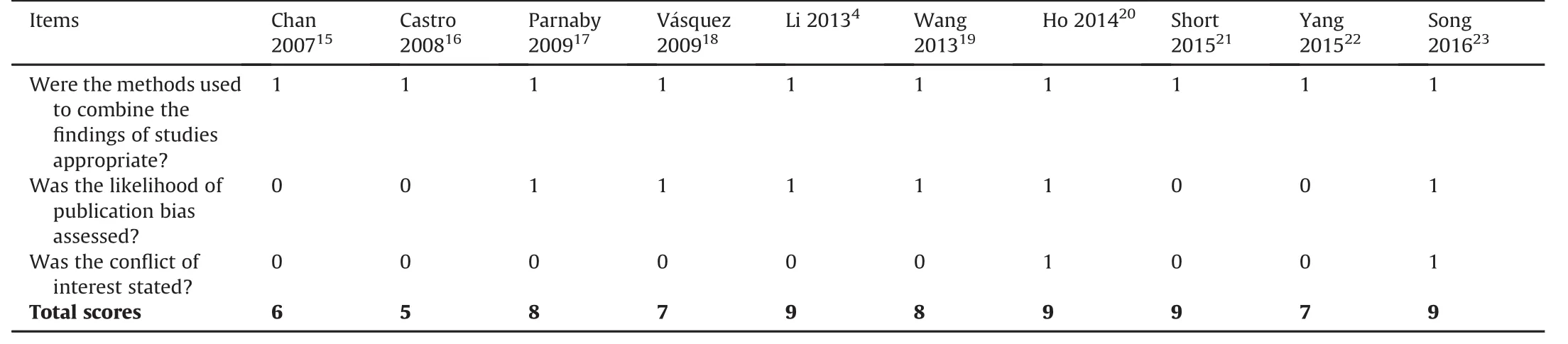
Table 5 (continued)
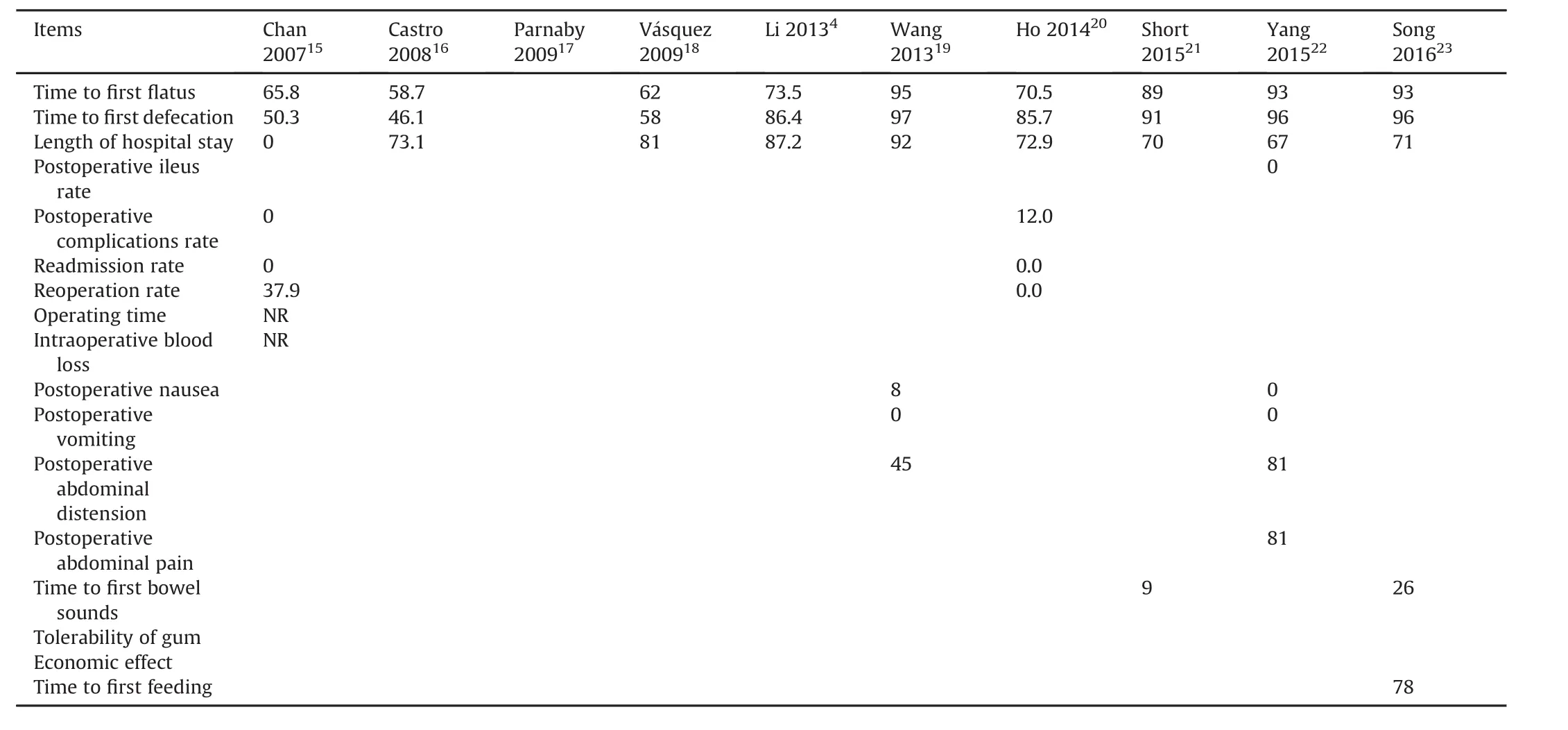
Table 6 I2statistical value of each outcome,subgroup and sensitivity analysis(%).
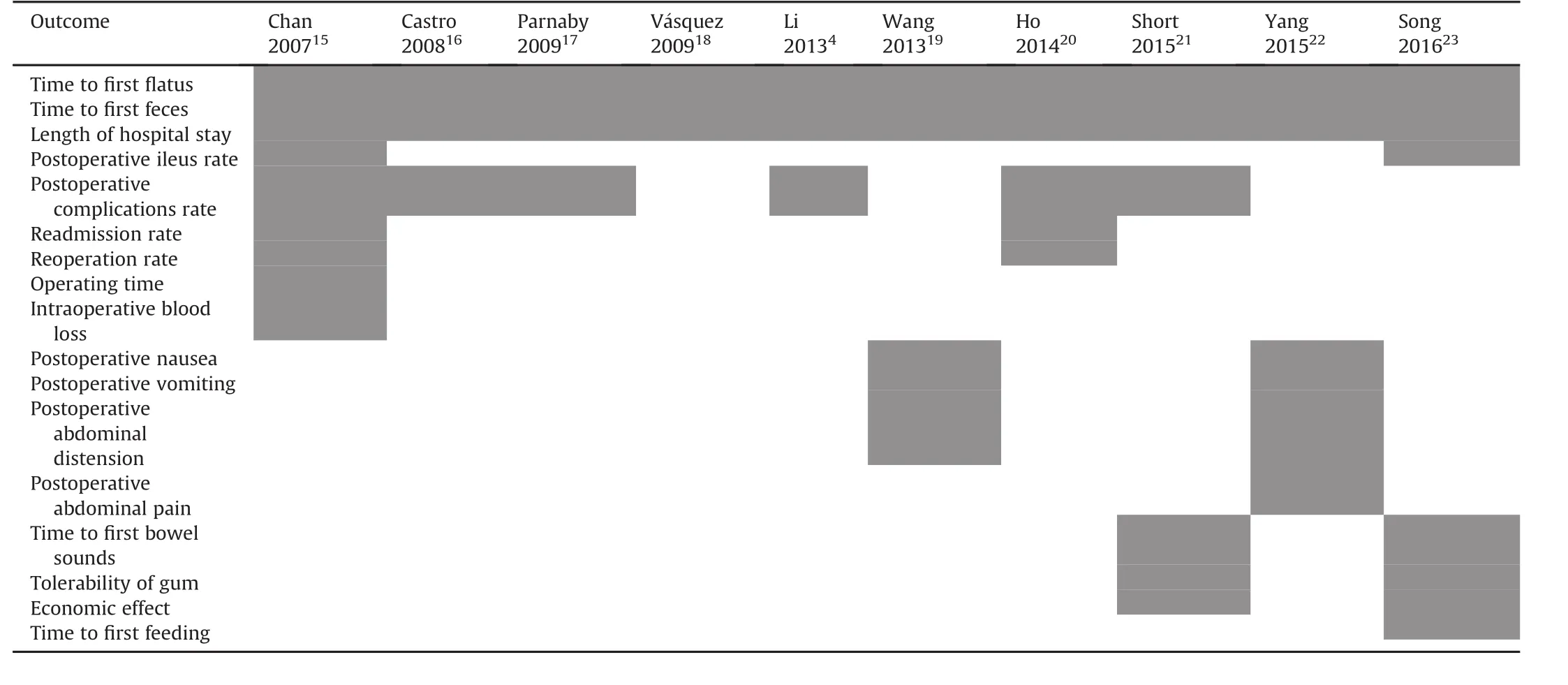
Table 7 Results of all outcome measures reported in eligible meta-analyses.
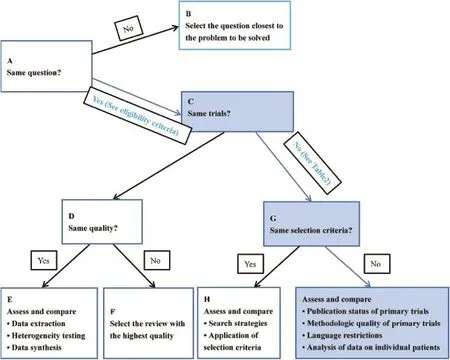
Fig.2.Flow diagram of the Jadad decision algorithm.
4.Discussion
Systematic reviews or meta-analyses including all available original trials were considered to be the best available evidence sources.60Decision makers,including policy makers,researchers and clinical workers,usually develop a systematic review with meta-analysis to provide recommendations for informed decisionmaking and to resolve complex clinical problems.Although there are numerous systematic reviews and meta-analyses on this topic, these reviews are inconsistent,and we thus attempted to determinewhich of these researchstudies provided the best evidence on this topic.
For the purpose of providing high qualityclinical evidence,Jadad and colleagues developed a method to con fi rm all possible sources that caused con fl ict among meta-analyses in 1997.The sources included the clinical question for the population of patients,interventions,outcome measures,settings and selection criteria(inclusion criteria and exclusion criteria),use of the selection criteria, literature search strategies,data abstraction,end points,human error(random or systematic),study quality assessment,quality assessment interpretations and methods of quality assessments in reviews,ability to combine studies through clinical criteria and statistical methods,and statistical methods for data analysis.14
After implementing the Jadad algorithm,two meta-analyses completed by Short et al21and Song et al23were selected to provide clinical treatment recommendations on the effect of chewing gum after colorectal resection for postoperative ileus based on the current best available evidence to promote decisionmaking in a clinical context.Short and colleagues21demonstrated that there was statistical evidence that the use of gum chewing reduced time to fi rst fl atus,time to fi rst defecation,time to bowel sounds and length of hospital stay.All patients tolerated the chewing gum well.However,there was little difference in infection risk,mortality,readmission rate and cost between the two groups.Some studies included in the meta-analysis found that gum chewing reduced nausea,vomiting and other complications. Due to the current research focus on small,poor quality trials and the target of postoperative ileus,the bene fi ts of gum chewing may be reduced.Therefore,the author suggested that larger and better quality RCTs are needed to improve the evidence on the use of gum chewing after surgery.The meta-analysis conducted by Song et al23also suggested that gum chewing can shorten time to fi rst fl atus,bowel sounds,and length of hospital stay and lower risk of postoperative ileus.Gum chewing was well tolerated by all patients.However,there were no signi fi cant differences in nausea,vomiting,wound infection,bloating,bleeding,dehiscence,overall complications,readmission,reoperation or mortality between the groups.The study found a lower net bene fi t and quality of life in the gum chewing group.Hence,the author suggested that gum chewing is conducive to enhance the return of intestinal function after colorectal resection and may decrease theriskofpostoperativeileus.However,theauthorsacknowledged several limitations in their meta-analysis.For example,most trials were rated as providing low quality evidence on risk of bias,which may lead to a misidenti fi cation of the effect of chewing gum.
We conducted this systematic review of overlapping metaanalyses,but some limitations may impact the power of our fi ndings.First,although we performed a comprehensive literature search to gather the potentially eligible meta-analyses,additional studies on the topic may be located if the search databases were extended.Second,to generate the highest level of evidence,we only selected meta-analyses that included RCTs.However,the level of overall evidence was low.
5.Conclusions
With the current best available evidence,we suggest that implementation of gum chewing as bene fi cial for gastrointestinal function and for reducing postoperative ileus.However,more studies should be completed to determine the safety of using gum chewing.
Con fl icts of interest
All contributing authors declare no con fl icts of interest.
1.Atkinson C,Penfold CM,Ness AR,et al.Randomized clinical trial of postoperative chewing gum versus standard care after colorectal resection.Br J Surg.2016;103:962-970.
2.Iyer S,Saunders WB,Stemkowski S.Economic burden of postoperative ileus associated with colectomy in the United States.J Manag Care Pharm.2009;15: 485-494.
3.Boeckxstaens GE,de Jonge WJ.Neuroimmune mechanisms in postoperative ileus.Gut.2009;58:1300-1311.
4.Li S,Liu Y,Peng Q,Xie L,Wang J,Qin X.Chewing gum reduces postoperative ileusfollowingabdominalsurgery:ameta-analysisof17randomized controlled trials.J Gastroenterol Hepatol.2013;28:1122-1132.
5.Barletta JF,Senagore AJ.Reducing the burden of postoperative ileus:evaluating andimplementinganevidence-basedstrategy.WorldJSurg.2014;38: 1966-1977.
6.Choi H,Kang SH,Yoon DK,et al.Chewing gum has a stimulatory effect on bowel motility in patients after open or robotic radical cystectomy for bladder cancer:a prospective randomized comparative study.Urology.2011;77: 884-890.
7.Asgeirsson T,El-Badawi KI,Mahmood A,Barletta J,Luchtefeld M,Senagore AJ. Postoperative ileus:it costs more than you expect.J Am Coll Surg.2010;210: 228-231.
8.Higgins J,Green S.Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0.The Cochrane Collaboration;2011[updated March 2011].
9.Moher D,Liberati A,Tetzlaff J,Altman DG,PRISMA Group.Preferred reporting items for systematic reviews and meta-analyses:the PRISMA Statement.Open Med.2009;3:e123-e130.
10.Slobogean G,Bhandari M.Introducing levels of evidence to the Journal of Orthopaedic Trauma:implementation and future directions.J Orthop Trauma. 2012;26:127-128.
11.Shea BJ,Bouter LM,Peterson J,et al.External validation of a measurement tool to assess systematic reviews(AMSTAR).PLoS One.2007;2:e1350.
12.Shea BJ,Grimshaw JM,Wells GA,et al.Development of AMSTAR:a measurement tool to assess the methodological quality of systematic reviews.BMC Med Res Methodol.2007;7:10.
13.Shea BJ,Hamel C,Wells GA,et al.AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews.J Clin Epidemiol. 2009;62:1013-1020.
14.Jadad AR,Cook DJ,Browman GP.A guide to interpreting discordant systematic reviews.CMAJ.1997;156:1411-1416.
15.Chan MK,Law WL.Use of chewing gum in reducing postoperative ileus after elective colorectal resection:a systematic review.Dis Colon Rectum.2007;50: 2149-2157.
16.de Castro SM,van den Esschert JW,van Heek NT,et al.A systematic review of the ef fi cacy of gum chewing for the amelioration of postoperative ileus.Dig Surg.2008;25:39-45.
17.Parnaby CN,MacDonald AJ,Jenkins JT.Sham feed or sham?A meta-analysis of randomized clinical trials assessing the effect of gum chewing on gut function after elective colorectal surgery.Int J Colorectal Dis.2009;24:585-592.
18.V′asquez W,Hern′andez AV,Garcia-Sabrido JL.Is gum chewing useful for ileus after elective colorectal surgery?A systematic review and meta-analysis of randomized clinical trials.J Gastrointest Surg.2009;13:649-656.
19.Wang XJ,Chi P.Chewing gum to promote colorectal disease after intestinal function recovery:a systematic review and meta-analysis.Chin J Gastrointest Surg.2013;16:1078-1083(in Chinese).
20.Ho YM,Smith SR,Pockney P,Lim P,Attia J.A meta-analysis on the effect of sham feeding following colectomy:should gum chewing be included in enhanced recovery after surgery protocols?Dis Colon Rectum.2014;57: 115-126.
21.Short V,Herbert G,Perry R,et al.Chewing gum for postoperative recovery of gastrointestinal function.Cochrane Database Syst Rev.2015;2,CD006506.
22.Yang XM,Zhang ZX,Tan XY,Yang AL,Tian JH,Zhang QX.Effect of early postoperative chewing gum on the recovery of gastrointestinal function after colorectal cancer surgery:a systematic review and meta-analysis.Chin J Evid Based Med.2015;5:542-549(in Chinese).
23.Song GM,Deng YH,Jin YH,Zhou JG,Tian X.Meta-analysis comparing chewing gum versus standard postoperative care after colorectal resection.Oncotarget. 2016;7:70066-70079.
24.Asao T,Kuwano H,Nakamura J,Morinaga N,Hirayama I,Ide M.Gum chewing enhances early recovery from postoperative ileus after laparoscopic colectomy. J Am Coll Surg.2002;195:30-32.
25.McCormick JT,Garvin R,Caushaj P,et al.The effects of gum-chewing on bowel function and hospital stay after laparoscopic vs open colectomy:a multiinstitution prospective randomized trial.J Am Coll Surg.2005;201:S66-S67.
26.Schluender SS,Gurland BHG,Divino CD,et al.Gum chewing does not enhance the return of bowel function in patients undergoing elective colon resection in a randomized blinded pilot study.Colorectal Dis.2005;7(suppl 1):92.
27.Hirayama I,Suzuki M,Ide M,Asao T,Kuwano H.Gum-chewing stimulates bowel motility after surgery for colorectal cancer.Hepatogastroenterology. 2006;53:206-208.
28.Matros E,Rocha F,Zinner M,et al.Does gum chewing ameliorate postoperative ileus?Results of a prospective,randomized,placebo-controlled trial.J Am Coll Surg.2006;202:773-778.
29.Schuster R,Grewal N,Greaney GC,Waxman K.Gum chewing reduces ileus after elective open sigmoid colectomy.Arch Surg.2006;141:174-176.
30.Chou SJ,Lin CH,Hsieh HF,Yu JC,Chen TW,Chan DC.Gum chewing in patients with subtotal gastrectomy.Chir Gastroenterol.2006;22:269-271.
31.Quah HM,Samad A,Neathey AJ,Hay DJ,Maw A.Does gum chewing reduce postoperative ileus following open colectomy for left-sided colon and rectal cancer?A prospective randomized controlled trial.Colorectal Dis.2006;8: 64-70.
32.Cao R,Chen Y,Chen H,Zhu X,Kang Z.Colorectal cancer patients chewing gum on intestinal function.Today Nurse.2008;11:45-46(in Chinese).
33.Watson H,Grif fi ths P,Lamaparelli M,Watson M.Does chewing(gum)aid recovery after bowel resection?A randomized controlled trial(RCT).Colorectal Dis.2008;10:6.
34.Zhang Q,Zhao P.In fl uence of gum chewing on return of gastrointestinal function after gastric abdominal surgery in children.Eur J Pediatr Surg. 2008;18:44-46.
35.Crainic C,Erickson K,Gardner J,et al.Comparison of methods to facilitate postoperative bowel function.Medsurg Nurs.2009;18:235-238.
36.Fan Q,Geng X,Chen H,Yu J,Hu M,Yi J.Effects of chewing gum on recovery of gastrointestinal motility in patients undergoing total resection of colorectal cancer.Med J Natl Defending Forces Southwest China.2009;19:1240-1241(in Chinese).
37.Zhong Z,Ye F,Lin J.A study on how chewing action promotes gastrointestinal functions recovery after colorectal cancer surgery.Chin J Gastrointest Surg. 2009;12:632-633(in Chinese).
38.Abd-El-Maeboud KH,Ibrahim MI,Shalaby DA,Fikry MF.Gum chewing stimulates early return of bowel motility after caesarean section.BJOG.2009;116: 1334-1339.
39.Cavus¸oˇglu YH,Azili MN,Karaman A,et al.Does gum chewing reduce postoperative ileus after intestinal resection in children?A prospective randomized controlled trial.Eur J Pediatr Surg.2009;19:171-173.
40.Bahena-Aponte JA,C′ardenas-Lailson E,Ch′avez-Tapia N,Flores-Gama F.Usefulness of chewing gum for the resolution of postoperative ileus in left colon resections.Rev Gastroenterol Mex.2010;75:369-373(in Spanish).
41.Schweizer W,H¨ane R.Sham-feeding of patients with chewing gum after abdominal operations.Br J Surg.2010;97:8.
42.Kafali H,Duvan CI,G¨ozdemir E,Simavli S,Onaran Y,Keskin E.In fl uence of gum chewing on postoperative bowel activity after cesarean section.Gynecol Obstet Invest.2010;69:84-87.
43.Ngowe MN,Eyenga VC,Kengne BH,Bahebeck J,Sosso AM.Chewing gum reduces postoperative ileus after open appendectomy.Acta Chir Belg.2010;110: 195-199.
44.Shang H,Yang Y,Tong X,Zhang L,Fang A,Hong L.Gum chewing slightly enhances early recovery from postoperative ileus after cesarean section:results of a prospective,randomized,controlled trial.Am J Perinatol.2010;27:387-391.
45.Wang S,Hou Y,Dong S.A randomized controlled trial of chewing gum to promote postoperative bowel recovery for patients with rectal cancer.Sichuan Med J.2011;32:1956-1958(in Chinese).
46.Li Y.Chewing gum on the impact of early postoperative gastrointestinal function in patients with colon cancer.World Health Dig.2012;41:69-70(in Chinese).
47.Ledari FM,Barat S,Delavar MA.Chewing gums has stimulatory effects on bowel function in patients undergoing cesarean section:a randomized controlled trial.Bosn Bosn J Basic Med Sci.2012;12:265-268.
48.Marwah S,Singla S,Tinna P.Role of gum chewing on the duration of postoperative ileus following ileostomy closure done for typhoid ileal perforation: a prospective randomized trial.Saudi J Gastroenterol.2012;18:111-117.
49.Lim P,Morris OJ,Nolan G,Moore S,Draganic B,Smith SR.Sham feeding with chewing gum after elective colorectal resectional surgery:a randomized clinical trial.Ann Surg.2013;257:1016-1024.
50.Tian M.Effect of chewing gums on gastrointestinal function of rectal cancer patients undergoing surgical operations.Mod Clin Nurs.2013;12:45-47(in Chinese).
51.Zaghiyan K,Felder S,Ovsepyan G,et al.A prospective randomized controlled trial of sugared chewing gum on gastrointestinal recovery after major colorectal surgery in patients managed with early enteral feeding.Dis Colon Rectum.2013;56:328-335.
52.Atkinson C,Penfold C,Ness A,et al.A randomised trial of chewing gum to reduce post-operative ileus.Clin Nutr.2014;33:S260.
53.Bonventre S,Inviati A,Di Paola V,et al.Evaluating the ef fi cacy of current treatments for reducing postoperative ileus:a randomized clinical trial in a single center.Minerva Chir.2014;69:47-55.
54.Forrester DA,Doyle-Munoz J,McTigue T,D'Andrea S,Natale-Ryan A.The ef ficacy of gum chewing in reducing postoperative ileus:a multisite randomized controlled trial.J Wound Ostomy Continence Nurs.2014;41:1-6.
55.van den Heijkant TC,Costes LM,van der Lee DG,et al.Randomized clinical trial of the effect of gum chewing on postoperative ileus and in fl ammation in colorectal surgery.Br J Surg.2015;102:202-211.
56.Kobayashi T,Masaki T,Kogawa K,Matsuoka H,Sugiyama M.Ef fi cacy of gum chewing on bowel movement after open colectomy for left-sided colorectal cancer:a randomized clinical trial.Dis Colon Rectum.2015;58: 1058-1063.
57.Zhang XX,Peng F,Yuan XJ.Effect of chewing gum on return of gastrointestinal function after colorectal surgery.Nurs Pract Res.2015;12:51-52(in Chinese).
58.Topcu SY,Oztekin SD.Effect of gum chewing on reducing postoperative ileus and recovery after colorectal surgery:a randomised controlled trial.Complement Ther Clin Pract.2016;23:21-25.
59.Wang XL,Ni JX.Effect of chewing gum on intestinal function recovery in colorectal cancer patients undergoing surgery.J Qiqihar Univ Med.2016;37: 674-675(in Chinese).
60.Young D.Policymakers,experts review evidence-based medicine.Am J Health Syst Pharm.2005;62:342-343.
How to cite this article:Zhang H,Deng Y-H,Shuai T,et al. Chewing gum for postoperative ileus after colorectal surgery: A systematic reviewof overlapping meta-analyses.Chin Nurs Res. 2017;4:92-104.http://dx.doi.org/10.1016/j.cnre.2017.02.001
6 December 2016
*Corresponding author.
E-mail address:songguomin134@163.com(G.-M.Song).
Peer review under responsibility of Shanxi Medical Periodical Press.
in revised form
- Frontiers of Nursing的其它文章
- Transitional care interventions to reduce readmission in patients with chronic obstructive pulmonary disease:A meta-analysis of randomized controlled trials
- A bibliometric study of the Journal of School Health:1965-2014☆
- In fl uence of mobile education on joint function and quality of life in patients after total hip arthroplasty☆
- Development of a frailty scale for elderly people in China☆
- How to establish an expected animal model of post-traumatic osteoarthritis?
- Retraction notice to“Relationships between perceived social support and retention patients receiving methadone maintenance treatment in China mainland”[CNR 3/1(2016)11-15]