
Development of a frailty scale for elderly people in China☆
2017-08-12 00:02:20XiaoHongZhangYangYangChunMeiZhangRuZhenLuoYanHuiLiu
Frontiers of Nursing 2017年2期
Xiao-Hong Zhang,Yang Yang,Chun-Mei Zhang,Ru-Zhen Luo,Yan-Hui Liu
Tianjin University of Traditional Chinese Medicine,Tianjin,300193,China
Development of a frailty scale for elderly people in China☆
Xiao-Hong Zhang,Yang Yang,Chun-Mei Zhang,Ru-Zhen Luo,Yan-Hui Liu*
Tianjin University of Traditional Chinese Medicine,Tianjin,300193,China
A R T I C L EI N F O
Article history:
10 March 2017
Accepted 4 April 2017
Available online 8 June 2017
Frailty
Elderly
Scale development
Reliability
Validity
Objective:The aim of this study was to develop a frailty scale for the elderly in China and to examine its reliability and validity.
Methods:The method of convenient sampling was used to select 375 elderly individuals in different communities of Tianjin,China.EuroQol-5D was used to evaluate the criterion validity.Cronbach'sα coef fi cients,correlation analysis,exploratory factor analysis,criterion-related validity,and internal consistency were used to evaluate the reliability and validity of the scale.To evaluate the test-retest reliability,30 old people were re-evaluated after 2 weeks.
Results:The fi nal version of the frailty scale(FI-35)consisted of 35 items.Eleven factors were extracted by a principal factor analysis and varimax rotation,with a cumulative contribution of 86.00%.Eleven dimensions were positively correlated(r=0.130-0.541,P<0.01).Cronbach'sαcoef fi cient was 0.952, and the alpha coef fi cients of 11 dimensions ranged from 0.730 to 0.992.The test-retest reliability was 0.874 for the total scale.The split-half reliability of the scale was 0.808.Structural equation modeling was used to perform a con fi rmatory factor analysis,and various parameters were all acceptable.
Conclusions:FI-35 met the requirement of scale development and showed good reliability and validity; thus,it can be used as an ef fi cient frailty measurement tool for Chinese elderly.
©2017 Shanxi Medical Periodical Press.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1.Introduction
Frailty is prevalent in the elderly in community and long-term care settings,and it can increase the risk of adverse events.1Although researchers have discussed the necessity of environmental factors to evaluate frailty,the corresponding evaluation tools have not been developed.Therefore,it is important to identify frailindividualsandtodevelopcomprehensivescreening instruments.
Frailty has been described as a reduction in the capacity of the organism that arises with increasing age;it makes elderly people vulnerable to changes in the environment.2,3Frailty has been considered a better predictor of adverse health events than age.4A large number of studies have demonstrated that frailty can be effectively used to predict disability,disease,death,hospitalization and other adverse health events.4-7In addition,frailty is a process that can be intervened.There are many effective interventions toprevent frailty,such as active exercise;adequate protein,calories, and vitamin D;and avoidance of drug abuse.8-10In 2013,experts from international organizations recommended that it is imperative toscreen forolder peoplewho are over70years old orhave lost more than 5%of body weight due to chronic diseases.11Therefore, early frailty screening and appropriate interventions can effectively preventor reduce the level of weaknessin the old and have bene fi ts for individuals,families and society.
There are two main branches of early research on frailty: Fried's12Frailty phenotype(FP)and Rockwood's13Frailty index(FI). Both have good predictive validity for physiological functional decline in the elderly,but there is no distinction between the concept of frailty and disease or disability.Subsequently,under the guidance of the multi-dimensional frailty model,scholars have developed a series of multi-dimensional frailty evaluation tools: Rolfson et al14designed the Edmonton frailty scale in 2006;Professor Steverink15created the Groningen frailty index in 2001; Gobbens et al16developed the Tilburg frailty index;and Nico De Witte et al17contrived a comprehensive frailty assessment instrument(CFAI).However,all of these tools only considered three aspects(physical,psychological and social)to assess the level of frailty in the old,ignoring functional de fi ciencies in environmental adaptation.
Environment has a great impact on the health of the elderly;a change in the environment will contribute to the risk of functional decline.Moreover,a decline in the ability of the elderly to adapt to the environment will make their health problems more serious. Nourhash′emi et al18noted that frailty was the interaction of physical,psychological,social,and environmental factors.Ferrazzoli et al19added the environmental adaption to the theory model of frailty and concluded that frailty was described by a reduction in the ability to adapt to the environment.Although researchers have discussed the feasibility and necessity of environmental factors,the corresponding theoretical models and evaluation tools have not been developed.A comprehensive frailty assessment tool is a basic necessity to accurately assess the frailty level of aged people,and it is a basis for the development of intervention measures.Therefore, it is necessary to develop more comprehensive frailty assessment tools for elderly people.
According to the above-reviewed literature,we investigated the association between environmental adaptation among elderly individuals and frailty and constructed an evaluation tool for elderly in China,which includes four dimensions:physiological,psychological,social and environmental.Furthermore,we analyzed and examined the reliability and validity of the items in the scale.
2.Methods
2.1.Design
The study consisted of the following 2 phases:(1)collection of data fromolder residents todevelopthe FI-35;(2)and evaluation of the reliability and validity of the scale.
2.2.Sample
Convenience sampling was used to recruit participants between October and December 2016.In this study,the elderly were included if they met three criteria as follows:(1)60 years of age or older;(2)able to communicate and conscious;and(3)volunteered to participate in the study.Samples missing more than 5%of the recovered questionnaires were deleted.Finally,420 older people were recruited from community dwellings in Tianjin,China.A total of 392 questionnaires were returned.Among them,375 valid questionnaires were received,of 17 which were rejected due to incomplete responses(effective response rate=89.2%).The demographic characteristics of the participants are summarized in Table 1.
2.3.Ethical considerations
Elders'rights were protected by the investigator by explaining the purpose and process at the beginning of the interview.All subjects were assured that their participation in the study was voluntary and that they had the right to refuse participation for any reason.To ensure anonymity in the use of data,we omitted the participants'names.Ethical approval was obtained from the relevant community.
2.4.Instrument
2.4.1.Scale design
The demographic data were composed of two parts,including gender,age,marital status,having children,degree of education and occupation before retirement and income.The next part included self-care ability,smoking,drinking,and exercise.These variables potentially in fl uence the frailty of the elderly.Based on the Gobbens frailty theory model,20a panel discussion and existingelder frailty appraisal tools,14,15,17,21we selected 81 items.The answers“yes”and“no”were used to evaluate the items(0=yes, 1=no).Some indicators were in the form of“yes”,“sometimes”and“no”,corresponding to a score of 0,0.5,or 1.
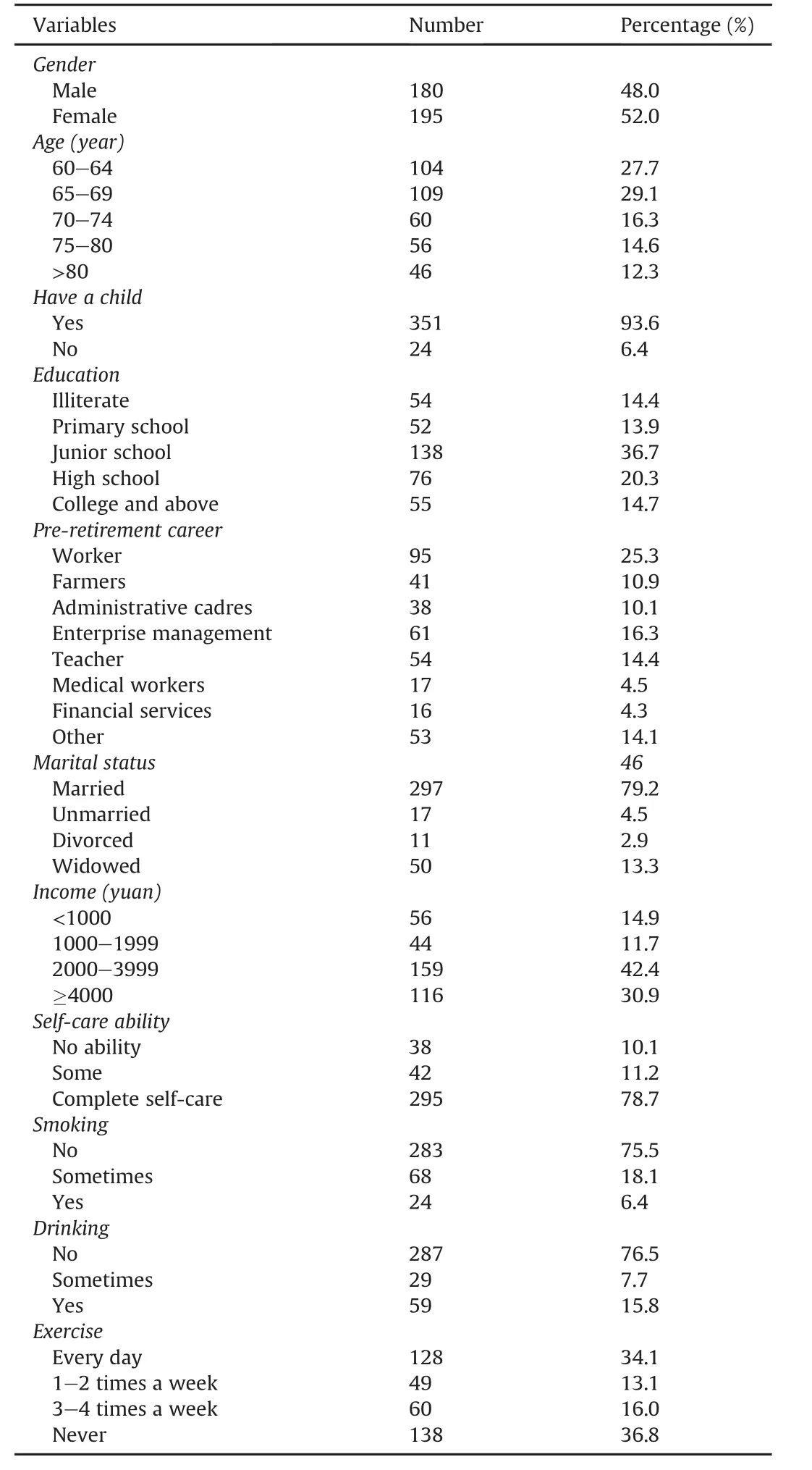
Table 1 Demographic characteristics of the participants.
We invited 15 experts in gerontology,nursing,and psychology to select the scale items.22In the fi rst round of 15 copies,13 were recovered,and the rate was 86.7%.In the second round of 13 copies, 12 were retrieved,and the rate was 92.3%.The participants rated each item using a fi ve-point Likert scale(1,not very important;2, not important;3,moderately important;4,important;and 5,very important).It is generally believed that the degree of expert authority(CR)is 0.7 or higher for acceptable reliability;this value was 0.89 in our study.We deleted 18 entries with values lower than 3.5 or coef fi cients of variation(CVs)higher than 0.25,23thus obtaining 63 items.Furthermore,to determine whether the language of thescale was suitable for the elderly,40 elders participated in a pilot study.The results indicated that it was easy for the elders to understand and answer the questions.
2.4.2.Data collection
Convenience sampling was used in this study.Questionnaires were completed by the elderly or were read by the investigators, who responded to the questions,options or explanations according to the oral responses of the elderly.After completing the scale,we invited 30 subjects who were interested in participating in a retest study after two weeks.
2.4.3.Data analysis
The data were analyzed using SPSS for Windows(version 20.0) (IBM Corporation,Armonk,New York,United States)and AMOS (Analysis of Moment Structures,version 17.0;Chicago,IL,USA). Descriptive statistics were used to summarize sample characteristics.The critical ratio method,correlation analysis,internal consistency reliability,commonality and factor load were used to screen items.In this study,the internal consistency coef fi cient and the split-half reliability were used to evaluate the internal reliability of the scale,and the external reliability of the scale was measured with theretest reliability.Furthermore,construct validity and criterion-related validity were used to evaluate the validity of the scale.The construct validity included an exploratory factor analysis(EFA)and con fi rmatory factor analysis(CFA).All statistical tests were two-sided(α=0.05).
3.Results
3.1.Item analysis
The internal correlation analysis of the scale was fi rst examined. Eight items(3,12,19,21,30,45,59,and 60)with correlations below 0.3 were deleted.24Next,we deleted items 5,6,20,28,29,42,54, and 58 because the total Cronbach'sαcoef fi cient of the scale was greater than(equal to)0.952 when we deleted them.
3.2.Validity analysis
3.2.1.Internal correlation
The internal correlation analysis of the scale is shown in Table 2. The scores on the eleven dimensions were positively correlated with each other(r=0.130-0.541,P<0.01).The correlation coef fi cients of each dimension and the total scale ranged from 0.550 to 0.671,indicating that the dimensions and the overall scale were moderately correlated.
3.2.2.Content validity
The content validity was determined by 13 experts in the fi elds of nursing andgerontology.The results revealed that the scale hada good content validity index(CVI=0.932).
3.2.2.1.Exploratory factor analysis.The Kaiser Meyer Olkin(KMO) was0.87,andBartlett'stestofsphericitywassigni fi cant (χ2=21595.04,P<0.001).Twelve items(16,8,44,43,50,46,41,18, 34,31,32,and 17)were deleted because their item loading was less than 0.4.25For the remaining 35 items,the KMO was 0.84 and Bartlett's test of sphericity was 2810.31(P<0.001),indicating that the correlations between items were adequate for the principal component analysis.Eleven factors with eigenvalues greater than 1 were extracted,which generated a cumulative contribution rate of 86.00%.As shown in Table 3,all loading on factors was greater than 0.4,which indicated good construct validity.The 11 factors were named as follows:Factor 1.nutrition(1-3 items),Factor 2.motion (4-7 items),Factor 3.strength(8-10 items),Factor 4.energy (11-13 items),Factor 5.sleep(14-16 items),Factor 6.emotion (17-19 items),Factor 7.cognition(20-23 items),Factor 8.role (24-26 items),Factor 9.contact(27-29 items),Factor 10.natural (30-32 items),and Factor 11.humanity(33-35 items).
3.2.2.2.Con fi rmatory factor analysis.A con fi rmatory factor analysis (CFA)was used to modify and improve the FI-35.The modi fi ed indexes of the CFA were as follows:χ2=501,df=418.2.Fitness parameters were within acceptable standards,excluding Adjusted Goodness of Fit Index(AGFI),which was slightly less than 0.90 (Table 4).The overall fi t of the model was better.Standard path and parameter estimates are shown in Fig.1.
3.2.3.Criterion-related validity
EQ-5D26is a multidimensional health assessment scale related to quality of life.The scale includes fi ve dimensions:“action”,“selfcare”,“daily activities”,“pain/discomfort”,and“anxiety/depression”.Each dimension is scored from 1 to 3.The higher is the score, the lower is the qualityof life.We evaluated the criterionvalidity by determining the correlation coef fi cients between the FI-35 and EuroQol-5D.The Spearman correlation coef fi cients were as follows (P<0.01):the total scale(0.643),nutrition(0.331),motion(0.300), strength(0.491),energy(0.228),sleep(0.345),cognition(0.501), emotion(0.506),contact(0.339),role(0.667),natural(0.321),and humanity(0.403).There was a moderate correlation between the FI-35 and the general health rating of the EQ-5D.
3.3.Reliability
Cronbach'sαcoef fi cient was used to estimate internal consistency with a coef fi cient of 0.70 or greater considered evidence ofreliability.27The Cronbach'sαcoef fi cients for the dimensions ranged from 0.730 to 0.992,and theαcoef fi cient for the total scale was 0.952,indicating good internal consistency reliability.The split-half reliability of the total scale was 0.808,which was acceptable.
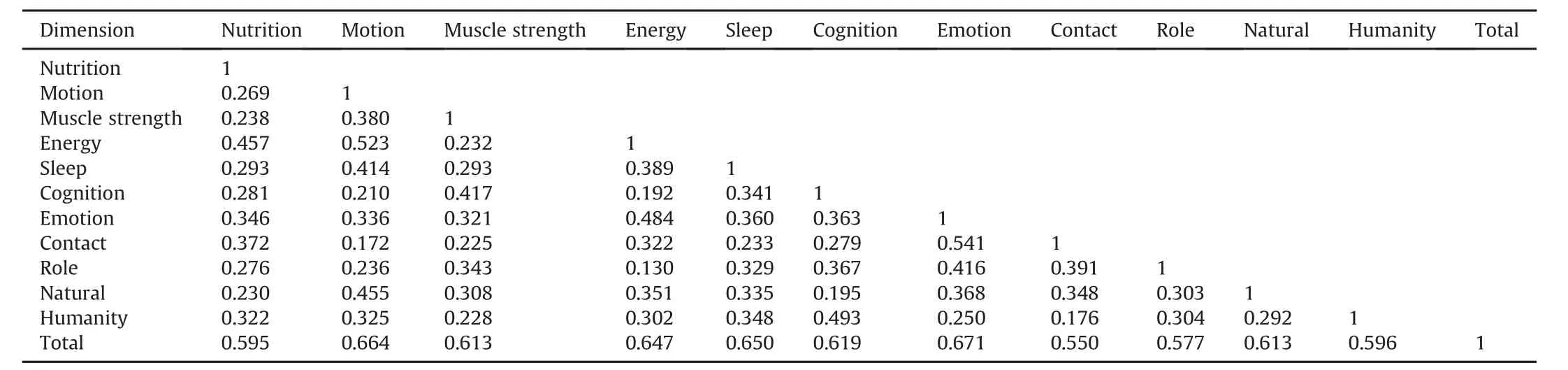
Table 2 Elderly frailty scale and internal correlation analysis between 11 dimensions and total score(r,n=375)(P<0.01).
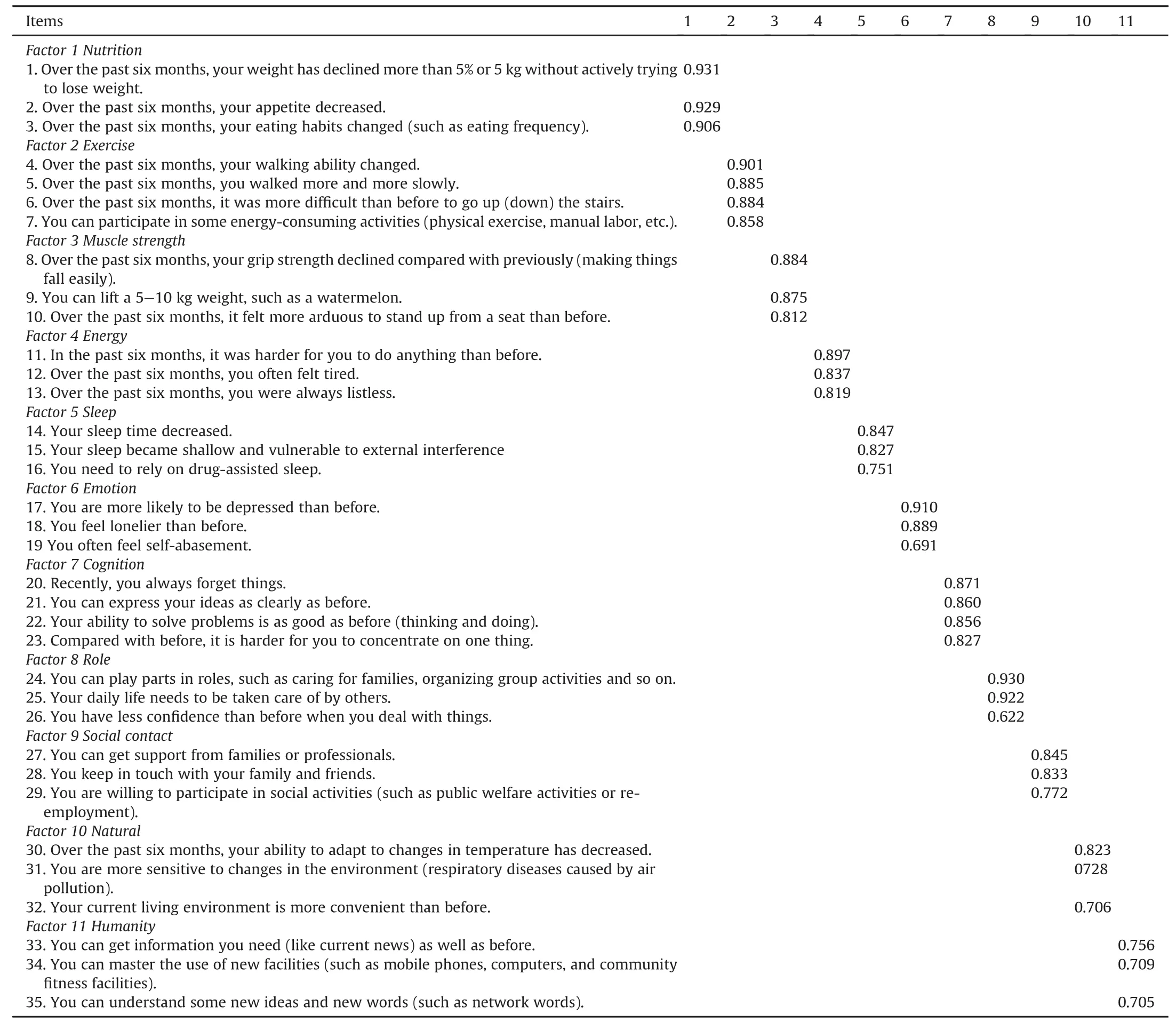
Table 3 Factor loading coef fi cients of the FI-35 scale after varimax rotation(n=375).
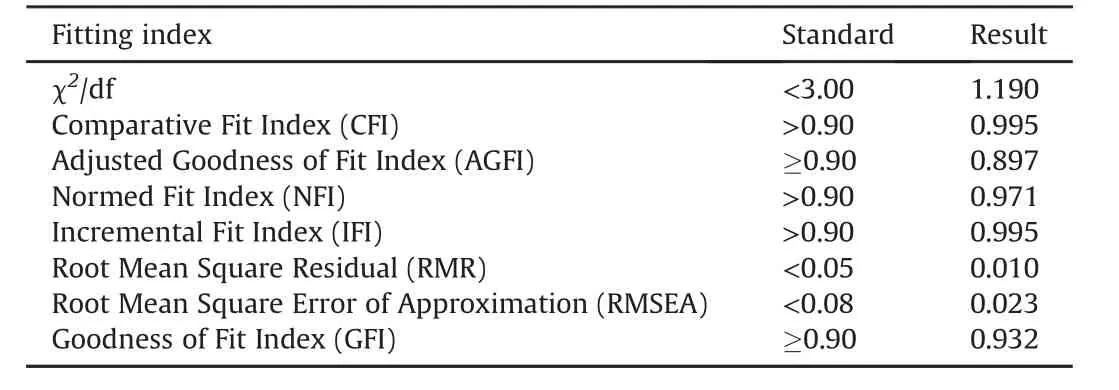
Table 4 Model fi t test standards and index results of FI-35.
We used the FI-35 to interview 30 elderly individuals who were willing to participate in measuring the test-retest reliability two weeks after the initial assessment.The correlation was high (r=0.874,P<0.01),which demonstrated that the scale is stable (Table 5).
4.Discussion
This study aimed to develop a frailtyassessment tool to improve health and quality of life in old adults.Nourhash′emi et al18noted that frailty was the interaction of physical,psychological,social,and environmental factors.FI-35 with 35 items from the four health domains was adapted to this theory.An exploratory factor analysis was used to test the construct validity of the scale,with a Cronbach'sαof 0.84,which explained 86%of the variance in frailty.The results show thatFI-35is a robust instrument forassessing the level of frailty with good validity and reliability.
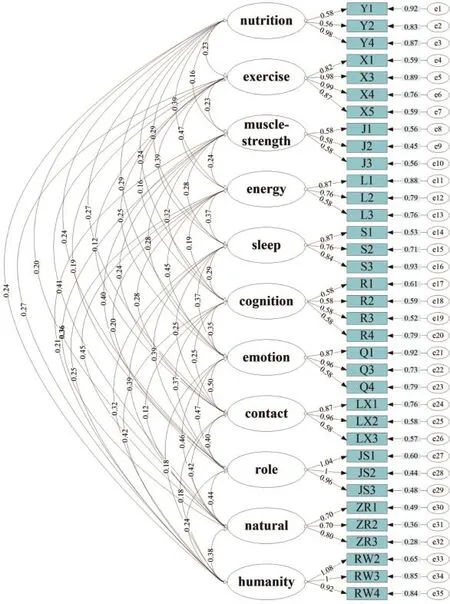
Fig.1.Standard path and parameter estimation for the FI-35 scale.
As described by Gobbens et al,16frailty was de fi ned as an individual loss of body function caused by various types of factors, which will increase the risk of adverse health events.Therefore,it is important to take effective measures to promote health and improve the quality of life of the elderly.A literature review and expert panel were used to screen items from several health domains instead of one limited health domain,forming the initial assessment tool of frailty among the elderly.
Criterion-related validity is used to examine the correlation between test indexes and other external criterion variables.Its results can represent or forecast the validity and accuracy of a criterion.28EQ-5D26is a multidimensional health assessment scale related to quality of life,which was chosen as a criterion.Our results showed that the total score and each dimension of the elderly individuals'frailty scale were signi fi cantly positively correlated with the quality of life scale,indicating that the criterion validity of the scale is good.
The most common method of determining internal reliability is Cronbach'sαcoef fi cient.29Cronbach'sαcoef fi cients for the 11 dimensions of the scale ranged from 0.730 to 0.992,indicating good internal consistency reliability.In addition,our test-retest analysis showed that the FI-35 was stable(r=0.874,P<0.01).In this work, we showed that the FI-35 is an appropriate method for assessing frailty among the elderly in communities in Tianjin,China.
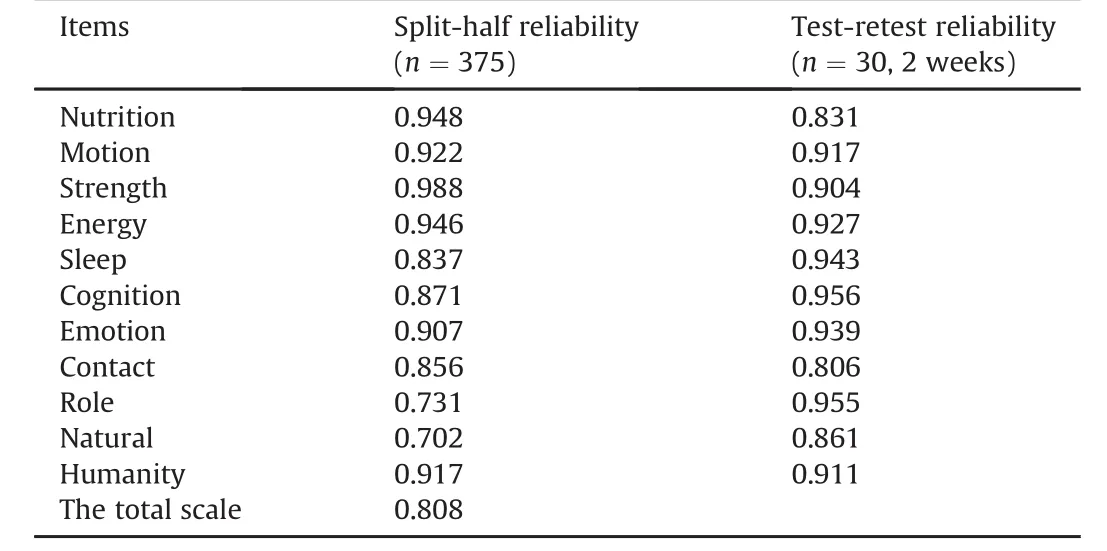
Table 5 Split-half reliability and test-retest reliability of FI-35(P<0.01).
The internal correlation analysis showed that the scores on the eleven dimensions(nutrition,exercise,muscle strength,energy, sleep,cognition,emotion,contact,role,natural,and humanity) were positively correlated with each other(r=0.130-0.541, P<0.01),which demonstrated that the construct validity of the frailty scale is good.In the fi rst stage of our study,EFA supported a 35-item scale with an 11-factor model:muscle(3 items),energy(3 items),action(4 items),cognitive(4 items),social contact(3 items),emotional(3 items),humanity(3 items),sleep(3 items), nutrition(3 items),role(3 items),and natural(3 items).The EFA showed that all factor loading coef fi cients of the 35 items were greater than 0.40.
Test-retest reliability coef fi cients and Cronbach'sαcoef fi cients were used to evaluate the reliability of the scale with a Cronbach'sα coef fi cient of 0.70 or greater considered evidence of reliability.24The Cronbach'sαcoef fi cients for the dimensions ranged from 0.730 to 0.992,and the coef fi cient for the total scale was 0.952, indicating good internal consistency reliability.The test-retest reliability was 0.874 for the total scale and 0.806-0.955 for the 11 sub-scales.A test-retest reliability coef fi cient above 0.75 is considered satisfactory.17The split-half reliability of the total scale was 0.808,which was acceptable.The results showed that the scale was stable.
Nonetheless,the study was limited in terms of conditions and time.We used convenience sampling,rather than random sampling,to choose the participants.The sample mainly came from the city of Tianjin in China,which indicates regional limitation and insuf fi cient coverage.Moreover,this study lacked participants who were in hospitals and nursing home,indicating that the characteristics of the old might be not comprehensive. Another limitation of the study was that we used measures of quantitative research such as reviewing the literature,group meetings and an expert panel to screen the items,excluding qualitative interviews.
5.Conclusions
This study established a reliable and valid FI-35 scale that covered four domains of functional ability in the elderly.The participants completed the questionnaires with scores of 0 for yes and 1 for no.The closer the score was to 1,the frailer the person was. The revised 35-item FI-35 has good estimates of reliability and validity.The reliability of the eleven sub-scales is also good and can be used to measure the frailty of Chinese elderly.The scale can be used as an assessment instrument when implementing frailty screening for the elderly.Since research on the frailty of the elderly is still limited,this scale also can make a contribution to related studies in the future.
Con fl icts of interest
All contributing authors declare no con fl icts of interest.
1.Juma S,Taabazuing MM,Montero-Odasso M.Clinical frailty scale in an acute medicine unit:a simple tool that predicts length of stay.Can Geriatr J.2016;19: 34-39.
2.Bielderman A,van der Schans CP,van Lieshout MR,et al.Multidimensional structure of the Groningen Frailty Indicator in community-dwelling older people.BMC Geriatr.2013;13:86.
3.Fried LP,Walston J.Frailty and failure to thrive.In:Hazzard W,Blass JP, Halter JB,et al.,eds.Principles of Geriatric Medicine and Gerontology.5th ed. New York:McGraw-Hill;2003:1487-1502.
4.Robinson TN,Wu DS,Pointer L,Dunn CL,Cleveland Jr JC,Moss M.Simple frailty score predicts postoperative complications across surgical specialties.Am J Surg.2013;206:544-550.
5.Ritt M,Gaßmann KG,Sieber CC.Signi fi cance of frailty for predicting adverse clinical outcomes in different patient groups with speci fi c medical conditions. Z Gerontol Geriatr.2016;49:567-572.
6.Adams P,Ghanem T,Stachler R,Hall F,Velanovich V,Rubinfeld I.Frailty as a predictor of morbidity and mortality in inpatient head and neck surgery.JAMA Otolaryngol Head Neck Surg.2013;139:783-789.
7.Abizanda P,Romero L,S′anchez-Jurado PM,Martínez-Reig M,G′omez-Arnedo L, Alfonso SA.Frailty and mortality,disability and mobility loss in a Spanish cohort of older adults:the FRADEA study.Maturitas.2013;74:54-60.
8.Zhang L,Weng C,Liu M,Wang Q,Liu L,He Y.Effect of whole-body vibration exercise on mobility,balance ability and general health status in frail elderly patients:a pilot randomized controlled trial.Clin Rehabil.2014;28:59-68.
9.Zaloga GP,Butterworth 4th JF.Hypovitaminosis D in hospitalized patients:a marker of frailty or a disease requiring treatment?Anesth Analg.2014;119: 613-618.
10.Bibas L,Levi M,Bendayan M,Mullie L,Forman DE,A fi lalo J.Therapeutic interventions for frail elderly patients:part I.Published randomized trials.Prog Cardiovasc Dis.2014;57:134-143.
11.Morley JE,Vellas B,van Kan GA,et al.Frailty consensus:a call to action.J Am Med Dir Assoc.2013;14:392-397.
12.Fried LP,Tangen CM,Walston J,et al.Frailty in older adults:evidence for a phenotype.J Gerontol A Biol Sci Med Sci.2001;56:M146-M156.
13.Rockwood K,Mitnitski A.Frailty de fi ned by de fi cit accumulation and geriatric medicine de fi ned by frailty.Clin Geriatr Med.2011;27:17-26.
14.Rolfson DB,Majumdar SR,Tsuyuki RT,Tahir A,Rockwood K.Validity and reliability of the Edmonton Frail Scale.Age Aging.2006;35:526-529.
15.Peters LL,Boter H,Buskens E,Slaets JP.Measurement properties of the Groningen Frailty Indicator in home-dwelling and institutionalized elderly people. J Am Med Dir Assoc.2012;13:546-551.
16.Gobbens RJ,Luijkx KG,Wijnen-Sponselee MT,Schols JM.Towards an integral conceptual model of frailty.J Nutr Health Aging.2010;14:175-181.
17.De Witte N,Gobbens R,De Donder L,et al.The comprehensive frailty assessment instrument:development,validity and reliability.Geriatr Nurs.2013;34: 274-281.
18.Nourhash′emi F,Andrieu S,Gillette-Guyonnet S,Vellas B,Albar`ede JL, Grandjean H.Instrumental activities of daily living as a potential marker of frailty:a study of 7364 community-dwelling elderly women(the EPIDOS study).J Gerontol A Biol Sci Med Sci.2001;56:M448-M453.
19.Ferrazzoli D,Sancesario G.Development and signi fi cance of the frailty concept in the elderly:a possible modern view.CNS Neurol Disord Drug Targets. 2013;12:529-531.
20.Gobbens RJ,van Assen MA,Luijkx KG,Schols JM.Testing an integral conceptual model of frailty.J Adv Nurs.2012;68:2047-2060.
21.Gobbens RJ,van Assen MA,Luijkx KG,Wijnen-Sponselee MT,Schols JM.The Tilburg Frailty Indicator:psychometric properties.J Am Med Dir Assoc.2010;11: 344-355.
22.Nimhurchadha S,Gallagher P,Maclachlan M,Wegener ST.Identifying successful outcomes and important factors to consider in upper limb amputation rehabilitation:an international web-based Delphi survey.Disabil Rehabil. 2013;35:1726-1733.
23.Keeney S,Hasson F,McKenna H.The Delphi Technique in Nursing and Health Research.Chichester,UK:Wiley-Blackwell;2011.
24.Nunnally JC,Bernstein IH.Psychometric Theory.3rd ed.New York:Mc Graw-Hill;1994.
25.Jia JP.Statistics.4th ed.Beijing:Renmin University of China Press;2011: 265-285(in Chinese).
26.Xing YB,Ma AX.Reliability and validity of the Chinese version of the European fi ve dimensional health scale EQ-5D-5L.Shanghai Med J.2013;34:40-43(in Chinese).
27.Strickland OL,Lenz ER,Waltz C.Measurement in Nursing and Health Research. 3rd ed.New York:Springer Publishing Company;2005.
28.Caplan G.Mastery of stress:psychosocial aspects.Am J Psychiatry.1981;138: 413-420.
29.Kim J,Lee SJ.Reliability and validity of the Korean version of the empathy quotient scale.Psychiatry Investig.2010;7:24-30.
How to cite this article:Zhang X-H,Yang Y,Zhang C-M,et al. Development of a frailty scale for elderly people in China.Chin NursRes.2017;4:64-70.http://dx.doi.org/10.1016/ j.cnre.2017.06.003
13 February 2017
☆This project was supported by the National Social Science Foundation(No. 14BSH124).
*Corresponding author.
E-mail address:yh_liu888@163.com(Y.-H.Liu).
Peer review under responsibility of Shanxi Medical Periodical Press.
in revised form
- Frontiers of Nursing的其它文章
- Transitional care interventions to reduce readmission in patients with chronic obstructive pulmonary disease:A meta-analysis of randomized controlled trials
- A bibliometric study of the Journal of School Health:1965-2014☆
- In fl uence of mobile education on joint function and quality of life in patients after total hip arthroplasty☆
- How to establish an expected animal model of post-traumatic osteoarthritis?
- Chewing gum for postoperative ileus after colorectal surgery: A systematic review of overlapping meta-analyses
- Retraction notice to“Relationships between perceived social support and retention patients receiving methadone maintenance treatment in China mainland”[CNR 3/1(2016)11-15]