
股骨近端锁定加压钢板治疗股骨转子间与转子下骨折内固定失效原因的 Meta 分析
2017-08-10 13:15:36余璐鑫高仕长史黎晗张安维刘洪涛
中国骨与关节杂志 2017年8期
余璐鑫 高仕长 史黎晗 张安维 刘洪涛
股骨近端锁定加压钢板治疗股骨转子间与转子下骨折内固定失效原因的 Meta 分析
余璐鑫 高仕长 史黎晗 张安维 刘洪涛
目的 探讨股骨近端锁定加压钢板 ( proximal femoral locking compression plates,PFLCP ) 固定股骨转子间、转子下骨折失效发生率及相关因素。方法 检索 PubMed Medline,Ovid Medline,Cochrane Database、Embase Database,检索时间范围:2005年 1月至 2015年 1月,以“PFLCP”、“Proximal Femoral Locking Compression Plate”、“treatment”为检索词,收集以英文发表的 PFLCP 治疗转子间、转子下骨折的文献,严格评价纳入研究的方法学质量并提取资料,采用 State 12.0以及 RevMan 5.2软件对检索结果进行系统分析。结果 共纳入 10篇文献,364例患者,PFLCP 治疗转子间及转子下骨折时内固定失效率为 20.05% ( 3.64%~73.68% )。其中钢板断裂发生率为 2.2% ( 95% CI:0.4%~4.0% ),螺钉断裂、松动、切出发生率为12.9% ( 95% CI:5.2%~20.6% ),骨折术后再移位发生率为 13.9% ( 95% CI:5.3%~22.4% )。年龄>60岁和转子区后内侧壁不完整者,术后内固定失效率较高。而骨折部位、术后首次下地部分负重的时间与 PFLCP 固定失效无明显关系。结论 PFLCP 治疗老年转子间、转子下骨折及转子区后内侧皮质不完整的患者时,术后内固定失效风险明显增高,而骨折部位、术后首次下地部分负重时间与 PFLCP 固定失效无关。
股骨骨折;髋骨折;骨折固定术,内;Meta 分析
股骨转子间骨折是髋关节囊线至小转子下方的骨折,好发于老年人,常为低能量损伤所致。股骨转子下区为小转子到股骨干髓腔峡窄部的解剖区域,骨质由松质骨转变为皮质骨,应力集中,周围有较多肌肉附着,因此转子下骨折移位明显,复位较困难。以上两类骨折若采用非手术治疗,均需长期卧床制动,极易出现骨折畸形愈合、下肢深静脉血栓、肺部感染、褥疮等并发症。因此,目前较为一致的意见是积极手术治疗[1-6]。
临床治疗股骨转子间、转子下骨折的方法有内固定和髋关节置换,其中常用的内固定装置有动力髋螺钉固定系统 ( dynamic hip screw,DHS )、动力髋联合大转子支持钢板 ( dynamic hip screw+trochanteric stabilising plate,DHS+TSP )、动力髁螺钉固定系统 ( dynamic condyle screw,DCS )、股骨近端锁定钢板 ( proximal femoral locking compression plate,PFLCP )、股骨近端防旋髓内钉 ( proximal femoral nail antirotation,PFNA ) 等。PFLCP 是近 10年出现的一种新型内固定装置,适用于股骨转子间及转子下骨折,其特点是钢板上有加压孔和锁定孔,既可作为桥接钢板使用,又可对骨折块加压,使骨折固定更稳定,可取得良好的疗效[9,14-15]。然而,也有文献报道 PFLCP 治疗转子间和转子下骨折的失效率较高[7-8]。为明确其临床疗效,收集近 10年有关PFLCP 治疗股骨转子间及转子下骨折疗效的文献,采用循证医学 Meta 分析的方法,研究内固定失败的发生率及其影响因素,为正确选择 PFLCP 治疗转子间、转子下骨折提供依据。
资料与方法
一、纳入与排除标准
1. 纳入标准:( 1) 与 PFLCP 治疗股骨转子间和( 或 ) 转子下骨折相关的国外文献;( 2) 文章发表时间为 2005年 1月至 2015年 1月;( 3) 需有 10例以上随访患者,随访时间≥6个月。
2. 排除标准:( 1) 不满足纳入标准的文章及重复性研究;( 2) 不同内固定材料治疗转子间和转子下骨折疗效对比的文献。
二、文献采集
1. 检索词:以“PFLCP”、“Proximal Femoral Locking Compression Plate”、“treatment”为检索词。
2. 检索库:PubMed Medline、Ovid Medline、Cochrane Database、Embase Database 等数据库。
3. 检索范围:2005年 1月至 2015年 1月。
查阅所有文献的标题及摘要,按纳入标准选择文献,摘要表述不明确时需查阅全文以确定是否采纳该文献,同时查阅文后所有参考文献,以全面查找相关资料 ( 图 1)。
4. 评价方法:所有纳入的文献均有 3名评价员独立进行质量评价和资料提取,对有争议的文献,三人合并第四人共同讨论决定,最后达成一致结果。根据 Cochrane Handbook 5.1.1评价标准,严格评价所纳入的研究论文。本研究收集文献 135篇,其中 PubMed Medline 113篇、Ovid Medline 12篇、Cochrane Database 6篇、Embase Database 4篇。经过查阅文献标题、摘要,排除重复文献 9篇及内容严重不符的文献 110篇。再深入阅读全文,根据纳入标准选择文献,保留 10篇英文文献进行归纳总结。所有文献均采用图表分析并发症情况 ( 表 1)。
三、测量指标
PFLCP 治疗股骨转子间和 ( 或 ) 转子下骨折发生内固定失效患者的数量及发生率,包括钢板断裂、螺钉断裂、松动、切出、术后骨折再移位等。
四、统计学处理
通过阅读全文,提取相关信息,用 Excel 表及手写笔记采集并记录数据,主要记录信息包括:第一作者、发表时间、研究人数、不同并发症发生人数、年龄分布、骨折分类 / 分型。整理所有数据,采用 State 软件及其 Meta 程序包、RevMan 软件对内固定失效例数进行统计分析,对多个研究结果进行合并及异质性分析。若 P>0.05,认为各项研究之间无异质性,采用固定效应模型进行分析,反之则用随机效应模型分析。得出结果后,再使用 State 软件对所纳入研究的数据进行 Begg 检验。若 P>0.05,则所纳入研究的文献之间不存在发表偏倚,采用结果。反之则不采用。Meta 分析的结果和特征用森林图来展示。
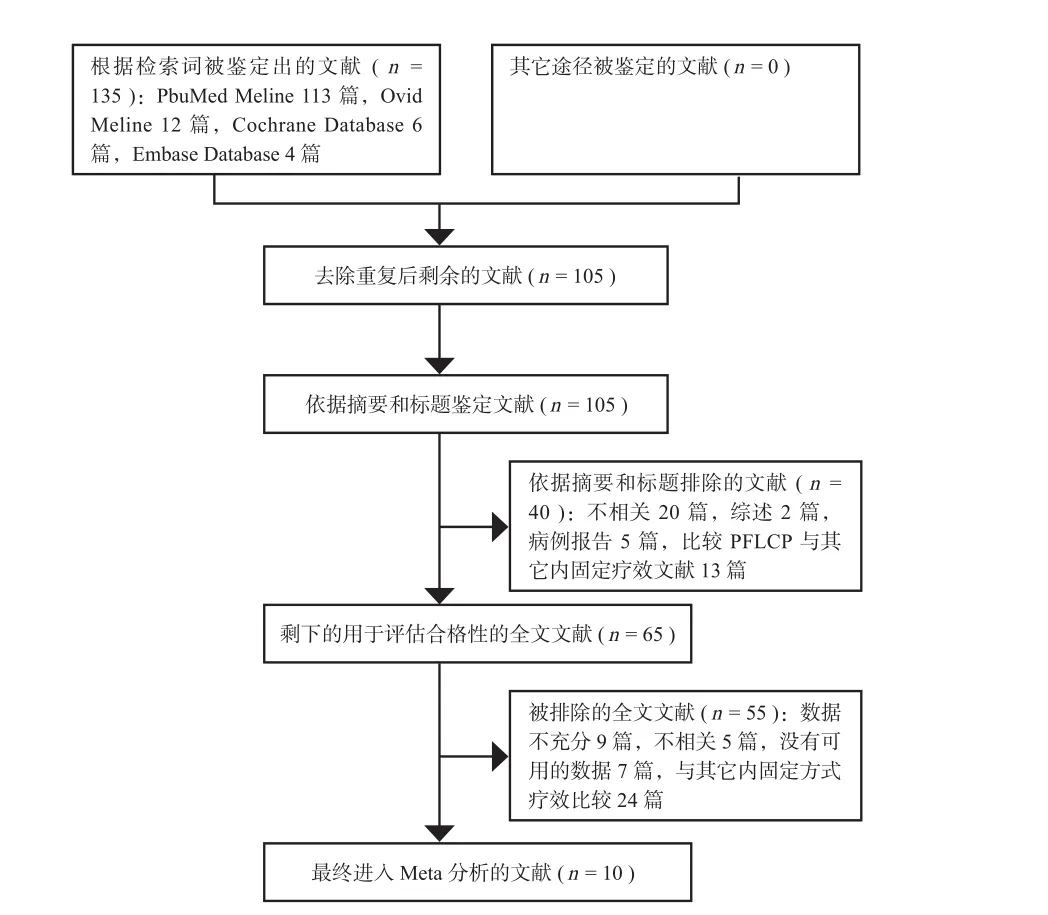
图1 文献筛选流程及结果Fig.1Screening process and results
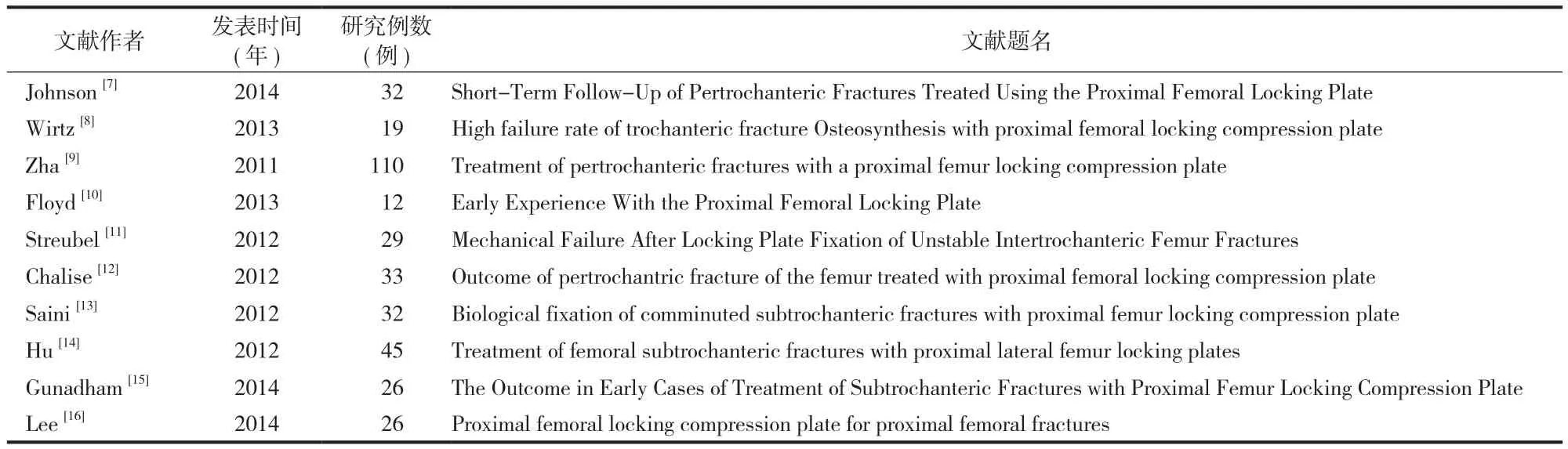
表1 纳入文献基本信息Tab.1Basic information on the literature
结 果
一、检索结果
本研究共纳入 10篇文献,364例,88例发生并发症,并发症发生率为 24.17%。常见并发症包括:钢板断裂 ( 11例 )、螺钉断裂 ( 11例 )、螺钉松动 / 切出( 21例 ) 及骨折再移位 ( 30例 )、术后感染 ( 10例 )、骨折愈合不良 ( 5例 )。其中与内固定失效相关的并发症有 73例,发生率为 20.05%。本研究主要统计内固定失效相关并发症有钢板断裂、螺钉断裂、螺钉松动及骨折再移位。
二、PFLCP 治疗转子间 / 转子下骨折发生内固定失效率的 Meta 分析森林图
10篇文献均报道了 PFLCP 发生内固定失效,发生率为 20.05% ( 3.64%~73.68% )。7篇文献报道了钢板断裂病例 ( P=0.389,采用固定效应模型分析 ),发生率为 2.2%,95% CI 为 0.4%~4.0% ( P=0.019);7篇文献报道了螺钉断裂、松动、切出病例 ( P<0.05,采用随机效应模型分析 ),发生率为12.9%,95% CI 为 5.2%~20.6% ( P=0.001);7篇文献报道了术后骨折再移位病例 ( P<0.05,采用随机效应模型分析 ),发生率为 13.9%。95% CI 为5.3%~22.4% ( P=0.001),见图 2~4。
三、分析 PFLCP 治疗转子间 / 转子下骨折术后部分负重时间与内固定失效的关系
根据不同医疗中心患者术后下地部分负重时间不同,分为术后 6周开始 ( 2篇 ) 和 8周及以后开始( 3篇 ) 2类,其中 51例术后 6周下地部分负重,出现内固定失效 17例 ( 33.33% )。100例术后 8周及以后开始下地功部分负重,出现内固定失效的患者27例 ( 27.0% )。经 χ2检验,二者差异无统计学意义( χ2=0.656,P=0.418),( 表 2)。
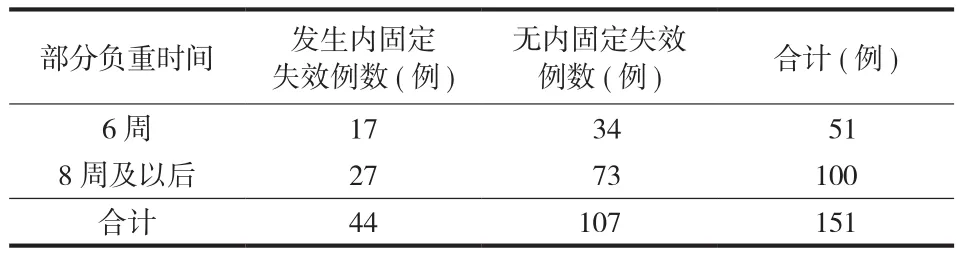
表2 不同术后部分负重开始时间的内固定失效率的比较Tab.2Comparison of the internal fixation failure rates between different starting times of postoperative partial weight-bearing walk
四、年龄与 PFLCP 失效相关性分析
共纳入 4项研究,各研究间无明显异质性 ( P= 0.43),采用固定效应模型。最小 Odds Ratio 值为0.08( 95% CI:0.01~1.25),最大 Odds Ratio 值为1.88( 95% CI:0.11~32.36),合并 Odds Ratio 值为0.35( 95% CI:0.16~0.74),PFLCP 治疗转子间 /转子下骨折老年组 ( 年龄≥60岁组 ) 内固定失效率明显高于对照组 ( P=0.006),( 图 5)。Begg 检验 z<1.96,Pr=0.317>0.05,研究不存在明显偏倚。
五、骨折部位、类型与内固定失效相关性分析
共纳入 6项研究,各研究间无明显异质性 ( P=0.39),采用固定效应模型分析。最小 Odds Ratio 值为 0.10( 95% CI:0.01~0.82),最大 Odds Ratio 值为 2.35( 95% CI:0.09~62.09),合并 OR 值为 0.75( 95% CI:0.30~1.87),PFLCP 治疗转子间及转子下骨折内固定失效率差异无统计学意义 ( P=0.54),( 图 6)。Begg 检验 z<1.96,Pr>|z|=0.497>0.05,研究不存在明显的偏倚。
笔者又将 4篇文章中转子间 / 转子下骨折分为股骨转子区后内侧皮质完整与后内侧皮质不完整两组,并分析内固定失效的差异。
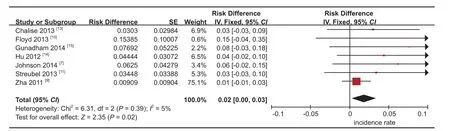
图2 PFLCP 治疗股骨转子间 / 转子下骨折钢板断裂发生率Fig.2The incidence of plate breakage in the treatment of intertrochanteric / subtrochanteric fracture with PFLCP
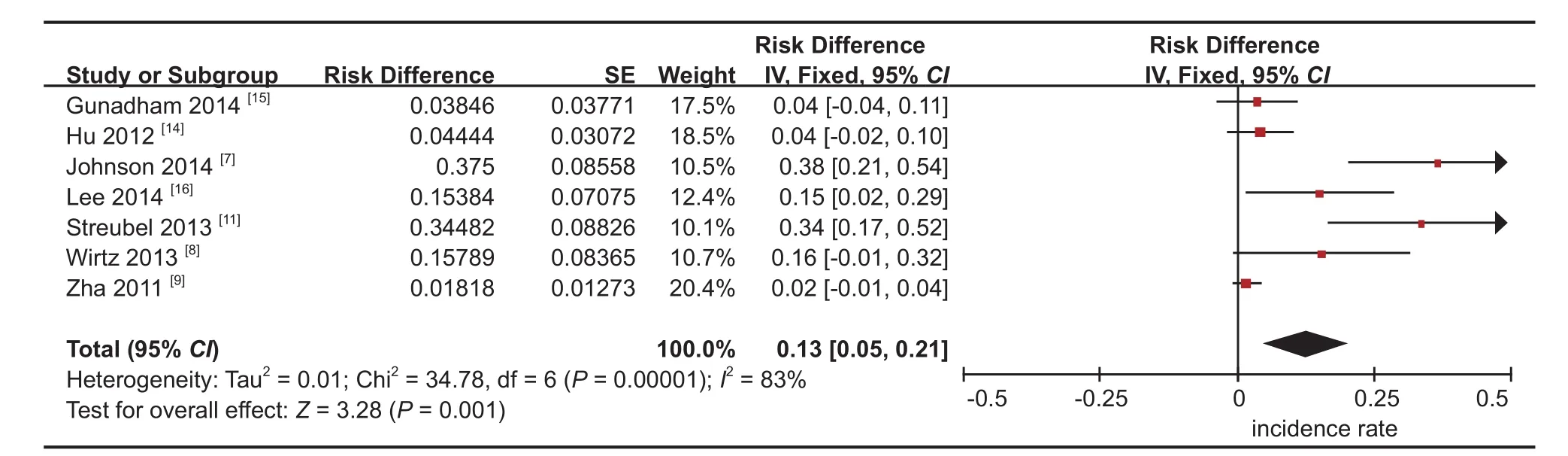
图3 PFLCP 治疗股骨转子间 / 转子下骨折螺钉失效发生率Fig.3The incidence of screw failure in the treatment of intertrochanteric / subtrochanteric fracture with PFLCP
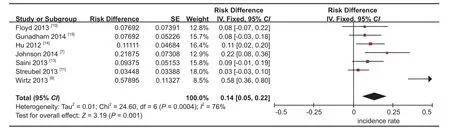
图4 PFLCP 治疗股骨转子间 / 转子下骨折术后再移位发生率Fig.4The incidence of postoperative displacement in the treatment of intertrochanteric / subtrochanteric fracture with PFLCP
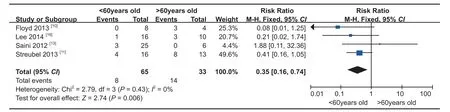
图5 年龄与出现内固定失效的关系Fig.5Correlative analysis between age and fi xation failure
共纳入 4项研究,各研究间无明显异质性 ( P= 0.76),采用固定效应模型分析。最小 Odds Ratio 值为 0.27( 95% CI:0.06~1.32),最大 Odds Ratio 值为 0.57( 95% CI:0.05~6.48),合并 OR 值为 0.26( 95% CI:0.09~0.76),PFLCP 治疗转子间 / 转子下骨折时,后内侧皮质不完整组的内固定失效率明显高于完整组 ( P=0.01),( 图 7)。Begg 检验 z<1.96,Pr>|z|=0.317>0.05,研究不存在明显的偏倚。
讨 论
PFLCP 是固定股骨近端骨折的一种新型钢板,其螺钉孔由动力加压孔和圆锥形螺纹孔复合构成。动力加压孔可使用标准螺钉实现轴向加压,圆锥形螺纹孔可与锁定螺钉的螺帽相扣锁。PFLCP 的优点包括:( 1) 适用于多种类型的转子间及转子下骨折;( 2) 术中复位与固定较方便;( 3) 可以局部轴向加压骨折块;( 4) 血运破坏较少:钢板与骨面之间最小接触,降低对骨膜血运的损伤;( 5) 对疏松骨质有较好的把持力;( 6) 允许早期功能锻炼等。缺点:偏心性结构设计,内固定失效率较高[7-8,11]。
一、PFLCP 治疗不同年龄患者内固定失效率的分析
共分为两组:老年组 ( 年龄≥60岁 ) 与非老年组 ( <60岁 ),统计分析发现老年组 PFLCP 失效率明显高于非老年组,这可能与转子区骨量丢失随年龄增长也逐渐增多从而降低了 PFLCP 固定的强度有关。
二、下地负重时间与 PFLCP 失效率分析
根据 Wolff 定律[17],骨折达到初期愈合需要增加骨折端的负荷,机械应力刺激是促进骨折愈合和提高愈合质量的必要条件。但过早的下地负重,可能造成内固定装置所受应力过大,出现内固定失效。对 5篇文献进行分析发现,6周与 8周以后开始下地负重的患者的内固定失效率差异无统计学意义。这可能与术后 6周骨折端已有骨痂形成可分担部分固定装置所受应力有关[18]。
三、转子区后内侧皮质不完整与内固定失效率较高的原因分析
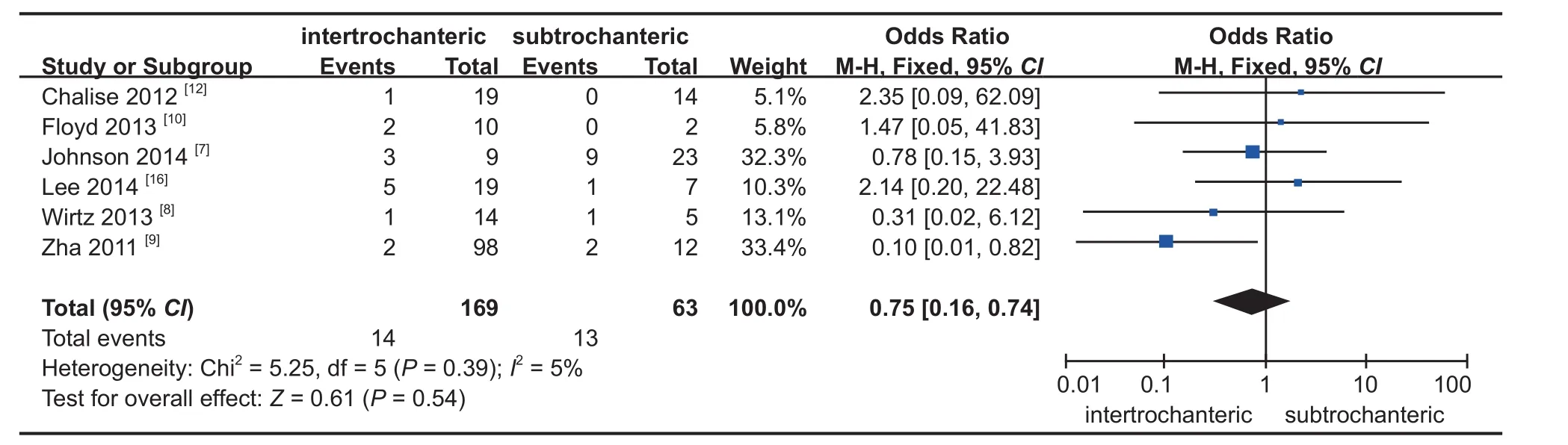
图6 PFLCP 治疗转子间、转子下骨折发生内固定失效相关性分析Fig.6Correlative analysis of fi xation failure of PFLCP in the treatment of intertrochanteric and subtrochanteric fracture
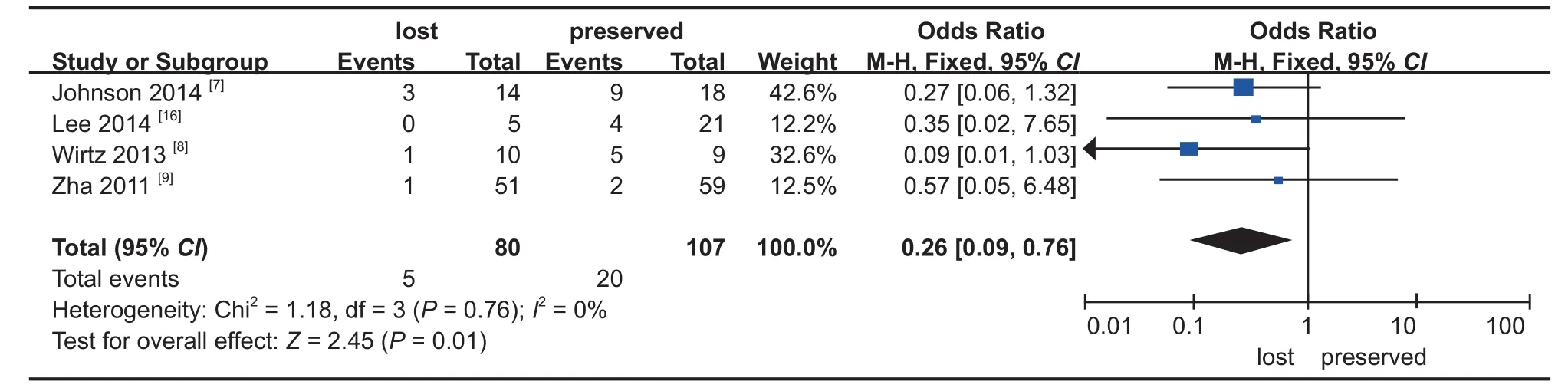
图7 股骨转子间、转子下骨折后内侧皮质完整性与 PFLCP 失效的相关性Fig.7Correlative analysis between the wholeness of the intertrochanteric / subtrochanteric posteromedial cortex and fi xation failure of PFLCP
转子区后内侧皮质缺损,常常累及股骨距。股骨距是股骨上端偏心性受载的着力点,正常人直立时承受巨大压力[19]。缺少完整股骨距结构的转子区骨折患者,如使用偏心性的 PFLCP 固定,术后患肢一旦下地负重,外侧的内固定装置会受到较大牵张应力,钢板承受周期性负荷, 极易发生疲劳而断裂[20]。因此,转子区后内侧皮质不完整者 PFLCP 内固定失效的风险明显增加。此时,术中应尽量恢复后内侧骨折块的接触,重建股骨距并尽量使用髓内固定系统以减少内固定装置的张应力。术后应避免在骨痂形成前过早下地负重行走,来降低内固定失效的风险。
目前 PFLCP 疗效的相关报道较少,本研究仅纳入合适文献 10篇 ( 共 367例 ),有一定的局限性。
综上所述,PFLCP 治疗老年转子间、转子下骨折及转子区后内侧皮质不完整的患者时,术后内固定失效风险明显增高,而骨折部位、术后首次下地部分负重时间与 PFLCP 固定失效无关。
[1] Sims SH. Subtrochanteric femur fractures[J]. Orthop Clin North Am, 2002, 33(1):113-126.
[2] Karn NK, Singh GK, Kumar P, et al. Comparison between external fi xation and sliding hip screw in the management of trochanteric fracture of the femur in Nepal[J]. J Bone Joint Surg Br, 2006, 88(10):1347-1350.
[3] Lundy DW. Subtrochanteric femoral fractures[J]. J Am Acad Orthop Surg, 2007, 15(11):663-671.
[4] Spruijt S, van der Linden JC, Dijkstra PD, et al. Prediction of tor-sional failure in 22cadaver femora with and without simulated sub- trochanteric metastatic defects: a CT scan based fin-ite element analysis[J]. Acta Orthopaedica, 2006, 77(3): 474-481.
[5] Goh SK, Yang KY, Koh JS, et al. Subtrochanteric insuff i ciency fractures in patients on alendr-onate therapy:a caution[J]. J Bone Joint Surg Br, 2007, 89(3):349-353.
[6] Bellabarba C, Herscovici D Jr, Ricci WM. Percutaneous treatment of peritrochanteric fractures using the Gamma nail[J]. Clin Orthop Relat Res, 2003, (375):30-42.
[7] Johnson B, Stevenson J, Chamma R, et al. Short-term follow-up of pertrochanteric fractures treated using the proximal femoral locking plate[J]. J Orthop Trauma, 2014, 28(5):283-287.
[8] Wirtz C, Abbassi F, Evangelopoulos DS, et al. High failure rate of trochanteric fracture osteo-synthesis with proximal femoral locking compression plate[J]. Injury, 2013, 44(6):751-756.
[9] Zha GC, Chen ZL, Qi XB, et al. Treatment of pertrochanteric fractures with a proximal femur locking compression plate[J]. Injury, 2011, 42(11):1294-1299.
[10] Floyd MW, France JC, Hubbard DF. Early experience with the proximal femoral locking plate[J]. Orthopedics, 2013, 36(12):e1488-1494.
[11] Streubel PN, Moustoukas MJ, Obremskey WT, et al. Mechanical failure after locking plate fixation of unstable intertrochanteric femur fractures[J]. J Orthop Trauma, 2013, 27(1):22-28.
[12] Chalise PK, Mishra AK, Shah SB, et al. Outcome of pertrochantric fracture of the femur treated with proximal femoral locking compression plate[J]. Nepal Med Coll J, 2012, 14(4):324-327.
[13] Saini P, Kumar R, Shekhawat V, et al. Biological fixation of comminuted subtrochanteric fractures with proximal femur locking compression plate[J]. Injury, 44(2):226-231.
[14] Hu SJ, Zhang SM, Yu GR. Treatment of femoral subtrochanteric fractures with proximal lateral femur locking plates[J]. Acta Ortop Bras, 2012, 20(6):329-333.
[15] Gunadham U, Jampa J, Suntornsup S, et al. The outcome in early cases of treatment of subtrochanteric fractures with proximal femur locking compression plate[J]. Malays Orthop J, 2014, 8(2):22-28.
[16] Lee WT, Murphy D, Kagda FH. Proximal femoral locking compression plate for proximal femoral fractures[J]. J Orthop Surg (Hong Kong), 2014, 22(3):287-293.
[17] Hu G. Traumatic Orthopedics fault and treatment[M]. Beiing, People Health Publishing. 2002: 53:65.
[18] Bucholz RW, Heckman JD, Koval KJ. Rockwood and Green’s fracture in adults[M]. 6th ed. North American. Lippincott Williams and Wilkins edition. 2014: 499.
[19] Le Corroller T, Dediu M, Pauly V, et al. The femoral calcar: a computed tomography anatomical study[J]. Clin Anat, 2011, 24(7):886-892.
[20] Ruedi TP, Buckley R, Moran CG, et al. AO principles of fracture management[M]. 2th ed. New York. AO Publishing Stuttgart. 2000: 192.
( 本文编辑:李慧文 王永刚 )
A Meta-analysis about the failure of proximal femoral locking compression plates to fix intertrechanteric or subtrochanteric fractures
YU Lu-xin, GAO Shi-chang, SHI Li-han, ZHANG An-wei, LIU Hong-tao.
Department of Orthopaedics, the fi rst aff i liated Hospital of Chongqing Medical University, Chongqing, 400016, China Corresponding author: GAO Shi-chang, Email: 778925053@qq.com
Objective To explore the fi xation failure incidence and related factors about proximal femoral locking compression plate ( PFLCP ) to fi x the intertroc-hanteric and subtrochanteric fractures. Methods “Proximal Femoral Locking Comp-ression Plate”, “PFLCP”and “treatment” were regarded as the terms searched in the PubMed Medline, Ovid Medline, Cochrane Database, and Embase Database. The collected references were published in English from January 2005to January 2015. The methodological quality of the included studies was critically appraised and the data were extracted. Ten references, including 364cases, were analyzed by the software of State 12.0and RevMan 5.2. Results The fi xation failure incidence of PFLCP was 20.05% ( 3.64% - 73.68% ), among which the incidence of plate broke 2.2% ( 95% CI 0.4% - 4.0% ), incidence of screw breakage, loose, and cut 12.9% ( 95% CI 5.2% - 20.6% ), and the incidence of postoperative fracture and displacement 13.9% ( 95% CI 5.3% - 22.4% ). When the patient’s age was older than 60years or the posterior-medial cortical bone of the intertrochanteric area was not intact, the fi xation failure rate of PFLCP was high, which was not relative to the site of fracture and the start time of postoperative partial weightbearing walk. Conclusions A high failure incidence will be predicted when PFLCP is used to fi x the intertrechanteric or subtrochanteric fractures of old patients or with posterior-medial cortex defect. The site of fracture, starting time of postoperative partial weight-bearing walk have no relations with the incidence.
Femoral fractures; Hip fracture; Fracture fi xation, internal; Meta-analysis
10.3969/j.issn.2095-252X.2017.08.009
R683.4
400016重庆医科大学附属第一医院骨科
高仕长,Email: 778925053@qq.com
2016-03-11,
2017-07-08)
猜你喜欢
化工管理(2023年17期)2023-06-16 05:56:54
数学物理学报(2022年2期)2022-04-26 14:08:46
中华骨与关节外科杂志(2021年12期)2021-08-31 09:10:54
计算机与数字工程(2019年7期)2019-07-31 09:55:10
电子机械工程(2018年3期)2018-08-02 05:08:24
中国继续医学教育(2015年3期)2016-01-06 01:36:36
分子影像学杂志(2015年3期)2015-12-04 03:28:58
实用手外科杂志(2015年2期)2015-08-28 09:50:40
医学研究杂志(2015年12期)2015-06-10 06:57:46
上海航天(2014年1期)2014-12-31 11:57:26
