
AFP、CA19-9、CEA联合检测对原发性肝癌的早期诊断价值
2017-08-07 10:05李嘉妍宋金云王建芳吴旭平
临床肝胆病杂志 2017年7期
李嘉妍, 宋金云, 王建芳, 吴旭平
(东南大学附属第二医院 临床科研中心, 南京 210003)
论著/肝脏肿瘤
AFP、CA19-9、CEA联合检测对原发性肝癌的早期诊断价值
李嘉妍, 宋金云, 王建芳, 吴旭平
(东南大学附属第二医院 临床科研中心, 南京 210003)
目的 研究AFP、CA19-9、CEA联合检测对原发性肝癌进行早期诊断的临床价值。 方法 收集2014年10月-2016年12月东南大学附属第二医院门诊和住院的肝病患者248例,分为原发性肝癌组(n=88)和非肿瘤性肝病组(n=160),另选取130例健康体检者为正常对照组。采用Roche cobas e 411 analyzer检测3组患者的血清肿瘤标志物AFP、CA19-9、CEA水平,分析3种肿瘤标志物单个检测和联合检测的灵敏度和特异度。采用Beckman Coulter AU5800检测肝功能生化指标。采用Biotek ELX808检测HBV血清学标志物和HCV抗体。应用受试者工作特征曲线(ROC曲线)对原发性肝癌患者的血清AFP、CA19-9、CEA及3者联合检测结果进行分析评价。计量资料多组间比较采用单因素方差分析,进一步两两比较采用SNK-q检验,2组间比较采用t检验;计数资料组间比较采用χ2检验。相关性分析采用Spearman分析。结果 在原发性肝癌组和非肿瘤性肝病组中,肝功能异常患者的AFP、CA19-9均显著高于肝功能正常组(原发性肝癌组:t值分别为35.64、3.38,P值均<0.05;非肿瘤性肝病组:t值分别为12.51、8.19,P值均<0.05);原发性肝癌组中肝功能正常患者的CEA均明显高于非肿瘤性肝病组中肝功能正常患者和正常对照组(P值均<0.05);原发性肝癌组中肝功能异常患者的AFP、CA19-9、CEA水平均明显高于非肿瘤性肝病组中的肝功能异常患者和正常对照组(P值均<0.05)。血清AFP、CA19-9、CEA水平随Child Pugh分级的升高而升高,在原发性肝癌组肝功能异常患者中,AFP、CA19-9、CEA水平B级较A级,C级较B级均显著升高(P值均<0.05);在非肿瘤性肝病组肝功能异常患者中, AFP、CA19-9水平B级较A级,C级较B级均显著升高(P值均<0.05),CEA水平C级显著高于A、B级(P值均<0.05)。原发性肝癌组AFP、CA19-9、CEA的阳性率高于非肿瘤性肝病组和正常对照组(P值均<0.05);各组的联合检测阳性率显著高于单项检测阳性率(P值均<0.05)。原发性肝癌组中,三项联合检测的灵敏度和特异度分别为86.36%和92.35%,单项检测中AFP、CA19-9、CEA的灵敏度分别为71.59%、52.27%和39.77%,原发性肝癌患者的血清AFP、CA19-9、CEA及三者联合检测ROC曲线下面积分别为0.776、0.704、0.681及0.817。AFP在原发性肝癌组中与GGT相关(r=0.54,P=0.04),在正常对照组中与IBil相关(r=0.50,P=0.01);CA19-9在原发性肝癌组与ALT、 DBil、 IBil、TBil、TBA存在不同程度相关(r值分别为0.58、0.63、0.61、0.65、0.58,P值均<0.05),在非肿瘤性肝病组与ALT、ALP、DBil、 IBil、TBil、TBA存在不同程度相关(r值分别为0.51、0.63、0.66、0.64、0.70、0.59,P值均<0.05)。结论 AFP能较好地反映肝损伤,但对原发性肝癌的诊断仍有部分假阴性;CEA轻度升高对原发性肝癌的指示性不强;CA19-9受ALP、胆红素等因素影响明显,假阳性较高;联合检测可提高原发性肝癌诊断的灵敏度,优于AFP、CA19-9、CEA的单项检测,可为早期诊断和早期治疗提供有力的依据。
肝肿瘤; 甲胎蛋白类; CA-19-9抗原; 癌胚抗原; 诊断
原发性肝癌是一种病死率高的恶性肿瘤,在世界范围内的发病率呈逐渐上升趋势[1]。由于影像学诊断和病理学检测对早期诊断原发性肝癌价值有限,目前多采用肿瘤标志物检测,辅助原发性肝癌早期诊断和治疗。本文旨在探讨血清肿瘤标志物AFP、CA19-9、CEA三者联合检测在原发性肝癌诊断中的价值。
1 资料与方法
1.1 研究对象 收集2014年10月-2016年12月于本院就诊的肝病患者248例,其中经病理检查确诊的原发性肝癌患者88例(原发性肝癌组),非肿瘤性肝病患者160例(非肿瘤性肝病组),同时收集体检健康的正常对照者130例(正常对照组)。本研究经医院医学伦理学委员会批准,且患者知情同意。
1.2 仪器 AFP、CA19-9和CEA采用Roche cobas e 411 全自动化学发光分析仪检测,肝功能采用Beckman Coulter AU5800检测,HBV血清学标志物和HCV抗体采用Biotek ELX808检测。
1.3 检测方法 所有研究对象均于清晨空腹采集外周血并及时分离血清,检测患者肝功能指标及肿瘤标志物水平,严格按照说明书进行操作。阳性判断标准分别为:AFP>20 μg/L,CA19-9>27 U/ml,CEA>4.7 ng/ml。AFP、CA19-9、CEA联合检测时其中1项阳性即视为三项联合检测为阳性。肝功能异常判断标准为:转氨酶(ALT>64 U/L或AST>50 U/L)、胆红素(DBil>8.0 μmol/L或IBil>14.0 μmol/L或TBil>22.0 μmol/L)及其他生化指标[ALP>150 U/L或总胆汁酸(TBA)>12.0 μmol/L或GGT>37 U/L]3项中有2项升高者被认为肝功能异常。HBV血清学标志物和HCV抗体阳性标准参照文献[2]。

2 结果
2.1 一般资料 原发性肝癌组88例患者中男67例,女21例,年龄33~75岁,平均(55.2±12.4)岁;HBsAg阳性83例,抗HCV阳性3例,HBsAg阳性合并抗HCV阳性2例;肝功能正常者25例,异常者63例。非肿瘤性肝病组160例患者中慢性肝炎55例,肝硬化57例,急性黄疸型病毒性肝炎48例;肝功能正常者92例,异常者68例。慢性肝炎55例患者中男43例,女12例,年龄20~67岁, 平均(37.50±10.06)岁,HBsAg阳性50例、抗HCV阳性3例、HBsAg阳性合并抗HCV阳性2例;肝硬化57例患者中男46例, 女11例, 年龄29~68岁, 平均(61 .34 ±30 .10)岁,HBsAg阳性49例、抗HCV阳性7例、HBsAg阳性合并抗HCV阳性1例;急性黄疸型病毒性肝炎48 例患者中男32例,女16例,年龄20~49岁, 平均(33.24±9.62)岁,抗HCV阳性5例、HBV感染43例。
2.2 3组AFP、CA19-9、CEA水平的比较 原发性肝癌组和非肿瘤性肝病组中,肝功能异常患者的AFP、CA19-9水平显著高于肝功能正常患者(P值均<0.05)(表1)。
原发性肝癌组和非肿瘤性肝病组的肝功能正常患者与正常对照组3者间CA19-9和CEA水平比较差异有统计学意义(F值分别为19.08、94.95,P值均<0.05)。进一步两两比较,原发性肝癌组肝功能正常患者的CEA水平明显高于非肿瘤性肝病组肝功能正常患者和正常对照组(P值均<0.05);原发性肝癌组与非肿瘤性肝病组的肝功能正常患者CA19-9水平均显著高于正常对照组(P值均<0.05)。2组的肝功能异常患者与正常对照组3者间AFP、CA19-9、CEA水平比较差异均有统计学意义(F值分别为32.73、2.24、109.10,P值均<0.05),进一步两两比较,原发性肝癌组肝功能异常患者的AFP、CA19-9、CEA水平均明显高于非肿瘤性肝病组肝功能异常患者和正常对照组(P值均<0.05)(表1)。
表1 3组血清AFP、CA19-9、CEA检测结果
注:1)与正常对照组比较,P<0.05;2)与非肿瘤性肝病组的肝功能正常患者比较;P<0.05;3)与非肿瘤性肝病组的肝功能异常患者比较,P<0.05
2.3 不同Child-Pugh评分的肝功能异常患者肿瘤标志物水平的比较 依据Child-Pugh评分,将原发性肝癌组和非肿瘤性肝病组中肝功能异常患者均分为Child-Pugh A、B、C 3个亚组。在原发性肝癌组肝功能异常患者中,AFP、CA19-9、CEA水平B级较A级,C级较B级均显著升高(P值均<0.05);在非肿瘤性肝病组肝功能异常患者中, AFP、CA19-9水平B级较A级,C级较B级均显著升高(P值均<0.05),CEA水平C级显著高于A、B级(P值均<0.05)(表2)。
2.4 3组AFP、CA19-9、CEA单项检测及联合检测的阳性率 3组单项检测和联合检测整体比较阳性率差异有统计学意义(χ2=20.23,P<0.05),原发性肝癌组AFP、CA19-9、CEA的阳性率均高于非肿瘤性肝病组和正常对照组(P值均<0.05)。各组的联合检测阳性率显著高于单项检测阳性率(P值均<0.05)(表3)。
2.5 原发性肝癌组AFP、CA19-9、CEA单项及三项联合检测的灵敏度、特异度和AUC 原发性肝癌组三项联合检测的灵敏度和特异度分别为86.36%和92.35%;在单项检测中,AFP灵敏度最高达71.59%, CA19-9和CEA的灵敏度分别为52.27%和39.77%。AFP、CA19-9、CEA的AUC分别为0.776、0.704、0.681,三项联合检测的AUC为0.817,高于单项检测(图1)。
表2 肝功能异常患者不同Child-Pugh评分的肿瘤标志物 水平比较
注:1)与Child-Pugh B级比较,P<0.05;2)与Child-Pugh C级比较,P<0.05
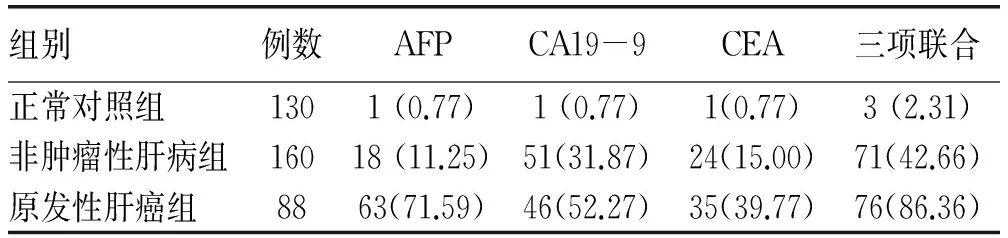
表3 3组AFP、CA199、CEA单项及三项联合检测的 阳性率[例(%)]
2.6 3组中AFP、CA19-9、CEA与肝功能指标的相关性分析 AFP在原发性肝癌组中与GGT相关(r=0.54,P=0.04),在正常对照组中与IBil相关(r=0.50,P=0.01)。CA19-9在原发性肝癌组中与ALT、 DBil、 IBil、TBil、TBA存在不同程度相关(r值分别为0.58、0.63、0.61、0.65、0.58,P值均<0.05),在非肿瘤性肝病组中与ALT、ALP、DBil、 IBil、TBil、TBA存在不同程度相关(r值分别为0.51、0.63、0.66、0.64、0.70、0.59,P值均< 0.05)。CEA在各组中与各指标未见明显相关。
3 讨论
随着社会经济的发展,生活方式的改变,原发性肝癌的相关危险因素普遍存在,早发现、早诊断、早治疗是提高原发性肝癌患者生存率的关键。血清肿瘤标志物在血清中出现要早于临床症状,当血清肿瘤标志物达到一定水平就能揭示某种肿瘤的存在[3],对肿瘤的早期诊断有重要意义,所以肿瘤标志物的检测越来越受到临床医生的重视。
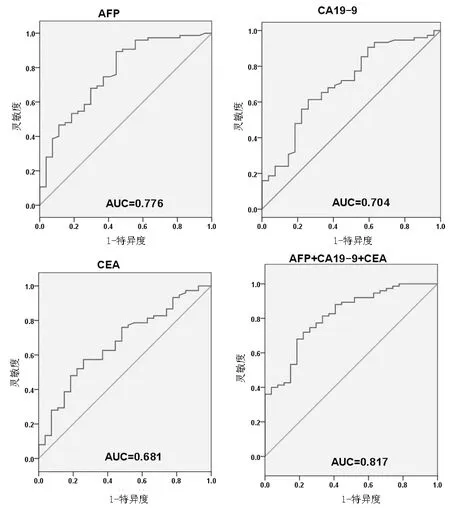
图1 单项和联合检测诊断原发性肝癌的ROC曲线分析
AFP、CA19-9、CEA是临床上常见的肿瘤标志物,主要用于消化道、乳腺以及呼吸道等系统肿瘤的检测。AFP主要在胎儿肝脏中合成,随着胎儿的发育肝脏逐渐发育成熟,AFP逐渐接近成人水平。当肝细胞癌变时,部分肝细胞恢复产生AFP的功能,使血清AFP水平升高,因此,AFP被广泛用于肝癌的辅助诊断[4]。CA19-9是由消化道肿瘤细胞分泌的一种类糖脂抗原,是一种与腺癌高度相关的抗原物质,又称胃肠癌相关抗原[5-6]。临床检测发现CA19-9在原发性肝癌中也有较高表达,有研究[7-9]报道,CA19-9在原发性肝癌患者中阳性率为40%~70%左右。CEA是从结肠腺癌和胎儿肠组织中提取的一种肿瘤相关抗原,是一种光谱肿瘤标志物,在转移性肝癌、胃癌、肺癌、结肠癌等中存在不同程度的阳性率[10]。
肝脏肿瘤标志物与肝功能密切相关[11-12]。本研究原发性肝癌中的AFP阳性率为71.59%,与以往的报道相近[13-14],肝功能异常组血清AFP水平显著高于正常组,血清AFP能较好地反映肝功能,但对部分AFP阴性的肝癌患者不存在诊断价值。在原发性肝癌组中,AFP与GGT呈正相关,与以往的报道一致[15]。在原发性肝癌组和非肿瘤性肝病组中,CA19-9与胆红素、ALP呈正相关,提示CA19-9与胆汁排出顺畅程度有关。当存在明显的胆道梗阻时,CA19-9失去了作为肿瘤标志物的意义,这与文献报道一致[12],因此,CA19-9需要联合多项肝功能生化指标及AFP、CEA才能提高对原发性肝癌诊断的准确度。CEA受肝功能生化指标影响小,在原发性肝癌组中阳性率较低,本研究中仅为39.77%,因此需要联合AFP、CA19-9进行分析以提高对原发性肝癌诊断的准确度。
AFP能较好地反映肝损伤,但对原发性肝癌的诊断仍有部分假阴性;CEA在3组中受肝功能生化指标影响较小;CA19-9受ALP、胆红素等因素影响明显,假阳性较高;联合检测AFP、CA19-9、CEA可提高原发性肝癌诊断的灵敏度,优于AFP、CA19-9、CEA的单项检测,可为早期诊断和早期治疗提供有力的依据。
[1] ZHAO YS, ZHANG LN, LI HC, et al. Clinical significance of serum GP73, AFP, and CA199 test in the diagnosis of hepatic cancer[J]. Chin J Gastroenterol Hepatol, 2013, 40(1): 29-32. (in Chinese) 赵运胜, 张丽娜, 李洪臣, 等. 血清GP73联合AFP和CA199检测在肝癌诊断中的临床意义[J]. 中国肿瘤临床, 2013, 40(1): 29-32.
[2] ZENG YL, MA QF, XIONG W, et al. Relationships between HBV-M patterns and liver function, HBV-DNA in patients with chronic HBV infection of different stages[J]. Int J Lab Med, 2015, 36(4): 433-435. (in Chinese) 曾雅莉, 马清峰, 熊微, 等.不同病期慢性HBV感染者肝功能、HBV-DNA与HBV-M模式的关系[J]. 国际检验医学杂志, 2015, 36(4): 433-435.
[3] RAIN AJ, CHAN DW. Cancer proteomics: serum diagnostics for tumor marker discovery[J]. Ann N Y Acad Sci, 2004, 1022: 286-294.
[4] SI X, TAN GJ. Value of tumor markers carcinoembryonic antigen, alpha-fetoprotein, and carbohydrate antigen 199 in diagnosis of liver cancer[J]. Jilin Med J, 2008, 29(16): 1392-1393. (in Chinese) 司序, 谭桂菊. 探讨肿瘤标志物CEA、AFP、CA199在肝癌诊断中的应用价值[J]. 吉林医学, 2008, 29(16): 1392-1393.
[5] TIAN MF, HAN B. The clinical value of the detections of CA199,CA125,CA153 and CEA in malignant tumors[J]. J Clin Exp Med, 2010, 9(7): 483-485. (in Chinese) 田满福, 韩波. 检测CA199、CA125、CA153及CEA在肿瘤诊断中的意义[J]. 临床和实验医学杂志, 2010, 9(7): 483-485.
[6] ZHANG N, WANG YX, HU J, et al. Application of levels of serum CA199,C3,C4 and lipid metabolism in clinical diagnosis of pancreatic cancer[J]. J Jilin Univ: Med Edit, 2016, 42(2): 295-300. (in Chinese) 张宁, 王颖娴, 胡健, 等. 血清CA199、C3、C4及脂类代谢水平在胰腺癌临床诊断中的应用[J]. 吉林大学学报, 2016, 42(2): 295-300.
[7] GUO HM. Value of measurement of serum CA199 levels for diagnosis of hepatocirrhosis and carcinoma of liver[J]. J Radioimmunol, 2003, 16(4): 207-208. (in Chinese) 郭红梅. 血清CA199在肝硬化与肝癌诊断中的价值[J]. 放射免疫学杂志, 2003, 16(4): 207-208.
[8] HUANG HT, ZHANG XF. CA199 Clinical significance of carbohydrate antigen 199 in liver cirrhosis and liver cancer[J]. J Clin Hepatol, 2006, 22(5): 379-380. (in Chinese) 黄海涛, 张筱风. CA199 在肝硬化和肝癌中的临床意义[J]. 临床肝胆病杂志, 2006, 22(5): 379-380.
[9] DONG JZ, DENG ZY, ZHANG F, et al. Diagnostic value of combined detection of AFP,CEA and CA199 in primary liver cancers[J]. Med J Natl Defend Forces Northwest China, 2011, 32(4): 276-277. (in Chinese) 董菊子, 邓芝云, 张峰, 等. AFP、CEA 和CA199 联合检测在原发性肝癌诊断中的应用[J]. 西北国防医学杂志, 2011, 32(4): 276-277.
[10] ZHU W, GE JL, ZHANG LQ, et al. Clinical value of combined determination of alpha-fetoprotein, carcinoembryonic antigen, carbohydrate antigen 199, and cancer antigen 125 in diagnosis of liver cancer and liver cirrhosis[J]. Int J Lab Med, 2012, 33(15): 1902-1904. (in Chinese) 朱薇, 葛君琍, 张利强, 等. AFP、CEA、CA199、CA-125联合检测对肝癌、肝硬化诊断的临床价值[J]. 国际检验医学杂志, 2012, 33(15): 1902-1904.
[11] MEI Y, PENG CJ, CHEN L, et al. Early detective value of serum CA199 levels for concomitant acute cholangitis in obstructive jaundice[J]. Chin J Pract Surg, 2015, 35(4): 445-447. (in Chinese) 梅永, 彭瓷军, 陈丽, 等. 血清CA199早期预判梗阻性黄疸发生急性胆管炎临床价值研究[J]. 中国实用外科杂志, 2015, 35(4): 445-447.
[12] RUAN SL, BI J. Influence of liver function on the detection of common tumor markers[J]. World Chin J Dig, 2008, 16(24): 2780-2784. (in Chinese) 阮水良, 毕军. 肝功能生化指标对常用肿瘤标志物检测的影响[J]. 世界华人消化杂志, 2008, 16(24): 2780-2784.
[13] XIN WJ, ZHAO WJ. Combined detection of GP73, AFP and CA-199 in the diagnosis of primary liver cancer[J]. Mod Oncol, 2016, 24(7): 1083-1084. (in Chinese) 辛文娟, 赵文静. GP73、AFP、CA-199联合检测在原发性肝癌诊断中的应用价值[J]. 现代肿瘤医学, 2016, 24(7): 1083-1084.
[14] ZHENG HL, ZHAO R, LI DP, et al. Utility of DCP and AFP in diagnosis of primary liver cancer[J]. Chin J Gen Prac, 2016, 14(1): 29-31. (in Chinese) 郑海伦, 赵睿, 李大鹏, 等. 肿瘤标志物DCP和AFP在原发性肝癌中的诊断价值[J]. 中华全科医学, 2016, 14(1): 29-31.
[15] ASUM N, CHOWDHURY HUA, CHOWDHURY MR, et al. Correlation of serum alpha-fetoprotein (AFP) level with liver function parameters in hepatitis B virus (HBV) infected patients in Bangladeshi population[J]. IntJBiosci, 2012, 2(9): 13-19.
引证本文:LI JY, SONG JY, WANG JF, et al. Value of combined detection of AFP, CA19-9, and CEA in early diagnosis of primary liver cancer[J]. J Clin Hepatol, 2017, 33(7): 1291-1295. (in Chinese) 李嘉妍, 宋金云, 王建芳, 等. AFP、CA19-9、CEA联合检测对原发性肝癌的早期诊断价值[J]. 临床肝胆病杂志, 2017, 33(7): 1291-1295.
(本文编辑:王 莹)
Value of combined detection of AFP, CA19-9, and CEA in early diagnosis of primary liver cancer
LIJiayan,SONGJinyun,WANGJianfang,etal.
(ClinicalResearchCenter,TheSecondAffiliatedHospitalofSoutheastUniversity,Nanjing210003,China)
Objective To investigate the value of combined measurement of alpha-fetoprotein (AFP), carbohydrate antigen 19-9 (CA19-9), and carcinoembryonic antigen (CEA) in the early diagnosis of primary liver cancer. Methods A total of 248 patients who visited the outpatient service or were hospitalized in The Second Hospital of Nanjing from October 2014 to December 2016 were enrolled and divided into primary liver cancer group with 88 patients and non-tumor liver disease group with 160 patients. A total of 130 healthy subjects who underwent physical examination were enrolled as normal control group. The Roche cobas e 411 analyzer was used to measure the serum levels of the tumor markers AFP, CA19-9, and CEA, and the sensitivities and specificities of these markers or a combination of them were analyzed. Beckman Coulter AU5800 was used to measure biochemical parameters for liver function, and Biotek ELX808 was used to measure hepatitis B virus markers and HCV antibody. The receiver operating characteristic (ROC) curve was used to analyze the results of measurements of serum AFP, CA19-9, and CEA alone or in combination in patients with primary liver cancer. A one-way analysis of variance was used for comparison of continuous data between multiple groups and the SNK-qtest was used for further comparison between two groups; thet-test was used for comparison of continuous data between two groups. The chi-square test was used for comparison of categorical data between groups. The Spearman correlation analysis was also performed. Results In the primary liver cancer group and the non-tumor liver disease group, the patients with abnormal liver function had significantly higher levels of AFP and CA19-9 than those with normal liver function (primary liver cancer group:t=35.64 and 3.38, bothP<0.05; non-tumor liver disease group:t=12.51 and 8.19, bothP<0.05). Among the patients with normal liver function, the primary liver cancer group had a significantly higher level of CEA than the non-tumor liver disease group and the normal control group (allP<0.05). Among the patients with abnormal liver function, the primary liver cancer group had significantly higher levels of AFP, CA19-9, and CEA than the non-tumor liver disease group and the normal control group (allP<0.05). The serum levels of AFP, CA19-9, and CEA increased with the increase in Child-Pugh class. Among the patients with abnormal liver function in the primary liver cancer group, Child-Pugh class B patients had significant increases in the levels of AFP, CA19-9, and CEA compared with Child-Pugh class A patients, and Child-Pugh class C patients had significant increases compared with Child-Pugh class B patients (allP<0.05). Among the patients with abnormal liver function in the non-tumor liver disease group, Child-Pugh class B patients had significant increases in the levels of AFP and CA19-9 compared with Child-Pugh class A patients, and Child-Pugh class C patients had significant increases compared with Child-Pugh class B patients (allP<0.05); Child-Pugh class C patients had a significant increase in the level of CEA than Child-Pugh class A/B patients (P<0.05). The primary liver cancer group had significantly higher positive rates of AFP, CA19-9, and CEA than the non-tumor liver disease group and the normal control group (allP<0.05), and the positive rates of these tumor markers were significantly higher when measured in combination than when measured alone (allP<0.05). In the primary liver cancer group, a combination of the three tumor markers had a sensitivity of 86.36% and a specificity of 92.35%, while AFP, CA19-9, and CEA measured alone had sensitivities of 71.59%, 52.27%, and 39.77%, respectively. In the patients with primary liver cancer, the areas under the ROC curve for serum AFP, CA19-9, CEA, and a combination of them were 0.776, 0.704, 0.681, and 0.817, respectively. AFP was positively correlated with gamma-glutamyl transpeptidase in the primary liver cancer group (r=0.54,P=0.04) and was positively correlated with indirect bilirubin (IBil) in the normal control group (r=0.50,P=0.01). In the primary liver cancer group, CA19-9 was positively correlated with alanine aminotransferase (ALT), direct bilirubin (DBil), IBil, total bilirubin (TBil), and total bile acid (TBA) (r=0.58, 0.63, 0.61, 0.65, and 0.58, allP<0.05), and in the non-tumor liver disease group, CA19-9 was positively correlated with ALT, alkaline phosphatase (ALP), DBil, IBil, TBil, and TBA (r=0.51, 0.63, 0.66, 0.64, 0.70, and 0.59, allP<0.05). Conclusion AFP can well reflect liver injury, but it may yield false-negative results in the diagnosis of primary liver cancer. A mild increase in CEA does not strongly indicate primary cancer. CA19-9 is easily influenced by the factors including ALP and bilirubin and has a high false-positive rate. Combined measurement of AFP, CA19-9, and CEA can improve the sensitivity of the diagnosis of primary liver cancer and is better than single measurement of AFP, CA19-9, or CEA. Therefore, it provides a strong basis for early diagnosis and treatment.
liver neoplasms;alpha-fetoproteins;CA-19-9 antigen;carcinoembryonic antigen;diagnosis
10.3969/j.issn.1001-5256.2017.07.017
2016-12-01;
2017-01-22。
李嘉妍(1988-),女,主要从事肝炎分子生物学相关研究。
吴旭平,电子信箱:xuping_wu@yahoo.com。
R735.7
A
1001-5256(2017)07-1291-05
猜你喜欢
肝博士(2022年3期)2022-06-30
肝博士(2022年3期)2022-06-30
浙江临床医学(2022年2期)2022-03-19
中国医学影像技术(2020年12期)2021-01-18
中西医结合肝病杂志(2020年2期)2020-10-27
天津医科大学学报(2019年6期)2019-08-13
中国生物医学工程学报(2017年6期)2017-02-10
中国卫生标准管理(2015年1期)2016-01-14
中国药业(2014年12期)2014-06-06
疑难病杂志(2014年12期)2014-04-16
