
桡骨干骺端骨折交叉克氏针固定后骨不连影响因素分析
2017-08-01 00:05:18史立伟张立军赵群李祁伟王恩波李连永
中国骨与关节杂志 2017年7期
史立伟 张立军 赵群 李祁伟 王恩波 李连永
桡骨干骺端骨折交叉克氏针固定后骨不连影响因素分析
史立伟 张立军 赵群 李祁伟 王恩波 李连永
目的 探讨桡骨干骺端骨折患儿的治疗方法,分析甲状旁腺亢进对骨不连可能影响因素的分析。方法 分别对既往治疗的桡骨骨不连和桡骨远侧干骺端骨折患儿进行回顾性分析。2 0 1 2 年 6 月至 2 0 1 4年 6 月治疗的新鲜桡骨远侧干骺端骨折患儿 4 9 例,男 4 0 例,女 9 例;治疗年龄平均 8.9 岁,4 6 例采用闭合复位克氏针内固定术,3 例采用切开复位克氏针内固定术。1 1 例采用双枚克氏针髓腔内贯穿固定 ( A 组 ),1 1 例采用单枚克氏针髓腔内贯穿固定 ( B 组 ),2 3 例采用双针固定,其中 1 枚克氏针髓腔内贯穿固定和 1 枚克氏针交叉固定 ( C 组 ),4 例采用双枚克氏针交叉固定 ( D 组 )。4 9 例均获得随访,随访时间平均为 8.6 ( 6~4 8 ) 个月,按 H e r t e l 的骨折愈合评价标准,其中 4 8 例骨折完全愈合,1 例发生骨不连,此 1 例与其余 2 例( 在外院首次治疗,到我科治疗时,已确诊为骨不连 ) 作为桡骨骨不连组 ( E 组 )。骨不连患儿为 3 例,均采用了切开复位、交叉克氏针内固定术,术后 6 个月骨折线处仍没有骨痂形成,诊为骨不连。所有骨不连患儿均采用了切开复位、自体髂骨移植、钢板固定术,术后石膏固定,拆石膏后患肢逐渐负重锻炼。术后定期随访2 年。术后随访与桡骨远侧干骺端骨折患儿相同。分析所有患儿的临床资料、影像学诊断、治疗方式和治疗结果。采用 S P S S 1 9.0 统计软件包进行数据处理,采用 χ2检验和 t 检验进行组间差异比较。结果 此 3 例骨不连患儿,均获得随访。其中 1 例术后 7 个月又发生了骨不连,再次手术治疗骨不连前化验提示甲旁亢,二次手术采用了切开复位、自体髂骨移植和髓内固定的方法,同时于内分泌科给予药物治疗甲旁亢,最终骨不连在第 2 次术后 6 个月愈合。其余 2 例没有骨生长代谢相关疾病,在术后 2.5 个月骨折处完全愈合。此 4 9 例新鲜干骺端骨折患儿均获得随访,平均随访时间为 8.6 个月,其中 4 8 例骨折完全愈合,1 例发生骨不连,发生在双枚克氏针交叉固定组,其余 3 组均未发生骨不连,其总体有效率为 9 7.9%。有髓内固定物组和无髓内固定物组,采用 χ2检验,差异有统计学意义。提示有髓内固定优于无髓内固定。骨不连患儿与无骨不连患儿的 X 线片对比发现,将其最远骨皮质固定点到骨折线的距离和该点到腕关节距离的比值进行分组比较,采用 t 检验,发现骨不连组比值明显小于无骨不连组,差异有统计学意义。结论 桡骨干骺端骨折切开复位后单纯交叉克氏针的固定需慎重采用,一旦采用交叉克氏针固定,其骨皮质固定点要尽可能的远离骨折线,最远克氏针骨皮质固定点到骨折线的距离和该固定点到腕关节距离的比值尽可能>0.5;一旦骨折切开复位,在患儿局部条件允许的情况下以钢板固定最佳,如果没有安放钢板的条件或者是骨折闭合复位的情况,至少有 1 枚克氏针贯穿髓腔的内固定是必不可少的。骨不连患儿在治疗前要注意骨生长代谢相关疾病的检查,以免在治疗后再发生骨不连。
桡骨;骨折;内固定器;干骺端;骨不连
前臂骨折是儿童骨折中最常见的一种,约占所有儿童骨折的 4 0%,桡骨远端又是前臂骨折最常见的部位,男孩多于女孩,可发生于任何年龄,但最常见于青春期,其中以干骺端骨折最为常见,其次是骺板处骨折[1-2]。前臂骨折治疗方式有多种,大多数学者认同的为闭合复位、单纯石膏固定术[3],但单纯石膏固定至少有 2 1.3% 的再移位率,最高者可达 9 0%,而骨折的再移位很容易导致骨折畸形愈合或骨不连接,因此,为了避免骨折的再移位,克氏针固定已得到很多学者的认可,但目前仍有患儿在使用克氏针内固定之后出现骨不连[1-2,4]。
2 0 1 2 年至 2 0 1 4 年 6 月,我科经治新鲜桡骨干骺端骨折 4 9 例,3 例桡骨干骺端骨不连患儿,现回顾分析如下。
资料与方法
一、一般资料
本组 4 9 例远端干骺端骨折患儿 ( 受伤时间<2 周 ),男 4 0 例,女 9 例;左侧 2 3 例,右侧2 5 例,双侧 1 例;合并尺骨骨折者 3 9 例。所有患儿均为摔伤或压伤所致,均为低暴力损伤,平均8.9 ( 1.3~1 5 ) 岁,患儿术前均行 X 线片和三维 C T检查。
本组患儿根据克氏针的固定情况,分为双枚克氏针髓腔内贯穿固定组 ( A 组 ) 1 1 例,单枚克氏针髓腔内贯穿固定组 ( B 组 ) 1 1 例;1 枚克氏针髓腔内贯穿固定和 1 枚克氏针交叉固定组 ( C 组 ) 2 3 例( 此 2 3 例双针固定者为 1 枚克氏针髓腔内贯穿固定联合 1 枚克氏针交叉固定 );双枚克氏针交叉固定组( D 组 ) 4 例 ( 图 1~4 );1 例骨不连者与其余 2 例( 在外院首次治疗,到我科治疗时,已确诊为骨不连 ) 作为桡骨骨不连组 ( E 组 )。
本组 4 9 例中 4 8 例术后愈合者根据桡骨髓腔内有无克氏针,分为无髓内固定组 3 例和有髓内固定组 4 5 例。
术后患肢采用长臂石膏固定至少 6 周,石膏拆除后患肢逐渐负重锻炼。术后 3 个月内每 6 周门诊复查 1 次,3 个月后每 3 个月门诊复查 1 次,术后1 年每 6 个月门诊复查 1 次。4 9 例均获 6~4 8 个月随访,平均 8.6 个月,按 H e r t e l 骨折愈合评价标准,其中 4 8 例骨折完全愈合,1 例发生骨不连 ( 表 1 )。
本组 3 例桡骨骨不连患儿均为男性,受伤原因为摔伤,左侧 1 例,右侧 2 例;3 例均合并尺骨骨折,其中 1 例为开放外伤,受伤到首次治疗间隔均未超过 1 2 h。3 例均采用切开复位、交叉克氏针内固定术。3 例分别于术后 6 个月、6 个月、7 个月复诊时诊断为骨不连。3 例均经 X 线片和三维 C T 明确诊断。此 3 例治疗采用切开复位、自体髂骨移植和钢板固定术,术后石膏固定至少 6 周,石膏拆除后患肢逐渐负重锻炼。
二、统计学处理
采用 S P S S 1 9.0 统计软件进行数据分析,采用 χ2检验进行组间疗效比较,采用 t 检验进行组间差异比较,P<0.0 5,差异有统计学意义。经随机设计两总体均数 t 检验,双枚克氏针交叉固定骨不连组与A、B、C、D 四组之间两两比较,P<0.0 5,差异有统计学意义。
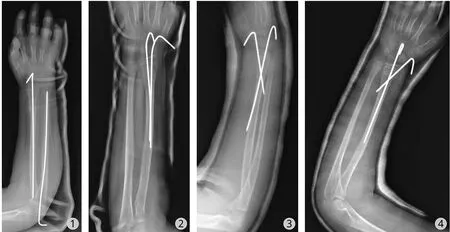
图1 患儿为桡骨远端干骺端骨折采用单枚克氏针髓腔内贯穿固定图2 患儿为桡骨远端干骺端骨折采用双枚克氏针髓腔内贯穿固定图3 患儿为桡骨远端干骺端骨折采用双枚克氏针交叉固定图4 患儿为桡骨远端干骺端骨折采用双枚克氏针固定,1 枚髓腔内贯穿固定和 1 枚交叉固定Fig.1 Patient with distal radius metaphyseal fracture was fixed by single Kirschner wire intramedullary throughFig.2 Patient with distal radius metaphyseal fracture was fixed by double Kirschner wires intramedullary through Fig.3 Patient with distal radius metaphyseal fracture was fixed by double Kirschner wires crossFig.4 Patient with distal radius metaphyseal fracture was fixed by double Kirschner wire with one through and one cross
结 果
3 例骨不连患儿均获得随访。其中 1 例术后7 个月再次发生骨不连,同时发生钢板折断,再次手术前化验提示甲状旁腺素增高。再行手术采用切开复位、自体髂骨移植和髓内固定的方法,同时于内分泌科给予药物治疗甲状旁腺功能亢进,最终骨不连在第 2 次骨不连治疗术后 6 个月愈合。其余2 例由于没有骨生长代谢相关疾病,在切开复位、自体髂骨移植和钢板固定术后 2.5 个月骨折处完全愈合。
4 8 例骨折完全愈合,1 例发生骨不连 ( 表 1 ),发生在双枚克氏针交叉固定组 ( 无髓内固定组 ),其余三组 ( 双枚克氏针髓腔内贯穿固定组、单枚克氏针髓腔内贯穿固定组、1 枚克氏针髓腔内贯穿固定和 1 枚克氏针交叉固定组 ) 均未发生骨不连,其总体有效为 4 8 例,总体有效率为 9 7.9% ( 4 8 / 4 9 ),平均愈合时间为术后 6.8 周。将新鲜桡骨干骺端骨折不同克氏针固定方法进行比较,分为有髓内固定物组和无髓内固定物组,采用 χ2检验进行组间疗效比较,P<0.0 0 5 差异有统计学意义 ( 表 2 )。治疗方法与既往发生骨不连的桡骨干骺端骨折治疗方法相比,明显区别在于髓内固定,在有髓内固定组,其8 周愈合率为 1 0 0% ( 4 5 / 4 5 ),而无髓内固定组,其8 周愈合率为 7 5% ( 3 / 4 ),差异有统计学意义。
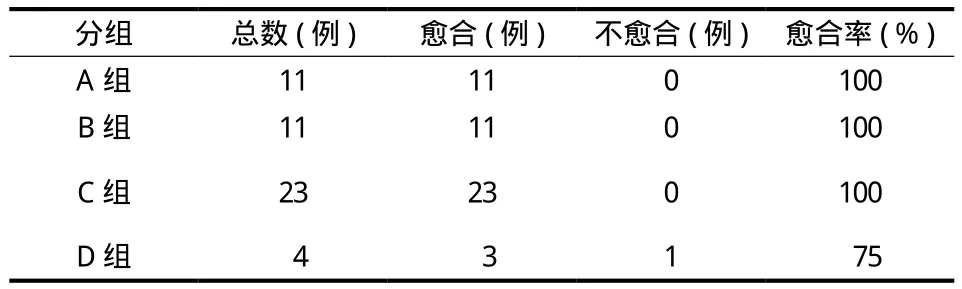
表1 新鲜桡骨干骺端骨折治疗结果Tab.1 Treatment results of fresh distal radius metaphyseal fracture
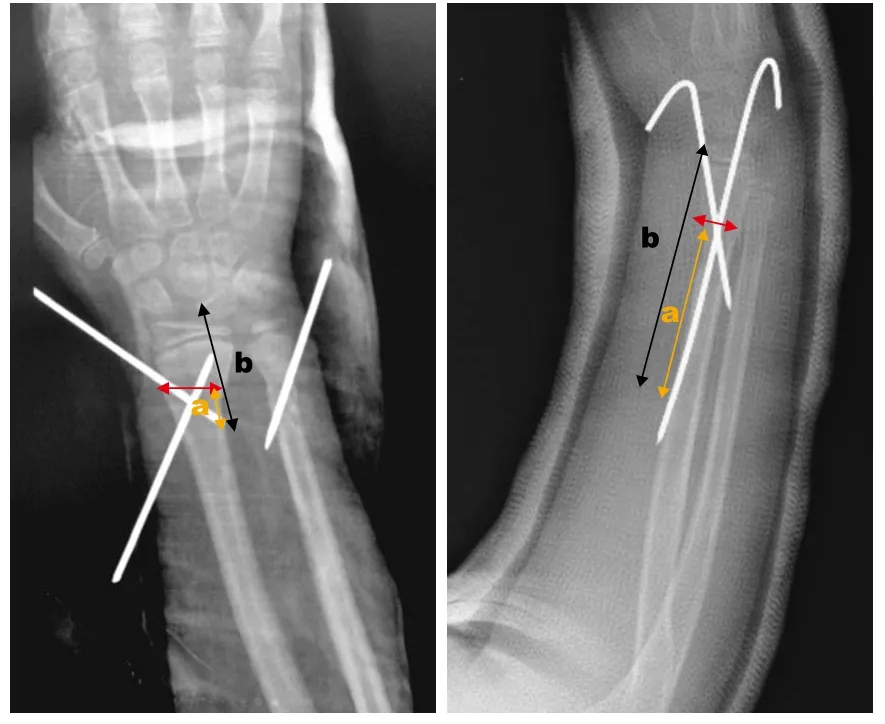
图5 红线代表骨折线,a ( 黄线 ) 代表克氏针最远骨皮质固定点到骨折线的距离,b ( 黑线 ) 代表克氏针最远骨皮质固定点到腕关节的距离。a / b 表示二者的比值,比值越小,对抗拔针的力量越小Fig.5 The red line: the fracture line. a ( yellow line ): the distance from the distal fi xation point to the fracture line; b ( black line ): the distance from the distal fi xation point to the wrist. a / b: the ratio of the distance from the distal fixation point to the fracture line to the distance from the same point to the wrist, and the smaller of the ratio, the less of the strength antagonized the loosening of Kirschner wire
骨不连患儿发生在双枚克氏针交叉固定组 ( 无髓内固定组 ),将骨不连患儿与非骨不连患儿的 X 线片对比发现,发生骨不连者,其克氏针骨皮质固定点距离骨折线过近,这样其抗骨折线移位的力量小,很容易造成固定点的拔针,从而失去克氏针的固定作用。而克氏针骨皮质固定点距离骨折线远者相反( 图 5 );髓内固定组虽没有骨皮质的固定点,但是由于髓腔的限制作用,髓内针的活动范围有限,骨折线的移动范围也有限,因此以上两种情况克氏针的固定作用不易失去。将上述发生骨不连组和无骨不连组之间的克氏针最远骨皮质固定点到骨折线的距离 ( a ) 和克氏针最远骨皮质固定点到腕关节距离 ( b )的比值进行组间比较,采用随机设计两总体均数 t 检验方法,P<0.0 1,发现骨不连组比值 ( a / b ) 明显小于无骨不连组,组间差异有统计学意义 ( 表 3 )。
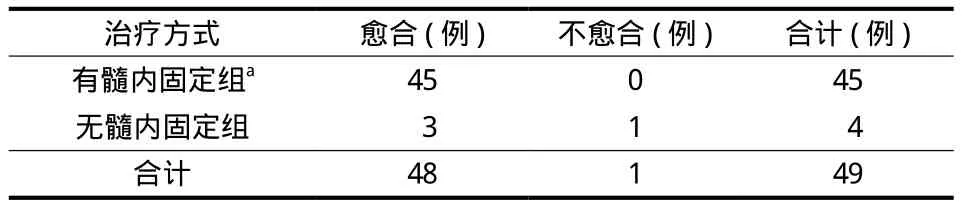
表2 新鲜桡骨干骺端骨折有髓内固定组和无髓内固定组比较Tab.2 Comparison between intramedullary fi xation group and nonintramedullary fixation group for fresh distal radius metaphyseal fracture
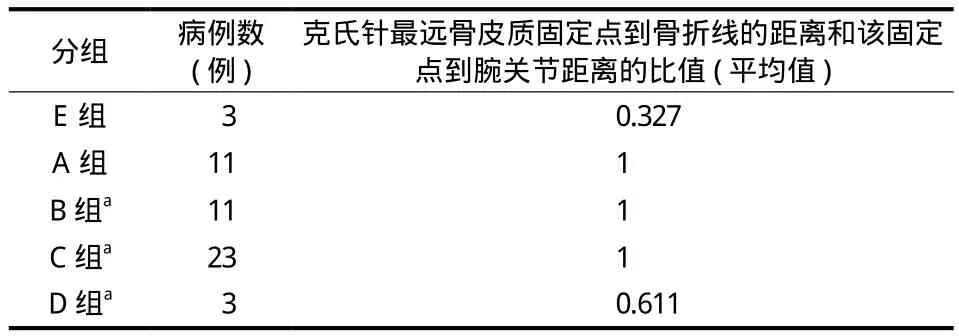
表3 克氏针最远骨皮质固定点到骨折线的距离和该点到腕关节距离的比值表Tab.3 Ratio of the distance from the distal fixation point to the fracture line to the distance from the same point to the wrist
讨 论
前臂骨折最常见的原因是摔倒,其次是运动损伤。8 1% 的患儿年龄>5 岁,高发年龄分别为男孩1 2~1 4 岁,女孩 1 0~1 2 岁。这一时期正是改建塑形的高峰期,桡骨干骺端相对疏松,因此容易在外力作用下发生骨折[1-6]。
桡骨远端干骺端骨折的治疗方法包括单纯制动、闭合复位石膏外固定、闭合复位经皮穿针固定和开放复位。由于桡骨远端干骺端骨折均为不稳定骨折,因此,保持骨折复位后骨折断端的稳定性,是治疗的关键,也是避免桡骨远端干骺端骨折治疗后畸形愈合和骨不连的核心因素。在既往研究中,G i b b o n s 等[7]报告闭合复位后分离移位的桡骨骨折的复位丢失率为 9 1%;M a n i 等[8]认为,开始有移位的桡骨干骨折 5 0% 以上会复位失败,桡骨骨折重新复位率为 2 1.3%;P r o c t o r 等[9]发现,开始有移位的儿童桡骨远端完全骨折,5 2% 会再移位,重新复位率为 2 3.5%;Wi d m a n n 等[10]对需要复位的儿童桡骨远端骨折进行长达 1 年的前瞻性研究发现,3 1% 的患儿发生复位丢失,需进行重新复位和固定,对于年龄 1 0 岁以上、成角>3 0° 的患儿,7 5% 需重新复位;Z a m z a m 等[11]认为最初的完全桡骨骨折是最重要的骨折复位后再移位因素;B o h m 等[12]发现,桡骨骨折复位后残留的成角畸形和骨折复位后再移位有密切关系;M o n g a 等[13]发现,桡骨骨折复位后残留的侧方移位程度和骨折复位后再移位也有密切关系;P r o c t o r 等[9]发现桡骨骨折闭合复位克氏针固定管型石膏制动后,再移位率为 0;M i l l e r 等[4]比较了单纯石膏固定和闭合复位克氏针固定管型石膏制动的结果,发现克氏针固定组没有患儿需要再复位;M c L a u c h l a n 等[14]与其结果类似。因此,桡骨干骺端骨折目前最优的治疗方法还是闭合复位、克氏针固定、管型石膏制动。
在既往研究中,没有关于桡骨干骺端骨折克氏针固定后出现骨不连的报道。但临床工作中桡骨远端骨折交叉克氏针固定后骨不连发生率并不低,本组中的 3 例骨不连患儿分别发生于 2 0 1 0 年、2 0 1 2 年和 2 0 1 3 年,但并没有具体总结相关资料。R o d r i g u e z 等[15-19]认为骨不连的主要原因为:骨折处过度的活动、断端骨折块大、骨折断端血运不佳。分析本文中骨不连发生的可能原因为:( 1 ) 均为干骺端横行骨折,非粉碎性骨折,因此,不存在断端骨折块过大的问题;( 2 ) 最初均采用了切开复位克氏针内固定的方法,因此,局部切开复位对骨折断端血运有一定影响,但这种切开复位对骨折断端的影响有限;( 3 ) 最终又进行了切开复位、自体髂骨移植和钢板固定,获得了骨不连处的愈合,这说明,虽然手术切开局部会损伤骨折处的血运,但要在手术时注意骨折断端局部的血运保护,保证骨折复位后的稳定性,骨不连处易于愈合,需注意再次骨不连的患儿,是否有与骨生长代谢相关的疾病,其对骨骼的生长发育有很大影响。笔者认为手术切开对骨折断端血运的影响有限,本组骨不连的主要原因为:骨折断端的不稳定,即骨折断端的微动。首先,根据对有髓固定组 ( 双枚髓腔内贯穿固定组、单枚髓腔内贯穿固定组、1 枚髓腔内贯穿固定和 1 枚交叉固定组 ) 和无髓固定组 ( 双枚交叉固定组 ) 的骨不连发生率进行比较分析,可见有髓固定组 ( 4 5 例 ) 均未发生骨不连,骨折愈合率 1 0 0%,四组之间愈合率差异明显,可见髓内固定对于预防骨不连的发生是有作用的。其次,根据对 3 例骨不连患儿 X 线片的回顾性分析,可见此类患儿的克氏针最远骨折固定点到骨折线的距离 ( a ) 过近,造成骨不连组克氏针最远骨折固定点到骨折线的距离与该固定点到腕关节距离比值 ( b ) 明显小于有无骨不连组 ( 表 3 ),这样其抗骨折线移位的力量小,并且克氏针局部钻孔产生的热量可以造成针孔周边的骨坏死,上述情况很容易造成固定点的脱针,从而失去克氏针的固定作用,失去克氏针对骨折线的固定和支撑作用,从而出现骨不连。因此,髓腔内克氏针的固定对于减少骨折断端之间的微动和预防骨不连有显著的作用。其主要优点:( 1 ) 贯穿的髓内克氏针虽然没有骨皮质的固定作用,但由于克氏针的髓腔内占位作用和骨髓腔宽度的有限性,使骨折断端之间不会有大的移位,可以限制骨折断端之间的活动范围,有利于骨痂的形成;( 2 ) 贯穿的髓内克氏针的固定力臂长,固定力量可靠,其抗骨折线移位的力量大;( 3 ) 贯穿的髓内克氏针对骨折断端周边的骨皮质没有损伤,因此不存在克氏针钻孔时局部骨质温度过高造成骨坏死的可能,因此不会降低骨骼的强度。其缺点是:贯穿的髓内克氏针由于没有骨皮质的固定作用,因此骨折线处抗旋转的力量小。贯穿的髓内克氏针的固定方法在桡骨不能使用钢板稳定固定的情况下,获得了和桡骨钢板固定相近的结果,均满足了儿童骨折治疗的基本原则之一,即坚强的内固定,因此,桡骨干骺端骨折使用贯穿髓腔的克氏针固定不失为一种好方法,在抗旋转方面,建议再加入 1 枚交叉固定桡骨骨皮质的克氏针,可能结果会更好,但由于病例数有限,具体的结果还需进一步收集资料,并且由于研究对象为人,因此也无法进行直接的生物力学检测,可制作类似的单纯骨骼模型或动物模型来进行直接的生物力学测定,可以使结果更有说服力。
综上所述,新鲜桡骨干骺端骨折后骨不连的发生率很低 ( 1 / 4 9 ),但由于骨不连治疗的困难性和治疗不当造成的灾难性结局,因此如何减少骨不连的发生成为当前的难题。桡骨干骺端骨折切开复位后单纯交叉克氏针的固定仍需慎重采用,一旦采用交叉克氏针固定,其骨皮质固定点要尽可能的远离骨折线,克氏针最远骨皮质固定点到骨折线的距离和该固定点到腕关节距离的比值尽可能>0.5;一旦骨折切开复位,在患儿局部条件允许的情况下以钢板固定为主,如果没有安放钢板的条件或者是骨折闭合复位的情况,至少 1 枚贯穿髓腔的克氏针内固定是必不可少的,如能再加入 1 枚交叉固定骨皮质的克氏针,可能结果会更好。骨不连患儿在治疗前要注意骨生长代谢相关疾病的检查,以免在治疗后又发生骨不连。
[1]Herring JA. Tachdjian’s Pediatric orthopedics: fractures of the distal forearm[M]. 5th ed. Philadelphia: saunders Elsevier. 2014: 1340-1346.
[2]Beaty JH, Kasser JR. Rockwood and wilkins fracture in children: fractures of the distal radius and ulna[M].7th ed. Philadelphia: Lippincott Williams & Wilkins. 2010: 292-338.
[3]Webb GR, Galpin RD, Armstrong DG. Comparison of short and long arm plaster casts for displaced fractures in the distal third of the forearm in children[J]. J Bone Joint Surg Am, 2006, 88(1):9-17.
[4]Miller BS, Taylor B, Widmann RF, et al. Cast immobilization versus percutaneous pin fixation of displaced distal radius fractures in children: a prospective, randomized study[J]. J Pediatr Orthop, 2005, 25(4):490-494.
[5]Hertel R, Pisan M, Lambert S, et al. Plate osteosunthesis of diaphyseal fractures of the radius and ulna[J]. Injury, 1996, 27(8):545-548.
[6]Alemdaroglu KB, Iltar S, Cimen O, et al. Risk factors in redisplacement of distal radius fractures in children[J]. J Bone Joint Surg Am, 2008, 90:1224-1230.
[7]Gibbons CL, Woods DA, Pailthorpe C, et al. The management of isolated distal radius fractures in children[J]. J Pediatr Orthop, 1994, 14(2):207-210.
[8]Mani GV, Hui PW, Cheng JC. Translation of the radius as a predictor of outcome in distal radial fractures of children[J]. J Bone Joint Surg Br, 1993, 75(5):808-811.
[9]Proctor MT, Moore DJ, Paterson JM. Redisplacement after manipulation of distal radial fractures in children[J]. J Bone Joint Surg Br, 1993, 75(3):453-454.
[10]Widmann R, Waters PM, Reeves S. Complications of closed treatment of distal radius fractures in children. Presented at the POSNA annual meeting, Miami, 1995.
[11]Zamzam MM, Khoshhal KI. Displaced fracture of the distal radius in children: factors responsible for redisplacement after closed reduction[J]. J Bone Joint Surg Br, 2005, 87(6):841-843.
[12]Bohm ER, Bubbar V, Yong Hing K, et al. Above and belowthe-elbow plaster casts for distal forearm fractures in children. A randomized controlled trial[J]. J Bone Joint Surg Am, 2006, 88(1):1-8.
[13]Monga P, Raghupathy A, Courtman NH. Factors affecting remanipulation in paediatric forearm fractures[J]. J Pediatr Orthop B, 2010, 19(2):181-187.
[14]McLauchlan GJ, Cowan B, Annan IH, et al. Management of completely displaced metaphyseal fractures of the distal radius in children. A prospective, randomised controlled trial[J]. J Bone Joint Surg Br, 2002, 84(3):413-417.
[15]Rodriguez-Merchan EC, Forriol F. Nonunion: general principles and experimental data[J]. Clin Orthop Relat Res, 2004, (419):4-12.
[16]An YH, Friedman RJ. Animal models in orthopaedic research: animal models of fracture or osteotomy[M]. Boca Raton, Fl: CRC Press. 1999: 197-218.
[17]Cañadell J, Forriol F. The external fi xator in the treatment of infected pseudoarthrosis and bone defects[J]. Osteosynthese Int, 1997, 5:221-225.
[18]Hulth A. Current concepts of fracture healing[J]. Clin Orthop Relat Res, 1989, (249):265-284.
[19]Jupiter JB, First K, Gallico GG 3rd, et al. The role of external fixation in the treatment of posttraumatic osteomyelitis[J]. J Orthop Trauma, 1988, 2(2):79-93.
An analysis of effective factors of nonunion after distal radius metaphyseal fracture with cross Kirschner wirefi xation
SHI Li-wei, ZHANG Li-jun, ZHAO Qun, LI Qi-wei, WANG En-bo, LI Lian-yong. Department of Pediatric
Orthopedics, Shengjing Hospital of China Medical University, Shenyang, Liaoning, 110000, China
Objective To retrospectively study the clinical data of the children with nonunion after distal radius metaphyseal fractures with cross Kirschner wire fixation, and to find the causes and effective factors in the treatment of nonunion. To compare the fi xation methods for both radius nonunion and fresh distal radius metaphyseal fracture, and then to suggest a reliable fi xation method for distal radius metaphyseal fracture. Methods The clinical data of both the children with radius nonunion and those with distal radius metaphyseal fractures were retrospectively analyzed. From June 2012 to June 2014, there were 49 children with fresh distal radius metaphyseal fractures. There were 40 males and 9 females, whose average age was 8.9 years at the time of treatment. Among them, 46 children weretreated by close reduction with Kirschner wire fi xation, and 3 children by open reduction with Kirschner wire fi xation. Eleven patients were treated by double Kirschner wires intramedullary fi xation through ( group A ), 11 patients by single Kirschner wire intramedullary fi xation through ( group B ), 23 patients by double Kirschner wires fi xation with one through and one cross ( group C ), and 4 patients by double Kirschner wires fi xation cross ( group D ). All the 49 patients were followed up for an average of 8.6 months ( range: 6 - 48 months ). According to Hertel’s criteria, bone union had been realized in 48 cases, with 1 case of nonunion. This case and another 2 cases, who were fi rstly treated outside the hospital with nonunion conf i rmed in our hospital, were taken as the radius nonunion group ( group E ). There were 3 patients with nonunion. Open reduction with Kirschner wire fixation were firstly performed. Six months after the operation, there was no bony callus. The diagnosis of radius nonunion was conf i rmed. In the second operation, all the patients were treated by open reduction with plate immobilization and autogenous bone graft in the nonunion. The plaster cast was used after the operation. After removal of the plaster cast, limb weight-bearing exercise gradually began. The patients had the regular follow-up of 2 years, the same as that for the patients with nonunion. The clinical data, imaging diagnosis, treatment methods and outcomes of all the patients were analyzed. All the data were processed by statistical software SPSS19.0, and χ2test and t-test were used to compare the differences among groups. Results The 3 nonunion children were followed up. Radius nonunion occurred again in 1 patient at 7 months after the fi rst surgery. The parathyroid hormone was increased before the second surgery. The therapy of the second surgery was open reduction with intramedullary fixation, and autogenous bone graft in the nonunion, at the same time the hyperparathyroidism was given in the Department of Endocrinology. The fi nal nonunion was cured at 6 months after the second operation. In the remaining 2 patients with no diseases related to bone growth or metabolism, the fi nal nonunion was cured at 2.5 months after the fi rst surgery. The other 49 children with fresh distal radius metaphyseal fractures were followed up. The mean follow-up was 8.6 months. A total of 48 patients were cured, and nonunion occurred in 1 patient. The patient was in the group of 4 patients treated by double Kirschner wires fi xation cross. No patients had nonunion in the other 3 groups. The overall effective rate was 97.9%. The data of intramedullary fi xation group and non-intramedullary fi xation group were compared by χ2test, and there were statistically signif i cant differences. It was presented that intramedullary fi xation was superior to non-intramedullary fi xation. Based on the comparison of X-ray in the patients with nonunion and those without nonunion, the ratio of the distance from the distal fi xation point to the fracture line to the distance from the distal fi xation point to the wrist was calculated. The ratio of nonunion group was obviously lower than that of the union group according to the analysis by t test, and there were statistically signif i cant differences. Conclusions The therapy with cross Kirschner wire fi xation after the open reduction for distal radius metaphyseal fracture should be carefully used. If cross Kirschner wire fi xation will be used, the distal fi xation point should be as far as possible from the fracture line. The ratio of the distance from the distal fi xation point to the fracture line to the distance from the distal fi xation point to the wrist should be 0.5 at least. If the patients with fractures are treated by open reduction, rigid plate fi xation is the best choice in the case of well local conditions. If there are bad local conditions or the patients are treated by close reduction, at least one Kirschner wire intramedullary fi xation through the radius is necessary. We have to pay attention to the diseases related to bone growth and metabolism before operation for the nonunion patients, in order to avoid the occurrence of nonunion after the treatment.
Radius; Fractures, Bone; Internal Fixators; Metaphyseal; Nonunion
10.3969/j.issn.2095-252X.2017.07.006
R726.8, R687.3
2017-03-27 )
( 本文编辑:李慧文 )
1 1 0 0 0 0 沈阳,中国医科大学附属盛京医院 小儿骨科
猜你喜欢
实用手外科杂志(2022年2期)2022-08-31 09:47:38
装备制造技术(2020年4期)2020-12-25 05:26:10
汽车工程学报(2017年2期)2017-07-05 08:13:04
中华骨与关节外科杂志(2016年6期)2016-05-17 06:11:12
汽车零部件(2015年9期)2015-10-25 02:27:48
实用手外科杂志(2015年4期)2015-08-27 01:54:08
实用手外科杂志(2015年3期)2015-08-27 01:53:14
实用手外科杂志(2015年3期)2015-08-27 01:53:14
汽车科技(2015年2期)2015-08-25 05:42:55
医学研究杂志(2015年5期)2015-06-10 06:43:26
