
Prognosis of gestational choriocarcinoma diagnosed incidentally during laparoscopy for a presumed cornual pregnancy: a report of five cases
2017-07-18 11:08ShipingLiuChenchenFanFengzhiFengYangXiangXirunWanTongRenPekingUniversityFirstHospitalBeijing00034ChinaPekingUnionMedicalCollegeHospitalBeijing00730China
Cancer Biology & Medicine 2017年2期
Shiping Liu, Chenchen Fan, Fengzhi Feng, Yang Xiang, Xirun Wan, Tong RenPeking University First Hospital, Beijing 00034, China;Peking Union Medical College Hospital, Beijing 00730, China
Prognosis of gestational choriocarcinoma diagnosed incidentally during laparoscopy for a presumed cornual pregnancy: a report of five cases
Shiping Liu1, Chenchen Fan2, Fengzhi Feng2, Yang Xiang2, Xirun Wan2, Tong Ren21Peking University First Hospital, Beijing 100034, China;2Peking Union Medical College Hospital, Beijing 100730, China
The clinical presentations of gestational choriocarcinoma vary markedly, and a misdiagnosis could be made in atypical patients if simply relying on clinical features. Laparoscopic resection of uterine mass lesion is rarely used in gestational choriocarcinoma diagnosis because of the fear of heavy blood loss and distant metastasis. Five patients who were preoperatively diagnosed as having cornual pregnancy underwent laparoscopic resection of mass lesion and then proved to have gestational choriocarcinoma based on pathological examinations. Chemotherapy was started within two days after surgery, and the rate of complete remission was 100%. The mean follow-up time was 29.8±19.1 months, and no patient showed signs of relapse. Laparoscopic resection of uterine mass followed by timely postoperative chemotherapy may be an effective and safe way to obtain pathologic results in patients with suspected gestational choriocarcinoma.
Gestational choriocarcinoma; cornual pregnancy; laparoscopy
Introduction
The clinical presentations of gestational choriocarcinoma vary markedly and may overlap with other conditions, such as ectopic pregnancies or retained products of conception. On certain occasions, a misdiagnosis could be made if simply relying on clinical features1,2, and a pathologic confirmation is indicated. Curettage is usually performed in these conditions, but with limited success. Given the fear of heavy blood loss and distant metastasis, laparoscopic resection of uterine mass lesions is rarely used in gestational choriocarcinoma diagnosis. In this article, we report five gestational choriocarcinoma patients who had undergone such resections.
Case report
This report includes five patients who were preoperatively diagnosed as having cornual pregnancy. The patients underwent laparoscopic resection of mass lesion and then proved to have gestational choriocarcinoma based on pathological examinations between 2010 and 2014. Approval by the Institutional Review Board of Peking Union Medical College Hospital was obtained in advance. All patients, with no self-reported history of molar pregnancy, presented with irregular vaginal bleeding, elevated hCG, and ultrasound of mass located in the right or left cornus of the uterus. The mean age of the patients at diagnosis was 34.6±9.6 years. The mean gravida and parity were 3.0±2.1 and 1.2±0.8 times, respectively. The mean preoperative hCG was 47930.6± 25128.3 mIU/mL. The mean size of mass was 2.9±1.1 cm in maximum diameter, with four cases showing moderate to marked vascularity. All cases had received preoperative chest radiography, and two patients had a suspected lung lesion (a small amount of pleural effusion or slight pleural thickening).
The laparoscopy demonstrated enlargement of the uterine cornual area in all patients (Figure 1). After incision of the myometrium, the mass lesions, which are located mainly in the myometrium, were exposed. Wedge resection of mass lesions and intraoperative frozen pathology were then performed. The results of pathological examinations were as follows: myometrium invaded by atypical trophoblast with absence of chorionic villi (Figure 2). Based upon the pathologic outcomes, all patients were diagnosed as having gestational choriocarcinoma. The average operation time and blood loss were 75±23.8 min and 192±148 mL, respectively.

Figure 1 Representative laparoscopic images. Laparoscopy showed enlargement of the uterine cornual area in case 1 (A) and case 2 (B).

Figure 2 Representative histological images. Histological examinations showed myometrium invaded by atypical trophoblast with absence of chorionic villi in case 1 (A) and case 2 (B) (H&E staining, 200×).
No new distant metastases were observed postoperatively. All patients received standard chemotherapy, based on their pathologic diagnosis, International Federation of Gynecology and Obstetrics (FIGO) stage, and prognostic scoring. The mean cycles of chemotherapy were 4.9±1.1. One patient received hysterectomy for persistent uterine mass during the third cycle of chemotherapy, and pathological examination showed necrosis with absence of trophoblast. The rate of complete remission was 100%. All patients were followed up by monitoring β-hCG. The mean follow-up time was 29.8±19.1 months, and no patient showed signs of relapse, with β-hCG<5 mIU/mL. Details of the reported cases are shown in Table 1.
Discussion
The presence of sensitive quantitative assays for hCG enables gestational choriocarcinoma to be diagnosed clinically even when definitive pathology is unavailable3. However, to avoid misdiagnosis, a histologic confirmation is required on certain occasions because the clinical features of gestational choriocarcinoma may overlap with ectopic pregnancy or retained products of gestation, especially in patients with gestational choriocarcinoma following a non-molar pregnancy. At present, curettage is usually performed to obtain biopsies, but it has a limited role in patients with uterine mass located in the cornual area. A more effective method is needed.
Resection of uterine mass has been performed in gestational choriocarcinoma patients with chemotherapy resistant disease; promising results are shown4. However, its use in gestational choriocarcinoma diagnosis remains controversial, with only several cases reported in the literature5,6. The main reason for its limited use is the fear of heavy blood loss and distant metastasis. In our study, laparoscopic resection of uterine mass was performed to remove the products of presumed cornual pregnancy, and the diagnosis of gestational choriocarcinoma was made incidentally. By analyzing the clinical data of these patients, we found that laparoscopic resection of uterine mass followed by timely chemotherapy may be a safe way to obtain pathologic confirmation of gestational choriocarcinoma, with no perioperative complications and new distant metastases observed. Furthermore, all these patients responded well to chemotherapy and showed no signs of relapse during follow-up.
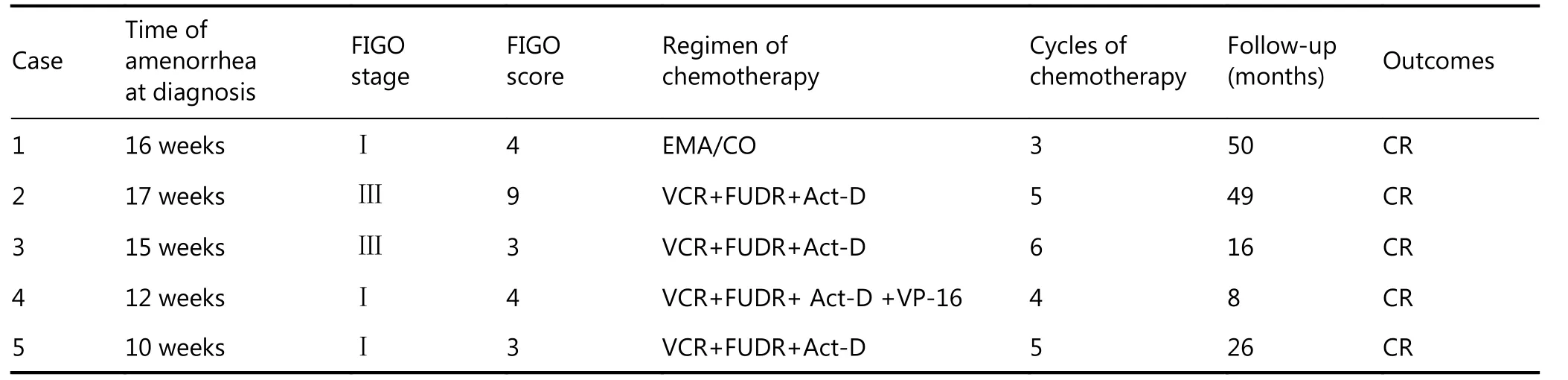
Table 1 Details of the reported cases
In conclusion, laparoscopic resection of uterine mass followed by postoperative chemotherapy may be an effective and safe method to obtain pathologic results in gestational choriocarcinoma patients with atypical presentations. Given the small sample size, further studies are warranted to investigate the role of uterine mass resection in gestational choriocarcinoma diagnosis.
Acknowledgments
This work was supported by a grant of Beijing Municipal Science & Technology Commission, China (Grant No. Z131107002213173).
Conflict of interest statement
No potential conflicts of interest are disclosed.
1.Tan AP. Degenerated retained product of conception misdiagnosed as invasive trophoblastic disease. Med J Malaysia. 2015; 70: 100-1.
2.Qian JH, Ye DF, Xie X. Clinical analysis of 13 cases of gestational trophoblastic tumor misdiagnosed as ectopic pregnancy. Chin J Obstetr Gynecol. 2005; 40: 91-4.
3.Goldstein DP, Berkowitz RS. Current management of gestational trophoblastic neoplasia. Hematol Oncol Clin North Am. 2012; 26: 111-31.
4.Lurain JR. Management of high-risk gestational trophoblastic disease. J Reprod Med. 1998; 43: 44-52.
5.Rotas M, Khulpateea N, Binder D. Gestational choriocarcinoma arising from a cornual ectopic pregnancy: a case report and review of the literature. Arch Gynecol Obstet. 2007; 276: 645-7.
6.Venturini PL, Gorlero F, Ferraiolo A, Valenzano M, Fulcheri E. Gestational choriocarcinoma arising in a cornual pregnancy. Eur J Obstet Gynecol Reprod Biol. 2001; 96: 116-8.
Cite this article as: Liu S, Fan C, Feng F, Xiang Y, Wan X, Ren T, et al. Prognosis of gestational choriocarcinoma diagnosed incidentally during laparoscopy for a presumed cornual pregnancy: a report of five cases. Cancer Biol Med. 2017; 14: 191-3. doi: 10.20892/j.issn.2095-3941.2017.0004
Fengzhi Feng
E-mail: fengfzh@pumch.cn
January 7, 2017; accepted February 7, 2017.
Available at www.cancerbiomed.org
Copyright © 2017 by Cancer Biology & Medicine
 Cancer Biology & Medicine2017年2期
Cancer Biology & Medicine2017年2期
- Cancer Biology & Medicine的其它文章
- Developmental pathways associated with cancer metastasis: Notch, Wnt, and Hedgehog
- Cellular immunity augmentation in mainstream oncologic therapy
- Mesenchymal stromal cells’ role in tumor microenvironment: involvement of signaling pathways
- Simplified microsatellite instability detection protocol provides equivalent sensitivity to robust detection strategies in Lynch syndrome patients
- Significance of stromal-1 and stromal-2 signatures and biologic prognostic model in diffuse large B-cell lymphoma
- Immunohistochemical evaluation of vitamin D receptor(VDR) expression in cutaneous melanoma tissues and four VDR gene polymorphisms