
食管癌三野淋巴结清扫术中胸内吻合的应用及其临床价值
2017-06-05 15:01周晓琪张海峰
实用癌症杂志 2017年4期
周晓琪 张海峰
食管癌三野淋巴结清扫术中胸内吻合的应用及其临床价值
周晓琪 张海峰
目的 研究胸内吻合方法在食管癌三野淋巴结清扫术中的应用以及胸内吻合方法的临床价值。方法 随机选取行食管癌治疗的患者97例,其中颈部吻合组82例,胸内吻合组15例。比较2种吻合方式下吻合口瘘的发生及其手术相关情况。结果 2组手术时间、淋巴结清扫数量、失血量等方面无统计学差异(P>0.05)。胸内吻合方法可显著降低食管癌三野淋巴结清扫手术后吻合口瘘的发生概率,发生吻合口瘘的概率与颈部比较,吻合组显著降低(3.22% vs.20.55%,P=0.015)。结论 食管癌三野淋巴结清扫术中采用胸内吻合能显著降低吻口瘘发生率,并且胸内吻合也没有对手术时间、清扫淋巴结的数量、手术失血情况等术中临床状况造成影响。
食管癌;三野淋巴结清扫术;胸内吻合;颈部吻合
(ThePracticalJournalofCancer,2017,32:609~612)
食管癌是常见的恶性肿瘤之一,同时也是死亡率较高的一种疾病,而我国又是一个食管癌的高发地区,据统计我国每年的食管癌发病人数和死亡人数高达20多万[1-2]。目前治疗食管癌的首选方法就是进行外科手术[3-6],其中颈胸腹三野淋巴结清扫术手术较彻底,但创伤较大,并且手术后容易发生各种并发症,其中吻合口瘘是最常见也是较严重的一种术后并发症[7-8]。食管癌三野淋巴结清扫手术中消化道重建一般采用颈部吻合,这是因为手术中颈部的切口暴露较好,手术难度低,可切除更长的病灶上方食管,但是术后吻合口瘘的发生率较高,而二野淋巴结清扫右胸内食管胃吻合,其术后吻合口瘘的出现率要低。基于以上观点,我们对食管癌三野淋巴结清扫术选择性采用右胸顶吻合,现报告如下。
1 资料与方法
1.1 研究对象
随机选取2010年1月至2015年12月期间入如皋市人民医院接受食管癌根治手术的97例患者。我们实施三野淋巴结清扫术的患者,必须满足以下条件之一:①在患者的食管中已经发现肿瘤细胞;②发现锁骨上的淋巴结部位开始肿大,并可进行清扫手术;③发现食管和气管旁边的淋巴结开始转移。根据以上标准在我们所选的97位接受了食管癌三野淋巴结清扫食管癌根治术的患者中,有15例患者手术时采用右胸顶吻合的方法,82例患者采用了传统的颈部吻合的方法。表1是2组患者的临床资料情况。
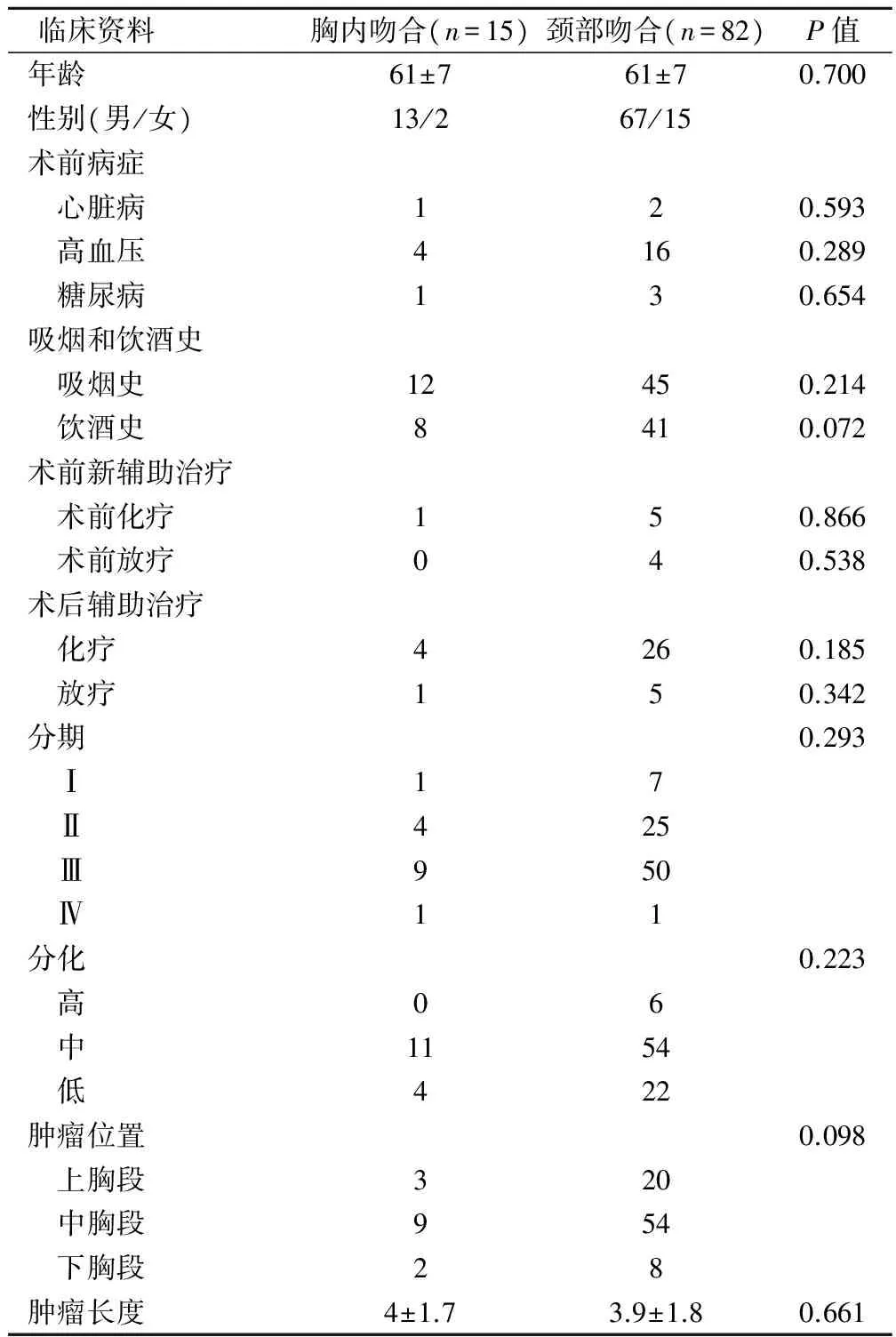
表1 2组临床病理资料
1.2 手术方法
2组均采用双腔气管插管,静吸复合全麻。颈部吻合组:颈部衣领状切口清扫气管食管旁沟(喉返神经旁)、双侧锁骨上及颈内静脉旁淋巴结后缝合切口。胸内吻合组:经上腹部正中切口进腹,游离胃、离断贲门,并用一次性切割缝合器切割缝合,制成管状胃,并清扫贲门旁、胃小弯、胃大弯、胃左动脉旁、腹腔动脉旁及肝总动脉旁淋巴结,用丝线将管状胃近端与食管远端连接,缝合腹部切口。取左侧卧位,选择右胸前外侧第4根肋间手术切口,行肿瘤切除和切除后的淋巴结清扫,特别把喉返神经链周围的淋巴作为重点清扫对象,离断近端食管,将管状胃通过膈肌裂孔拉入胸腔,将食管与胃在右胸顶行端侧器械吻合,送入胃管,放置引流后关胸。
1.3 研究方法
1.3.1 吻合口瘘的诊疗 如果患者在手术后的3天后依然存在不明原因的发烧,在排除掉临床肺炎以及手术伤口感染等原因之后,对于发生的消化道瘘,我们会给予相应检查,如果检查结果中任何一项呈阳性,则被认定是吻合口瘘症。一旦患者确诊为消化道瘘,除了对其加强抗感染和营养支持治疗外,需要打开颈部切口,放置引流处理;胸内吻合口瘘进行相应的冲洗引流治疗。
1.3.2 患者术后服务 在患者吻合口瘘痊愈后每隔30~90天进行一次康复检查,1年后改为每隔半年复查1次,包括胸腹部B超、CT和消化道造影等常规检查,借助患者资料,我们通过电话联系以获得患者术后情况。
1.4 统计方法
采用SPSS20.0软件,应用t检验或U检验来分析连续性变量,卡方检验或Fisher确切概率法用来分析分类变量,P<0.05为差异有统计学意义。
2 结果
2.1 2组效果比较
只有1例患者进行了第2次手术,也只有1例患者死亡,并且死亡患者出现在颈部吻合组。2组患者在手术后出现了一些并发症,但是胸部吻合组出现并发症的几率要小。手术过程中和术后相关具体情况见表2。2组吻合口瘘发生率差异有统计学意义(P<0.05);手术相关情况比较无统计学意义(P>0.05)。

表2 手术过程中和术后相关情况
2.2 吻合口瘘的诱发因素分析
为了找出诱发吻合口瘘的原因,本文又进行了更具体的分析,单因素和多因素分析。单因素中颈部吻合口瘘与吻合位置有关,而在多因素分析中,发现吻合口瘘不仅与吻合口位置有关,还与吻合方式、总淋巴结清扫数有关,肿瘤大小不会对吻合口瘘产生影响,见表3。

表3 诱发吻合口瘘的可能性因素
2.3 2组生存率比较
在后期随访中,胸内吻合组和颈部吻合组患者的术后第1年存活率分别为79.3% vs.81.8%,第2年存活率分别为61.2% vs.70.7%,第3年存活率分别为61.2% vs.65.6%。术后2组患者存活率差异无统计学意义(P>0.05)。
3 讨论
采用三野淋巴结清扫术治疗食管癌在上个世纪已被临床应用,但是人们对其疗效褒贬不一[9-13]。经过一段时间的发展和手术改良,食管癌三野淋巴结清扫术确实可以给患者带来不少临床受益,如:术后患者复发率降低、术中患者死亡率较低、术后并发症降低,因此该手术被越来越多的应用到临床对食管癌的治疗中[14-17]。然而食管癌三野淋巴结清扫术也存在一个一直困扰人们的问题,就是吻合口瘘的出现没有得到有效控制,且有较高的发生率,而二野淋巴结清扫右胸内食管胃吻合,其术后吻合口瘘的发生较低。
本研究为了使得在配对后,2个对照组的患者在性别、年龄、肿瘤分期、手术前合并症以及手术后辅助治疗等多项因素的9个变量中的分布尽量趋向一致,本文在配对时,选择采用倾向性评分的方法,胸内吻合能够显著降低手术之后吻合口瘘发生的概率(95% CI =0.011~0.833,P=0.033)。吻合位置的差异是本文在食管癌三野淋巴结清扫手术中所采用的两种吻合方式最大的差别[18-20]。本研究的缺点之一便是胸内吻合组病例数量比较少,2个对比组病例数量不均衡,同时作为一项回顾性研究,本文也出现了不可避免的选择性偏倚。所以为了对各类混杂因素予以平衡,本文选择采用了倾向性评分标准,使得本研究对象是否接受处理因素时是完全随机的,以此来增强研究结果的说服力。
综上所述,食管癌三野淋巴结清扫术中采用胸内吻合能降低吻合口瘘发生率,并且胸内吻合也没有对手术时间、清扫淋巴结的数量、手术失血等术中临床状况造成影响。
[1] Fernández J,Gustot T.Management of bacterial infections in cirrhosis〔J〕.J Hepatol,2012,56(4):1-12.
[2] Li H,Yang S,Zhang Y,et al.Thoracic recurrent laryngeal lymphnode metastases predict cervical node metastases and benefit from three-field dissection in selected patients with thoracic esophageal squamous cell carcinoma〔J〕.J Surg Oncol,2012,105(6):548-552.
[3] Li B,Chen H,Xiang J,et al.Pattern of lymphatic spread in thoracic esophageal squamous cell carcinoma:A single-institution experience 〔J〕.J Thorac Cardiovasc Surg,2012,144(4):778-85.
[4] Shim YM,Kim HK,Kim K,et al.Comparison of survival and recurrence pattern between two-field and three-field lymph node dissections for upper thoracic esophageal squamous cell carcinoma〔J〕.J Thorac Oncol,2015,5(2):707-712.
[5] Asteriou C,Barbetakis N,Lalountas M,et al.Modified pleural tenting for prevention of anastomotic leak after Ivor Lewis esophagogastrectomy〔J〕.Ann Surg Oncol,2015,18(13):3737-42.
[6] Linnemann B,Lindhoff-Last E.Risk factors,management and primary prevention of thrombotic complication-s related to the use of central venous catheters〔J〕.Vasa,2012,41(5):319-32.
[7] 贲晓松,陈 刚,唐继鸣,等.食管-胃颈部侧侧机械吻合法在三切口食管癌切除术中的应用〔J〕.中国癌症杂志,2010,20(2):130-132.
[8] Mine S,Udagawa H,Tsutsumi K,et al.Colon interposition after esophagectomy with extended lymphadenectomy for esophageal cancer〔J〕.Ann Thorac Surg,2015,88(5):47-53.
[9] Wang WP,Gao Q,Wang KN,et al.A prospective randomized controlled trial of semi-mechanical versus hand-sewn or circular stapled esophagogastrostomy for prevention of anastomotic stricture〔J〕.World J Surg,2013,37(5):43-50.
[10] Merritt RE,Whyte RI,D'Arcy NT,et al.Morbidity and mortality after esophagectomy following neoadjuvant chemoradiation〔J〕.Ann Thorac Surg,2014,92(6):34-40.
[11] Saluja SS,Ray S,Pal S,et al.Randomized trial comparing side-to-side stapled and hand-sewn esophagogastric anastomosis in neck〔J〕.J Gastrointest Surg,2012,16(7):87-95.
[12] Zingg U,Smithers BM,Gotley DC,et al.Factors associated with postoperative pulmonary morbidity after esophagectomy for cancer〔J〕.Ann Suxg Oncol,2015,18(5):1460-1468.
[13] Gotley DC.EASL Clinical Practice Guidelines on the management of ascites,spontaneous bacterial peritonitis,and hepatorenal syndrome in cirrhosis〔J〕.J Hepatol,2010,53(3):397-417.
[14] Weist R,Krag A,Gerbes A,et al.Spontaneous bacterial p- eritonitis:recent guidelines and beyond〔J〕.Gut,2012,61(7):297-310.
[15] Li M,Pan P,Hu C,et al.Pathogen distribution and antibiotic resistance for hospital aquired pneumonia in respiratory medicine intensive care unit〔J〕.Zhong Nan Da Xue Xue Bao Yi Xue Ban,2013,38(3):251-257.
[16] Shizuma T,Fu Kuyama N.Investigation into bacteremia and spontaneous bacterial peritonitis in patients with liver cirrhosis in Japan〔J〕.Turk J Gastroenterol,2012,23(2):122-126.
[17] Ciruzzi.Case-control study of passive smoking at home and risk of acute myocardial infarction.Argentine FRICAS Investigators.Factores de Riesgo Coronario en America del Sur〔J〕.J Am Coll Cardiol,2015,31(4):797-803.
[18] Griffiths IT,Bryant ST,Dummer PM,et al.Canalshapes produced sequentially during instrumentation with Quantec LX rotary nick-el-titanium instruments:a study in simulated canals〔J〕.Int Endod J,2014,33(4):346-354.
[19] Zafiropoulos GG,di Prisco MO,Deli G,et al.Maintenance af-ter a complex orthoperio treatment in a case of generalized ag-gressive periodontitis:7-year result〔J〕.Int Acad Periodontol,2010,12(4):112-122.
[20] Speer C,Pelz K,Hopfenmüller W,et al.Investigations on the influ-enc of the subgingival microflora in chronic periodontitis.A study in adult patients during fixed appliance therapy〔J〕.J Orofac Orthop,2015,65(1):34-47.
(编辑:甘 艳)
Risk Factors Resulting in Patients Suffering from Venous Thromboembolism andChanges of Coagulation after Central Venous Catheters
ZHOUXiaoqi,ZHANGHaifeng.
ThePeople'sHospitalofRugao,Rugao,226500
Objective To study the clinical value of intrathoracic esophageal anastomosis method in three-field lymph node dissection,and intrathoracic anastomosis methods.Methods 97 cases of esophageal cancer patients (cervical anastomosis 82 cases,15 cases of intrathoracic anastomosis) were randomly selected,clinical data of the 2 groups were compared.Results Conventional logistic regression analysis,and we further the clinical and pathological data and contributing factors that may anastomotic fistula were analyzed comparison,it was found intrathoracic anastomosis can significantly reduce the three-field lymph after dissection anastomotic fistula probability,the probability of occurrence of anastomotic leakage in intrathoracic was significantly lower (3.22% vs.20.55%,P=0.015) anastomosis group.Conclusion Three field intraoperative use of intrathoracic anastomosis can significantly reduce the incidence of fistula,and intrathoracic anastomosis nor operative time,intraoperative clinical condition affecting the number of lymph node dissection,surgical blood loss.
Esophageal cancer;Three-field lymph node dissection;Intrathoracic anastomosis;Internal carotid anastomosis
226500 江苏省如皋市人民医院
10.3969/j.issn.1001-5930.2017.04.025
R735.1
A
1001-5930(2017)04-0609-04
2016-06-23
2016-11-04)
猜你喜欢
中老年保健(2022年5期)2022-08-24
中老年保健(2022年6期)2022-08-19
安徽医学(2022年5期)2022-05-21
中国现代药物应用(2021年17期)2021-10-06
浙江中西医结合杂志(2019年8期)2019-08-24
实验与检验医学(2019年3期)2019-06-18
西南军医(2016年1期)2016-01-23
中国继续医学教育(2015年4期)2016-01-07
川北医学院学报(2015年5期)2015-12-05
肿瘤预防与治疗(2015年5期)2015-09-26
