
Depression, Anxiety, and Cardiovascular Disease in Chinese: A Review for a Bigger Picture
2017-05-26 03:12:59XiongFeiPanRuiweiMengNaLiuandAnPan
Xiong-Fei Pan, Ruiwei Meng, Na Liu,2, and An Pan
1Department of Epidemiology and Biostatistics Ministry of Education Key Laboratory of Environment and Health, and State Key Laboratory of Environmental Health (Incubating), School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
2Department of Health Care, The First Affiliated Hospital with Nanjing Medical University, Nanjing, China
lntroduction
China has experienced rapid economic development in the past several decades. With economic prosperity, urbanization, rapid lifestyle change, rising income, and aging, noncommunicable diseases have surpassed infectious diseases as the major burden among diseases. Cardiovascular disease(CVD), particularly stroke (1.7 million deaths) and ischemic heart disease (0.9 million deaths), was the leading cause of death in China in 2013 [1]. In the same year, CVD accounted for 40.7% of all deaths,and the age-standardized CVD mortality reached 307 per 100,000 persons. From 1990 to 2013, total deaths caused by CVD increased from 2.6 million to 3.7 million in China [1]. Despite increasing average life expectancy in the past few decades in China,it is projected that the increasing trend of noncommunicable diseases, particularly CVD, might be a hurdle to such progress in the next two decades [2].
Multiple risk factors have been implied in the pathophysiology of CVD. Among them, mental health has received considerable attention recently.Depression and anxiety are two major forms of mental health issues in China. According to estimates from the 2010 Global Burden of Disease Study [3],depression was the fourth leading cause of disability-adjusted life years in China in 2010. Depression can range from mild depressive symptoms to major depressive disorder (MDD). Many questionnaires have been developed to screen patients for depressive symptoms, but MDD is mainly diagnosed by a psychiatrist on the basis of a clinical diagnostic interview and requires persistence of certain symptoms for a period. Similarly, although anxiety can occur as a symptom at some point of any individual’s life, the diagnosis of anxiety disorder requires the individual to meet certain criteria, and it includes several subtypes, such as generalized anxiety disorder, panic disorder, and phobia. A few studies have reported high prevalence of depression and anxiety in the Chinese population. In a large study in four provinces of China in 2001–2005, the 1-month prevalence of MDD and anxiety disorders was estimated to be 2.1 and 5.6%, respectively [4]. Both were more prevalent in women and in older individuals compared with their counterparts. A review of 17 studies showed that the overall estimates of current,12-month, and lifetime prevalence of MDD were 1.6, 2.3, and 3.3%, respectively [5]. Meanwhile, the prevalence of depressive symptoms in Chinese older adults was 23.6% from a meta-analysis of 81 crosssectional studies [6]. Another review, of 21 crosssectional studies in Chinese adults, showed that the pooled estimates of current and lifetime prevalence of anxiety disorders were 2.4 and 4.1%, respectively[7]. Therefore depression and anxiety have become major public health challenges and warrant more studies on their primary prevention, early detection,and effective treatment programs [8].
It is widely acknowledged that depression and anxiety are intercorrelated with CVD: patients with CVD usually have higher prevalence of depression and anxiety than the general population, and individuals who have depressive and anxiety disorders tend to have a higher likelihood of cardiac events and even death [9]. However, there is generally lack of original studies on this topic in the Chinese population.In such a context, we aimed to summarize the latest evidence for the role of depression and anxiety in the onset and prognosis of CVD, with emphasis on cohort studies conducted in Chinese settings. Our review is limited to studies that used a standard screening scale for depressive or anxiety symptoms, or a structured clinical interview for diagnosis. In this review, we use the term “disorder” mostly when structured clinical interviews were applied or when more severe cases were indicated, and otherwise use “depressive symptoms” and “anxiety symptoms,” while more general terms such as “anxiety” and “depression” are meant to include both symptoms and disorders.
Literature Search and Evidence Synthesis
A literature search was conducted in four Englishlanguage and three Chinese-language databases for original articles published in China (including mainland China, Hong Kong, and Taiwan). The Englishlanguage databases were PubMed/MEDLINE,Embase, SCOPUS, and ISI Web of Knowledge.The Chinese-language databases were China National Knowledge Infrastructure, Wanfang, and Chongqing VIP. Chinese-language and Englishlanguage search algorithms were established for searches in the seven databases. Six groups of MeSH terms, keywords, and free text were used in different combinations, including “depression,”“anxiety,” “cardiovascular disease,” “risk,” “prognosis,” and geographical area limitations to China.References cited in the articles were also manually reviewed to identify any additional articles. The search ended on November 31, 2016, with no lower time limit.
Studies were eligible for assessment if (1) they had a cohort study design (particularly a prospective study design), (2) the exposure of interest was depression or anxiety (either screened or diagnosed), and(3) the outcome was CVD incidence or death when the study participants had no CVD at the baseline,or recurrent cardiovascular events (including death)when study participants had CVD at the baseline.Abstracts from preliminary searches were screened to exclude irrelevant articles, followed by a review of the full text for the remaining articles. All original studies identified were qualitatively appraised, and major information such as participant characteristics, study setting, exposures, outcomes, and findings were extracted (Table 1).
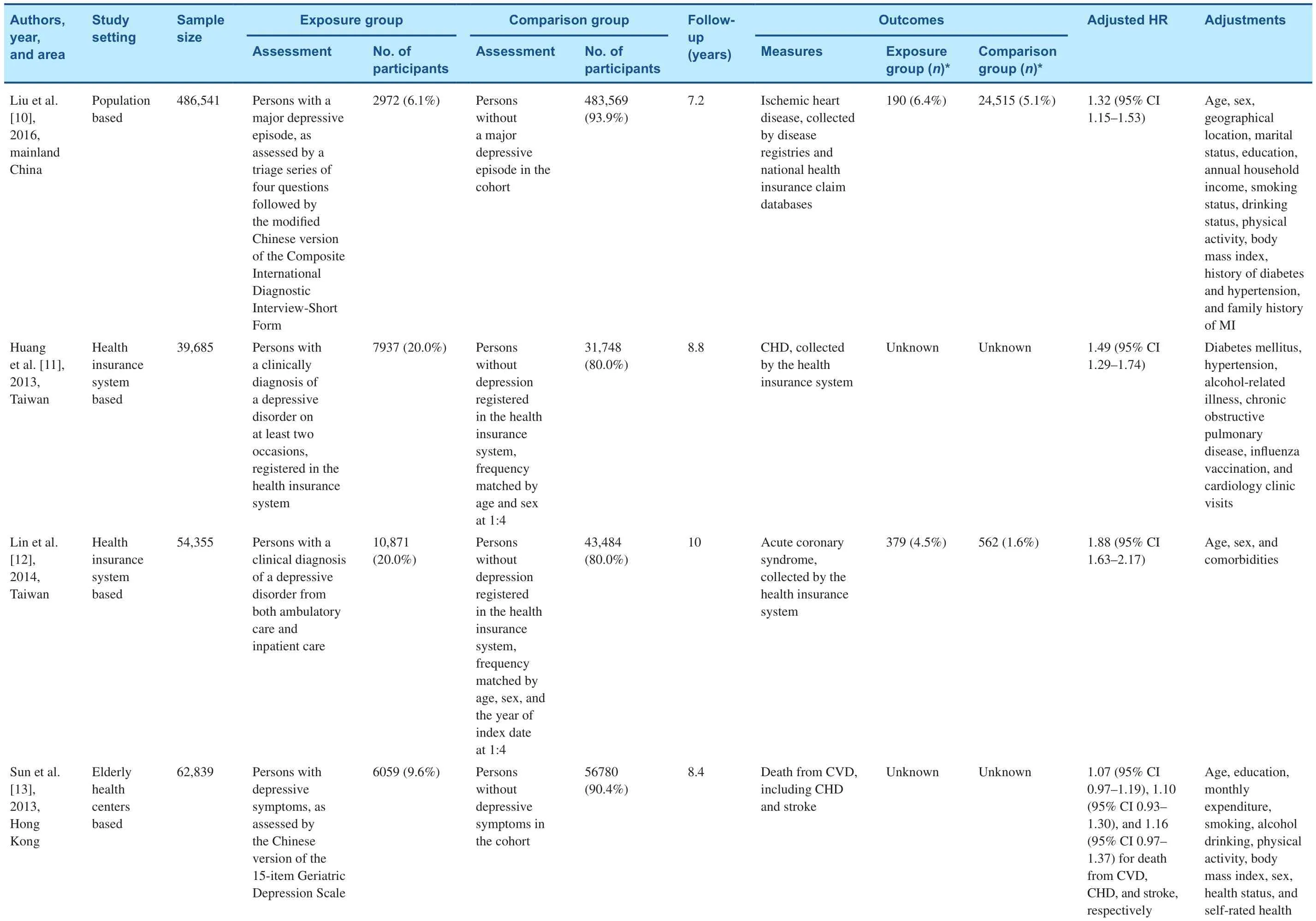
Table 1Summary of Cohort Studies on the Association BetweenDepression/Anxiety and Cardiovascular Disease in Chinese Populations.
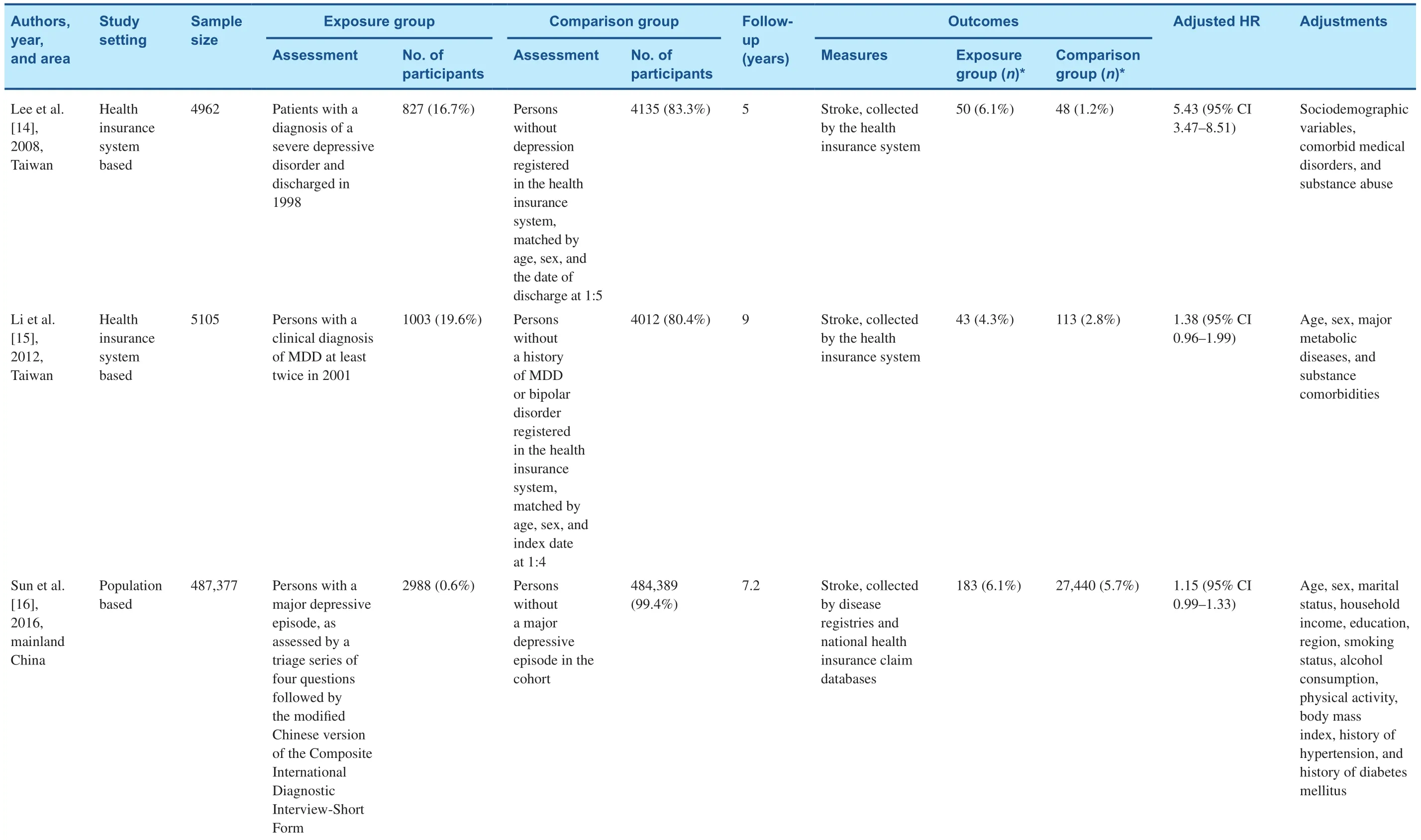
Table 1(continued)
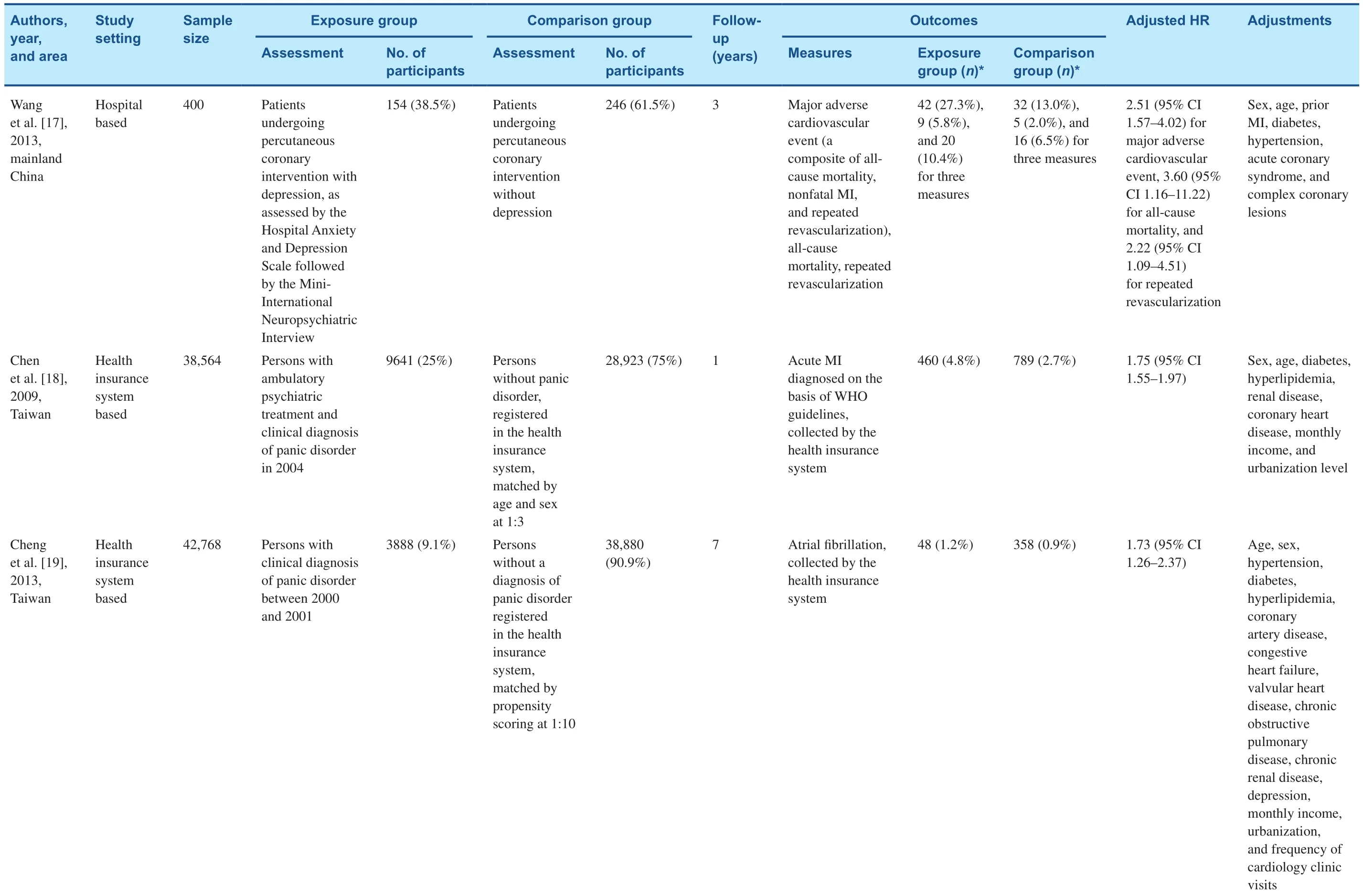
Table 1(continued)
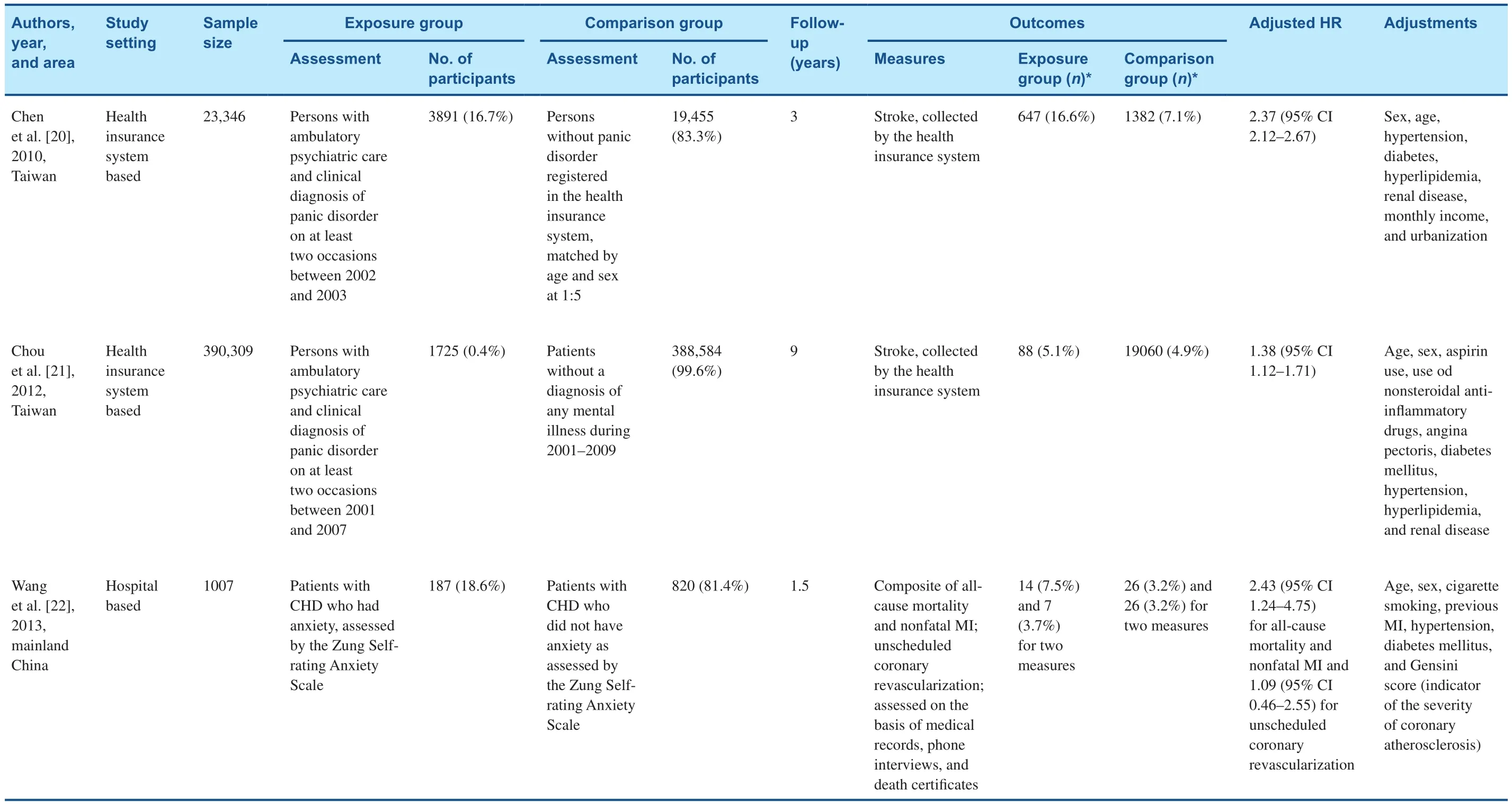
Table 1(continued)
Besides searching for original studies, we performed a complementary search for reviews on the basis of similar search terms in the abovementioned databases and the Cochrane Library, but without geographical area limitation to China. The purpose of the search for reviews was to provide international evidence in the case of a lack of Chinese original studies.
Depression and CVD Depression and Risk of CVD
Several meta-analyses of cohort studies at different times have demonstrated that depression is a risk factor for incident CVD [23–28]. Three early metaanalyses consistently found that depression conferred about 60% increased risk of coronary heart disease (CHD) [23–25]. In addition, MDD was a stronger predictor for the development of CHD than depressive mood, suggesting a dose-response relationship between depression and CHD [24, 28].A later meta-analysis showed that depression was associated with about 30% increased risk of CHD and myocardial infarction (MI) combined [26]. A recent meta-analysis also reported similar results for MI and cardiac death [27].
However, studies in the Chinese population are still lacking, and only a few large-scale cohort studies in mainland China [10], Taiwan [11, 12], and Hong Kong [13] add to the evidence that depression is a risk factor for CVD. A recent study published by our group found that participants with a major depressive episode had a higher incidence rate of ischemic heart disease compared with those without a major depressive episode (8.76 versus 7.21 per 1000 person-years) during a median followup of 7.2 years [10]. We used data from the China Kadoorie Biobank (CKB) study, which is a community-based cohort established since 2004 with more than 0.5 million Chinese aged 30–79 years. After adjustment for other CVD risk factors, participants with a major depressive episode in the past year were 1.32 times as likely to have ischemic heart disease as those without a major depressive episode in the past year [hazard ratio (HR) 1.32, 95% confidence interval (CI) 1.15–1.53]. In addition, we found that the adjusted HR of ischemic heart disease was 1.13(95% CI 1.04–1.23) for participants with depressive symptoms only and 1.33 (95% CI 1.15–1.53) for those with a major depressive episode versus those without depression, indicating a dose-response relation. Two large cohort studies analyzed the relations between depression and new-onset coronary events and acute coronary syndrome on the basis of data from the Taiwan National Health Insurance Program[11, 12]. One study randomly selected 39,685 individuals (7937 with depression and 31,748 without depression) aged 20–99 years to examine risk factors for incident coronary events during a median follow-up period of 8.8 years [11]. The multivariable-adjusted HR was 1.49 (95% CI 1.29–1.74) for individuals with depression compared with age- and sex-matched controls. In a separate study, 10,871 patients with newly diagnosed MDD were included,and each patient was randomly frequency-matched for age and sex with four participants [12]. The risk of developing acute coronary syndrome was 88%higher (HR 1.88, 95% CI 1.63–2.17) in those with MDD versus those without MDD. In a study among elderly Chinese in Hong Kong [13], depressive symptoms were screened with use of the 15-item Geriatric Depression Scale among 21,473 men and 41,366 women at elderly health centers. A positive association was reported between depressive symptoms and CHD death in men (HR 1.41, 95%CI 1.08–1.84) but not in women (HR 0.94, 95% CI 0.75–1.16). However, such sex-specific estimates were not reported in other cohort studies [10–12].
With regard to stroke, a previous meta-analysis of 28 cohort studies demonstrated that depression is associated with 45% increased risks of stroke morbidity and death, and strong associations were evident particularly for fatal and ischemic stroke[29]. An updated meta-analysis published in 2015 reached similar conclusions [30]. So far, only four cohort studies have been conducted in the Chinese population [13, 14–16], of which two were based on the Taiwan National Health Insurance database[14, 15]. In a study of 827 patients (aged 18–44 years) hospitalized for depressive disorder and 4135 individuals matched at 1:5 for sex, age, and date of discharge, depressed patients were 5.43 times(95% CI 3.47–8.51) as likely to develop stroke as nondepressed individuals during a 5-year followup [14]. The large effect size of depression in that study might be due to the inclusion of hospitalized severely depressed patients as cases. In a separate cohort study among 5015 participants (1003 MDD patients and 4012 control individuals without MDD)for a follow-up of up to 9 years, patients with MDD had a higher risk of stroke (HR 1.44, 95% CI 1.01–2.06) after adjustment for age, sex, and substance dependence [15]. However, since the association became not statistically significant after additional adjustment for major metabolic diseases (including diabetes, hypertension, and hyperlipidemia), it was suspected that the risk of stroke among MDD patients was mediated by the development of major metabolic diseases. A more recent study using the CKB data found that major depressive episode was associated with a 1.15-fold increased risk of stroke(95% CI 0.99–1.33) [16]. In addition, there was a positive dose-response relationship between the number of depressive symptoms and stroke risk(Pfor trend of 0.011). Of note, in the cohort study among elderly adults in Hong Kong, the positive association between depressive symptoms and death from stroke did not show statistical significance (HR 1.16, 95% CI 0.97–1.37), even in subgroup analysis by sex (HR 1.21, 95% CI 0.90–1.63 in men; HR 1.16, 95% CI 0.94–1.43 in women) [13].
In summary, a few cohort studies suggested that depression was associated with increased risks of CHD and stroke in the Chinese population in a doseresponse manner. However, several studies were based on the Taiwan National Health Insurance database, and more studies in the general populations, like the CKB study, are needed to better control for other covariat es and understand the role of different magnitudes of depression (from mild symptoms to MDD) in the development of CVD.
Depression and Cardiovascular Prognosis
Depression is highly prevalent among patients with CVD. A systematic review of eight studies including 10,785 patients with acute MI showed that the prevalence of MDD was 19.8% (95% CI 19.1–20.6%) by means of structured clinical interviews [31]. The prevalence of significant depressive symptoms ranged from 7.3% (Hospital Anxiety and Depression Scale score ≥ 11) to 31.1% (Beck Depression Inventory score ≥ 10) depending on the screening scales. In addition, in a meta-analysis of 61 studies with 25,488 patients with stroke,31% (95% CI 28–35%) experienced depression after stroke [32], which was consistent with the finding from a review (33%; 95% CI 29–36%) a decade ago [33]. More importantly, 23% (95% CI 14–31%) of patients had depression even 5 years after stroke (Beck Depression Inventory score ≥ 10)[32]. The prevalence of depression is similarly high among Chinese patients with CVD. A 2013 review included 23 studies with 5236 CHD patients in hospital settings and four studies with 1353 patients in community settings in China [34]. The overall prevalence of depression was 51% (95% CI 43–58%)in patients with CHD in hospital settings, and was between 34.6 and 45.8% in community settings depending on the screening technique.
Several systematic reviews have consistently demonstrated the substantial impact of depression in patients with CVD on the recurrence of nonfatal cardiac events, and even death [28, 35–43]. Two systematic reviews showed that depression was associated with an 80% increased risk of all-cause death among CHD patients [28, 35]. In particular,a review qualitatively assessed the available literature for depression’s negative impact on the prognosis for acute coronary syndrome, and found that depression was associated with all-cause and cardiac death, as well as composite outcomes that combined death and nonfatal cardiac events [36]. A pooled analysis of 10,175 patients with MI from 30 studies found that a standard deviation increase in post-MI depressionzscores was associated with an increased risk of all-cause mortality (HR 1.32, 95% CI 1.26–1.38) and cardiovascular events (HR 1.19, 95% CI 1.14–1.24) [37]. The association between post-MI depression and all-cause mortality was stronger in men than in women [38]. Consistently, two reviews focusing on short-term prognosis showed that post-MI depression was associated with a 1.6- to 2.7-fold increased risk of impaired cardiovascular outcomes within 2 years after the index MI [39, 40]. Another two reviews examined the impact of depression after heart failure on all-cause and cardiovascular death [41, 42]. Depression was associated with an about 1.5-fold increased risk of all-cause mortality[41, 42], and the association was evident for major depression (HR 1.98, 95% CI 1.23–3.19) but not mild depression (HR 1.04, 95% CI 0.75–1.45) [41].In addition, depression after heart failure was associated with a more than twofold (HR 2.19, 95% CI 1.46–3.29) increased risk of cardiovascular death[41]. With regard to stroke, a review including 14 studies with 4498 stroke patients found that depression was associated with adverse prognosis, such as higher mortality and poor life satisfaction, and less efficient use of rehabilitation services [43].
Few prospective studies have examined the association between depression and prognosis among CVD patients in China. Some studies found that depression was associated with increased mortality [17], poor health-related quality of life [44, 45],and even longer hospital stay [46] among Chinese patients with CVD. In particular, a study of 400 CHD patients during a 3-year follow-up found that depression (as assessed by the Hospital Anxiety and Depression Scale and Mini-International Neuropsychiatric Interview) after percutaneous coronary intervention was positively associated with all-cause mortality (HR 3.60, 95% CI 1.16–11.22)and repeated revascularization (HR 2.22, 95% CI 1.09–4.51) [17]. Since most of these Chinese studies were cross-sectional with small sample sizes,efforts are urgently needed to generate Chinese evidence in this area.
In summary, although studies have provided ample evidence for the association between depression and poor cardiovascular prognosis in other countries, there is a lack of robust prospective Chinese studies on this topic, which reflects inadequate attention to the mental status of CVD patients in clinical practice in China. Evidence from longterm cohort studies is needed to understand the role of depression in the prognosis of patients with CVD in Chinese settings.
Anxiety and CVD
Anxiety and Risk of CVD
The association between anxiety and the risk of CVD has been studied in multiple populations, and a positive association has been consistently reported[47–50]. Two systematic reviews published in 2016 examined the association between anxiety and the risk of multiple CVD outcomes [49, 50]. The overall risk of CVD increased by 52% (HR 1.52, 95%CI 1.36–1.71) among anxious individuals compared with those without anxiety among 1,565,699 individuals from 37 cohort studies [49]. Specifically,anxiety was associated with increased risks of CHD[relative risk (RR) 1.49, 95% CI 1.31–1.69; 26 studies], stroke (RR 1.74, 95% CI 1.25–2.43; 7 studies), MI (RR 1.38, 95% CI 1.16–1.64; 11 studies),and CVD death (RR 1.61, 95% CI 1.22–2.12; 14 studies). A separate review included 2,017,126 participants from 46 cohort studies or nested case-control studies [50]. Besides CHD, stroke, and CVD death, anxiety was also associated with an elevated risk of heart failure (RR 1.35, 95% CI 1.11–1.64).However, the association between anxiety and atrial fibrillation was not statistically significant (RR 1.27,95% CI 0.90–1.80), maybe because there were only three studies on this topic. Among all subtypes of anxiety, phobic anxiety was more strongly associated with CVD risk than other anxiety disorders,and posttraumatic stress disorder was more associated with stroke risk [50].
Two studies in Taiwan investigated the relation between anxiety or its subtypes and incident MI [18]and atrial fibrillation [19]. In a large cohort study of 9641 patients with panic disorder and 28,923 without panic disorder [18], 4.8% of patients with panic disorder and 2.7% of patients without panic disorder experienced an acute MI within 1 year of follow-up. The corresponding RR was 1.75 (95%CI 1.55–1.97), and the association persisted in stratified analyses by hypertension, CHD, and age.Besides acute MI, another study, of 42,768 individuals (300 patients with panic disorder and 38,880 individuals without panic disorder, mean age of 42 years), showed that panic disorder was associated with an increased risk of atrial fibrillation (RR 1.73,95% CI 1.26–2.37) [19].
Two large studies also specifically assessed the association between panic disorder and the risk of stroke on the basis of the Taiwan National Health Insurance database [20, 21]. One study included 3891 patients with panic disorder and 19,455 individuals without panic disorder matched for sex and age in 2010 [20]. In a follow-up of three years,16.6% of patients with panic disorder and 8.7%of individuals without panic disorder developed stroke, and the corresponding HR was 2.37 (95%CI 2.12–2.67) after adjustment for sex, age, income,level of urbanization, and comorbidities. The strong association persisted in stratified analyses by medical conditions and age. However, the validity of this study was weakened by no explicit exclusion of individuals with a history of stroke at the baseline.
In a similar study of 390,309 individuals (1725 patients with panic disorder and 388,584 without panic disorder) enrolled in 2001–2007, the cumulative incidence rate of stroke was 5.1% in the panic disorder group and 4.9% in the companion group by the end of 2009 [21]. The RR was 1.38 (95%CI 1.12–1.71) after for sex, age, medications, and comorbidities had been controlled for.
In conclusion, consistent with systematic reviews,current studies in the Chinese population support the proposition that anxiety might be a risk factor for CVD. Since most of the original studies [18–21]were based on the Taiwan Health Insurance database, which may be subject to unmeasured/residual confounding and limited generalizability, more population-based cohort studies are urgently needed to explore the relation between anxiety and the risk of CVD in Chinese adults.
Anxiety and Cardiovascular Prognosis
In the general population, the 1-year and lifetime prevalence of anxiety disorders was estimated to be 11.0% (95% CI 7.5–14.3%) and 16.6% (95%CI 12.7–21.1%), respectively [51]. A systematic review reported that the prevalence of anxiety disorders in stroke patients was 18% (95% CI 8–29%)if clinical interview was used and 25% (95% CI 21–28%) if screening scales were used [52]. In particular, the prevalence of generalized anxiety disorder was 10.9% (95% CI 7.8–14%) among patients with CHD, and the lifetime prevalence could be as high as 25.8% (95% CI 20.8–30.8%) [53]. Available Chinese studies also reported a high prevalence of anxiety among CVD patients. In a study of 700 Chinese inpatients with CVD, the prevalence of anxiety symptoms (Zung Self-rating Anxiety Scale score ≥ 50) was 26.7%, and the prevalence was higher in women (31.5%) than in men (21.4%) [54].Another study, of 509 hospitalized patients with CHD, reported a similar prevalence of 23.4% [55].In a multicenter study of 1144 patients with premature ventricular contraction but no structural heart disease in 12 hospitals from five provinces across China, 33.3% had anxiety symptoms (Zung Selfrating Anxiety score ≥ 40) [56]. The prevalence was higher in patients aged more than 45 years than in those aged 45 years or younger (52.1 versus 17.4%),and was higher in women than in men (36.1 versus 29.6%).
Anxiety may arise before or after diagnosis of CVD, and may further trigger recurrent cardiac events or other adverse events. Two major reviews systematically evaluated the association between anxiety and the risk of cardiac events among CVD patients [57, 58]. One systematic review included 5750 patients with MI from 12 cohort studies with at least 6 months of follow-up [57]. Post-MI anxiety was associated with all-cause mortality [odds ratio(OR) 1.47, 95% CI 1.02–2.13; four studies), cardiac death (OR 1.23, 95% CI 1.03–1.47; four studies),and new cardiac events (OR 1.71, 95% CI 1.31–2.23; seven studies). Another review evaluated the relationship between anxiety and death in 30,527 patients with CHD from 44 studies [58]. Anxiety was associated with an increased risk of poor outcomes (death and other negative outcomes, such as rehospitalizations or recurrent cardiac events)only in patients with stable CHD, but not in those who just had acute coronary syndrome. The authors hypothesized that the discrepancy was because anxiety symptoms in the immediate post–acute coronary syndrome period may be transient and related to the cardiac event itself instead of its prognosis.
Despite evidence from systematic reviews, very few prospective studies have explored the relationship between anxiety and adverse prognosis in Chinese CVD patients. A Chinese study examined the association between anxiety after coronary angiography or percutaneous coronary intervention and the risk of all-cause mortality and nonfatal MI in 1007 CHD patients with a mean follow-up of 17 months after hospital discharge [22]. The Zung Self-rating Anxiety Scale score was associated with coronary atherosclerosis as determined by the Gensini score (β=1.35,P<0.001). In addition, anxiety symptoms (Zung Selfrating Anxiety Scale score ≥ 50) were associated with increased risk of all-cause mortality and nonfatal MI(adjusted HR 2.43, 95% CI 1.24–4.75).
In summary, existing evidence shows that anxiety is associated with increased risks of adverse outcomes in patients with CVD. However, more studies are needed in the Chinese population to examine the relationship. Since depression and anxiety coexist in many CVD patients [53], future studies may need to consider their independent and synergetic effects for the risk of adverse cardiovascular outcomes.
Mechanisms for the Link Between Depression and Anxiety and CVD
The mechanisms underlying the link between depression, anxiety, and CVD are still uncertain,and results from etiological studies are inconsistent.However, two plausible levels of mechanisms have been proposed: behavioral and biological pathways[9, 59]. At the behavioral level, depression and/or anxiety may be associated with unhealthy lifestyles and behaviors that lead to the occurrence of CVD,and nonadherence with interventions for CVD that contribute to adverse prognosis. Both depression and anxiety are associated with several major risk factors for CVD, such as physical inactivity, cigarette smoking, and excessive alcohol consumption [9]. On the one hand, these risk factors may partially account for the effects of depression and anxiety on CVD [60]. On the other hand, depression and anxiety may potentiate the effects of these risk factors for CVD. Patients with depression and anxiety may be less likely to adhere to medications,lifestyle interventions, and rehabilitation programs,which may result in compromised effectiveness [9,60]. In addition, the existence of depression and anxiety among patients with CVD may reflect a higher severity of CVD [61], and thus result in an increased risk of death or morbidity in patients with CVD.
At the biological level, depression and anxiety might induce autonomic nervous system dysfunction, cardiac rhythm disturbances, in flammation,platelet dysfunction, and hypercoagulability [9, 59,62, 63]. Depression and anxiety are associated with neurohormonal abnormalities that cause an imbalance in sympathetic and parasympathetic activity,leading to increased heart rate and blood pressure as well as increased risk of atherosclerotic plaque rupture and acute coronary thrombosis [9, 64]. The neurohormonal abnormalities also increase irritability of the heart muscle, which causes a disturbance in heart rhythm, leading to ventricular fibrillation and cardiac arrest. In addition, depression and anxiety may increase in flammatory reactions associated with unstable coronary artery plaques that contribute to coronary syndromes [63, 64]. Moreover,depression may induce platelet dysfunction, which may cause vascular damage, thrombus formation,and even coronary events. Since depression and anxiety are often coexistent and their associations with CVD can be bidirectional, the etiological model might be multifaceted and even form feedback loops [9].
lmplications for lnterventions
Psychological disorders are generally stigmatized,and there is a lack of optimal investment in health services in China [65]. They are often unrecognized and untreated in clinical practice. The current body of evidence demonstrates that both depression and anxiety are involved in the onset and prognosis of CVD. Given the disease burden of anxiety and depression and their role in CVD, it is imperative to target primary interventions to prevent CVD onset and secondary/tertiary interventions to improve prognosis. Generally, depression and anxiety should be screened and diagnosed in a timely manner, and should be treated appropriately once they have been diagnosed in any setting [66, 67]. Depressive and anxiety symptoms can occur at any point in the lifetime and can be transient, and their impact on the cardiovascular system is invisible. Several scales can be used for screening purposes in different settings, such as the Beck Depression Inventory [68]for depression and the Zung Self-rating Anxiety Scale [69] for anxiety, most of which have been adapted for Chinese settings and tested for validity and reliability. Once individuals have been assessed as probably having depression or anxiety disorders, they should be referred to qualified psychiatrists for clinical diagnosis based on the Chinese Classification of Mental Disorders III, which is similar in structure and classification to the fourth edition of theDiagnostic and Statistical Manual of Mental Disordersor the tenth revision of the International Statistical Classification of Diseases and Related Health Problems. Current standard treatments for depressive and anxiety disorders in the general population include psychotherapies such as cognitive behavioral therapy and medications such as selective serotonin reuptake inhibitors,and they are recommended for the two conditions among CVD patients by professional organizations [67]. Although selective serotonin reuptake inhibitors and certain psychotherapies are generally proven to be safe for patients with CVD in clinical trials, their efficacy in reducing cardiac morbidity and mortality remains unclear because of the lack of large controlled trials [9, 70]. Thus current treatment recommendations among patients with CVD target only the two psychological conditions themselves,and aim to reduce the symptoms and improve the health-related quality of life. In addition, patients with CVD being treated for these conditions should still be closely monitored for adherence to medical care, drug efficacy, and safety with respect to their cardiovascular and mental health [67]. In Chinese settings, because few CVD patients ever receive a diagnosis or treatment for mental disorders in clinical practice [71], future efforts might be directed toward inclusion of psychiatrists in the multidisciplinary clinical group for CVD treatment, a collaborative care model that shows a potential advantage for management of psychological conditions and physical diseases [72].
Conclusions
Both depression and anxiety are highly prevalent among patients with CVD compared with the general population in China. Current evidence from other populations and only a few Chinese studies suggests that depression and anxiety are associated with an increased risk of CVD onset in the general population and adverse outcomes in CVD patients.More high-quality and large-scale prospective studies are urgently needed to investigate the impact of depression/anxiety on the cardiovascular system in the Chinese population, particularly for the prognosis among CVD patients. The available evidence does not suf fi ciently support the ef fi cacy of depression or anxiety treatments for reducing CVD mortality or morbidity, but they are recommended for mitigating symptoms and improving the mental health-related quality of life for CVD patients with depression and/or anxiety. Finally, the collaborative care model needs to be tested in clinical settings in China.
Con fl ict of lnterest
The authors declare that they have no conflicts of interest.
REFERENCES
1. Zhou M, Wang H, Zhu J, Chen W,Wang L, Liu S, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013.Lancet 2016;387:251–72.
2. Wu Y, Benjamin EJ, MacMahon S. Prevention and control of cardiovascular disease in the rapidly changing economy of China.Circulation 2016;133:2545–60.
3. Yang G, Wang Y, Zeng Y, Gao GF, Liang X, Zhou M, et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010.Lancet 2013;381:1987–2015.
4. Phillips MR, Zhang J, Shi Q, Song Z, Ding Z, Pang S, et al. Prevalence,treatment, and associated disability of mental disorders in four provinces in China during 2001–05:an epidemiological survey. Lancet 2009;373:2041–53.
5. Gu L, Xie J, Long J, Chen Q, Chen Q, Pan R, et al. Epidemiology of major depressive disorder in mainland china: a systematic review.PLoS One 2013;8:e65356.
6. Li D, Zhang DJ, Shao JJ, Qi XD,Tian L. A meta-analysis of the prevalence of depressive symptoms in Chinese older adults. Arch Gerontol Geriatr 2014;58:1–9.
7. Guo X, Meng Z, Huang G, Fan J,Zhou W, Ling W, et al. Meta-analysis of the prevalence of anxiety disorders in mainland China from 2000 to 2015. Sci Rep 2016;6:28033.
8. Charlson FJ, Baxter AJ, Cheng HG, Shidhaye R, Whiteford HA.The burden of mental, neurological, and substance use disorders in China and India: a systematic analysis of community representative epidemiological studies. Lancet 2016;388:376–89.
9. Cohen BE, Edmondson D, Kronish IM. State of the art review: depression, stress, anxiety, and cardiovascular disease. Am J Hypertens 2015;28:1295–302.
10. Liu N, Pan XF, Yu C, Lv J, Guo Y,Bian Z, et al. Association of major depression with risk of ischemic heart disease in a mega-cohort of Chinese adults: the China Kadoorie Biobank Study. J Am Heart Assoc 2016;5:e004687.
11. Huang CJ, Hsieh MH, Hou WH, Liu JC, Jeng C, Tsai PS.Depression, antidepressants, and the risk of coronary heart disease: a population-based cohort study. Int J Cardiol 2013;168:4711–6.
12. Lin YN, Lin CL, Chang YJ, Peng CL, Sung FC, Chang KC, et al.Increased subsequent risk of acute coronary syndrome for patients with depressive disorder: a nationwide population-based retrospective cohort study. Psychiatry Clin Neurosci 2014;68:263–9.
13. Sun WJ, Xu L, Chan WM, Lam TH, Schooling CM. Are depressive symptoms associated with cardiovascular mortality among older Chinese: a cohort study of 64,000 people in Hong Kong? Am J Geriatr Psychiatry 2013;21:1107–15.
14. Lee HC, Lin HC, Tsai SY. Severely depressed young patients have over five times increased risk for stroke:a 5-year follow-up study. Biol Psychiatry 2008;64:912–5.
15. Li CT, Bai YM, Tu PC, Lee YC,Huang YL, Chen TJ, et al. Major depressive disorder and stroke risks: a 9-year follow-up population-based, matched cohort study.PLoS One 2012;7:e46818.
16. Sun J, Ma H, Yu C, Lv J, Guo Y,Bian Z, et al. Association of major depressive episodes with stroke risk in a prospective study of 0.5 million Chinese adults. Stroke 2016;47:2203–8.
17. Wang ZJ, Guo M, Si TM, Jiang MM,Liu SM, Liu YY, et al. Association of depression with adverse cardiovascular events after percutaneous coronary intervention. Coron Artery Dis 2013;24:589–95.
18. Chen YH, Tsai SY, Lee HC, Lin HC. Increased risk of acute myocardial infarction for patients with panic disorder: a nationwide population-based study. Psychosom Med 2009;71:798–804.
19. Cheng YF, Leu HB, Su CC, Huang CC, Chiang CH, Huang PH, et al.Association between panic disorder and risk of atrial fibrillation: a nationwide study. Psychosom Med 2013;75:30–5.
20. Chen YH, Hu CJ, Lee HC, Lin HC.An increased risk of stroke among panic disorder patients: a 3-year follow-up study. Can J Psychiatry 2010;55:43–9.
21. Chou PH, Lin CH, Loh EW,Chan CH, Lan TH. Panic disorder and risk of stroke: a population-based study. Psychosomatics 2012;53:463–9.
22. Wang G, Cui J, Wang Y, Deng B,Liang X, Bai J, et al. Anxiety and adverse coronary artery disease outcomes in Chinese patients.Psychosom Med 2013;75:530–6.
23. Wulsin LR, Singal BM. Do depressive symptoms increase the risk for the onset of coronary disease?A systematic quantitative review.Psychosom Med 2003;65:201–10.
24. Rugulies R. Depression as a predictor for coronary heart disease.a review and meta-analysis. Am J Prev Med 2002;23:51–61.
25. Van der Kooy K, van Hout H,Marwijk H, Marten H, Stehouwer C, Beekman A. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry 2007;22:613–26.
26. Gan Y, Gong Y, Tong X, Sun H,Cong Y, Dong X, et al. Depression and the risk of coronary heart disease: a meta-analysis of prospective cohort studies. BMC Psychiatry 2014;14:371.
27. Wu Q, Kling JM. Depression and the risk of myocardial infarction and coronary death: a metaanalysis of prospective cohort studies. Medicine (Baltimore)2016;95:e2815.
28. Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146 538 participants in 54 observational studies. Eur Heart J 2006;27:2763–74.
29. Pan A, Sun Q, Okereke OI, Rexrode KM, Hu FB. Depression and risk of stroke morbidity and mortality: a meta-analysis and systematic review.J Am Med Assoc 2011;306:1241–9.
30. Li M, Zhang XW, Hou WS, Tang ZY. Impact of depression on incident stroke: a meta-analysis. Int J Cardiol 2015;180:103–10.
31. Thombs BD, Bass EB, Ford DE,Stewart KJ, Tsilidis KK, Patel U, et al. Prevalence of depression in survivors of acute myocardial infarction. J Gen Intern Med 2006;21:30–8.
32. Hackett ML, Pickles K. Part I: frequency of depression after stroke:an updated systematic review and meta-analysis of observational studies. Int J Stroke 2014;9:1017–25.
33. Hackett ML, Yapa C, Parag V,Anderson CS. Frequency of depression after stroke: a systematic review of observational studies. Stroke 2005;36:1330–40.
34. Ren Y, Yang H, Browning C,Thomas S, Liu M. Prevalence of depression in coronary heart disease in China: a systematic review and meta-analysis. Chin Med J(Engl) 2014;127:2991–8.
35. Barth J, Schumacher M, Herrmann-Lingen C. Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis. Psychosom Med 2004;66:802–13.
36. Lichtman JH, Froelicher ES,Blumenthal JA, Carney RM,Doering LV, Frasure-Smith N,et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations: a scientific statement from the American Heart Association. Circulation 2014;129:1350–69.
37. Meijer A, Conradi HJ, Bos EH,Anselmino M, Carney RM,Denollet J, et al. Adjusted prognostic association of depression following myocardial infarction with mortality and cardiovascular events: individual patient data meta-analysis. Br J Psychiatry 2013;203:90–102.
38. Doyle F, McGee H, Conroy R,Conradi HJ, Meijer A, Steeds R, et al. Systematic review and individual patient data metaanalysis of sex differences in depression and prognosis in persons with myocardial infarction:a MINDMAPS study. Psychosom Med 2015;77:419–28.
39. Meijer A, Conradi HJ, Bos EH,Thombs BD, van Melle JP, de Jonge P. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta-analysis of 25 years of research. Gen Hosp Psychiatry 2011;33:203–16.
40. van Melle JP, de Jonge P, Spijkerman TA, Tijssen JG, Ormel J, Van Veldhuisen DJ, et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events:a meta-analysis. Psychosom Med 2004;66:814–22.
41. Fan H, Yu W, Zhang Q, Cao H, Li J,Wang J, et al. Depression after heart failure and risk of cardiovascular and all-cause mortality: a metaanalysis. Prev Med 2014;63:36–42.
42. Sokoreli I, de Vries JJ, Pauws SC,Steyerberg EW. Depression and anxiety as predictors of mortality among heart failure patients: systematic review and meta-analysis.Heart Fail Rev 2016;21:49–63.
43. Kutlubaev MA, Hackett ML. Part II: predictors of depression after stroke and impact of depression on stroke outcome: an updated systematic review of observational studies. Int J Stroke 2014;9:1026–36.
44. Sun X, Hu F, Jiao Y, Zhao P, Yu H,Cao S, et al. Impact of depression on quality of life and long term prognosis in patients with coronary heart disease after percutaneous coronary intervention (in Chinese).J Clin Cardiol 2013;29:74–5.
45. Kong L, Jiang W. Study on correlation between postoperative anxiety,depression and quality of life in the late in patients with coronary heart disease undergoing stent implantation (in Chinese). Chin Gen Pract Nurs 2014;12:967–9.
46. Sun CJ, He JH, Zhu HY. The impact of depressive symptoms on the time to discharge of inpatients with coronary heart disease (in Chinese). J Card Pulm Dis 2010;29:395–7.
47. Roest AM, Martens EJ, de Jonge P, Denollet J. Anxiety and risk of incident coronary heart disease: a meta-analysis. J Am Coll Cardiol 2010;56:38–46.
48. Tully PJ, Turnbull DA, Beltrame J,Horowitz J, Cosh S, Baumeister H,et al. Panic disorder and incident coronary heart disease: a systematic review and meta-regression in 1131612 persons and 58111 cardiac events. Psychol Med 2015;45:2909–20.
49. Batelaan NM, Seldenrijk A, Bot M, van Balkom AJ, Penninx BW.Anxiety and new onset of cardiovascular disease: critical review and meta-analysis. Br J Psychiatry 2016;208:223–31.
50. Emdin CA, Odutayo A, Wong CX,Tran J, Hsiao AJ, Hunn BH. Metaanalysis of anxiety as a risk factor for cardiovascular disease. Am J Cardiol 2016;118:511–9.
51. Somers JM, Goldner EM, Waraich P, Hsu L. Prevalence and incidence studies of anxiety disorders: a systematic review of the literature.Can J Psychiatry 2006;51:100–13.
52. Campbell Burton CA, Murray J,Holmes J, Astin F, Greenwood D, Knapp P. Frequency of anxiety after stroke: a systematic review and meta-analysis of observational studies. Int J Stroke 2013;8:545–59.
53. Tully PJ, Cosh SM. Generalized anxiety disorder prevalence and comorbidity with depression in coronary heart disease: a meta-analysis.J Health Psychol 2013;18:1601–16.
54. Wang L, Fan J. The status and in fluential factors of depression and anxiety among 700 cardiovascular inpatients (in Chinese). Chin J Med Educ 2014;30:151–153.
55. Cui J, Liang X, Li C, Yu R, Guo SW, Yang Z, et al. Analysis of psychological status of 509 hospitalized patients with coronary artery disease (in Chinese). Jiangsu Med J 2009;35:1120–2.
56. Liang JJ, Huang H, Yang B, Wan J,Tang YH, Bao MW, et al. A crosssectional survey on the prevalence of anxiety symptoms in Chinese patients with premature ventricular contractions without structural heart disease. Chin Med J (Engl)2012;125:2466–71.
57. Roest AM, Martens EJ, Denollet J,de Jonge P. Prognostic association of anxiety post myocardial infarction with mortality and new cardiac events: a meta-analysis. Psychosom Med 2010;72:563–9.
58. Celano CM, Millstein RA,Bedoya CA, Healy BC, Roest AM, Huffman JC. Association between anxiety and mortality in patients with coronary artery disease: a meta-analysis. Am Heart J 2015;170:1105–15.
59. Joynt KE, Whellan DJ, O’Connor CM. Depression and cardiovascular disease: mechanisms of interaction.Biol Psychiatry 2003;54:248–61.
60. Carney RM, Freedland KE, Miller GE, Jaffe AS. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897–902.
61. Vogelzangs N, Seldenrijk A,Beekman AT, van Hout HP, de Jonge P, Penninx BW. Cardiovascular disease in persons with depressive and anxiety disorders. J Affect Disord 2010;125:241–8.
62. Hare DL, Toukhsati SR, Johansson P, Jaarsma T. Depression and cardiovascular disease: a clinical review.Eur Heart J 2014;35:1365–72.
63. Davies SJ, Allgulander C. Anxiety and cardiovascular disease. Mod Trends Pharmacopsychiatry 2013;29:85–97.
64. Goldston K, Baillie AJ. Depression and coronary heart disease: a review of the epidemiological evidence, explanatory mechanisms and management approaches. Clin Psychol Rev 2008;28:288–306.
65. Patel V, Xiao S, Chen H, Hanna F, Jotheeswaran AT, Luo D,et al. The magnitude of and health system responses to the mental health treatment gap in adults in India and China. Lancet 2017;388:3074–84.
66. Rozanski A. Psychosocial risk factors and cardiovascular disease:epidemiology, screening, and treatment considerations. Cardiovasc Innov Appl 2016;1:417–31.
67. Lichtman JH, Bigger JT, Jr.,Blumenthal JA, Frasure-Smith N, Kaufmann PG, Lespérance F,et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention,and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Psychiatric Association.Circulation 2008;118:1768–75.
68. Beck AT, Steer RA, Carbin MG.Psychome tric properties of the Beck Depression Inventory:twenty- five years of evaluation.Clin Psychol Rev 1988;8:77–100.
69. Zung WW. A rating instrument for anxie ty disorders. Psychosomatics 1971;12:371–9.
70. Mavrides N, Nemeroff C.Treatment of depression in cardiovascular disease. Depress Anxiety 2013;30:328–41.
71. Zeng, G, Fu C, Luan R. Analysis o f anxiety and depression among cardio-cerebrovascular disease patients in comprehensive hospitals(in Chinese). Chin J Public Health 2006;22:1141–2.
72. Tully PJ, Baumeister H.Collaborative care for comorbid depression and coronary heart disease: a systematic review and meta-analysis of randomised controlled trials. BMJ Open 2015;5:e009128.
 Cardiovascular Innovations and Applications2017年1期
Cardiovascular Innovations and Applications2017年1期
- Cardiovascular Innovations and Applications的其它文章
- Inherited Cardiomyopathies: Genetics and Clinical Genetic Testing
- The Role of Echocardiography in Hypertrophic Cardiomyopathy
- Rationale and Design of the Randomized Controlled Trial of Intensive Versus Usual ECG Screening for Atrial Fibrillation in Elderly Chinese by an Automated ECG System in Community Health Centers in Shanghai(AF-CATCH)
- Clinical Utility of Amlodipine/Valsartan Fixed-Dose Combination in the Management of Hypertension in Chinese Patients
- The Effect of Home-Based Cardiac Rehabilitation on Functional Capacity,Behavior, and Risk Factors in Patients with Acute Coronary Syndrome in China
- Catheter Ablation of Atrial Fibrillation:Where Are We?