
Role of Second-Generation Drug-Eluting Stents and Bypass Grafting in Coronary Artery Disease: A Systematic Review and Meta-analysis
2017-05-26 03:12LinjuanGuoMDYingDingMDFuweiLiuMDWengenZhuMDandXinghuaJiangMDPhD
Linjuan Guo, MD, Ying Ding, MD, Fuwei Liu, MD, Wengen Zhu, MD and Xinghua Jiang, MD, PhD
1 Department of Cardiovascular Medicine, the Second Affiliated Hospital of Nanchang University, Nanchang of Jiangxi,330006, China
aLinjuan Guo, Ying Ding are co- first authors.
Introduction
Coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) are treatment options for patients with coronary artery disease(CAD) [1]. For the past 30 years, CABG was seen as a better choice compared with PCI therapy for CAD by improving the long-term prognosis [2]. PCI has gradually matured and developed to include drugeluting stents (DESs), and newer PCI further fueled the lowering of restenosis rates [3]. Since 2002,two types of first-generation DESs – sirolimuseluting stents and paclitaxel-eluting stents – have been used in the treatment of CAD [4]. Previous meta-analyses have compared CABG and first-generation DESs as treatments for CAD [5–9]. These studies have indicated that CABG might be more efficacious than first-generation DESs in reducing the risk of death, myocardial infarction (MI) and revascularization, although CABG is associated with an increased risk of stroke. With the introduction of second-generation DESs, which include zotarolimus-eluting stents (ZESs) and everolimuseluting stents (EESs), researchers have started to compare the role of second-generation DESs with that of CABG. In 2012, Kim et al.[10] first showed that second-generation DESs are associated with a similar risk of major adverse cardiac and cerebrovascular events (MACCEs; mainly including death,MI, revascularization, and stroke) as for CABG for CAD patients after 2 years of follow-up [10].Increasing numbers of studies have been designed to compare CABG with second-generation DESs[11–14]. Therefore we aimed to perform a systematic review and meta-analysis to compare the outcomes with regard to second-generation DESs and CABG for patients with CAD.
Methods
Study Selection
The inclusion criteria for eligible trials included the following:
1. Types of studies: randomized controlled trials (RCTs) and nonrandomized controlled trials(NRCTs) comparing the safety and efficacy of CABG and second-generation DESs. Studies with a follow-up time of less than 1 year were excluded.
2. Study participants: patients with CAD (diagnostic coronary angiography showing severe stenosis of 70% or more in major epicardium coronary arteries [11] and/or diagnostic coronary angiography showing unprotected stenosis of more than 50% of the diameter of the left main coronary artery [15]).
3. Outcomes: all-cause death, cardiovascular death,MI, revascularization, stroke and MACCEs.
The following exclusion criteria were applied:
1. Studies including participants who had undergone other cardiac surgery (valve surgery or CABG) because these patients are less likely to undergo repeated CABG than be treated with a second-generation DES.
2. Duplicate studies, basic research studies, and certain publication types (e.g., review, letter,case report, comment).
3. Studies with insufficient data and for which we were unable to obtain sufficient data because the author could not be contacted or did not reply.
Literature Search Strategy
We performed a systematic search using the PubMed, Cochrane Library, Ovid, and Elsevier databases for studies comparing the safety and ef fi cacy of CABG and second-generation DESs in patients with CAD. There were no language restrictions. The search of the databases was done from their inception through December 2016 with the terms “coronary artery bypass graft,” “drug-eluting stents,” “everolimus-eluting stents,” “second-generation drug-eluting stents,” “zotarolimus-eluting stents,” “coronary artery disease,” “unprotected left main coronary artery disease,” and “multivessel disease.” Then we manually searched the conference abstracts, relevant reviews, reference lists, and relevant journals to identify additional studies. We contacted the author via e-mail for studies that did not report outcomes of interest.
Data Extraction and Quality Assessment
Studies were retrieved by our searching electronic and manual databases. Three independent reviewers (L.G., Y.D., and W.Z.) assessed the reports independently for their eligibility on the basis of the title or the abstract. In the case of discrepancies, issues were resolved through discussion or supervised by a fourth investigator (X.J.) if needed. Data extraction was standardized, and all disagreements were resolved by consensus. Pertinent data were extracted according to the prespecified forms: journal, first author, year of publication, country, location of the study group, source of controls, baseline clinical and interventional features. We assessed the quality of NRCT studies following the methodological standards of the Newcastle-Ottawa scale [16] and the quality of RCT studies following the methodological standards of the Cochrane Collaboration [17].
Risk of Bias and Consistency Test
Two independent reviewers (L.G. and Y.D.) assessed the risk of bias to determine the quality of the studies included. The risk of bias was determined according to the risk of publication bias assessment tool developed by the Cochrane Collaboration. Heterogeneity of the studies included was quantified by theI2statistic. According to Higgins’s method,I2≤25% indicated low heterogeneity,I2greater than 25% but not greater than 50% indicated intermediate heterogeneity, andI2>50% indicated high heterogeneity. Afixed-effects model analysis was used whenI2≤50%, and ifI2>50%, a random-effects model was used. In this regard, the results should be interpreted cautiously. Sensitivity analysis was performed on the primary end points by our changing the effects model and adjusting the inclusion criteria. A funnel plot was used to examine potential publication bias for the outcomes.
Statistical Analysis
The data were extracted from applicable articles and were calculated with RevMan 5.3 from the Cochrane Collaboration (The Nordic Cochrane Center, Rigshospitalet, Denmark, http://ims.cochrane.org/revman). As the pooledI2≤50%, we used the fixed-effects model to assess the occurrence risk of the primary end points. The risk ratio(RR) and corresponding 95% confidence interval(CI) were calculated, and statistical significance was set at P≤0.05.
Results
Search Results and Study Characteristics
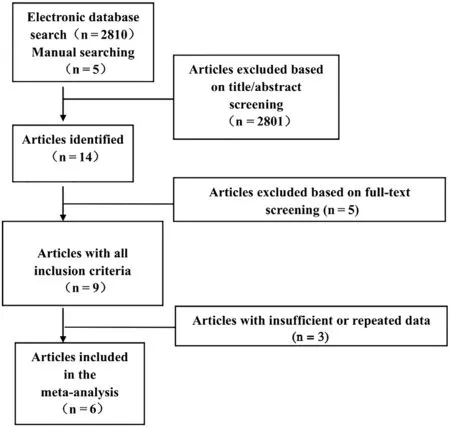
Figure 1 Overview of the Search Strategy.
As shown in Figure 1, 2815 potentially relevant articles were identified, 2801 of which were excluded after we read the titles and abstracts. Then the fulllength texts of 14 potentially relevant publications were assessed for eligibility. Of these, six articles[10, 11, 13–15, 18] fulfilled our eligibility criteria,and 6604 CAD patients treated with second-generation DESs (total number of participants 3295) or treated with CABG (total number of participants 3309) were included in the meta-analysis (Figure 1).No additional studies were found during our manual search of relevant reviews, published studies, and conference abstracts. Among the studies included,two were RCTs and four were NRCTs. Two of the four NRCT studies used propensity score matching to assemble a cohort of patients with similar baseline characteristics for statistical adjustment.Patients in four studies were treated with EESs, in one study patients were treated with ZESs, and in one study the type of second-generation DES was not mentioned. The basic characteristics of each of the studies included are summarized in Table 1.The reporting quality of the studies was globally acceptable; RCT studies were evaluated according to the methodological standards of the Newcastle-Ottawa scale [16] and NRCT studies were evaluated according to the methodological standards of the Cochrane Collaboration [17].
Meta-analysis
In our current meta-analysis, the RR and its 95%CI in each study are presented in Figure 2. There was no significant heterogeneity among the studies included (allI2<50%). Therefore all of the RRs and 95% CIs were pooled with use of a fixed-effects model in our meta-analysis.
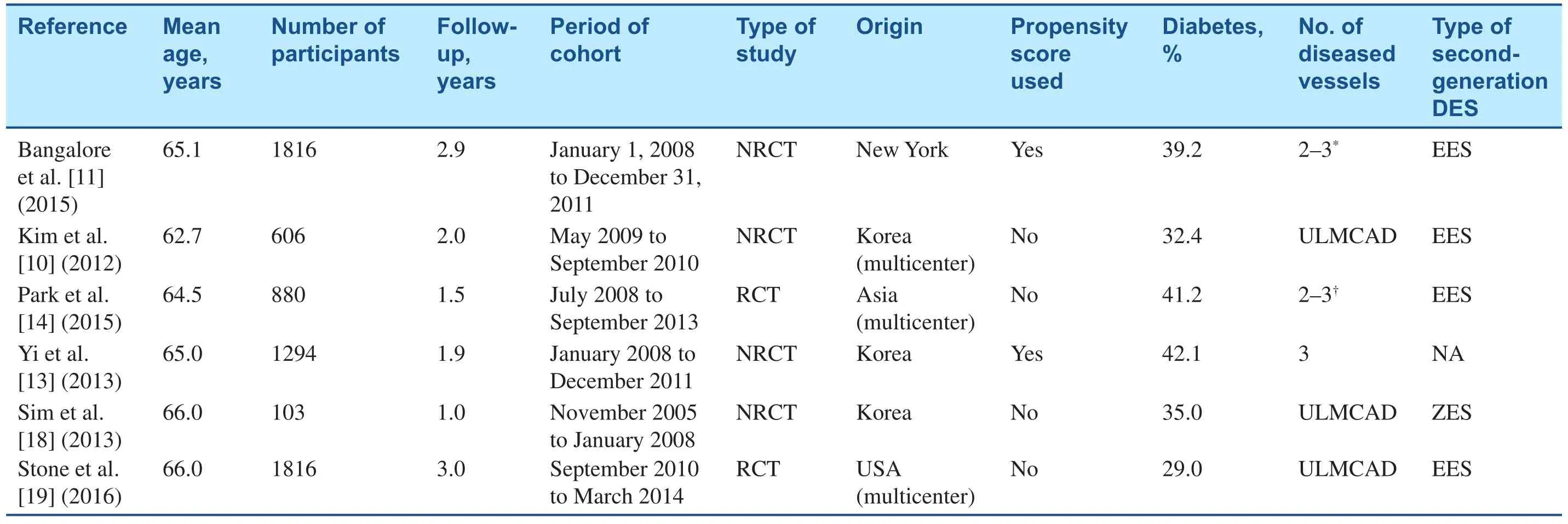
Table 1General Characteristics of All Studies Included in the Meta-analysis.
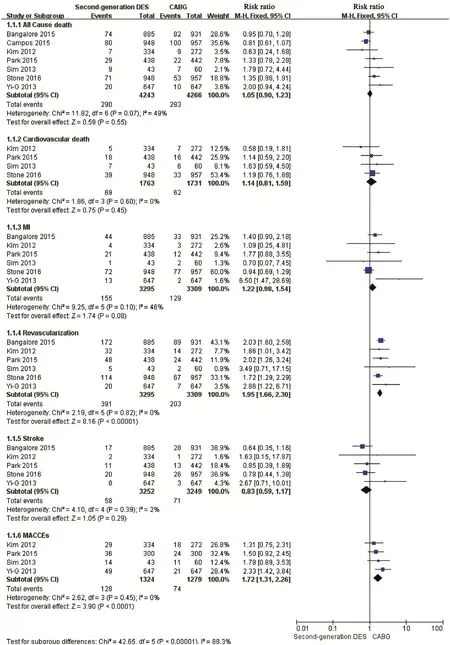
Figure 2 Forest Plot for Comparative Analysis of the Occurrence of All-cause Death, Cardiovascular Death, Myocardial Infarction, Revascularization, and Stroke in Coronary Artery Disease Patients Treated with Second-generation Drug-eluting Stents (DES) or Coronary Artery Bypass Grafting (CABG).
All-Cause Death
Six studies reported the outcome of all-cause death that occurred in 393 patients [10, 11, 13, 14, 18, 19].In the pooled results, the risk of all-cause death in the CAD patients treated with second-generation DESs was similar to that of patients treated with CABG(RR 1.18, 95% CI 0.98–1.43, P=0.09, Figure 2).
Cardiovascular Death
Four studies reported cardiovascular death in 3494 CAD patients [10, 14, 18, 19]. The pooled risk for cardiovascular death in the second-generation DES group showed no significant difference from that in the CABG group (RR 1.14, 95% CI 0.81–1.59,P=0.45, Figure 2).
Myocardial Infarction
Six studies reported the outcome of MI in 6604 patients [10, 11, 13, 14, 18, 19]. After we had pooled the data, the risk of MI in the second-generation DES group was not significantly different from that in the CABG group (RR 1.22, 95% CI 0.98–1.54,P=0.08, Figure 2).
Revascularization
Six studies met all the inclusion criteria [10, 11, 13,14, 18, 19]. Of these, one study [18] showed no significant difference between the second-generation DES group and the CABG group for revascularization. The other five studies [10, 11, 13, 14, 19] had a significant reduction of revascularization risk in the CABG group. As a result, the pooled risk for the incidence of revascularization in the second-generation DES group was 1.95-fold higher than that of the CABG group (RR 1.95, 95% CI 1.66–2.03,P<0.001, Figure 2).
Stroke
Data on the risk of stroke were available from five studies [10, 11, 13, 14, 19]. At the mean follow-up time, the pooled RR values demonstrated that there was no difference in the risk of stoke associated with second-generation DESs and that associated with CABG (RR 0.83, 95% CI 0.59–1.17, P=0.29,Figure 2).
Major Adverse Cardiac and Cerebrovas cular Events
Four studies (total number of patients 2603) were evaluated to compare the occurrence of MACCEs between second-generation DESs and CABG for treating CAD patients [10, 13, 14, 18]. There were no significant differences between second-generation DESs and CABG in relation to MACCEs in three of those studies [10, 14, 18]. In the other study, the second-generation DES group showed a higher risk of MACCEs than the CABG group [13].After pooling the data, we found that the risk of MACCEs in the second-generation DES group was higher than in the CABG group (RR 1.72, 95% CI,1.31–2.26,P<0.0001, Figure 2).
Publication Bias
We visually inspected the funnel plot for the outcomes of CAD patients treated with second-generation DESs and with CABG, and found that there was no potential publication bias (Figure 3).
Discussion
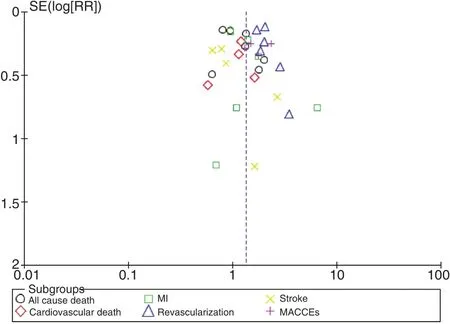
Figure 3 Funnel Plot of the Adverse Cardiovascular Outcomes for Second-Generation Drug-Eluting Stent and Coronary Artery Bypass Grafting Treatment in Patients with Coronary Artery Disease.
CAD is a leading cause of major adverse cardiac events, especially in industrialized nations [20].Therefore the optimal strategy for the treatment of CAD has received considerable attention. Earlier studies suggested that CABG was more efficacious than first-generation DESs in reducing the rates of death, MI, and revascularization, although CABG increased the rate of stroke [5, 21, 22]. With the introduction of second-generation DESs, numerous studies have compared major adverse cardiac events in individuals treated with a first-generation DES or a second-generation DES [23–25]. Because secondgeneration DESs have thinner struts, more biocompatible polymers, and improved deliverability [26],they are more efficacious than first-generation DESs in CAD patients. Meta-analytic combinations of these cohort studies have shown that second-generation DESs have reduced risk rates of all-cause death, MI, revascularization, and stroke compared with first-generation DESs [6, 27, 28]. Therefore,because of the longer-term safety and efficacy than first-generation DESs, second-generation DESs have been widely used. Since 2012, studies comparing the effectiveness of second-generation DESs and CABG have been conducted. Our study is the first meta-analysis to compare the clinical efficacy and safety of second-generation DESs versus CABG among CAD patients in terms of adverse cardiovascular outcomes. Using data from 6604 CAD patients,our meta-analysis shows that compared with CABG,second-generation DESs were associated with no difference in the rates of all-cause death, cardiovascular death, MI, and stroke, but were associated with increased rates of revascularization and MACCEs.
The major finding of this meta-analysis is that the use of second-generation DESs for CAD patients is as safe and effective as CABG, as shown by the same incidence of all-cause death, cardiovascular death, MI, and stroke. This result disagrees with the results of studies that compared first-generation DESs with CABG [29]. The risk of revascularization and MACCEs was higher after second-generation DES treatment than after CABG treatment in this analysis. These results are driven mainly by the following reasons. First, routine angiography followup after second-generation DES treatment has been shown to increase the risk of revascularization[30], and the data on the risk of revascularization play a large role in assessing the risk of MACCEs for CAD disease in the pooled results. Second,CAD patients with diabetes mellitus treated by CABG had a significantly reduced rate of MACCEs compared with patients treated with DESs [31]. Up to 36.8% of diabetic patients were included in each study of our meta-analysis, and we speculate that these results might be affected largely by diabetes.
The results of the present study demonstrate that the optimal treatment for CAD patients still needs to be identified. As second-generation DESs were associated with no difference in the rates of all-cause death, cardiovascular death, MI, and stroke compared with CABG, and could be applied more easily and expeditiously and have the potential advantage of providing more rapid reperfusion, this method is a good alternative in patients without diabetes and with less complex disease [32]. However, in the treatment of CAD patients with diabetes mellitus or complex disease, CABG is the optimal strategy because CABG could reduce the risks of revascularization and MACCEs [31]. To obtain more de finitive knowledge of the safety and efficacy of second-generation DESs and CABG for the treatment of patients with CAD, further study is needed.
Several limitations in this meta-analysis should be carefully addressed. First, our study did not obtain sufficient data to control for the type of antiplatelet drugs and the duration of antiplatelet therapy, which might have a significant impact on the results.Second, the studies included in this meta-analysis included patients with both mild and serious CAD,which might have in fluenced the different risks of major adverse cardiac events, therefore potential biases might exist in the clinical results. For example, we could not exclude the phenomenon that most of the patients with serious and complex disease were included in CABG groups. Third, it has been reported that diabetes might have an important role in major cardiovascular events [33]. We did not conduct a subgroup analysis of CAD patients with diabetes because of a lack of detailed information.Fourth, because of the limited number of studies and the limited availability of data, we included randomized and nonrandomized studies in this meta-analysis, although there was low heterogeneity between the studies selected.
Conclusions
We found that second-generation DESs have no differential efficacy compared with CABG in regard to all-cause death, cardiovascular death, MI, and stroke.These results suggest that CAD patients with an intermediate or high risk of stroke are best treated with a second-generation DES. By contrast, CABG reduces the risk of revascularization and MACCEs compared with second-generation DESs. As a result, CABG remains the optimal revascularization strategy for CAD patients with complex disease or diabetes.
Acknowledgements
Xinghua Jiang oversaw the entire project and revised the draft. Linjuan Guo, Ying Ding, and Fuwei Liu performed the systematic literature review, constructed the database, and analyzed the data. Linjuan Guo and Wengen Zhu drafted the first version of the manuscript. All authors took part in the interpretation of the results and prepared the final version of the manuscript. This work was supported by the National Natural Science Foundation of China (8153000545).
Conflict of Interest
The authors have no conflicts of interest.
REFERENCES
1 Costa F, Ariotti S, Valgimigli M,Kolh P, Windecker S. Perspectives on the 2014 ESC/EACTS guidelines on myocardial revascularization: fifty years of revascularization:where are we and where are we heading? J Cardiovasc Transl Res 2015;8:211–20.
2 Hillis LD, Smith PK, Anderson JL,Bittl JA, Bridges CR, Byrne JG,et al. 2011 ACCF/AHA guideline for coronary artery bypass graft surgery: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2011;124:2610–42.
3 Kandzari DE, Kini AS,Karmpaliotis D, Moses JW,Tummala PE, Grantham JA, et al.Safety and effectiveness of everolimus-eluting stents in chronic total coronary occlusion revascularization: results from the EXPERT CTO multicenter trial (Evaluation of the XIENCE Coronary Stent,Performance, and Technique in Chronic Total Occlusions). JACC Cardiovasc Interv 2015;8:761–9.
4 Windecker S, Stortecky S, Stefanini GG, Da CB, Rutjes AW, Di Nisio M, et al. Revascularisation versus medical treatment in patients with stable coronary artery disease: network meta-analysis. BMJ 2014;348:g3859.
5 Al AJ, Franck C, Filion KB,Eisenberg MJ. Coronary artery bypass graft surgery versus percutaneous coronary intervention with first-generation drug-eluting stents:a meta-analysis of randomized controlled trials. JACC Cardiovasc Interv 2014;7:497–506.
6 Dangas GD, Serruys PW, Kereiakes DJ, Hermiller J, Rizvi A, Newman W, et al. Meta-analysis of everolimus-eluting versus paclitaxeleluting stents in coronary artery disease: final 3-year results of the SPIRIT clinical trials program(Clinical Evaluation of the Xience V Everolimus Eluting Coronary Stent System in the Treatment of Patients with De Novo Native Coronary Artery Lesions). JACC Cardiovasc Interv 2013;6:914–22.
7 Capodanno D, Capranzano P, La Manna A, Tamburino C: Metaanalysis of everolimus-eluting stents versus first-generation drug-eluting stents in patients with left main coronary artery undergoing percutaneous coronary intervention. Int J Cardiol 2013;168:1718–9.
8 Ariyaratne TV, Ademi Z, Yap CH,Billah B, Rosenfeldt F, Yan BP,et al. Prolonged effectiveness of coronary artery bypass surgery versus drug-eluting stents in diabetics with multi-vessel disease:an updated systematic review and meta-analysis. Int J Cardiol 2014;176:346–53.
9 Athappan G, Patvardhan E, Tuzcu ME, Ellis S, Whitlow P, Kapadia SR. Left main coronary artery stenosis: a meta-analysis of drug-eluting stents versus coronary artery bypass grafting. JACC Cardiovasc Interv 2013;6:1219–30.
10 Kim YH, Park DW, Ahn JM,Yun SC, Song HG, Lee JY, et al.Everolimus-eluting stent implantation for unprotected left main coronary artery stenosis. The PRECOMBAT-2 (Premier of Randomized Comparison of Bypass Surgery versus Angioplasty Using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease) study. JACC Cardiovasc Interv 2012;5:708–17.
11 Bangalore S, Guo Y, Samadashvili Z, Blecker S, Xu J, Hannan EL.Everolimus-eluting stents or bypass surgery for multivessel coronary disease. N Engl J Med 2015;372:1213–22.
12 Campos CM, van Klaveren D,Farooq V, Simonton CA, Kappetein AP, Sabik JR, et al. Long-term forecasting and comparison of mortality in the Evaluation of the Xience Everolimus Eluting Stent vs. Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization (EXCEL)trial: prospective validation of the SYNTAX Score II. Eur Heart J 2015;36:1231–41.
13 Yi G, Joo HC, Youn YN, Hong S,Yoo KJ. Stent versus off-pump coronary bypass grafting in the secondgeneration drug-eluting stent era.Ann Thorac Surg 2013;96:535–41.
14 Park SJ, Ahn JM, Kim YH, Park DW, Yun SC, Lee JY, et al. Trial of everolimus-eluting stents or bypass surgery for coronary disease. N Engl J Med 2015;372:1204–12.
15 Park SJ, Kim YH, Park DW, Yun SC, Ahn JM, Song HG, et al.Randomized trial of stents versus bypass surgery for left main coronary artery disease. N Engl J Med 2011;364:1718–27.
16 Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses.Eur J Epidemiol 2010;25:603–5.
17 Robertson C, Ramsay C, Gurung T, Mowatt G, Pickard R, Sharma P. Practicalities of using a modifi ed version of the Cochrane Collaboration risk of bias tool for randomised and non-randomised study designs applied in a health technology assessment setting. Res Synth Methods 2014;5:200–11.
18 Sim DS, Ahn Y, Jeong MH, Kim YJ,Chae SC, Hong TJ, et al. Clinical outcome of unprotected left main coronary artery disease in patients with acute myocardial infarction.Int Heart J 2013;54:185–91.
19 Stone GW, Sabik JF, Serruys PW,Simonton CA, Genereux P, Puskas J, et al. Everolimus-eluting stents or bypass surgery for left main coronary artery disease. N Engl J Med 2016;375:2223–35.
20 Davierwala PM, Mohr FW. Surgical versus percutaneous revascularization in patients with multivessel coronary artery disease. Curr Atheroscler Rep 2014;16:461.
21 Kappetein AP, Feldman TE,Mack MJ, Morice MC, Holmes DR, Stahle E, et al. Comparison of coronary bypass surgery with drug-eluting stenting for the treatment of left main and/or threevessel disease: 3-year follow-up of the SYNTAX trial. Eur Heart J 2011;32:2125–34.
22 Sa MP, Ferraz PE, Escobar RR,Nunes EO, Soares AM, Araujo ESF,et al. Five-year outcomes following PCI with DES versus CABG for unprotected LM coronary lesions:meta-analysis and meta-regression of 2914 patients. Rev Bras Cir Cardiovasc 2013;28:83–92.
23 Pendyala L, Loh J, Kitabata H,Minha S, Chen F, Torguson R,et al. Clinical impact of secondgeneration everolimus-eluting stents compared with first-generation drug-eluting stents in diabetic patients undergoing multivessel percutaneous coronary intervention. J Invasive Cardiol 2015;27:263–8.
24 Stone GW, Rizvi A, Newman W,Mastali K, Wang JC, Caputo R,et al. Everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease. N Engl J Med 2010;362:1663–74.
25 Kedhi E, Gomes M, Joesoef KS,Wassing J, Goedhart D, McFadden E, et al. Everolimus-eluting stents and paclitaxel-eluting stents in patients presenting with myocardial infarction: insights from the two-year results of the COMPARE prospective randomised controlled trial. Eurointervention 2012;7:1376–85.
26 Kolandaivelu K, Swaminathan R, Gibson WJ, Kolachalama VB,Nguyen-Ehrenreich KL, Giddings VL, et al. Stent thrombogenicity early in high-risk interventional settings is driven by stent design and deployment and protected by polymer-drug coatings. Circulation 2011;123:1400–9.
27 Lanka V, Patel VG, Saeed B, Kotsia A, Christopoulos G, Rangan BV,et al. Outcomes with first- versus second-generation drug-eluting stents in coronary chronic total occlusions (CTOs): a systematic review and meta-analysis. J Invasive Cardiol 2014;26:304–10.
28 Gorla R, Lof fi M, Verna E,Margonato A, Salerno-Uriarte J.Safety and efficacy of first-generation and second-generation drug-eluting stents in the setting of acute coronary syndromes. J Cardiovasc Med (Hagerstown)2014;15:532–42.
29 Smit Y, Vlayen J, Koppenaal H,Eefting F, Kappetein AP, Mariani MA. Percutaneous coronary intervention versus coronary artery bypass grafting: a meta-analysis. J Thorac Cardiovasc Surg 2015;149:831–8.
30 Yu XP, Wu CY, Ren XJ, Yuan F,Song XT, Luo YW, et al. Very long-term outcomes and predictors of percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting for patients with unprotected left main coronary artery disease. Chin Med J (Engl) 2016;129:763–70.
31 Qi X, Xu M, Yang H, Zhou L, Mao Y, Song H, et al. Comparing mortality and myocardial infarction between coronary artery bypass grafting and drug-eluting stenting in patients with diabetes mellitus and multivessel coronary artery disease: a meta-analysis. Arch Med Sci 2014;10:411–8.
32 Mohr FW, Morice MC, Kappetein AP, Feldman TE, Stahle E,Colombo A, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease:5-year follow-up of the randomised,clinical SYNTAX trial. Lancet 2013;381:629–38.
33 Martin DM, Boyle FJ. Drugeluting stents for coronary artery disease: a review. Med Eng Phys 2011;33:148–63.
 Cardiovascular Innovations and Applications2017年1期
Cardiovascular Innovations and Applications2017年1期
- Cardiovascular Innovations and Applications的其它文章
- Hospitalization for Congenital Heart Disease in Beijing: Patient Characteristics and Temporal Trends
- The Effect of Home-Based Cardiac Rehabilitation on Functional Capacity,Behavior, and Risk Factors in Patients with Acute Coronary Syndrome in China
- Catheter Ablation of Atrial Fibrillation:Where Are We?
- Antithrombotic Therapy: Focus on the Elderly
- Inherited Cardiomyopathies: Genetics and Clinical Genetic Testing
- Depression, Anxiety, and Cardiovascular Disease in Chinese: A Review for a Bigger Picture