钩骨-掌骨关节骨折背侧脱位患者的跨关节桥接钢板内固定治疗
2017-04-24 08:16:43李忠哲郜永斌田光磊
中国骨与关节杂志 2017年4期
李忠哲 郜永斌 田光磊
钩骨-掌骨关节骨折背侧脱位患者的跨关节桥接钢板内固定治疗
李忠哲 郜永斌 田光磊
目的介绍应用跨关节桥接钢板内固定技术治疗钩骨-掌骨关节骨折背侧脱位的手术技术及疗效。方法 2008 年 8 月至 2015 年 12 月,应用跨关节桥接钢板内固定技术治疗 55 例钩骨-掌骨关节骨折背侧脱位患者。采用 Cain 分型,其中 I A 型 8 例,I B 型 27 例,II 型 13 例,III 型 7 例。应用 2.3 mm Stryker 微型直钢板,切开复位钩骨-掌骨关节骨折背侧脱位并跨钩骨和 4,5 腕掌关节固定,手术后行早期功能锻炼。术后 4 个月去除钢板。结果 术后所有患者获随访 6~48 个月,平均 2.5 年。55 例骨折均顺利愈合,愈合时间平均 5.5 周。术后疼痛程度和关节活动度评价,优 39 例,良 14 例,可 2 例,差 0 例,优良率为 96.3%。术后未发生严重并发症和脱位复发。结论 应用跨关节桥接钢板内固定技术治疗钩骨-掌骨关节骨折背侧脱位,复位固定可靠,允许早期关节活动,无术后脱位复发和关节不稳定的风险,有效降低术后关节疼痛和关节活动受限,是治疗钩骨-掌骨关节骨折背侧脱位的有效方法。
钩骨;掌骨;骨折固定术,内;腕掌关节;手
钩骨-掌骨关节由第 4、5 掌骨基底及钩骨远端构成,即第 4、5 腕掌关节。钩骨-掌骨关节骨折背侧脱位并不常见,在手和腕部损伤中的比例不到1%[1]。但损伤类型复杂,除第 4、5 掌骨骨折脱位外常合并钩骨骨折和韧带损伤,且常为不稳定型骨折脱位[2-3]。传统的治疗方法采用闭合复位经皮克氏针内固定,存在关节内骨折不能精确复位,脱位复发,关节活动受限和继发骨性关节炎的缺点。对于不稳定类型的骨折脱位,很多学者倾向切开复位内固定手术,内固定方式包括克氏针螺钉钢板固定等,但大多为个案或小宗病例的报道[2,4-5]。2008年 8 月至 2015 年 12 月,我科采用切开复位桥接钢板内固定技术治疗钩骨-掌骨关节背侧骨折脱位55 例,疗效满意,报告如下。
资料与方法
一、临床资料
本组 55 例,男 42 例,女 13 例;左 26 例,右 29 例;年龄 18~54 岁,平均 36 岁。受伤距手术 2~21 天,平均 9 天。致伤原因主要为跌倒摔伤16 例,握拳击打伤 28 例以及交通车祸伤 11 例。所有病例均存在第 4、5 腕掌关节背侧肿痛,屈曲及对掌运动受限,握力降低,局部有压痛及异常活动。
本组所有患者均有明确外伤史,握拳击打伤为主要的致伤原因。所有病例均存在第 4、5 腕掌关节背侧肿痛,屈曲活动受限,握力降低,局部有压痛及异常活动。所有病例均拍摄后前正位,30°前后斜位和侧位 X 线片,43 例 ( 78% ) 得到明确诊断。其余 12 例 ( 22% ) 除 X 线外通过 CT 检查得到明确诊断。
二、影像学检查和临床分型
本组 55 例术前均摄后前正位,30° 前后斜位和侧位 X 线片,12 例行 CT 检查。临床分型根据放射学检查结果采用 Cain 分型将钩骨-掌骨关节骨折背侧脱位分为:存在第 4 掌骨骨折和第 5 腕掌关节骨折脱位或半脱位。I A 型,第 5 掌骨基底脱位或半脱位,伴随腕掌关节背侧韧带损伤;I B 型,第5 掌骨基底脱位或半脱位,伴随钩骨背侧撕脱骨折;II 型,钩骨背侧粉碎性骨折;III 型,钩骨冠状面劈裂骨折。
本组 55 例,根据 Cain 分型包括不稳定 I A 型8 例,I B 型 27 例,II 型 13 例,III 型 7 例。本组患者均采用跨关节桥接钢板技术,复位和固定第 4、5 腕掌关节,钢板呈 V 形固定第 4、5 掌骨和钩骨治疗。
三、手术方法及术后处理
第 4、5 掌骨间以钩骨-掌骨关节为中心作纵行皮肤切口,保护尺神经背侧支,并牵开环小指伸指肌腱和小指固有伸肌腱,显露 4、5 掌骨基底和钩骨背侧韧带撕裂和骨折。复位脱位的第 4、5 腕掌关节,探查并恢复第 5 腕掌关节关节面的平整,0.8 mm 克氏针临时固定。Stryker5 孔直板复位固定第 4 掌骨骨折并桥接固定第 4 腕掌关节,Stryker6 孔直板复位固定第 5 掌骨基底骨折并桥接固定第 5 腕掌关节,钢板呈 V 行近端固定于钩骨远半段,同时固定钩骨背侧撕脱骨块或冠状面骨折。3-0 可吸收线修复背侧损伤的韧带和关节囊,检查复位的稳定性和 X 线透视下观察关节复位情况,拔除或保留临时固定克氏针。术后采用腕关节支具固定 3 周,固定期间掌指关节可主动屈伸活动。术后 3 周拆除支具,开始主动活动腕关节。术后 4 个月拆除钢板。
四、随访
本组 55 例全部获 6~48 个月的随访,平均2.5 年。随访内容包括:握力 ( 与对侧对比 ),疼痛VAS 评分,手功能 DASH 评分。
疗效评价采用 Darrow 标准[6],优:与对侧相比活动充分,无疼痛和功能受限;良:与对侧相比活动轻微受限,用力时轻微不适;可:与对侧相比活动中度受限,用力时不适,功能受限不能完全恢复原工作;差:持续疼痛,功能活动受限不能恢复原工作或骨不愈合。
结 果
本组 55 例握力 ( 与对侧对比 ) 平均 93%。VAS评分平均为 1.1。DASH 评分平均为 3.5。55 例中,优39 例,良 14 例,可 2 例,差 0 例,优良率为 96.3% ( 表1 )。
本组 55 例骨折均愈合,平均愈合时间 5.5 周,钢板去除时间平均为 4 个月。随访期内关节脱位无复发和再脱位,2 例术后出现尺神经背支卡压症状,均于去除钢板后消失。3 例出现钢板断裂,断裂时间均在术后 1 年以上。在随访期内未发现退行性骨关节炎表现和钩骨缺血性坏死。

表1 本组疗效指标评估表Tab.1 Function evaluation results

图1 Cain I A 型钩骨 - 掌骨关节脱位图2 跨关节桥接钢板固定Fig.1 Cain type I A fracture-dislocation of the hamate-metacarpal articulationFig.2 Across-joint internal fixation using the bridging plate

图3 骨折愈合,关节脱位无复发图4 Cain I B 型钩骨 - 掌骨关节脱位Fig.3 After the operation fracture union and no recurrence of dislocationFig.4 Cain type I B fracture-dislocation of the hamate-metacarpal articulation
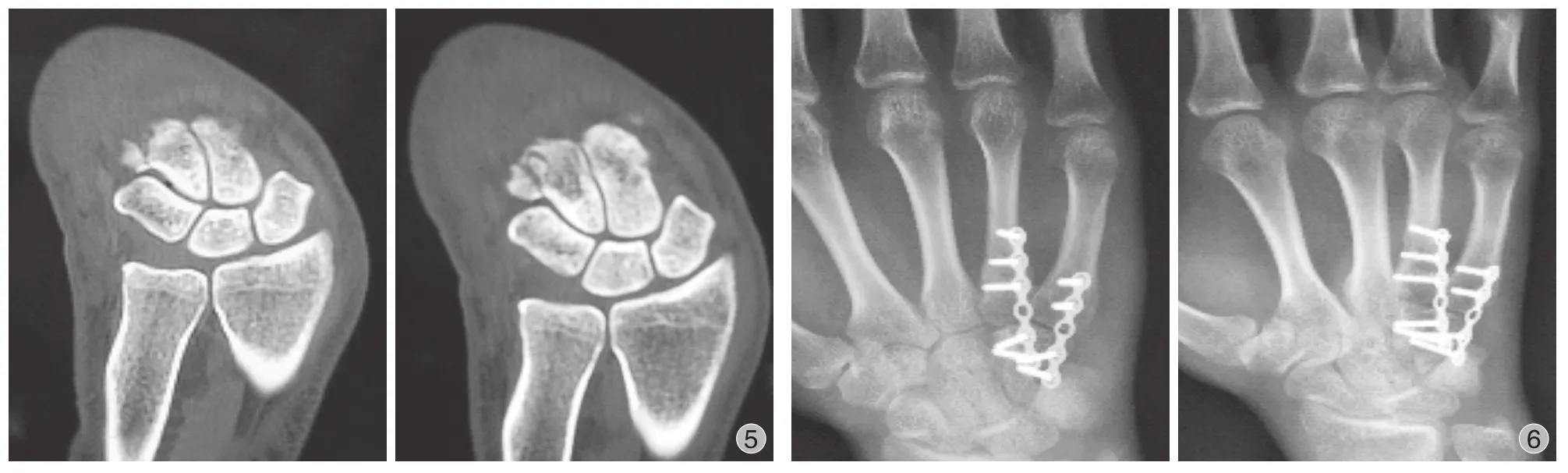
图5 钩骨 - 掌骨关节脱位,钩骨背侧撕脱骨折图6 骨折愈合,关节脱位无复发Fig.5 Dislocation of the hamate-metacarpal articulation with avulsion fracture of the dorsal hamateFig.6 After the operation fracture union and no recurrence of dislocation
讨 论
钩骨-掌骨关节骨折背侧脱位是多种损伤的总称,包括第 4、5 掌骨基底骨折和 ( 或 ) 脱位、钩骨远端关节面骨折或韧带损伤,有着多种组合类型。其发生率虽不高,文献报道大多为个案和小宗病例报道,但可严重影响手的功能,理应予以足够的重视[5,7-8]。由于钩骨-掌骨关节骨折背侧脱位临床症状和体征缺少特异性,常规 X 线检查常难以诊断,漏诊时有发生[4,7,9]。第 4、5 腕掌关节活动幅度15°~30°,参与手横弓、纵弓构成,是完成握物功能不可缺少的条件[5,9-10]。钩骨-掌骨关节骨折背侧脱位发生后,关节稳定性受到破坏,如不熟悉该部位的局部解剖和 X 线片的影像特征,则可能满足于骨折或脱位的诊断而易漏诊,造成患者的手功能障碍及畸形。
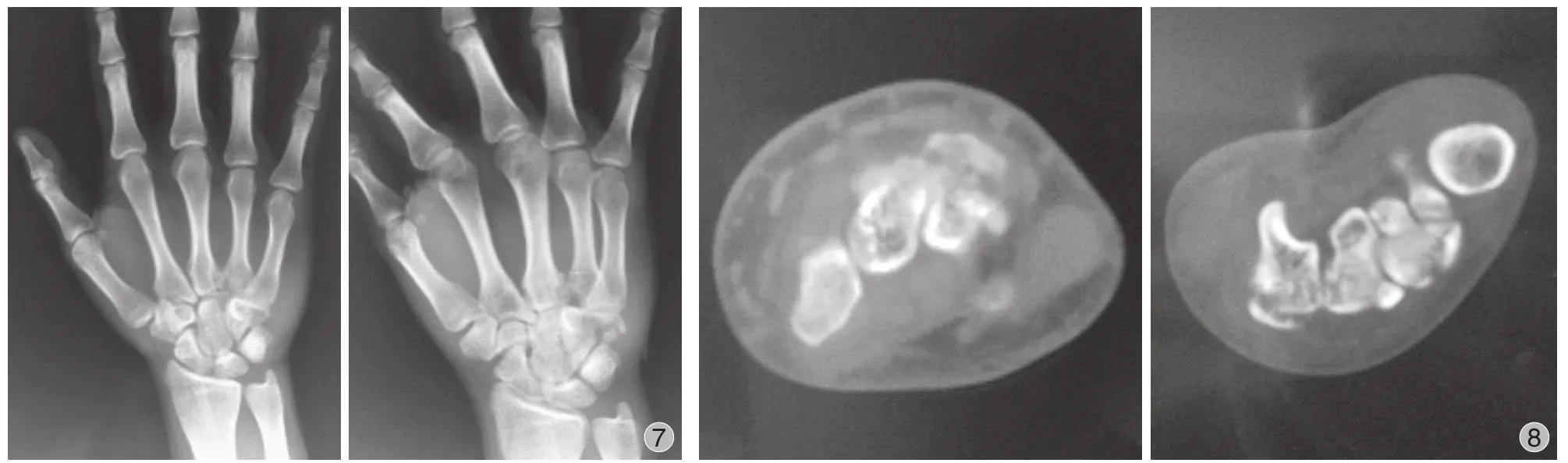
图7 Cain II 型钩骨 - 掌骨关节脱位图8 钩骨 - 掌骨关节脱位,钩骨背侧粉碎性骨折Fig.7 Cain type II fracture-dislocation of the hamate-metacarpal articulationFig.8 Dislocation of the hamate-metacarpal articulation with comminuted fracture of the dorsal hamate

图9 骨折愈合,关节脱位无复发图10 Cain III 型钩骨 - 掌骨关节脱位Fig.9 After the operation fracture union and no recurrence of dislocationFig.10 Cain type III fracture-dislocation of the hamate-metacarpal articulation

图11 钩骨 - 掌骨关节脱位,钩骨冠状面劈裂骨折图12 骨折愈合,关节脱位无复发Fig.11 Dislocation of the hamate-metacarpal articulation with coronal fracture of the hamateFig.12 After the operation fracture union and no recurrence of dislocation
钩骨-掌骨关节骨折背侧脱位类型复杂,有多种组合,目前还缺乏一个系统的分类。文献中已有的分类,都是针对某一型损伤的。绝大多数钩骨骨折会伴发第 4 和 ( 或 ) 第 5 掌骨基底背侧脱位或半脱位[3,8],为此,Cain 等[3]将钩骨-掌骨关节骨折背侧脱位分为:存在第 4 掌骨骨折和第 5 腕掌关节的脱位或半脱位。I A 型,第 5 掌骨基底脱位或半脱位,伴随腕掌关节背侧韧带损伤;I B 型,第 5 掌骨基底脱位或半脱位,伴随钩骨背侧撕脱骨折;II 型,钩骨背侧粉碎性骨折;III 型,钩骨冠状面劈裂骨折。本组病例 55 例中 I B 型最多,II 型次之,I A 型和III 型最少。

图13 术后 1 年功能恢复情况Fig.13 After operation, recovery of the function of the hand
钩骨-掌骨关节背侧骨折脱位,既可由直接暴力所致也可源于间接暴力,如手握拳击打硬物、摔倒后手着地,以及摩托车车祸伤等[2-3,9]。其中,拳击硬物最常见。诊断主要依靠放射学检查,其中X 线片摄影最常用,如腕关节后前、前后正位及侧位 X 线片,但对钩骨-掌骨关节骨折脱位则由于骨影重叠而不能很好地显示。Bora 等[5]认为正位投照第 5 掌骨基底和钩骨会有部分骨影重叠,无移位或轻度移位者容易漏诊,而 30° 前后斜位投照,则可以清楚地显示掌骨和钩骨的关节面。Niechajev[2]发现旋前 60° 斜位可清楚显示第 5 掌骨基底,而旋后60° 更佳,可以清楚显示第 4、5 掌骨基底间关节,因此 30° 前后斜位投照对第 4、5 腕掌关节损伤的诊断具有重要意义。Henderson 等[4]认为侧位 X 线片更有诊断价值,原因是有部分病例的正、斜位 X 线片基本正常,只有侧位 X 线片上能表现出脱位。综上所述,通过后前正位、30° 前后斜位及侧位摄影,多可准确评估第 4、5 腕掌关节损伤的范围和程度,诊断不清者需做 CT 检查[8]。本组所有病例均拍摄后前正位,30° 前后斜位和侧位 X 线片,43 例 ( 78% )得到明确诊断。其余 12 例 ( 22% ) 除 X 线外通过 CT检查得到明确诊断。
钩骨-掌骨关节骨折背侧脱位的治疗,一直存在争议,但随着解剖和生物力学研究的进展,早期诊断、早期采取适当的治疗已经成为共识。第 4、5 掌骨基底骨折和背侧脱位或半脱位大多数会伴发钩骨骨折,由于腕掌关节背侧的稳定结构遭到破坏,虽然复位比较容易,但维持复位却比较困难,是一种不稳定骨折。因此越来越多的学者倾向使用内固定治疗此损伤,是否需要切开复位,则应根据损伤的类型和程度区别对待[9-13]。Marck 等[11]把切开复位内固定的指征定义为:( 1 ) 闭合复位失败者;( 2 ) 开放损伤或并发严重软组织损伤者;( 3 )陈旧损伤。Henderson 等[4]认为,病程不足 10 天者闭合复位常可成功,超过 3 周者则往往需要切开复位。Prokuski 等[14]认为,闭合复位失败的主要原因是软组织过度肿胀以及软组织或碎骨片嵌顿,而切开复位可有效清理关节内碎屑,评估小的骨软骨损伤并进行治疗,可以准确地复位。
第 4 或第 5 掌骨基底关节内骨折,闭合复位克氏针内固定虽然牢靠,但复位难以精确[9]。即使闭合复位成功,关节仍然不稳定,仍有较高的再脱位比率。使用克氏针固定时,一旦发生移位,会导致固定失效。穿针时可能影响伸肌装置的滑动,影响环、小指掌指关节的伸直,可能导致环小指近指间关节出现屈曲畸形[12]。骨折块较大者,可用螺钉、Herbert 钉固定,虽需再次手术取内固定,但可早期功能活动,这一点要优于克氏针[9-10]。使用螺钉固定,骨折块直径应至少为螺钉直径的 3 倍,否则容易碎裂[15]。掌骨基底和 ( 或 ) 钩骨背侧粉碎骨折者,用 AO 微型钢板跨腕掌关节固定是一种好的选择[9,11]。通过桥接腕掌关节内固定可有效撑开关节,在直视下精确复位关节内骨折,恢复关节面平整,同时复位和固定钩骨背侧关节内骨折或冠状面劈裂骨折,其固定可靠,关节稳定,可早期功能活动。Schortinghuis[9]使用此法治疗 5 例第 4、5 腕掌关节骨折背侧脱位患者,平均 3.6 个月取出钢板,3 例手功能完全恢复,2 例腕关节背伸轻度受限。第 4、5 腕掌关节骨折背侧脱位伴发的钩骨骨折一般为冠状面骨折,且多发生于远端,很少发生不愈合和骨坏死。桥接钢板固定钩骨一般位于钩骨远端,不妨碍钩骨的血运,内固定不会造成钩骨近端坏死。
对于 Cain I A 型骨折应先尝试闭合复位,并于复位后测试稳定性,稳定者用石膏或支具外固定,不稳定者经皮穿克氏针固定。I B 型骨折多不稳定,保守治疗很难获得好的疗效,且于 X 线片上容易低估钩骨骨折块的大小,宜采用切开复位内固定术。II 型骨折属不稳定骨折,应做切开复位,并重建钩骨背侧的稳定结构。III 型损伤最容易漏诊,也最不稳定,需要切开复位内固定[3]。本组 55 例均为不稳定型骨折的病例,其中包括 8 例 I A 型骨折复位后仍不稳定的病例,本组病例均采用桥接钢板固定骨折和脱位,取得了非常满意的疗效。尤其是相对于克氏针或螺钉固定,复位更加稳定和精确,可满足早期功能锻炼的要求。在随访过程中没有发现再脱位和不稳定的情况出现,在整个随访期间也没有发现出现术后创伤性关节炎的病例。虽然本方法疗效满意,但也存在治疗费用相对较高,术后须行钢板去除手术的缺点。建议术后 4 个月取出钢板,如果超过 1 年,钢板断裂的风险将明显增加。
应用跨关节桥接钢板内固定技术治疗钩骨-掌骨关节骨折背侧脱位,复位固定可靠,允许早期关节活动,无术后脱位复发和关节不稳定的风险,有效降低术后关节疼痛和关节活动受限,是治疗钩骨-掌骨关节骨折背侧脱位的有效方法。
[1] Dobyns JH, Linscheid RL, Cooney WP 3rd. Fractures and dislocations of the wrist and hand, then and now[J]. J Hand Surg Am, 1983, 8(5 Pt 2):687-690.
[2] Niechajev I. Dislocated intra-articular fracture of the base of the fifth metacarpal:a clinical study of 23 patients[J]. Plast Reconstr Surg, 1985, 75(3):406-410.
[3] Cain JE, Shepler TR, Wilson MR. Hamatometacarpal fracturedislocation: classification and treatment[J]. J Hand Surg, 1987, 12(5 Pt 1):762-767.
[4] Henderson JJ, Arafa MA. Carpometacarpal dislocation. An easily missed diagnosis[J]. J Bone Joint Surg Br, 1987, 69(2):212-214.
[5] Bora FW Jr, Didizian NH. The treatment of injuries to the carpometacarpal joint of the little finger[J]. J Bone Joint Surg Am, 1974, 56(7):1459-1463.
[6] Darrow JC Jr, Linscheid RL, Dobyns JH, et al. Distal ulnar recession for disorders of the distal radioulnar joint[J]. J Hand Surg Am, 1985, 10(4):482-491.
[7] Langenhan R, Hohendorff B, Probst A. Coronal fracture dislocation of the hamate and the base of the fourth metacarpal bone: a rare form ofcarpometacarpal injury[J]. Handchir Mikrochir Plast Chir, 2011, 43(3):140-146.
[8] Kim JK, Shin SJ. A novel hamatometacarpal fracturedislocation classification system based on CT scan. Injury, 2012, 43(7):1112-1117.
[9] Schortinghuis J. Open reduction and internal fixation of combined fourth and fifth carpometacarpal (fracture) dislocations[J]. J Trauma, 1997, 42(6):1052-1055.
[10] Liaw Y, Kalnins G, Kirsh G. Combined fourth and fifth metacarpal fracture and fifth carpometacarpal joint dislocation[J]. J Hand Surg, 1995, 20(2):249-252.
[11] Marck KW, Klasen HJ. Fracture-dislocation of the hamatometacarpal joint: a case report[J]. J Hand Surg, 1986, 11(1):128-130.
[12] Kjaer-Petersen K, Jurik AG, Petersen LK. Intra-articular fractures at the base of the fifth metacarpal:a clinical and radiographical study of 64 cases[J]. J Hand Surg, 1992, 17(2):144-147.
[13] Van Demark RE, Parke WW. Avascular necrosis of the hamate: a case report with reference to the hamate blood supply[J]. J Hand Surg, 1992, 17(6):1086-1090.
[14] Prokuski LJ, Eglseder WA Jr. Concurrent dorsal dislocations and fracture-dislocations of the index:long:ring:and small (second to fifth) carpometacarpal joints[J]. J Orthop Trauma, 2001, 15(8):549-554.
[15] Freeland AE, Finley JS. Displaced dorsal oblique fracture of the hamate treated with a cortical mini lag screw[J]. J Hand Surg, 1986, 11(5):656-658.
( 本文编辑:李贵存 )
Treatment of fracture-dislocation of the hamate-metacarpal articulation with across-joint internal fixation usingthe bridging plate technique
LI Zhong-zhe, GAO Yong-bin, TIAN Guang-lei. Department of Hand Surgery, Beijing Jishuitan Hospital, Beijing, 100035, China
Objective To introduce the clinical application results and surgical technique in the treatment of fracture-dislocation of the hamate-metacarpal articulation with across-joint internal fixation using the bridging plate technique. Methods From August 2008 to December 2015, 55 cases of fracture-dislocation of the hamate-metacarpal articulation were treated with this kind of method and followed up. According to Cain type, there were 8 cases of type I A, 27 cases of type I B, 13 cases of type II and 7 cases of type III. Open reduction and across-joint internal fixation were performed on fracture-dislocation of the hamate-metacarpal articulation using a 2.3mm Stryker bridging plate, as well as fixation of the 4th and 5th carpometacarpal joint. Early motion was allowed after the operation. The plate was removed at 4 months after the operation. Results All the cases were followed up for an average period of 2.5 years ( range: 6 - 48 months ). Fracture union was achieved successfully in all the cases, and the average union time was 5.5 weeks. Function evaluation was made according to pain degree and flexor and extensor activity of the wrist joint. There were 39 excellent cases, 14 good cases, 2 fair cases and 0 poor case. The overall excellent and good rate was 96.3%, and the clinical results were satisfactory without severe complications or recurrence of dislocation. Conclusions Treatment of fracture-dislocation of the hamate-metacarpal articulation with across-joint internal fixation using the bridging plate technique is better than conventional methods. This technique avoids redislocation and instability of the hamate-metacarpal joint. It is allowed to begin early active motion of the wrist joint, and meanwhile strong and stable fixation can be achieved. Postoperative joint pain can be relived and limited joint activity can be avoided. It is an effective method in treatment of fracture-dislocation of the hamate-metacarpal articulation.
Hamate bone; Metacarpal bone; Fracture fixation, internal; Carpometacarpal joint; Hand
10.3969/j.issn.2095-252X.2017.04.004
R683.4
100035 北京积水潭医院手外科
2017-01-18 )
猜你喜欢
实用手外科杂志(2022年2期)2022-08-31 09:47:26
汽车零部件(2021年4期)2021-04-29 01:47:10
中华养生保健(2020年8期)2021-01-14 01:14:04
西北园艺(果树)(2016年2期)2016-02-19 04:04:16
中国卫生标准管理(2015年25期)2016-01-14 09:29:32
新疆医科大学学报(2015年10期)2015-12-26 12:33:30
实用手外科杂志(2015年2期)2015-08-28 09:50:58
实用手外科杂志(2015年4期)2015-08-27 01:54:08
实用手外科杂志(2015年1期)2015-08-27 01:52:04
医学研究杂志(2015年8期)2015-06-22 14:00:56