
Effectiveness of some herbals on initial enamel caries lesion
2016-10-22 01:08:27GulcinBilginGocmenFundaYanikogluDilekTagtekinGeorgeStookeyBruceSchemehornOsmanHayran
Gulcin Bilgin Gocmen,Funda Yanikoglu,Dilek Tagtekin*,George K.Stookey,Bruce R.Schemehorn,Osman Hayran
1Kartal Kosuyolu Education and Research Hospital,Istanbul,Turkey
2Department of Restorative Dentistry,Marmara University,Istanbul,Turkey
3Therametric Technologies,Inc.,Noblesville,Indiana,USA
4Department of Health Science,Istanbul Medipol University,Istanbul,Turkey
Effectiveness of some herbals on initial enamel caries lesion
Gulcin Bilgin Gocmen1,Funda Yanikoglu2,Dilek Tagtekin2*,George K.Stookey3,Bruce R.Schemehorn3,Osman Hayran4
1Kartal Kosuyolu Education and Research Hospital,Istanbul,Turkey
2Department of Restorative Dentistry,Marmara University,Istanbul,Turkey
3Therametric Technologies,Inc.,Noblesville,Indiana,USA
4Department of Health Science,Istanbul Medipol University,Istanbul,Turkey
ARTICLE INFO
Article history:
in revised form 23 Feb,2nd revised form 24 Mar 2016
Accepted 10 Jun 2016
Available online 26 Aug 2016
Remineralization
Ginger
Rosemary
Chocolate
Honey
FluoreCam
QLF
Initial enamel lesion
Objective:To evaluate the effectiveness of herbal medicaments such as ginger,rosemary and honey on remineralization of initial enamel lesion.
Methods:Demineralized human enamel specimens were measured for baseline surface microhardness and fluorescence methods.Ten specimens in each of four groups were used in this in vitro recycling study with the following treatments which applied three times a day:1)sodium fluoride toothpaste(Ipana,Procter&Gamble,Turkey),2)gingerhoney(Arifoglu Herbals,Anzer Honey,Turkey),3)ginger-honey-chocolate(Bind Chocolate,Turkey),4)rosemary oil(Arifoglu Herbals,Turkey).Treatment regimens of demineralization and remineralization cycle were applied for 21 days.The post-treatment data were obtained by measurements of surface microhardness and fluorescence methods. Data were statistically analyzed by ANOVA test with Tukey's honest significant difference test.
Results:Enhanced remineralization was observed with several of the treatment systems including ginger+honey and rosemary.Significant differences between treatments were observed by microhardness and FluoreCam fluorescence assesment,compared to the positive control group(NaF dentifrice).Significantly,greater remineralization was observed with the honey+ginger treatment regimen.No significant differences between groups were observed using the fluorescence assessment method,quantitative lightinduced fluorescence.
Conclusions:Herbals(ginger,honey and rosemary)have enhanced remineralization of initial enamel lesion.
Original articlehttp://dx.doi.org/10.1016/j.apjtb.2016.08.005
1.Introduction
The first sign of tooth caries,opaque lesion defined as“subsurface enamel porosity from carious demineralization”is manifested clinically by a milky white opacity.This subsurface porosity is being caused by an imbalance between the dynamic biological processes of de-and remineralization.In minimally invasive dentistry paradigm,incipient enamel carious lesions should be treated with non-invasive remineralization strategies. On this purpose,topical gels,varnishes,mouthwashes and dentifrices contain fluoride being used by dentists for the treatment of white spot lesions[1].
Fluoride is proved agent for caries prophylaxis,however,excess use of fluoride causes fluorosis,and hardening of cartilage.Moreover,the usage of bactericides or antibacterial agents has several negative effects on gastrointestinal system with increased resistance to these chemicals.Due to financial situation,developing countries need biocompatible and cost effective preventive methods.Therefore,instead of using artificial antibiotics and bactericides,it has been proposed to use medicinal plant extracts which have an effect on causative bacteria of tooth decay[2].
Among natural food sources,ginger rhizome(Zingiber officinale Roscoe,Zingiberaceae)and rosemary(Rosmarinus officinalisL.,Lamiaceae)arenaturalherbalswiththeir antimicrobial activities.Additionally,they do not show any toxicity approved by‘generally recognized as safe'in the Food and Drug Administration of the United States.Pungent oil contents of these herbals harbor some polyphenolic ketones with many pharmacological activities.Their antifungal and antimicrobial effects on oral cavity pathogens have been reported in many studies[3-7].However,there is no study in current literature about the effect of these herbal medicaments on remineralization of initial enamel caries.
Another regimen used in most ancient cultures for nutritional and/or medicinal aim is honey.It is believed that honey is a nutrient and can be used as a drug for a long time.Honey is a supersaturated sugar solution with low water activity that does not support the growth of bacteria[8].The average pH value of honey is 3.9,and can show bacteriostatic effect on pathogens as most thrive at pH between 4.0 and 4.5[9].However,dilution of honey,for example by saliva will increase the pH and reduce this effect.On the other hand,dilution results in 2500-50000 times increase in enzyme activity and this glucose oxidase enzyme is the production of hydrogen peroxide,an oxidizing agent.Hydrogen peroxide is present in honey in small amounts,yetisstillveryeffectiveantibacterialagent compatible with cellular preservation[10].There are a few studies on efficacy of honey on oral pathogenic bacteria[11-13]and none is about effect of honey on remineralization of initial enamel caries.
Methylxanthines are plant-produced natural products.Most plants used for preparation of beverages on human consumption are enriched in methylxanthines[14].The antioxidants of Theobroma cacao beans have psychoactive effects at high amounts because of methylxanthines[15].Besides,theobromine could show protective effect on enamel surface of human molars as shown by a pilot study[16].This protection was attributed to carbohydrate content of cacao which can be metabolized and a trap for bacteria to protect dental enamel from caries.
The purpose of this study is to evaluate remineralization potential of herbals(ginger,rosemary and also honey).
In addition to our main purpose,we investigated the efficiency of new detection device(FluoreCam),for demineralization and remineralization of human dental enamel by microhardness,also quantitative light-induced fluorescence(QLF)systems.
2.Materials and methods
2.1.Enamel specimens and preparation of subsurface lesions
A total of 40 human enamel specimens were used in this study.Extracted teeth obtained from oral surgeons were used;the teeth were stored in 0.10%thymol solution immediately after extraction and maintained in this solution prior to use.The sound enamel specimens required for this study were 3 mm in diameter and 1.6-2.0 mm thick from surface of enamel.These enamel cores were mounted on acrylic rods.Surfaces of specimens were polished by a 600-grit grinding disk and with a slurry of 0.05μm gamma alumina polishing gel.Artificial subsurface carious lesions were formed on each enamel specimen by placing the specimens individually for 72 h at 37°C in 7.0 mL of a demineralizing solution containing lactic acid as 0.1 molar amount and Carbopol 907 as 0.2%,50%hydroxyapatitesaturated in volume and adjusted to pH 5.0 using NaOH[17]. This procedure resulted in lesions approximately 35-50μm in depth.
2.2.Study design
The specimens were divided randomly to six groups(10 specimens/group)withthetreatmentmaterials.Treatment regimen was designed with approximate pH oral environment and modified by Dunipace et al.[18].The demineralization and remineralization cycles showed episodes as observed in Table 1. Each cycle contained 3 h of demineralization to simulate the daily acidchallengesinoralcavity.Thesampleswerekeptinlaboratory produced saliva which consisted of 2.00 g/L methyl p-hydroxybenzoate,10.0 g/L sodium carboxymethyl cellulose,8.38 mmol/ L KCl,0.29 mmol/L MgCl2·6H2O,1.13 mmol/L CaCl2·2H2O,4.62 mmol/L KH2PO4,2.40 mmol/L K2HPO4;and adjusted pH was 7.0 using KOH and there was not any precipitation observed during the experiment[19].Repeated treatment regimen lasted during 21 days.This saliva was changed each day and these treatment materials were freshly prepared in every application. All the time except applications,the samples were kept in artificial saliva that was mixed by a magnetic stirring machine(Multipoint HP15P,Variomag,USA).
2.3.Treatment materials
Ipana,NaF toothpaste consisted of 1450 mg/kg fluoride and was used as a positive control group.Based on the previous studies that have found the minimum inhibition concentration(MIC)of ginger(5-8 mg/mL)[4,20],we used ginger in powder form(Arifoglu Herbals,Turkey)and applied 8 mg into 1 mg honey(Anzer honey,Turkey).Chocolate(Sokella,Turkey)was added as 1 mg into the mixture of ginger+honey.All materials were mixed homogeneously and applied on the surfaces by smearing.Rosemary(Arifoglu Herbals,Turkey)oil was applied with an applicator.All pastes were prepared freshly at each application of remineralization materials.
2.4.Assessment of mineral content-FluoreCam&QLF
Before and after each test period,assessments of the mineral content of demineralized area of each specimen were obtained using both the FluoreCam(Daraza,Corporate Headquarters,Indiana,USA)and QLF(Inspektor Pro,Inspektor Research Systems,Amsterdam,Holland)systems.Using the FluoreCam instrument,the images were collected with and withoutdehydration for 5 s and analyzed using the specially designed software.The parameters to be assessed included fluorescence loss(%),area(mm2)and lesion volume(mm2×%).Any significant change in fluorescence indicated that remineralization(or demineralization)had taken place.
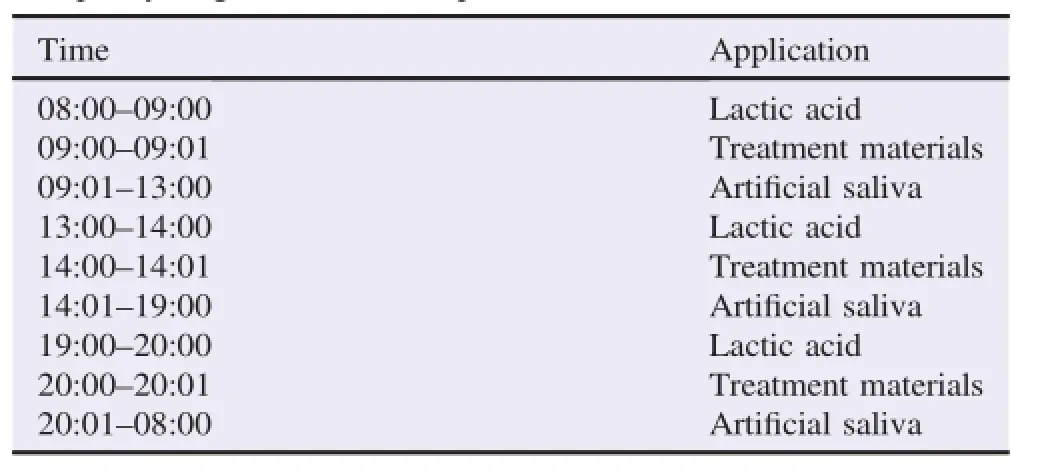
Table 1 The pH-cycling model in the experiment.
2.5.Surface microhardness measurements
Following the lesion formation procedure,the surface microhardness was measured(LECO LM247AT microhardness tester).The parameters were 200 g force for 15 s with a Vickers indenter.Four indentations were made on each specimen(one in each quadrant)and averaged for an average specimen value. This value had provided a baseline surface hardness value.By performing the indentations prior to the polycrystalline diamond inserts assessments,the indentation marks were in both the pretest and the post-test determinations.
Following the removal of the specimens,they were individually mounted on plexiglas rods as flat as possible so post-test hardness and mineral content determinations could be made. After the post-test polycrystalline diamond inserts measurements,the post-test surface microhardness indentations were made in the same manner as described above.Any significant increase in hardness over the test period was indicative for remineralization and any significant softening was indicative for demineralization.
2.6.Statistical analysis
For comparison of any remineralization effects of the treatment materials in each group,ANOVA repeated measures tests were conducted,with Tukey's multiple tests.The statistical analyses were processed using SPSS 15.0 for Windows(SPSS Inc.,Chicago,IL)with significant level of 0.001.
3.Results
Over time almost all treatment values in the groups were significantly higher than in the baseline following three weeks. The meanΔF(lesion depth)andΔQ(lesion volume)values(±SEM)for QLF were Ipana(1.01±1.22)%and(15.25± 8.75)%×mm2,ginger+;honey(1.89±0.57)%and(21.30± 6.67)%×mm2,ginger+honey+chocolate(0.38±1.03)%and(10.45±6.00)%×mm2,and rosemary oil(0.23±0.80)% and(4.55±4.56)%×mm2.Although all samples resulted in remineralization,there was not any significant difference between the groups with QLF(P>0.05).MeanΔF andΔQ values(±SEM)for FluoreCam were Ipana(3.53±2.05)%and(7.75±5.03)%×mm2,ginger+honey(12.12±1.72)%and(38.49±4.65)%×mm2,ginger+honey+chocolate(9.00±1.39)%and(27.22±2.84)%×mm2,and rosemary oil(7.86±1.39)%and(22.17±4.58)%×mm2.In contradiction for FluoreCam assessment,we observed significantly greater remineralization in ginger+honey group(P<0.001).
The surface microhardness results showed significant differencesbetweenalltreatmentmaterials.ThemeanVickershardness number values were Ipana(6.76±1.96),ginger+honey(11.69±1.19),ginger+honey+chocolate(10.72±2.34),and rosemary oil(2.72±3.71).Among all treatment materials,ginger+honey group showed the greatest remineralization(P<0.001).There was not significant difference between rosemaryoilgroupandNaFtoothpastebuttheresultsshowedthat rosemary oil group was almost equal on effect to positive control group,NaF toothpaste(P>0.05).Ginger+honey+chocolate group showed still some demineralization but there was no statistical difference with NaF toothpaste(P>0.05).
4.Discussion
Main process occurs at the outer layer of enamel which is principallyincontactwithoralenvironment[21].The remineralizingagentsappliedonthesurfaceofenamel specimens were evaluated by QLF,FluoreCam and surface microhardness test methods.They are quick,easy and simple,moreover nondestructive methods,giving the mineral changes following the treatments.In addition to these,they provide repeated measurements of same sample at any other time by eliminating any variation in the experiment.
QLF has shown great promise as an early caries detection method.The study concluded that it is suitable for monitoring mineral changes in vivo except the cost of the system[22].Also there are some factors confining its success such as dehydration[23]and angulation[24].It seems there is conflicting results with ginger+honey group which was found highly remineralized in microhardness and FluoreCam test methods(P<0.001)while QLFhasshownnosignificancebetweenthetreatment materials(P>0.05).The FluoreCam system is an innovative approach for quantification of enamel called fluorescence enamel imaging.Surface of a tooth is induced with a high intensity light and the instrument has sent the fluorescent image and measurements to a computer.Determining the suspected de-or remineralization area is automatically done by FluoreCam software.
Nowadays,more phytochemicals,especially antibacterial agents,have been derived from edible plants.Many reports revealed some antibacterial activities of ones,against Streptococcus mutans(S.mutans),main pathogen of dental caries. Ohara et al.searched 81 edible plants'antibacterial activities against S.mutans in polarity-differing solvents(hexane and ethyl acetate)and ginger is found to be effective(MIC 23 mg/g and 8 mg/g)[4].Moreover,after boiling 10 min at 100°C or afterstoragefor1weekat4°C,gingerprotectsits antibacterial activity[1].White found that in glycolic or hydroalcoholic solvents,5 mg/mL MIC of ginger is effective on S.mutans[17].Honey is potentially antibacterial agent and studies demonstrated that manuka honey is likely to be noncariogenic.Patel et al.reported ginger and honey are more effective than gentamycin on S.mutans.They found the MIC is ginger31.25mg/mL,whilehoney1:2(%,v/v),and ginger+honey 15.63 mg/mL[13].Our study was consistent with these reports demonstrating that ginger+honey(8 mg/mL)was astrongremineralizingagent.Theobtainedhigh remineralization is probably due to antimicrobial properties of ginger which might be the result of high amount of fluoride content(79 mg/kg fluoride in 8 mg).By addition of honey,thecontentoffluoridehasdecreasedto23.7mg/kg. Additionally,pH of ginger and honey content was quite high with 6.35(Therametric Technologies,Inc.,Indiana,USA). EventhoughNaFtoothpastehadmuchmorefluoride(1450 mg/kg),it has provided less remineralization than ginger and honey mixture.These results were consistent with the in situ study done by Bilgin et al.[25].
Tsai et al.showed that rosemary had some inhibitory effect on Streptococcus sobrinus(S.sobrinus)[26].They found the inhibitoryconcentrationsasminimumofaqueousand methanolic rosemary extracts on S.sobrinus were 4 and 16. Dalirsani et al.compared rosemary methanolic extract(30 g/ 100 mL)with chlorhexidine and found that rosemary has inhibitory effects on S.mutans[27].Being consistent with these studies,we found that rosemary was effective on remineralization process of enamel with high remineralization on fluorescence and microhardness assessments.Although there is no significant difference between rosemary and NaF toothpaste,Ipana,they had the same effective results(P>0.05).
S.mutans produce glucosyltransferases and synthesize the water-insoluble glucan causing the organisms firmly adhere to the tooth surface.Cacao beans are main ingredient of chocolate containing some anti-glucosyltransferase activity.Ooshima et al. reported that cacao bean husk has anticarcinogenic effect on S.mutans and S.sobrinus in rats,reporting that the extract may be an anticaries substance as a mild chemoprophylactic agent[28].They found the husk extract might be able to change a cariogenic into non-cariogenic flora without destroying the ecological balance inside the oral cavity,as it markedly reduces the growth rate of S.mutans,but does not strongly affect the other oral streptococci[28].Osawa et al.demonstrated that 50% ethanol extract of cacao bean husk was much better than 30% ethanol extract.They found cacao bean husk has higher molecular weight polyphenolic compounds and unsaturated free fatty acids for cariostatic actions.The former studies showed anti-glucosyltransferase and the latter antibacterial activity against S.mutans[29].Percival et al.observed that cacao polyphenols can inhibit biofilm formation and acid production by S.mutans[30].In our study,the chocolate we used was a carrier for the ginger and honey mixture,not used as a treatment material.Since it was sold in a public market with inexpensive price,probably it was not a pure cacao extract;contrary there might have sugar added into.Therefore,the results we obtained in ginger+honey+chocolate group were not consistent with the other studies;the demineralization was probably due to chocolate content.However,the cause of the inconsistencybetweenfluorescencemethods(QLFand FluoreCam)withmicrohardnesscouldbeduetothe remineralization on the surface of the lesion,but under this remineralized surface there was still demineralized area left. Thus,we might detect demineralization with microhardness assessment.
The applications of ginger,honey and rosemary as herbal medicaments demonstrated inhibitory effect on demineralization,and have enhanced remineralization on enamel under the conditions of this in vitro study.Quantitative assessment using FluoreCam was useful for detecting mineral density changes occurring in enamel demineralization.
Conflict of interest statement
We declare that we have no conflict of interest.
[1]Mount GJ.A new paradigm for operative dentistry.J Conserv Dent 2008;11:3-10.
[2]Palombo EA.Traditional medicinal plant extracts and natural products with activity against oral bacteria:potential application in the prevention and treatment of oral diseases.Evid Based Complement Alternat Med 2011;2011:680354.
[3]Bernardes WA,Lucarini R,Tozatti MG,Souza MG,Silva ML,Filho AA,et al.Antimicrobial activity of Rosmarinus officinalis against oral pathogens:relevance of carnosic acid and carnosol. Chem Biodivers 2010;7:1835-40.
[4]Ohara A,Saito F,Matsuhisa T.Screening of antibacterial activities of edible plants against Streptococcus mutans.Food Sci Technol Res 2008;14:190-3.
[5]Park M,Bae J,Lee DS.Antibacterial activity of[10]-gingerol and[12]-gingerol isolated from ginger rhizome against periodontal bacteria.Phytother Res 2008;22:1446-9.
[6]Smullen J,Finney M,Storey DM,Foster HA.Prevention of artificial dental plaque formation in vitro by plant extracts.J Appl Microbiol 2012;113:964-73.
[7]Kubra IR,Jaganmohanrao L.An overview on inventions related to ginger processing and products for food and pharmaceutical applications.Recent Pat Food Nutr Agric 2012;4(1):31-49.
[8]Israili ZH.Antimicrobial properties of honey.Am J Ther 2014;21(4):304-23.
[9]Bansal V,Medhi B,Pandhi P.Honey-a remedy rediscovered and its therapeutic utility.Kathmandu Univ Med J(KUMJ)2005;3: 305-9.
[10]Stephen-Haynes J.Evaluation of a honey-impregnated tulle dressing in primary care.Br J Community Nurs 2004;Suppl:S21-7.
[11]Ghabanchi J,Bazargani A,Daghigh Afkar M,Balady Foroshan S,Dad Ayeen S.In vitro assessment of anti-Streptococcus mutans potential of honey.Iran Red Crescent Med J 2010;12:61-4.
[12]Nassar HM,Li M,Gregory RL.Effect of honey on Streptococcus mutans growth and biofilm formation.Appl Environ Microbiol 2012;78:536-40.
[13]Patel RV,Thaker VT,Patel VK.Antimicrobial activity of ginger and honey on isolates of extracted carious teeth during orthodontic treatment.Asian Pac J Trop Biomed 2011;1:S58-61.
[14]Franco R,Onatibia-Astibia A,Martinez-Pinilla E.Health benefits of methylxanthines in cacao and chocolate.Nutrients 2013;5: 4159-73.
[15]Martinez-Pinilla E,Oñatibia-Astibia A,Franco R.The relevance of theobromine for the beneficial effects of cocoa consumption.Front Pharmacol 2015;6:30.
[16]Kargul B,¨Ozcan M,Peker S,Nakamoto T,Simmons WB,Faster AU.Evaluation of human enamel surfaces treated with theobromine:a pilot study.Oral Health Prev Dent 2012;10:275-82.
[17]White DJ.Use of synthetic polymer gels for artificial carious lesion preparation.Caries Res 1987;21:228-42.
[18]Dunipace AJ,Zhang W,Beiswanger AJ,Stookey GK.An in vitro model for studying the efficacy of fluoride dentifrices in preventing root caries.Caries Res 1994;28:315-21.
[19]Amaechi BT,Higham SM.In vitro remineralisation of eroded enamel lesions by saliva.J Dent 2001;29:371-6.
[20]Buhner SH.Herbal antibiotics,natural alternatives for treating drug-resistant bacteria.2nd ed.North Adams:Storey Publishing;2012.
[21]Argenta RM,Tabchoury CP,Cury JA.A modified pH-cycling model to evaluate fluoride effect on enamel demineralization. Pesqui Odontol Bras 2003;17:241-6.
[22]Iijima Y.Early detection of white spot lesions with digital camera and remineralization therapy.Aust Dent J 2008;53:274-80.
[23]Pretty IA,Edgar WM,Higham SM.The effect of dehydration on quantitative light-induced fluorescence analysis of early enamel demineralization.J Oral Rehabil 2004;31:179-84.
[24]Ando M,Eckert GJ,Stookey GK,Zero DT.Effect of imaging geometry on evaluating natural white-spot lesions using quantitative light-induced fluorescence.Caries Res 2004;38:39-44.
[25]Bilgin G,Yanıkoˆglu F,Tagtekin D.Remineralization potential of herbal mixtures:an in situ study.Paripex Indian J Res 2016;5: 264-8.
[26]Tsai PJ,Tsai TH,Ho SC.In vitro inhibitory effects of rosemary extracts on growth and glucosyltransferase activity of Streptococcus sobrinus.Food Chem 2007;105:311-6.
[27]Dalirsani Z,Aghazadeh M,Adibpour M,Amirchaghm M,Pakfetrat A,Mozaffari PM,et al.In vitro comparison of the antimicrobial activity of ten herbal extracts against Streptococcus mutans with chlorhexidine.J Appl Sci 2011;11:878-82.
[28]OoshimaT,OsakaY,SasakiH,OsawaK,YasudaH,Matsumura M,et al.Caries inhibitory activity of cacao bean husk extract in in-vitro and animal experiments.Arch Oral Biol 2000;45:639-45.
[29]Osawa K,Miyazaki K,Shimura S,Okuda J,Matsumoto M,Ooshima T.Identification of cariostatic substances in the cacao bean husk:their anti-glucosyltransferase and antibacterial activities.J Dent Res 2001;80:2000-4.
[30]Percival RS,Devine DA,Duggal MS,Chartron S,Marsh PD.The effect of cocoa polyphenols on the growth,metabolism,and biofilm formation by Streptococcus mutans and Streptococcus sanguinis.Eur J Oral Sci 2006;114:343-8.
2 Feb 2016
Prof.Dr.Dilek Tagtekin,Department of Restorative Dentistry,Marmara University,Istanbul,Turkey.
Tel:+90 5423124294
E-mail:dtagtekin@marmara.edu.tr
Peer review under responsibility of Hainan Medical University.The journal implements double-blind peer review practiced by specially invited international editorial board members.
2221-1691/Copyright©2016 Hainan Medical University.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
 Asian Pacific Journal of Tropical Biomedicine2016年10期
Asian Pacific Journal of Tropical Biomedicine2016年10期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- A review on promising phytochemical,nutritional and glycemic control studies on Moringa oleifera Lam.in tropical and sub-tropical regions
- A rare cause of acute abdomen-Spontaneous rectus sheath hematoma
- Evaluation of proline,chlorophyll,soluble sugar content and uptake of nutrients in the German chamomile(Matricaria chamomilla L.)under drought stress and organic fertilizer treatments
- ProductionofsecondarymetaboliteE2.2fromPhaleriamacrocarpaendophyticfungus
- Cytotoxic,genotoxic and apoptotic effects of naringenin-oxime relative to naringenin on normal and cancer cell lines
- Pandanusamaryllifoliusleafextractincreasesinsulinsensitivityinhigh-fatdiet-induced obese mice