
Risk of Treatment Failure in Patients with Drug-susceptible Pulmonary Tuberculosis in China*
2016-10-19 06:33:56WANGNiMAYanLIUYUHongDUJianZHANGHuiXIEShiHengZhuKunLYUXiaoYaSHUWeiWANGHongHongZHUGuoFengTANShouYongFUYanYongMALiPingZHANGLianYingLIUFeiYing0HUDaiYuZHANGYanLing2LIXiangQunandLILiang
WANG Ni, MA Yan, LIU YU Hong, DU Jian, ZHANG Hui, XIE Shi Heng,Zhu Kun, LYU Xiao Ya, SHU Wei, WANG Hong Hong, ZHU Guo Feng,TAN Shou Yong, FU Yan Yong, MA Li Ping, ZHANG Lian Ying, LIU Fei Ying0,HU Dai Yu, ZHANG Yan Ling2, LI Xiang Qun, and LI Liang,#
Policy Forum
Risk of Treatment Failure in Patients with Drug-susceptible Pulmonary Tuberculosis in China*
WANG Ni1,^, MA Yan2,3,4,^, LIU YU Hong2,3,4,^, DU Jian2,3,4, ZHANG Hui1, XIE Shi Heng2,3,4,Zhu Kun2,3,4, LYU Xiao Ya2,3,4, SHU Wei2,3,4, WANG Hong Hong2,3,4, ZHU Guo Feng5,TAN Shou Yong6, FU Yan Yong7, MA Li Ping8, ZHANG Lian Ying9, LIU Fei Ying10,HU Dai Yu11, ZHANG Yan Ling12, LI Xiang Qun5, and LI Liang2,3,4,#
The objective of this prospective study of the risks of treatment failure in patients with drug-susceptible pulmonary tuberculosis (PTB) was to provide reference data to help develop a disease control strategy. Participants were recruited in eight provinces of China from October 2008 to December 2010. A total of 1447 patients with drug-susceptible PTB and older than 15 years of age were enrolled. Demographic characteristics, bacteriological test results, and patient outcome, i.e., cure or treatment failure were recorded and compared using the chi-square or Fisher's exact tests. Multivariate logistic regression was used to identify factors associated with risk of treatment failure. Of the 1447 patients who were enrolled, 1349 patients(93.2%) were successfully treated and 98 (6.8%)failed treatment. Failure was significantly associated with age ≥65 years [odds ratio(OR)=2.522, 95% confidence interval (CI):(1.097-5.801)], retreatment [OR=2.365, 95% CI:(1.276-4.381)], missed medicine [OR=1.836, 95% CI:(1.020-3.306)], treatment not observed [OR=1.879 95% CI: (1.105-3.195)], and positive culture result after the first [OR=1.971, 95% CI: (1.080-3.597)] and second month [OR=4.659, 95% CI: (2.590-8.382)]. The risk factors associated with treatment failure were age ≥65 years, retreatment, missed
medication, treatment not observed, and positive culture at the end of month 1 or month 2. These risk factors should be monitored during treatment and interventions carried out to reduce or prevent treatment failure and optimize treatment success. Tuberculosis (TB) continues to be a significant public health problem in the world. According to the World Health Organization, China was third among 22 high-TB burden countries, with an estimated 930,000 pulmonary tuberculosis (PTB) patients in 2015[1]. The global TB control target is to end the TB epidemic by 2035, which represents a 95% reduction in TB deaths, and a 90% reduction in incidence rate compared with 2015. The basic strategy to detect and cure all PTB patients and end the TB epidemic is patient centered. Patients with tuberculosis require retreatment if they are not cured in order to avoid being a source of infection or developing drug-resistant TB, which is a serious public health challenge that makes TB control more difficult[2]. We designed this prospective study to identify the factors associated with risk of treatment failure and to provide evidence to help develop TB control strategies.
Study Setting and Population The study was conducted from October 2008 to December 2010 in eight provinces, Tianjin, Hebei, Henan, Shanghai,Chongqing, Yunnan, Guangxi, and Guangdong,situated in eastern, central, and western China. The study was integrated w ith the routine procedures of the national TB control program of each province,including sputum smears, chemotherapy, and treatment management. Sputum culture and drug susceptibility testing (DST) were added during the conduct of the study.
All study participants satisfied the follow ing inclusion criteria: 1) ≥15 years of age; 2) provided informed consent; 3) PTB culture-positive at initial treatment and retreatment; 4) free of nontuberculous mycobacterium infection; and 5)infected with a strains susceptible to all four first-line anti-TB drugs (isoniazid, rifampicin, streptomycin,and ethambutol). A total of 1447 participants receiving initial treatment or retreatment of drug-susceptible PTB were enrolled. Treatment was successful in 93.2% (1349/1447) of the participants and failed in 6.8% (98/1447). Sputum smears, sputum cultures, and DST were performed during months 1,2, and 5 of anti-TB treatment.
Study Definitions The definitions used in this study were those recommended in the guidelines for implementing tuberculosis control programs in China[3]. Initial treatment is that given to 1) a patient who has never been treated for TB, or 2) a patient who has taken anti-TB drugs for less than 1 month. Retreatment is that given to 1) a patient who has taken anti-TB drugs for 1 month or more, or 2) a patient who failed initial treatment or has relapsed. Cured patients are those who completed prescriptive treatment and had two negative sputum smears during treatment and at least one after completing treatment. Patients who complete treatment are sputum smear-positive at the beginning,smear-negative at the end of the intensive-treatment phase, have not more than one positive smear during the continuing phase of treatment, and remain sputum smear-negative in the last month of treatment. Successful treatment describes cured patients and those who completed treatment;Treatment failure describes smear-positive patient who is still positive at 5 months or smear-negative patients who become smear-positive during treatment.
Treatment Regimens Anti-TB treatment followed the guidelines of the tuberculosis control program in China[3]. The initial treatment and retreatment regimens were standard short-course chemotherapy protocols. Initial PTB patients received 2 months of isoniazid (H), rifampin (R), and pyrazinamide (Z) plus 4 months of H and R(2H3R3Z3E3/4H3R3). Retreatment PTB patients received streptomycin (S), H, R, Z, and E during the intensive phase plus 6 months of H, R, and E (2H3R3Z3S3E3/6H3R3E3).
Ethical Statement This study was approved by the Institutional Ethics Review Committee of Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis and Thoracic Tumor Research Institute,and the eight provincial TB Control and Prevention Centers (TB hospitals).
Statistical Analysis The participant characteristics were analyzed descriptively. Chi-square or Fisher's exact tests were used to compare demographic characteristics, bacteriological test results, and management outcomes in the treatment success and treatment failure groups. Variables found to be significant in univariate analysis were subsequently analyzed by multivariate logistic regression with odds ratios (ORs) and their 95% confidence intervals (CIs)to identify the factors that remained statistically significant in the final model. Data analysis was performed using SAS version 9.1 (SAS institute Inc.,Cory, NC, USA), and P-values <0.05 were considered as statistically significant.
Demographic Characteristics of Study Participants Of 2142 confirmed smear-positive PTB patients evaluated during the study period, 67 were infected with nontuberallous mycobacteria (NTM), 54 were sputum-culture negative, 383 had drug-resistant TB,36 died, 39 were default cases, 44 transferred out,and 72 others refused treatment. The remaining 1447 participants with drug-susceptible TB included 1349 treatment success cases and 98 treatment failure cases. DST confirmed that all cases were treatable with the four first-line anti-TB drugs; all 1447 were enrolled and received standard anti-TB treatment. Table 1 includes the demographic characteristics of the 1447 study participants.
Risk Factors Associated with Treatment Failure The treatment failure rate was 6.77% (98/1447). The chi-square and Fisher's exact tests found significant differences (P<0.5) in sex, age, profession,educational attainment, treatment type, missed medication, directly observed treatment (DOT) for patients, and sputum culture at the end of months 1stand 2ndin the treatment success and treatment failure groups (Table 2). Treatment failure was more frequent in men (7.80%) than in women (4.17%). By age, the failure rate was highest in those ≥65 years of age (11.70%). By profession, the rate was highest in‘employees' (9.52%); and by educational attainment,was highest in those who completed primary school(9.57%).Treatment failure occurred more often with retreatment(12.64%)than in initial treatment(5.97%),in participants missing medicine(12.00%),and in those who were culture-positive at the end of month 1st(13.08%)or month 2nd(16.34%)compared with culture-negative at the end of month 1(3.28%)or month 2(4.37%).
Multivariate logistic regression analysis found that six variables included in the univariate analysis remained independently associated with treatment failure.These were≥65 years of age(OR,2.522;95%CI:1.097-5.801),retreatment(OR,2.365;95%CI:1.276-4.381),missed medicine(OR,1.836;CI:1.020-3.306),treatment not observed(OR,1.879;95%CI:1.105-3.195),and positive culture at the end of month 1(OR,1.971;95%CI:1.080-3.597),or month 2(OR,4.659;95%CI:2.590-8.382).
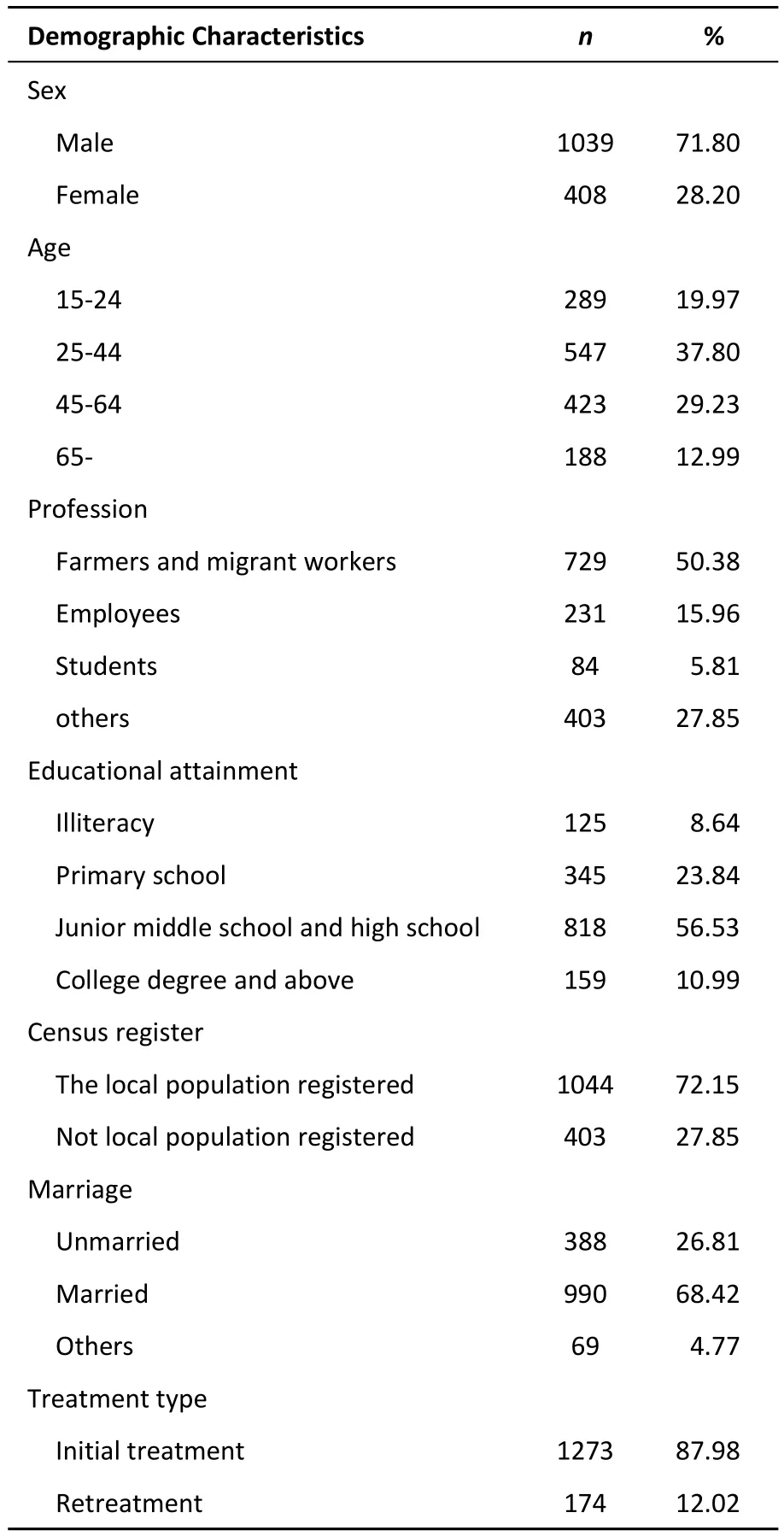
Table 1.Demographic Characteristics of the 1447 Study Participants
Previous studies have reported TB treatment failure rates ranging from 0.2%to 18.6%[4-11].In this study of drug-susceptible PTB patients in China,the treatment failure rate was 6.8%(98/1447).Failed patients easily develop drug-resistant or chronic TB,and thus become an important infection source that makes TB control even more difficult.Therefore,it is very important to recognize and act on factors that increase the risk of treatment failure.
We found that the risk of treatment failure was 2.522 times greater in patients≥65 years of age than in those younger than 25 years of age,which is consistent with other reports[12-16].The increased risk may result from age-related factors such as long onset time,atypical symptoms,a weakened immune system,complications of disease,or poor adherence to treatment.Specific interventions should be directed at the elderly to promote early detection,diagnosis,and treatment.Overall supervision and management should stress,individualized treatment when necessary and as indicated by specific patient conditions in order to improve the cure rate and reduce the failure rate.
The result of sputum bacteria testing at the end of 2ndmonth was an important index of the effectiveness of intensive phase treatment[17].Recent studies[18-23]reported thatnon-conversion of sputum bacteria test results predicted treatment failure and relapse.In our study,nonconversion of sputum culture at the end of 1stmonth increased the risk of treatment failure by 1.971 times com pared with conversion.The risk of failure was increased 4.659 times in patients who had not become sputum-culture negative at the end of 2ndmonth. The significance of nonconversion of sputum culture results at the end of 2ndmonth is in line w ith recent studies[24-30].Monitoring of sputum bacteria is thus a key element in the process of TB treatment,especially during the first two months.Regular sputum testing should be carried out every month,and DST should be performed if the results of bacteriological evaluation remain positive.The treatment regimen can be adjusted depending on the DST results.
Poor adherence to anti-TB regimens is known to result in treatment failure[31-32].If patients feel better at a time when their treatment is not being observed,they may decide to discontinue their medication,which predicts im pending treatment failure.Our study revealed that missed medicine and lack of treatment observation were independently associated with risk of failure.We should adopt appropriate measures to improve treatment adherence and thus avoid increased disease severity. There is evidence that counseling and regular communication between patients and health-care stuff is effective in improving patient adherence to treatment[33-34].We should improve the health education of patients and their family members to raise awareness of the dangers of irregular medication.Implementing strict observation of drug taking,and intensified medicine management with enhanced tracking to prevent missed and intermittent medication doses would further improve adherence,ensure a full treatment course,and thus reduce failure rates.
Retreatment significantly affects treatment outcome,and need for PTB retreatment has been related to not using standard regimens for initial treatment[35-38],resulting in increased incidence of drug-resistance[39].However,there is still hope to cure PTB by treatment using standard,first-line drugs. In this study we found that risk of treatment failure was2.365 times greater in retreatment patients than in those receiving initial treatment.Retreatment has also been associated with development drug-resistant TB[13-14,40-41].Thus,improved success of initial treatment is very important,and the choice of standard first-line drugs or second-line drugs for retreatment of patients can be individualized by DST.
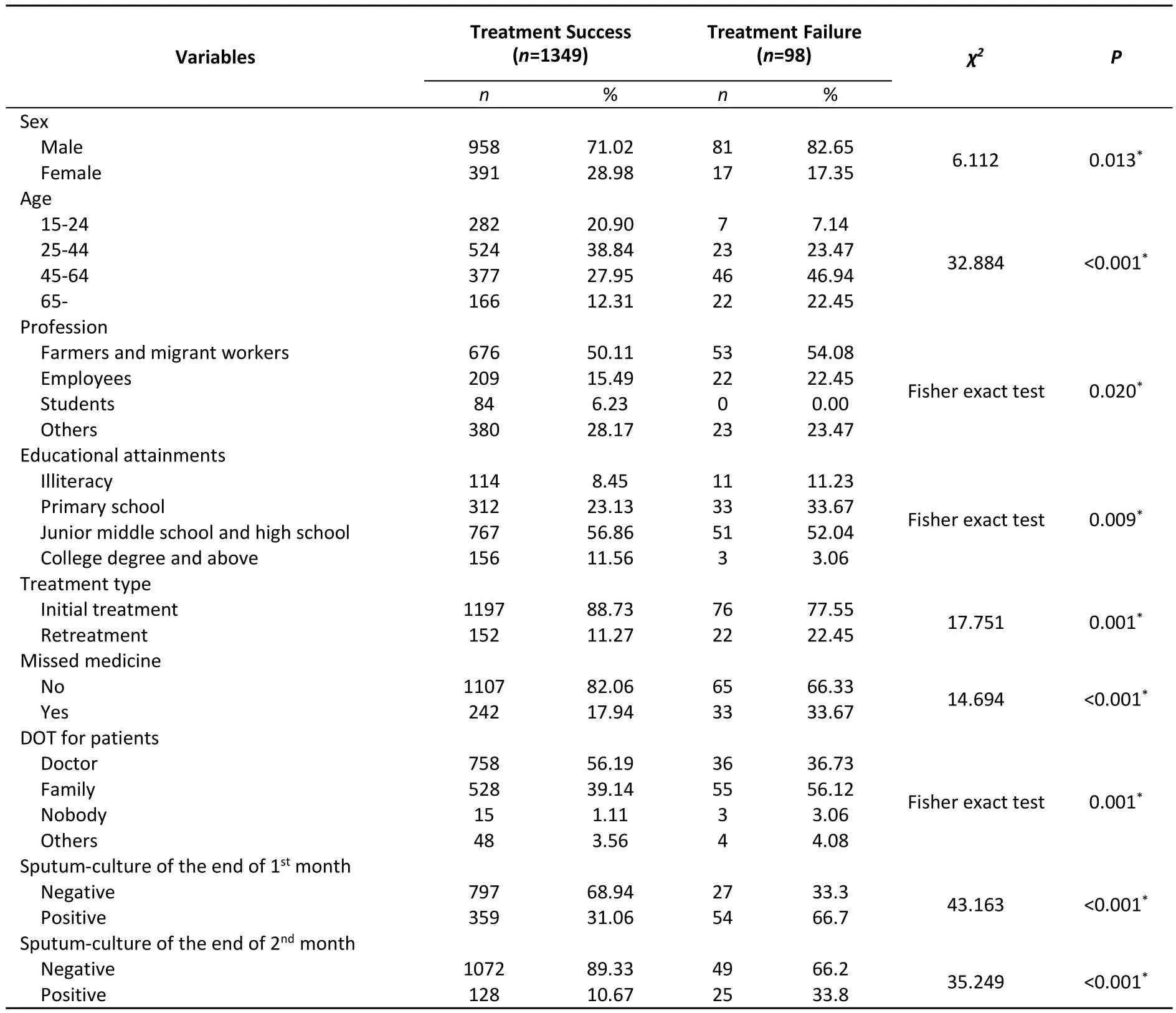
Table 2.Univariate Analysis of Risk Factors Associated with Treatment Failure

Table 3. Multivariate Analysis of Risk Factors Associated with Treatment Failure
In conclusion, the treatment failure rate (6.8%)of drug-susceptible PTB in this study was relatively high. By identifying factors that increased the risk of treatment failure, our findings provide evidence to help develop public health policy designed to improve treatment effectiveness. First, monitoring of sputum testing during intensive phase treatment should be strengthened and DST of positive results should be routinely used to adjust treatment regimens. Second, all PTB patients who need retreatment should be evaluated by DST to guide choice of the treatment regimen. Third, patient treatment and management needs improvement to reduce the occurrence of missed doses of medicine. New management tools such as electronic medication monitors might be used to improve patient adherence and reduce reliance on direct observation. Comprehensive TB control strategies are needed for effective reduction or prevention of treatment failure.
Study Limitations This study has several limitations. First, because it was based on data collected in questionnaires it may be subject to recall bias. Second, some factors that may influence treatment failure, including comorbidities such as chronic obstructive pulmonary disease, chronic hepatitis, and HIV were not considered in our study,and thus could not be assessed.
Acknowledgements We would like to express our deep thanks to the participants for their cooperation in this study.
^These authors contributed equally to this study and share first authorship.
#Correspondence should be addressed to LI Liang, Fax:86-10-80885205, Tel: 86-10-89509216, E-mail: liliang@ tb123.org
Biographical notes of the first authors: WANG Ni, male,born in 1981, master of public health, majoring in tuberculosis control and prevention; MA Yan, female, born in 1980, master of public health, majoring in tuberculosis control and prevention; LIU Yu Hong, female, born in 1969,bachelor, majoring in tuberculosis control and prevention.
REFERENCES
1. World Health Organization. G Global Tuberculosis Report 2015,WHO, Geneva, Switzerland, 2015.
2. Chen KS, Liu T, Lin RR, et al. Tuberculosis transmission and risk factors in a Chinese antimony mining community. Int J Tuberc Lung Dis, 2016; 20, 57-62.
3. Department of Disease Control, Ministry of Health,Department of Medical Administration, Ministry of Health,Chinese Center for Disease Control and Prevention. Guidline of implementing tuberculosis control programme China. Beijing:Pecking Union Medical College Press, 2008, 89.
4. Endris M, Moges F, Belyhun Y, et al. Treatment outcome of tuberculosis patients at enfraz health center, northwest ethiopia: a five-year retrospective study. Tuberc Res Treat, 2014;2014, 726193.
5. Kurbatova EV, Taylor A, Gamm ino VM, et al. Predictors of poor outcomes among patients treated for multidrug-resistant tuberculosis at DOTS-plus projects. Tuberculosis (Edinb), 2012;92, 397-403.
6. Johnston JC, Shahidi NC, Sadatsafavi M, et al. Treatment outcomes of multidrug-resistant tuberculosis: a systematic review and meta-analysis. PLoS One, 2009; 4, e6914.
7. Orenstein EW, Basu S, Shah NS, et al. Treatment outcomes among patients with multidrug-resistant tuberculosis:systematic review and meta-analysis. Lancet Infect Dis, 2009; 9,153e61.
8. Tessema B, Muche A, Bekele A, et al. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital,Northwest Ethiopia: A five-year retrospective study. BMC Public Health, 2009; 9, 371.
9. Ramos JM, Reyes F, Tesfamariam A. Childhood and adult tuberculosis in a rural hospital in Southeast Ethiopia: a ten-year retrospective study. BMC Public Health, 2010; 10, 215.
10.Shargie EB1, Lindtjørn B. DOTS improves treatment outcomes and service coverage for tuberculosis in South Ethiopia:a retrospective trend analysis. BMC Public Health, 2005; 5, 62.
11.Berhe G1, Enquselassie F, Aseffa A. Treatment outcome ofsmear-positive pulmonary tuberculosis patients in Tigray Region, Northern Ethiopia. BMC Public Health, 2012; 12, 537.
12.Ananthakrishnan R, Kumar K, Ganesh M, et al. The profile and treatment outcomes of the older (aged 60 years and above)tuberculosis patients in Tamilnadu, South India. PLoS One,2013; 8, e67288.
13.Choi H, Lee M, Chen RY, et al. Predictors of pulmonary tuberculosis treatment outcomes in South Korea: a prospective cohort study, 2005-2012. BMC Infect Dis, 2014; 14, 360.
14.Vasankari T, Holmström P, Ollgren J, et al. Risk factors for poor tuberculosis treatment outcome in Finland: a cohort study. BMC Public Health, 2007; 14, 291.
15.Noubom M, Nembot FD, Donfack H, et al. Characteristics of TB patients in west Cameroon: 2000-2009. Pan Afr Med J, 2013;16, 39.
16.Lee J, Lee BJ, Yoon HI, et al. Influence of previous tuberculosis treatment history on acid-fast bacilli smear and culture conversion. Int J Tuberc Lung Dis, 2012; 16, 1344-8.
17.WHO/Stop TB Partnership. Compendium of Indicators for Monitoring and Evaluating National Tuberculosis Programs. Geneva: World Health Organisation; 2004;WHO/HTM/TB/2004.344.
18.Gopi PG, Chandrasekaran V, Subramani R, et al. Association of conversion & cure with initial smear grading among new smear positive pulmonary tuberculosis patients treated with category I regimen. Indian J Med Res, 2006; 123, 807-14.
19.Babali A, Kiziltas S, Arda H, et al. Factors affecting smear conversion in tuberculosis management. Med Sci, 2012; 1,351-62.
20.BanuRekha VV, Balasubramanian R, Swam inathan S, et al. Sputum conversion at the end of intensive phase of category-1 regimen in the treatment of pulmonary tuberculosis patients w ith diabetes mellitus or HIV infection: an analysis of risk factors. Indian J Med Res, 2007; 126, 452-8.
21.Guler M, Unsal E, Dursun B, et al. Factors influencing sputum smear and culture conversion time among patients with new case pulmonary tuberculosis. Int J Clin Pract, 2007; 61, 231-5.
22.Wang JY, Lee L, Yu CJ, et al. Factors influencing time to smear conversion in patients with smear-positive pulmonary tuberculosis. Respirology, 2009; 14, 1012-9.
23.Singla R, Bharty SK, Gupta UA, et al. Sputum smear positivity at two months in previously untreated pulmonary tuberculosis patients. Int J Mycobacteriol, 2013; 2, 199-205.
24.Unsematham S, Kateruttanakul P. Factors predicting sputum smear conversion and treatment outcomes in new smear-positive pulmonary tuberculosis. J Med Assoc Thai, 2013;96, 644-9.
25.Djouma FN, Noubom M, Ateudjieu J, et al. Delay in sputum smear conversion and outcomes of smear-positive tuberculosis patients: a retrospective cohort study in Bafoussam, Cameroon. BMC Infect Dis, 2015; 21, 139.
26.Zhao FZ, Levy MH, Wen S. Sputum m icroscopy results at two and three months predict outcome of tuberculosis treatment. Int J Tuberc Lung Dis, 1997; 1, 570-2.
27.Rieder HL. Sputum smear conversion during directly observed treatment for tuberculosis. Tuber Lung Dis, 1996; 77, 124-9.
28.Lienhardt C, Manneh K, Bouchier V, et al. Factors determ ining the outcome of treatment of adult smear-positive tuberculosis cases in the Gambia. Int J Tuberc Lung Dis, 1998; 2, 712-8.
29.R Singla, D Srinath, S Gupta, et al. Risk factors for new pulmonary tuberculosis patients failing treatment under the Revised National Tuberculosis Control Programme, India. INT J Tuberc Lung Dis, 2009; 13, 521-6.
30.Amante TD, Ahemed TA. Risk factors for unsuccessful tuberculosis treatment outcome (failure, default and death) in public health institutions, Eastern Ethiopia. Pan Afr Med J,2015; 20, 247.
31.Charles P. Felton National Tuberculosis Center. Adherence to Treatment for Latent Tuberculosis Infection. A Manual for Health Care Providers. 2005.
32.Franke F, Appleton C, Arteaga F, et al. Risk factors and mortality associated with defaultfrom multidrug-resistant tuberculosis treatment. Clin Infect Dis, 2008; 46, 1844-51.
33.Bello I, Itiol A. Drug adherence amongst tuberculosis patients in the University of Ilorin Teaching Hospital, Ilorin, Nigeria. Afri J Phar Pharmacol, 2010; 4, 109-14.
34.Simon L, Judy D, Merrick Z, et al. Staff training and ambulatory treatment outcomes: a cluster randomized controlled trial in South Africa. Bull WHO, 2005; 83, 250-9.
35.Azhar GS. DOTS for TB relapse in India: A systematic review. Lung India, 2012; 29, 147-53.
36.Anaam MS, Ibrahim M I, Al Serouri AW, et al. A nested case-control study on relapse predictors among tuberculosis patients treated in Yemen's NTCP. Public Health Action, 2012; 2,168-73.
37.Lee H, Kim J. A study on the relapse rate of tuberculosis and related factors in Korea using nationw ide tuberculosis notification data. Osong Public Health Res Perspect, 2014;5(Suppl), S8-S1 .
38.Das R, Baidya S, Das JC, et al. A study of adherence to DOTS regimen among pulmonary tuberculosis patients in West Tripura District. Indian J Tuberc, 2015; 62, 74-9.
39.Sawadogo B, Tint KS, Tshimanga M. Risk factors for tuberculosis treatment failure among in four health regions of Burkina Faso, 2009: case control study. Pan Afr Med J, 2015; 21,152.
40.Zhao Y, Xu S, Wang L, et al. National survey of drug-resistant tuberculosis in China. Nngl J Med, 2012; 366, 2161-70.
41.Kuksa L, Riekstina V, Leimane V, et al. Multi- and extensively drug-resistant tuberculosis in Latvia: trends, characteristics and treatment outcomes. Public Health Action, 2014; 4(Suppl 2):S47-53.
10.3967/bes2016.083
March 26, 2016;Accepted: August 1, 2016
*This study was supported by the National Science and Technology Major Project of China(2008ZX10003-008-02).
1. National Center for Tuberculosis Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 102206, China; 2. Center office, Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing 101149, China; 3. Beijing Chest Hospital, Capital Medical University, Beijing 101149, China; 4. Clinical Center on Tuberculosis, China CDC, Beijing 101149, China; 5. Shanghai Municipal Center for Disease Control and Prevention, Shanghai 200336, China; 6. Guangzhou Chest Hospital, Guangzhou 510095, Guangdong, China; 7. Tianjin Centers for Disease Control and Prevention, Tianjin 300041, China; 8. Department of TB Control, Henan Center for Disease Control and Prevention, Zhengzhou 450016, Henan,China; 9. Hebei Center for Disease Control and Prevention, Shijiazhuang 050021, Hebei, China; 10. Department of TB Control, Guangxi Center for Disease Control and Prevention, Nanning 530021, Guangxi, China; 11. Chongqing Anti-tuberculosis Institute, Chongqing 400050, China; 12. Department of TB Control, Yunnan Center for Disease Control and Prevention, Kunming 650022, Yunnan, China
 Biomedical and Environmental Sciences2016年8期
Biomedical and Environmental Sciences2016年8期
- Biomedical and Environmental Sciences的其它文章
- Viral Contamination Source in Clinical Microbiology Laboratory*
- Evaluation o f Xpert MTB/RIF for the Diagnosis of Extrapulmonary Tuberculosis in China*
- Effect of Smo SiRNA-mediated Hedgehog Signaling Pathway Inhibition on Palatal Fusion*
- 8-isop rostane as Oxidative Stress Marker in Coal Mine Wo rkers
- Bio logical Effec ts o f Clo th Con taining Specific Ore Pow der in Patien ts w ith Po llen Allergy
- Alcohol Drinking, Dyslipidemia, and Diabetes: A Population-based Prospective Cohort Study among lnner Mongolians in China*