
血尿酸水平与冠心病发病关系的剂量-反应Meta分析
2016-08-18 10:20芦永斌程治远赵亚学常晓宇程宁
中国循环杂志 2016年7期
芦永斌,程治远,赵亚学,常晓宇,程宁
冠心病研究
血尿酸水平与冠心病发病关系的剂量-反应Meta分析
芦永斌,程治远,赵亚学,常晓宇,程宁
目的:用Meta分析方法评价血尿酸水平与冠心病发病间的剂量-反应关系。
方法:通过数据库(PubMed, Elsevier和Web of Science)检索已经公开发表的国外关于血尿酸水平与冠心病发病的队列研究。利用Stata软件对其进行综合分析。
结果:纳入11项队列研究,463 918例研究对象。在男性和女性中,血尿酸水平增高均是冠心病发病的危险因素,其相对危险度(RR)及其95%可信区间(95%CI)分别为:1.11(1.00~1.24)和1.24(1.15~1.34)。剂量-反应Meta分析:随着血尿酸水平的增加,冠心病发病风险也在逐步增加;血尿酸水平每增加1mg/dl,在男性和女性中冠心病发病风险分别增加4.8%和12.4%,且女性明显高于男性。
结论:血尿酸水平与冠心病发病存在密切相关。
尿酸;冠状动脉疾病
Abstract
Objective: To evaluate the relationship between the levels of serum uric acid (SUA) and prevalence of coronary artery disease (CAD) by Meta analysis.
Methods: We searched the databases of Pub Med, Elsevier and Web of Science for internationally published cohort study for the relationship between SUA levels and CAD prevalence and conducted a general analysisby using Stata software.
Results: A total of 11 cohort study including 463,918 subjects were enrolled in this study. For both male and female genders, increase SUA level was the risk factor for CAD occurrence (RR=1.11, 95% CI 1.00-1.24) and (RR=1.24, 95% CI 1.15-1.34). Dose-response Meta-analysis indicated that by 1 mg/dl SUA elevation, the risk of CAD occurrence would increase 4.8% in male and 12.4% in female, the risk in female gender was higher than male.
Conclusion: SUA level has been closely related to CAD prevalence.
(Chinese Circulation Journal, 2016,31:640.)
随着人们生活水平提高,膳食结构也发生了改变。近年来,我国冠心病发病率迅速增长,已经严重危害国民健康[1]。自Gertler等[2]提出血尿酸与心血管疾病之间可能存在相互作用以来,国内外学者展开了大量相关方面研究。有研究表明,尿酸对冠心病发病起一定促进作用[3],但对于它们之间的剂量-反应关系,没进行相关评价。我们深入分析已经发表的血尿酸水平与冠心病发病关系的队列研究,通过评价血尿酸水平与冠心病发病之间的剂量-反应关系,以确定尿酸水平与冠心病发病的风险。
1 资料与方法
1.1 文献检索
主要检索的数据库有PubMed, Elsevier和Web of Science (1950-01至2015-04)。使用的主题词包括:[uric acid或 hyperuricemia]和 [coronary disease或myocardial infarction 或 coronary artery disease或angina pectoris或 unstable angina或 cardiovascular disease或coronary heart disease或acute coronary syndrome]。
1.2 纳入标准
文献纳入必须同时满足:(1)研究类型是队列研究;(2)至少可以提供血尿酸水平与冠心病发病的相对危险度(RR)及其95%可信区间(95%CI),或提供的原始数据可以进行上述指标计算。对重复发表的文献予以剔除,如果是相同队列不同时间点上的研究,则仅选取最新研究。
1.3 质量评价与数据提取
按照纽卡斯尔-渥太华量表对纳入文献进行质量评价。该量表主要从研究对象选择、组间可比性及结局测量3个方面评价纳入Meta分析文献质量,每方面3分,满分9分。该研究中,评分≥7分被定义为高质量文献。文献筛选和数据提取均有2位作者完成,结果相矛盾的地方由二人讨论后达成一致。具体要提取的数据资料如下:(1)研究作者、发表年份;(2)纳入研究的研究对象总人数;(3)血尿酸的不同剂量及界限值(一个研究至少包括三个剂量组,一般取原始暴露剂量区间的中位数);(4)结局事件及其发生的病例数(各暴露剂量组间的病例数)、总数(各暴露剂量区间的随访人年数)、效应量(各暴露区间相对于各对照组的相对危险度的对数值)和效应量的标准误(各暴露剂量区间效应量的标准误,若只提供RR值和95%CI也可)[4]。
1.4 统计学方法
该研究采用Stata 11及其glst命令完成,用Q值进行异质性检验,以I2值来评估纳入研究的异质性的大小;当I2<50%,采用固定效应模型,反之则采用随机效应模型,即将随机误差纳入考虑范围,必要时进行亚组分析和Meta回归来排除异质性来源。剂量-反应Meta分析是基于广义最小二乘法,即通过“glst”命令实现,采用“两步法”进行分析[4]。先建立回归模型并计算出每个研究对象各单位尿酸与冠心病发病风险的关系,再在随机效应模型下合并上一步计算出的每项研究的发病风险,应用Wald检验是否存在线性相关[5],当P>0.05时,呈线性相关,反之亦然,并拟合图形。采用Begg和Egger法对潜在的发表偏倚进行检验[6]。
2 结果
2.1 文献筛选结果
该研究收集的文献总量为1 294篇,全为英文文献。根据题目、摘要以及重复发表等原因剔除1 211篇文献后,对83篇研究进行进一步的评估,根据纳入标准及剔除标准,剔除不合格的文献72篇(研究类型不符31篇,研究结果不符36篇,无法提取结果4篇,低质量文献1篇)。最终有11篇,463918例研究对象纳入研究,男246 735例,女217 183例。11篇文献纳入研究的基本特征见表1。采用Begg和Egger法对潜在的发表偏倚进行检验,结果发表偏倚的可能性较小(P>0.05)。

表1 11篇纳入研究的文献资料基本特征
2.2 血尿酸水平与冠心病发病的关系
血尿酸水平与冠心病发病风险的关系[7-17](表2):在男性和女性中,血尿酸水平增高均是冠心病发病的危险因素,男性RR(95% CI):1.11 (1.00~1.24);女性RR(95% CI):1.24(1.15~1.34)。将男性血尿酸水平分为4组:≤4.7、4.8~5.7、5.8~6.7和≥6.8 mg/dl组,冠心病发病风险RR(95% CI)分别为:1.00(1.00)、0.94(0.81~1.06)、 1.00 (0.84~1.19)和1.10(0.90~1.36)。将女性血尿酸水平分为3组:≤4.7、4.8~5.7和≥5.8 mg/dl组,冠心病发病风险RR(95% CI)分别为:1.00(1.00)、1.37(1.06~1.77)和2.42(1.45~4.06),女性血尿酸水平与冠心病发病呈正相关。
2.3 血尿酸水平与冠心病发病的剂量-反应Meta分析
在男性中,4个研究[10,12,14,17]无明显异质性(I2=23.46%),用固定效应模型合理。显著性检验χ2=638.13,P<0.001,建立的固定效应非线性回归模型有意义。进一步进行统计学检验χ2=34.39,P<0.001,存在非线性剂量-反应关系(图1A)。RR(95%CI):1.0479 (1.0440~1.0519),即在最低血尿酸水平(0 mg/dl)的基础上,每增加1 mg/ dl,发生冠心病的危险增加4.8%。血尿酸水平为4、5、6、7和8 mg/dl时,冠心病发病风险RR(95%CI)分 别为:1.04(0.99~1.10)、1.11(1.05~1.16)、1.22 (1.16~1.28)、1.34(1.26~1.42)和1.41(1.34~1.49)。随着血尿酸水平的增加,冠心病发病风险也在逐步增加。
在 女 性 中,4个 研 究[9, 10, 15, 16]存 在 异 质性(I2=67.70%),用随机效应模型。显著性检验χ2=8.62,P<0.001,建立的随机效应非线性回归模型有意义。进一步进行统计学检验χ2=34.39,P<0.01,存在非线性剂量-反应关系(图1B)。RR (95%CI):1.1241(1.0396~1.2154),即在最低尿酸水平(0 mg/dl)的基础上,每增加1 mg/dl,发生冠心病的危险增加12.4%。血尿酸水平为4、5、6、7和8 mg/dl时,冠心病发病风险RR(95%CI)分别为:1.07 (0.92~1.25)、1.37(1.20~1.58)、1.71(1.46~1.99)、1.87(1.60~2.19)和1.95(1.68~2.26)。随着血尿酸水平的增加,冠心病发病风险也在逐步增加,且女性增加速度高于男性。
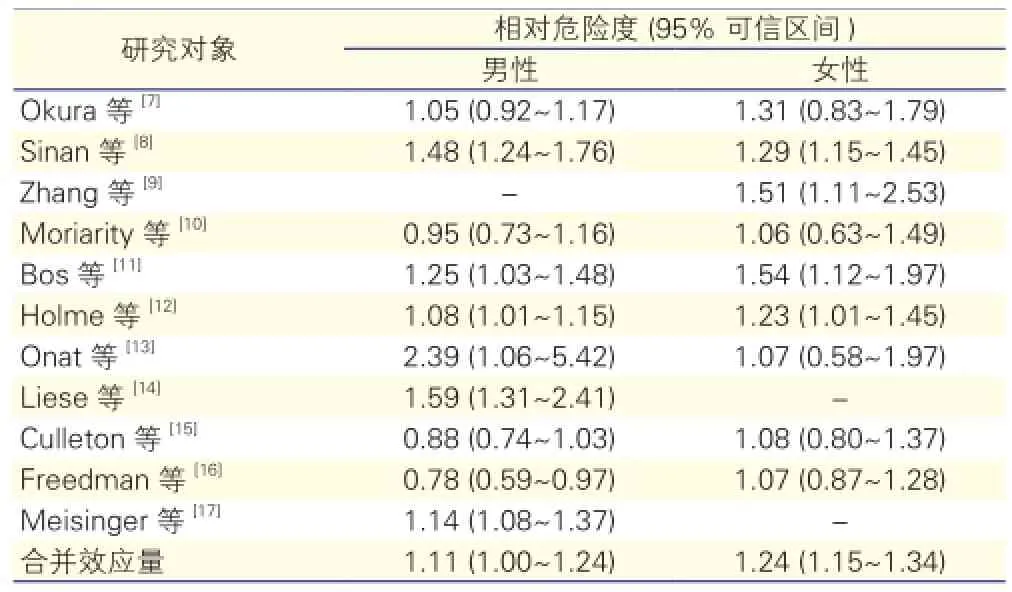
表2 血尿酸水平与冠心病发病风险的关系

图1 血尿酸水平与冠心病发病风险的剂量-反应关系
3 讨论
目前,有很多尿酸水平与冠心病研究,但不能很好的解释随着尿酸水平增加冠心病发病风险也在增加,更不能分析尿酸水平与冠心病发病风险间的剂量-反应关系。剂量-反应评价的本质就是回归分析,来定量评价效应量与暴露剂量的关系,因此我们深入分析已经发表的尿酸与冠心病的队列研究,通过评价血尿酸水平与冠心病发病风险间的剂量-反应关系,以确定血尿酸水平与冠心病发病风险。本文纳入的队列研究,信息完整可靠,可减少偏倚,因果论证科学性强。
Wheeler等[18]首次对尿酸与冠心病进行了荟萃分析,纳入16项病例对照研究,认为尿酸水平与冠心病发生没有相关性。Kim等[19]发现,尿酸增加了冠心病发病风险,是冠心病的独立危险因素,其RR(95%CI):1.09(1.03~1.16),但在其亚组分析中,只在女性中,血尿酸水平与冠心病发病有关。而本研究发现:在男性和女性中,血尿酸水平增高均是冠心病发病的危险因素,其RR(95%CI)分别为:1.11 (1.00~1.24)和1.24(1.15~1.34)。在剂量-反应Meta分析中发现:随着血尿酸水平的增加,冠心病发病风险也在逐步增加;血尿酸水平每增加1 mg/dl,在男性和女性中冠心病发病风险分别增加4.8%和12.4%,且女性明显高于男性。与Kim研究相比,本文纳入了最近几年新发表的文献[8,9,13],并应用Meta分析方法评价尿酸水平与冠心病发病风险的剂量-反应关系:随着尿酸水平的增加,冠心病发病风险也在逐步增加。一些研究得出尿酸与心血管事件的发生存在相关性[17,20],并且女性高于男性,这也与本研究结论一致。对于冠心病发病的风险,为什么女性高于男性?Holme等[21]发现原因有:(1)高尿酸血症在女性中较男性常见;(2)具有高尿酸血症的女性年龄通常大于男性;(3)高尿酸血症与高血压、糖尿病和C反应蛋白等心血管疾病因素有很强的关联,但女性中含量高于男性;(4)高尿酸血症对女性的肾损伤强于男性。遗憾的是在男性尿酸水平亚组分析中未能发现尿酸水平与冠心病发病存在相关性,原因可能是分层过导致各层间样本量流失,使得整体统计效能降低[21],其具体原因有待进一步研究。
本研究的优点:(1)纳入的研究为队列研究,尽可能的增强精度,减小异质性;(2)对血尿酸水平进行了明确的分组并进行了亚组分析;(3)运用不同的方法对剂量-反应关系进行了分析,结果更加可靠。
展望:(1)不同血尿酸水平存在异质性,应引起相关研究重视;(2)高尿酸血症的界限值尚存在争议,有待进一步研究。
[1] 杨伟宪, 杨铮, 窦克非, 等. 217例青年冠心病患者临床特点分析.中国循环杂志, 2014, 29: 339-342.
[2] Gertler MM, Garn SM, Levine SA. Serum uric acid in relation to age and physique in health and in coronary heart disease. Ann Intern Med,1951, 34: 1421-1431.
[3] 郭志平, 林金秀, 刘慧兰, 等. 原发性高血压患者血尿酸与冠心病关系的研究. 中国循环杂志, 2010, 25: 188-191.
[4] Luo ML, Lin XJ, Liu RC, et al. Dose-response relationship of Metaanalysis in the Stata software implementation. JEBM, 2014, 13: 182-187.
[5] Orsini N, Bellocco R, Greenland S. Generalized least squares for trend estimation of summarized dose-response data. Stata J, 2006, 6: 44-57.
[6] Sterne J, Egger M. Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J ClinEpidemiol, 2001, 54: 1046-1055.
[7] Okura T, Higaki J, Kurata M, et al. Elevated serum uric acid is an independent predictor for cardiovascular events in patients with severe coronary artery stenosis subanalysis of the Japanese coronary artery disease (JCAD) study. Circulation, 2009, 73: 885-891.
[8] Sinan Deveci O, Kabakci G, Okutucu S, et al. The association between serum uric acid level and coronary artery disease. Int J Clin Pract,2010, 64: 900-907.
[9] Zhang J, He L, Cao S, et al. Association of serum uric acid and coronary artery disease in premenopausal women. Plos One, 2014, 9:106.
[10] Moriarity JT, Folsom AR, Iribarren C, et al. Serum uric acid and risk of coronary heart disease: Atherosclerosis Risk in Communities (ARIC)Study. Ann Epidemiol, 2000, 10: 136-143.
[11] Bos MJ, Koudstaal PJ, Hofman A, et al. Uric acid is a risk factor for myocardial infarction and stroke the Rotterdam study. Stroke, 2006,37: 1503-1507.
[12] Holme I, Aastveit AH, Hammar N, et al. Uric acid and risk of myocardial infarction, stroke and congestive heart failure in 417 734 men and women in the ApolipoproteinMortalityRISk study (AMORIS). J Intern Med, 2009, 266: 558-570.
[13] Onat A, Can G, Örnek E, et al. Elevated serum uric acid in nondiabetic people mark pro-inflammatory state and HDL dysfunction and independently predicts coronary disease. Clinical rheumatology, 2013,32: 1767-1775.
[14] Liese AD, Hense HW, Löwel H, et al. Association of Serum Uric Acid with All-Cause and Cardiovascular Disease Mortality and Incident Myocardial Infarction in the MONICA Augsburg Cohort. Epidemiology,1999, 10: 391-397.
[15] Culleton BF, Larson MG, Kannel WB, et al. Serum uric acid and risk for cardiovascular disease and death: the Framingham Heart Study. Ann Intern Med, 1999, 131: 7-13.
[16] Freedman DS, Williamson DF, Gunter EW, et al. Relation of serum uric acid to mortality and ischemic heart disease the NHANES I epidemiologic follow-up study. Am J Epidemiol, 1995, 141: 637-644.
[17] Meisinger C, Koenig W, Baumert J, et al. Uric acid levels are associated with all-cause and cardiovascular disease mortality independent of systemic inflammation in men from the general population the MONICA/KORA cohort study. Arterioscler Thromb Vasc Biol, 2008, 28: 1186-1192.
[18] Wheeler JG, Juzwishin KD, Eiriksdottir G, et al. Serum uric acid and coronary heart disease in 9, 458 incident cases and 155, 084 controls:prospective study and meta-analysis. Plos Med, 2005, 2: 236.
[19] Kim SY, Guevara JP, Kim KM, et al. Hyperuricemia and coronary heart disease: a systematic review and meta-analysis. Arthritis Care Res, 2010, 62: 170-180.
[20] Fang J, Alderman MH. Serum uric acid and cardiovascular mortality:the NHANES I epidemiologic follow-up study, 1971-1992. Jama,2000, 283: 2404-2410.
[21] Royston P, Ambler G, Sauerbrei W. The use of fractional polynomials to model continuous risk variables in epidemiology. Int J Epidemiol,1999,28: 964-974.
(编辑:王宝茹)
Meta Analysis for the Relationship Between the Levels of Serum Uric Acid and Prevalence of Coronary Artery Disease
LU Yong-bin, CHENG Zhi-yuan, ZHAO Ya-xue, CHANG Xiao-yu, CHENG Ning.
Institute of Epidemiology and Statistics, School of Public Health, Lanzhou University, Lanzhou (730000), Gansu, China
Corresponding Author: CHENG Ning, Email:chengn@lzu.edu.cn
Uric acid; Coronary artery disease
730000 甘肃省兰州市,兰州大学 公共卫生学院(芦永斌、赵亚学、常晓宇),基础医学院(程治远、程宁)
芦永斌 硕士研究生 主要从事流行病与卫生统计学研究 Email:luyb14@lzu.edu.cn 通讯作者:程宁 Email:chengn14@lzu.edu.cn
R54
A
1000-3614(2016)07-0640-04
10.3969/j.issn.1000-3614.2016.07.005
(2016-01-20)
猜你喜欢
中老年保健(2022年4期)2022-08-22
茶道(2022年3期)2022-04-27
昆明医科大学学报(2022年1期)2022-02-28
中老年保健(2021年6期)2021-11-30
天津医科大学学报(2021年4期)2021-08-21
昆明医科大学学报(2021年6期)2021-07-31
现代临床医学(2021年2期)2021-03-29
中成药(2018年11期)2018-11-24
益寿宝典(2018年5期)2018-01-28
中西医结合心脑血管病杂志(2016年20期)2016-03-01
