轻度认知障碍磁共振扩散张量成像研究的Meta分析
2016-06-27 06:34:10王东东姜春晖王俭
磁共振成像 2016年2期
王东东,姜春晖,王俭
轻度认知障碍磁共振扩散张量成像研究的Meta分析
王东东,姜春晖,王俭*
[摘要]目的 用Meta分析法评价磁共振扩散张量成像对轻度认知障碍(mild cognitive impairment, MCI)的诊断价值。材料与方法 使用计算机检索数据库Pubmed、CNKI、万方、维普等,收集有关磁共振扩散张量成像对MCI研究的文献,检索时限均为自建库至2015年1月31日。从文献中提取轻度认知障碍组与正常对照组(NC)所使用的定量指标各向异性(fractional anisotrophy, FA)值对不同脑区(额叶、顶叶、颞叶、枕叶、后扣带束、海马、海马旁回、内囊后肢、上、下纵束、穹窿、胼胝体膝部及压部、钩束)的测量数据,用Meta分析软件(Review manager 5.3)对最终符合标准的文献进行汇总分析,获得汇总加权均数差(weighted mean difference, WMD)及95%可信区间(95%CI)。结果 共纳入47篇文献(30篇英文、17篇中文),MCI组的FA值低于NC组,汇总WMD及95%CI为–0.05[–0.05, 0.04],上述脑区除枕叶外差异均具有统计学意义。结论 MCI患者存在脑白质微细结构的损害,弥散张量成像(diffusion tensor imaging, DTI)技术能够提供MCI的早期诊断指标。
[关键词]轻度认知障碍;扩散张量成像;Meta分析;帕金森病
作者单位:新疆医科大学第一附属医院影像中心核磁室,乌鲁木齐 830054
接受日期:2016-01-06
王东东, 姜春晖, 王俭. 轻度认知障碍磁共振扩散张量成像研究的Meta分析.磁共振成像, 2016, 7(2): 81–89.
*Correspondence to: Wang J, E-mail: jeanw1265@sina.com
Received 5 Nov 2015, Accepted 6 Jan 2016
轻度认知障碍(mild cognitive impairment,MCI)是介于正常老化和老年痴呆(alzheimer disease, AD)之间的中间过渡阶段,MCI转化为AD的概率高,因此,加强MCI群体的研究,对AD的早期诊断以及早期干预有着非常重要的意义。弥散张量成像(diffusion tensor imaging, DTI)技术是在弥散加权成像(diffusion weighted imaging, DWI)的基础上发展起来的,能够更精确地描述水分子的各向异性(fractional anisotrophy, FA),通过测定MCI患者不同脑区的FA值,根据FA值的变化可为MCI患者的早期诊断提供可靠的有价值的影像学资料。国内外使用DTI技术研究MCI的相关文献非常多,但常由于种种原因造成研究结果存在较大的差异。为客观的评价DTI技术对MCI的诊断价值,本研究全面收集国内外公开发表的中英文文献进行Meta分析。
1 材料与方法
1.1文献检索
文献检索主要包括中文检索及英文检索,搜索Pubmed、CNKI、万方、维普等数据库,中文检索词“轻度认知障碍”或“轻度认知功能损害”或“轻度认知功能损伤”、“扩散张量成像”或“弥散张量成像”或“磁共振扩散张量成像”或“磁共振弥散张量成像”。英文检索词“magnetic resonance imaging”、“diffusion tensor imaging”、“mild cognitive impairment”或“mild cognitive disorders”,发表年限从建库至2015年1月31日。
1.2纳入与排除标准
纳入标准:(1)选择的文献为2015年1月31日前公开发表的中、英文文献且文献中的研究对象为“人类”;(2)MCI以记忆减退主诉,时间超过6个月并由知情者确认,其余认知功能相对正常,简易精神状态检查(mini-mental state examination,MMSE)总分≥24分;(3)日常活动能力无显著缺损,无任何精神或神经病史,MRI检查发现除了脑萎缩和深部白质少量T2WI高信号(最大直径<1 cm)外,无其它异常改变;(4)利用DTI对MCI患者和正常对照组(NC)特定的脑区(额叶、顶叶、颞叶、枕叶、后扣带束、海马、海马旁回、内囊后肢、上、下纵束、穹窿、胼胝体膝部及压部、钩束)进行FA值的提取,所得数据均以±s表示。
排除标准:(1)公开发表的中文及英文以外的文献;(2)所研究数据无法获取的文献;(3)尚未发表或重复发表的文献;(4)发表类型为综述、讲座、会议、个案报道、述评等。
1.3文献质量评价与资料提取
参考Newcastle-Ottawa[1]标准、纳入标准与排除标准,由2名评价员对文献质量方法学进行评价,评价过程如遇不一致,则经第三方共同商讨解决。评价后,在纳入的文献中提取:(1)文献第一作者、研究国家、发表年限、磁场强度、MCI组和NC组例数、平均年龄、性别比例;(2)不同脑区(额叶、顶叶、颞叶、枕叶、后扣带束、海马、海马旁回、内囊后肢、上、下纵束、穹窿、胼胝体膝部及压部、钩束)的FA值,若含有双侧大脑半球的数据,则统一选取左侧。
1.4数据分析
用Meta分析软件(Review manager 5.3)对MCI组和NC组整体脑区及不同脑区的FA值分别进行比较。在α=0.05水平下,以χ2检验对各组比较进行异质性检验,若P≥0.05,则不拒绝同质性假设,采用固定效应模型(fixed effects models,FEM)进行分析;若P<0.05,则拒绝同质性假设,采用随机效应模型(random effects models,REM)进行分析。根据相应的效应模型进行分析,获得汇总加权均数差(weighted mean difference,WMD)及95%可信区间(95%CI),同时绘制森林图(forest plot)。
2 结果
2.1文献检出结果及纳入文献基本特征
共初检出437篇文献,通过评价和筛选共纳入47篇文献(30篇英文[2-31]、15篇中文[32-48]),文献筛选流程见图1,纳入文献基本特征见表1。

图1 文献筛选流程及结果Fig. 1 Literature screening process and results

表1 纳入文献的基本特征Tab. 1 Basic characteristics of the literature

续表1 纳入文献的基本特征Continued tab. 1 Basic characteristics of the literature
2.2数据分析结果
47篇文献共包含174项比较,如图2所示。其中19篇含有MCI组与NC组额叶的FA值比较,15篇含有MCI组与NC组顶叶的FA值比较,16篇含有MCI组与NC组颞叶的FA值比较,12篇含有MCI组与NC组枕叶的FA值比较,22篇含有MCI组与NC组后扣带束的FA值比较,8篇含有MCI组与NC组海马的FA值比较,9篇含有MCI组与NC组海马旁回的FA值比较,6篇含有MCI组与NC组内囊后肢的FA值比较,9篇含有MCI组与NC组上纵束的FA值比较,4篇含有MCI组与NC组下纵束的FA值比较,3篇含有MCI组与NC组穹窿的FA值比较,23篇含有MCI组与NC组胼胝体膝部的FA值比较,23篇含有MCI组与NC组胼胝体压部的FA值比较,5篇含有MCI组与NC组钩束的FA值比较。其中,海马旁回、穹窿、钩束等脑区FA值的汇总使用的是固定效应模型,额叶、顶叶、颞叶、枕叶、后扣带束、海马、内囊后肢、上、下纵束、胼胝体膝部及压部、等脑区使用的随机效应模型。
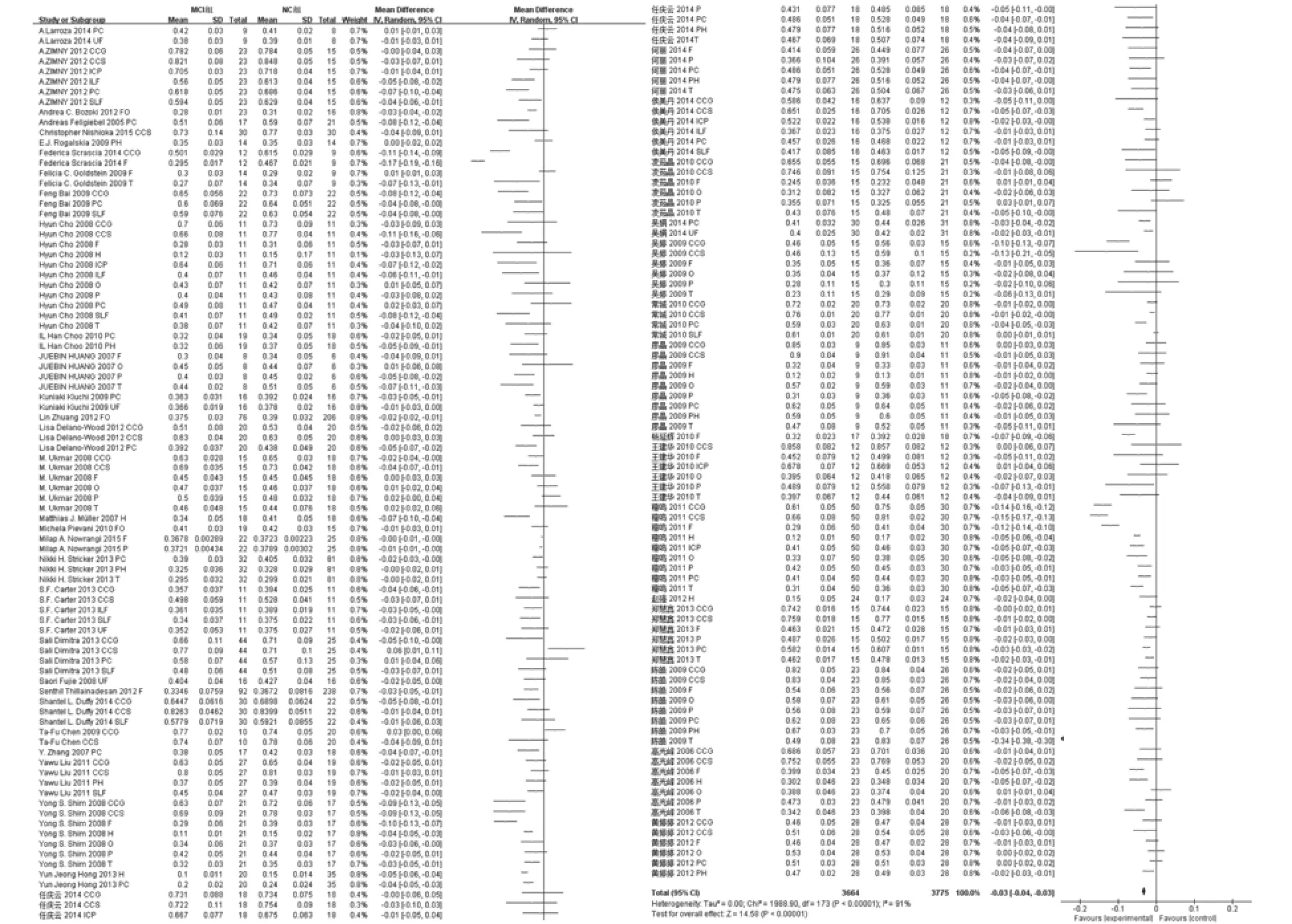
图2 整体森林图Fig. 2 Integrated forest map
2.3Meta分析结果
整体森林图(图2)所示,合并后病变共3664处,正常对照共3775处,整体汇总WMD及其95%CI为–0.03[–0.04,–0.03],差异具有统计学意义(P<0.05)。额叶FA值合并后,病变共428处,正常对照为555处,额叶汇总WMD及其95%CI为–0.04[–0.06,–0.02],差异具有统计学意义(P<0.05)。顶叶FA值合并后,病变共283处,正常对照为271处,顶叶汇总WMD及其95%CI为–0.02[–0.03,–0.01],差异具有统计学意义(P<0.05)。颞叶FA值合并后,病变共307处,正常对照为336处,颞叶汇总WMD及其95%CI为–0.06[–0.08,–0.03],差异具有统计学意义(P<0.05)。枕叶FA值合并后,病变共230处,正常对照为215处,枕叶汇总WMD及其95%CI为–0.01[–0.03,–0.00],差异不具有统计学意义(P>0.05)。后扣带束FA值合并后,病变共485处,正常对照为507处,后扣带束汇总WMD及其95%CI为–0.03[–0.04,–0.02],差异具有统计学意义(P<0.05)。海马FA值合并后,病变共176处,正常对照为166处,海马汇总WMD及其95%CI为–0.04[–0.05,–0.03],差异具有统计学意义(P<0.05)。海马旁回FA值合并后,病变共196处,正常对照为241处,海马旁回汇总WMD及其95%CI为–0.02[–0.02,–0.01],差异具有统计学意义(P<0.05)。内囊后肢FA值合并后,病变共130处,正常对照为98处,内囊后肢汇总WMD及其95%CI为–0.03[–0.05,–0.01],差异具有统计学意义(P<0.05)。上纵束FA值合并后,病变共204处,正常对照为157处,上纵束汇总WMD及其95%CI为–0.03[–0.05,–0.01],差异具有统计学意义(P<0.05)。下纵束FA值合并后,病变共61处,正常对照为49处,下纵束汇总WMD及其95%CI为–0.03[–0.06,–0.01],差异具有统计学意义(P<0.05)。穹窿FA值合并后,病变共118处,正常对照为237处,穹窿汇总WMD及其95%CI为–0.02[–0.03,–0.01],差异具有统计学意义(P<0.05)。胼胝体膝部FA值合并后,病变共478处,正常对照为425处,胼胝体膝部汇总WMD及其95%CI为–0.04[–0.06,–0.02],差异具有统计学意义(P<0.05)。胼胝体压部FA值合并后,病变共486处,正常对照为436处,胼胝体压部汇总WMD及其95%CI为–0.03[–0.05,–0.02],差异具有统计学意义(P<0.05)。钩束FA值合并后,病变共82处,正常对照为82处,钩束汇总WMD及其95%CI为–0.02[–0.02,–0.01],差异具有统计学意义(P<0.05)。
3 讨论
Meta分析已广泛应用于医学的各个领域之中,在医学影像学中主要应用于两大方面:一是对影像技术的测量指标的评价,如Sexton CE等[49]的研究;二是对影像诊断实验效能的评价,如李树金等[50]的研究,本文所使用的方法与前者类似,即从文献中提取MCI组和NC组的例数及为连续性数据的结果指标x±s,通过Meta分析软件进行统计合并得到加权均数差及森林图等,用来评估DTI技术对FA值测量结果有一个全面、整体的认识。
在Meta分析软件Review manager 5.3中,连续性变量采用W M D进行比较分析。当总体WMD>0(或某研究的95%CI上下限均大于0)时,或在森林图中某个研究的95%CI的横线不与无效竖线相交,且该横线落在无效线右侧时,可认为实验组某指标的均数大于对照组,实验因素可增加某指标的均数;当总体WMD<0(或某研究的95%CI上下限均小于0)时,或在森林图中某个研究的95%CI的横线不与无效竖线相交,且该横线落在无效线左侧时,可认为实验组某指标的均数大于对照组,实验因素可增加某指标的均数。
DTI主要利用水分子的分数FA来表示,FA可以反映纤维束轴突结构的方向程度,反映结构的完整性,反映各向异性的弥散张量强度信息,与髓鞘的结构完整性、纤维的密度及走向一致性均具有密切关系,能够反映白质纤维束是否完整。除磁场强度外,FA值受扩散敏感梯度方向和扫描所选取的b值的影像。如果已知被测脑白质纤维的张量方向,那么沿3个编码方向即可得到全部的信息;如果被测纤维的张量方向未知,只要梯度方向达到最优化,6个以上编码方向即可确定FA值。本研究中纳入的文献中所取的编码方向均在6个以上。Yoshiura等人[5 1]得出,当b值≥600 s/mm2时,各个感兴趣区所测得的FA值不会随着b的改变而变化。研究表明在MRI功能成像中DTI对于区分正常老化、MCI及AD最有帮助[52]。Zhang等人[53]研究发现MCI病人与正常对照组相比较其纤维回路的FA值下降,特别是在左侧半球,而且本文的纳入文献中左侧大脑半球差异有统计学意义者居多,故本文分析若存在双侧大脑半球数据的均统一选取左侧大脑半球。
本文共包含174项比较,合并后得到3664处病灶和3775处对照,汇总分析得出WMD及其95%可信区间为–0.03[–0.04,–0.03],差异具有统计学意义(P<0.05)。整体汇总表明MCI组与NC组的FA值相比较是降低的,这预示着在MCI人群中存在着广泛区域的脑白质损害,这种损害可以通过FA值进行测量所得,FA值和认知功能的变化密切相关[54-55],而且MCI人群脑白质完整性的损害是早于相应脑区体积的变化[56]。纳入分析的各个脑区,额叶和顶叶白质和MCI人群的执行功能密切相关[5];MCI组的颞叶、后扣带束、海马旁回等区域的脑白质完整性的改变比相应皮质厚度的改变在早期诊断AD时更敏感,而且这些区域与记忆功能密切相关[8];MCI组海马区的FA降低,海马是参与记忆与认知功能的重要结构,可以通过白质纤维通路产生各种记忆功能[57];钩束是额叶运动性语言区和眶回之间的联络纤维,与记忆和行为密切相关;上纵束与执行控制功能[58]和工作记忆有关[59],上、下纵束起着传递从大脑后部到大脑前部的感官、视觉、听觉等体觉信息[60];胼胝体是连接双侧大脑半球最大的纤维束,有研究表明胼胝体白质的不完整与AD的发生有关[60];穹窿是下丘脑最粗大的传入纤维,穹窿损伤可增加引起情景记忆障碍的可能[51]。这些脑区的相关功能符合MCI患者出现的临床表现。
脑区分别进行比较时,枕叶汇总分析得出WMD及其95%可信区间为–0.01[–0.03, –0.00],95%可信区间与无效线相交,差异不具有统计学意义(P>0.05),这与纳入文献中大多数观点一致,说明在MCI尚未过渡到AD时,枕叶白质的纤维束是完整的、没有损伤的。其中,额叶、颞叶、胼胝体膝部进行汇总分析时,合并后所得结果存在高度的异质性,这是由于本文纳入的部分文献不是单纯使用感兴趣区(region of interest,ROI)测量的FA值,而是(还)使用了基于体素分析的技术,还有部分文献进行合并时“额上回”归于额叶、“颞横回”归于颞叶进行汇总等,此外这些被纳入的文献中在选取病例时存在着纳入个体间的变异等。由于基于体素的分析是在像素水平对脑MR图像进行的一种自动而又客观的分析技术,与ROI相比受人为因素的影响较小,混杂因素较少,因此引起上述部位的高度异质性。
综上所述,本文将DTI对轻度认知障碍诊断的相关研究进行汇总分析,避免了大多数研究样本量小的不足,大大增加了研究的样本量,提高了汇总分析结果的可信度。通过汇总分析可知,在未发展为AD时的MCI人群中,已存在多区域的脑白质纤维的损害。DTI作为一种无创的显示活体大脑白质神经纤维通路的方法,在临床上有广阔的运用前景。本文也存在着以下不足之处:(1)本文的纳入文献仅限于公开发表的中英文,存在着语种的偏倚;(2)部分纳入文献不仅采用了ROI分析,而且有基于体素的分析方法,存在测量偏倚;(3)少数文献样本量较少,存在选择偏倚;(4)本文未做出与AD的鉴别,没有将结果与疾病分级指标MMSE进行关联分析。希望在以后的研究中,对以上不足进行改善。
参考文献[References]
[1]Ownby RL, Crocco E, Acevedo A, et al. Depression and risk for alzheimer’s disease: systematic review, meta-analysis, and metaregression analysis. Arch Gen Psychiatry, 2006, 63(5): 530-538.
[2]Bai F, Zhang Z, Watson DR, et al. Abnormal integrity of association fiber tracts in amnestic mild cognitive impairment. J Neurol Sci, 2009, 278(1-2): 102-106.
[3]Cho H, Yang DW, Shon YM, et al. Abnormal integrity of corticocortical tracts in mild cognitive impairment: a diffusion tensor imaging study. J Korean Med Sci, 2008, 23(3): 477-483.
[4]Zhuang L, Wen W, Trollor JN, et al. Abnormalities of the fornix in mild cognitive impairment are related to episodic memory loss. J Alzheimers Dis, 2012, 29(3): 629-639.
[5]Pievani M, Agosta F, Pagani E, et al. Assessment of white matter tract damage in mild cognitive impairment and alzheimer’s disease. Hum Brain Mapp, 2010, 31(12): 1862-1875.
[6]Nowrangi MA, Okonkwo O, Lyketsos C, et al. Atlas-based diffusion tensor imaging correlates of executive function. J Alzheimers Dis, 2015, 44(2): 585-598.
[7]Duffy SL, Paradise M, Hickie IB, et al. Cognitive impairment with and without depression history: an analysis of white matter microstructure. J Psychiatry Neurosci, 2014, 39(2): 135-143.
[8]Fellgiebel A, Müller MJ, Wille P, et al. Color-coded diffusiontensor-imaging of posterior cingulate fiber tracts in mild cognitive impairment. Neurobiol Aging, 2005, 26(8): 1193-1198.
[9]Stricker NH, Salat DH, Foley JM, et al. Decreased white matter integrity in neuropsychologically defined mild cognitive impairment is independent of cortical thinning. J Int Neuropsychol Soc, 2013, 19(8): 925-937.
[10]Müller MJ, Greverus D, Weibrich C, et al. Diagnostic utility of hippocampal size and mean diffusivity in amnestic MCI. Neurobiol Aging, 2007, 28(3): 398-403.
[11]Shim YS, Yoon B, Shon YM, et al. Difference of the hippocampal and white matter microalterations in MCI patients according to the severity of subcortical vascular changes: neuropsychological correlates of diffusion tensor imaging. Clin Neurol Neurosurg, 2008, 110(6): 552-561.
[12]Liu Y, Spulber G, Lehtimäki KK, et al. Diffusion tensor imaging and tract-based spatial statistics in alzheimer’s disease and mild cognitive impairment. Neurobiol Aging, 2011, 32(9): 1558-1571.
[13]Zhang Y, Schuff N, Jahng GH, et al. Diffusion tensor imaging of cingulum fibers in mild cognitive impairment and alzheimer’s disease. Neurology, 2007, 68(1): 13-19.
[14]Bozoki AC, Korolev IO, Davis NC, et al. Disruption of limbic white matter pathways in mild cognitive impairment and alzheimer’s disease: a DTI/FDG-PET study. Hum Brain Mapp,2012, 33(8): 1792-1802.
[15]Ukmar M, Makuc E, Onor ML, et al. Evaluation of white matter damage in patients with alzheimer’s disease and in patients with mild cognitive impairment by using diffusion tensor imaging. Radiol Med, 2008, 113(6): 915-922.
[16]Hong YJ, Yoon B, Lim SC, et al. Microstructural changes in the hippocampus and posterior cingulate in mild cognitive impairment and alzheimer’s disease: a diffusion tensor imaging study. Neurol Sci, 2013, 34(7): 1215-1221.
[17]Choo IH, Lee DY, Oh JS, et al. Posterior cingulate cortex atrophy and regional cingulum disruption in mild cognitive impairment and alzheimer’s disease. Neurobiol Aging, 2010,31(5): 772-779.
[18]Delano-Wood L, Stricker NH, Sorg SF, et al. Posterior cingulum white matter disruption and its associations with verbal memory and stroke risk in mild cognitive impairment. J Alzheimers Dis, 2012, 29(3): 589-603.
[19]Carter SF, Embleton KV, Anton-Rodriguez JM, et al. Regional neuronal network failure and cognition in late-onset sporadic alzheimer’s disease. AJNR Am J Neuroradiol, 2014, 35(6 Suppl): 18-30.
[20]Scrascia F, Curcio G, Ursini F, et al. Relationship among diffusion tensor imaging, EEG activity, and cognitive status in mild cognitive impairment and alzheimer’s disease patients. J Alzheimers Dis, 2014, 38(4): 939-950.
[21]Goldstein FC, Mao H, Wang L, et al. White matter Integrity and episodic memory performance in mild cognitive impairment: a diffusion tensor imaging study. Brain Imaging Behav, 2009,3(2): 132-141.
[22]Kiuchi K, Morikawa M, Taoka T, et al. Abnormalities of the uncinate fasciculus and posterior cingulate fasciculus in mild cognitive impairment and early alzheimer’s disease: a diffusion tensor tractography study. Brain Res, 2009, 1287(9): 184-191.
[23]Huang J, Auchus AP. Diffusion tensor imaging of normal appearing white matter and its correlation with cognitive functioning in mild cognitive impairment and alzheimer’s disease. Ann N Y Acad Sci, 2007, 1097(1): 259-264.
[24]Nishioka C, Poh C, Sun SW. Diffusion tensor imaging reveals visual pathway damage in patients with mild cognitive impairment and alzheimer’s disease. J Alzheimers Dis, 2015,45(1): 97-107.
[25]Zimny A, Szewczyk P, Bladowska J, et al. Quantitative evaluation of changes in the selected white matter tracts using diffusion tensor imaging in patients with alzheimer’s disease and mild cognitive impairment. Neuroradiol J, 2012, 25(3): 300-310.
[26]Fujie S, Namiki C, Nishi H, et al. The role of the uncinate fasciculus in memory and emotional recognition in amnestic mild cognitive impairment. Dement Geriatr Cogn Disord, 2008,26(5): 432-439.
[27]Chen TF, Lin CC, Chen YF, et al. Diffusion tensor changes in patients with amnesic mild cognitive impairment and various dementias. Psychiatry Res, 2009, 173(1): 15-21.
[28]Thillainadesan S, Wen W, Zhuang L, et al. Changes in mild cognitive impairment and its subtypes as seen on diffusion tensor imaging. Int Psychogeriatr, 2012, 24(9): 1483-1493.
[29]Rogalski EJ, Murphy CM, deToledo-Morrell L, et al. Changes in parahippocampal white matter integrity in amnestic mild cognitive impairment: a diffusion tensor imaging study. Behav Neurol, 2009, 21(1): 51-61.
[30]Sali D, Verganelakis DA, Gotsis E, et al. Diffusion tensor imaging (DTI) in the detection of white matter lesions in patients with mild cognitive impairment (MCI). Acta Neurol Belg, 2013, 113(4): 441-451.
[31]Larroza A, Moratal D, D’Ocón AV, et al. Tractography of the uncinate fasciculus and the posterior cingulate fasciculus in patients with mild cognitive impairment and Alzheimer disease. Neurologia, 2014, 29(1): 11-20.
[32]Gao GF. DTI study of alzheimer’s disease, mild cognitive impairment. Tianjin: Tianjin Medical University, 2006.高光峰. Alzheimer病及轻度认知障碍磁共振扩散张量成像的研究. 天津: 天津医科大学, 2006.
[33]Wang JH, Lv PY, Wang H, et al. Study of microstructural white matter lesions in patients with mild cognitive impairment and mild and moderate alzheimer’s disease. Chinese Journal of Neuroimmunology and Neurology, 2010, 17(3): 211-214.王建华, 吕佩源, 王贺波, 等. DTI评价轻度认知障碍及轻中度阿尔茨海默病脑白质微细结构损害的研究. 中国神经免疫学和神经病学杂志, 2010, 17(3): 211-214.
[34]Wu T, Liu W, Xiao CY, et al. Study of diffusion tensor imaging in patients with alzheimer’s disease and mild cognitive impairment. Journal of Clinical Psychiatry, 2009, 19(4): 224-226.吴婷, 刘文, 肖朝勇, 等. 阿尔茨海默病与轻度认知障碍弥散张量成像研究. 临床精神医学杂志, 2009, 19(4): 224-226.
[35]Chen H, Hong N, Yu X, et al. Diffusion tentor imaging evaluation of white matter alternations in patients with mild cognitive impairment. Chin J Med Imaging Technol, 2009,25(8): 1358-1360.陈皓, 洪楠, 于欣, 等. 磁共振扩散张量成像评价轻度认知障碍患者的脑白质变化. 中国医学影像技术, 2009, 25(8): 1358-1360.
[36]Chang C, Li WB, Xie WH, et al. Diffusion tensor imaging of association fiber tracts in amnestic mild cognitive. Chin J Med Imaging Technol, 2010, 26(1): 56-59.常城, 李文彬, 谢文晖, 等. 扩散张量成像观察遗忘型轻度认知障碍患者联合纤维束. 中国医学影像技术, 2010, 26(1): 56-59.
[37]Ji M, Ye CT, Miao HD, et al. Quantitive evaluation of senile mild cognitive impairment using MR DTI. Shanghai Medical Imaging, 2011, 20(3): 200-204.嵇鸣, 叶春涛, 苗华栋, 等. 老年轻度认知功能障碍的高场MR脑DTI定量研究. 上海医学影像, 2011, 20(3): 200-204.
[38]Ren QY, He L, Liu Z, et al. Diffusion tensor imaging study of cingulum fibers in mild cognitive impairment. Journal of clinical rational druguse, 2014, 7(2): 23-24.任庆云, 何丽, 刘斋, 等. 轻度认知功能障碍患者后扣带回的磁共振扩散张量成像研究. 临床合理用药杂志, 2014, 7(2): 23-24.
[39]Ren QY, He L, Liu Z, et al. FA value alteration in white in patients with mild cognitive impairment measured by MR diffusion tensor imaging. Journal of difficult diseases, 2014,13(1): 34-36, 39.任庆云, 何丽, 刘斋, 等. 轻度认知功能障碍患者在MR扩散张量成像中脑白质各向异性分数值的变化. 疑难病杂志, 2014,13(1): 34-36, 39.
[40]Liao J, Yuan HS, Zhu Y, et al. MR diffusion tensor imagingbased white matter studies in mild cognitive impairment and Alzheimer disease. Zhonghua Fang She Xue Za Zhi, 2009,43(5): 490-494.廖晶, 袁慧书, 朱玥, 等. 轻度认知功能障碍及阿尔茨海默病脑白质的MR扩散张量成像研究. 中华放射学杂志, 2009,43(5): 490-494.
[41]He L, Liu Z, Ren QY, et al. The study of diffusion tensor imaging in patients with mild cognitive impairment. J Pract Radiol, 2014, 30(8): 1255-1258.何丽, 刘斋, 任庆云, 等. 轻度认知障碍的 MR 扩散张量成像研究. 实用放射学杂志, 2014, 30(8): 1255-1258.
[42]Huang TT, Liu F, Liu ZL, et al. The application tensor imaging on 3.0 T MR in amnestic mild cognitive impairment. J Chin Clin Med Imaging, 2012, 23(2): 77-80.黄婷婷, 刘鹏飞, 刘志兰, 等. 遗忘型轻度认知障碍的弥散张量成像研究. 中国临床医学影像杂志, 2012, 23(2): 77-80.
[43]Hou MD, Fan GG, Li SB, et al. Diffusion tensor imaging for evaluating white matter fiber tracts in patients with amnestic mild cognitive impairment. Radiology Practice, 2014, 29(12): 1392-1395.侯美丹, 范国光, 李松柏, 等. 遗忘型轻度认知障碍脑白质纤维束扩散张量成像研究. 放射学实践, 2014, 29(12): 1392-1395.
[44]Wu J, Gu HM, Cao L, et al. Study of white matter tractography in patients with amnestic mild cognitive impairment. J Pract Radiol , 2014, 30(11): 1787-1790, 1801.吴娟, 顾红梅, 曹亮, 等. 遗忘型轻度认知障碍的脑白质纤维束成像研究. 实用放射学杂志, 2014, 30(11): 1787-1790, 1801.
[45]Ling RJ, Ni XS, Zhang L, et al. The correlation between diffusion tensor imaging and cognitive function in elders. Chinese Clinical Neuroscience, 2010, 18(6): 622-630.凌茹晶, 倪秀石, 张琳, 等. 弥散张量成像与老年人认知功能的相关性. 中国临床神经科学, 2010, 18(6): 622-630.
[46]Yang YH, Liang PP, Qin W, et al. DTI study of the white matter of dorsa lateral prefrontal cortex in patients with mild cognitive impairment. J Clin Radiol, 2010, 29(4): 432-435.杨延辉, 梁佩鹏, 秦文, 等. 轻度认知障碍患者背外侧前额叶白质的DTI研究. 临床放射学杂志, 2010, 29(4): 432-435.
[47]Zheng HX. The applying value of diffusion kurtosis imaging in mild cognitive impairment and alzheimer’s disease. Taiyuan: Shanxi Medical University, 2013.郑慧鑫. 扩散峰度成像在轻度认知障碍及阿尔茨海默病中的应用价值. 太原: 山西医科大学, 2013.
[48]Zhao Q. The value of magnetic resonance diffusion tensor imaging in patients with mild cognitive impairment. Jinan: Shandong University, 2013.赵强. 磁共振弥散张量成像在轻度认知功能障碍中的应用价值研究. 济南: 山东大学, 2012.
[49]Sexton CE, Kalu UG, Filippini N, et al. A meta-analysis of diffusion tensor imaging in mild cognitive impairment and alzheimer’s disease. Neurobiol Aging, 2011, 32(12): 5-18.
[50]Li SJ, Wu XB, Zhang SW, et al. Meta analysis on apparent diffusion coefficient used to differentiate benign from malignant soft tissue tumors. Chin J Magn Reson Imaging, 2012, 3(4): 255-259.李树金, 吴晓冰, 张绍伟, 等. 表观扩散系数鉴别良恶性软组织肿瘤价值的Meta分析. 磁共振成像, 2012, 3(4): 255-259.
[51]Yoshiura T, Wu O, Zaheer A, et al. Highly diffusion-sensitized MRI of brain: dissociation of gray and white matter. Magn Reson Med, 2001, 45(5): 734-740.
[52]Zimny A, Szewczyk P, Trypka E, et al. Multimodal imaging in diagnosis of alzheimer’s disease and amnestic mild cognitive impairment: value of magnetic resonance spectroscopy,perfusion, and diffusion tensor imaging of the posterior cingulate region. J Alzheimers Dis, 2011, 27(3): 591-601.
[53]Zhang Y, Schuff N, Jahng GH, et al. Diffusion tensor imaging of cingulum fibers in mild cognitive impairment and alzheimer’s disease. Neurology, 2007, 68(1): 13-19.
[54]Mielke MM, Kozauer NA, Chan KC, et al. Regionally-specific diffusion tensor imaging in mild cognitive impairment and alzheimer’s disease. Neuroimage, 2009, 46(1): 47-55.
[55]Nowrangi MA, Lyketsos CG, Leoutsakos JM, et al. Longitudinal, region-specific course of diffusion tensor imaging measures in mild cognitive impairment and alzheimer’s disease. Alzheimers Dement, 2013, 9(5): 519-528.
[56]Clerx L, Visser PJ, Verhey F, et al. New MRI markers for alzheimer’s disease: a meta-analysis of diffusion tensor imaging and a comparison with medial temporal lobe measurements. J Alzheimers Dis, 2012, 29(2): 405-429.
[57]Tang SX, Dai JP. DTI and SWI application progress on hipppcampus in patients with alzheimer’s disease. Chin J Magn Reson Imaging, 2015, 6(9): 699-703.唐守现, 戴建平. 扩散张量成像和磁敏感加权成像在阿尔茨海默病海马的研究进展. 磁共振成像, 2015, 6(9): 699-703.
[58]Elderkin-Thompson V, Ballmaier M, Hellemann G, et al. Executive function and MRI prefrontal volumes among healthy older adults. Neuropsychology, 2008, 22(5): 626-37.
[59]Hamidi M, Tononi G, Postle BR. Evaluating frontal and parietal contributions to spatial working memory with repetitive transcranial magnetic stimulation. Brain Res, 2008, 1230(9): 202-210.
[60]Pantel J, Schröder J, Jauss M, et al.Topography of callosal atrophy reflects distribution of regional cerebral volume reduction in alzheimer’s disease. Psychiatry Res, 1999, 90(3): 181-192.
Measurement of diffusion tensor imaging in patients with mild cognitive impairment: a meta analysis
WANG Dong-dong, JIANG Chun-hui, WANG Jian*
MRI room of Imaging Center, the first affiliated hospital of Xinjiang Medical University, Urumqi 830054, China
Key wordsMild cognitive impairment; Diffusion tensor imaging; Meta-analysis;Parkinson disease
AbstractObjective: To investigate the value of MR diffusion tensor imaging in diagnosis of mild cognitive impairment (MCI) with Meta-analysis. Materials and Methods: A search in computer databases such as PubMed, CNKI WanFang and VIP Data was performed, the relevant literature which are related to the MR diffusion tensor imaging in diagnosis of MCI were collected from the date of the above mentioned databases’ establishment to January 31, 2015. The measured data of MCI and normal control (NC) was extracted from different brains (frontal lobe, parietal lobe, temporal lobe, occipital lobe, posterior cingulated fasciculus, hippocampus,parahippocampal gyrus, posterior limb of the internal capsule, fasciculus longitudinal superior, fasciculus longitudinal inferior, fornix, genu of corpus callosum, splenium of corpus callosum, uncinatus fasciculus), the relevant articles were analyzed with the Review Manager 5.3 to achieve weighted mean difference (WMD) with 95% confidence level CI. Results: Totally 47 articles including 30 English articles and 17 Chinese articles were collected. The outcome indicates the values of FA in the MCI group are lower than that in the NC group, and the WMD with 95% CI is –0.05[–0.05,0.04], the values of FA of both the above metioned brains have significantly statistical difference except occipital lobe. Conclusion: The microstructural white matter in MCI group have been impaired, DTI can provide early diagnosis index of MCI.
通讯作者:王俭,E-mail:jeanw1265@sina.com
收稿日期:2015-11-05
中图分类号:R445.2;R742
文献标识码:A
DOI:10.12015/issn.1674-8034.2016.02.001
猜你喜欢
保健医苑(2022年6期)2022-07-08 01:25:28
中国民间疗法(2021年10期)2021-07-22 02:32:40
成都医学院学报(2021年2期)2021-07-19 08:35:14
活力(2019年22期)2019-03-16 12:47:04
现代商贸工业(2016年25期)2016-12-26 14:56:36
中外医学研究(2016年26期)2016-11-30 02:38:27
云南中医中药杂志(2016年9期)2016-11-29 08:02:14
风湿病与关节炎(2016年10期)2016-11-23 07:06:16
中国中药杂志(2016年20期)2016-11-19 13:25:02
中国现代医生(2016年23期)2016-11-15 03:22:39