地中海贫血患者肝脏T2*、血清铁蛋白预测心肌铁过载价值研究
2016-05-17 02:58李大创黄海波尹晓林周亚丽管俊覃明黄桂雄
磁共振成像 2016年12期
李大创,黄海波*,尹晓林,周亚丽,管俊,覃明,黄桂雄
地中海贫血患者肝脏T2*、血清铁蛋白预测心肌铁过载价值研究
李大创1,黄海波1*,尹晓林2,周亚丽2,管俊1,覃明1,黄桂雄1
目的定量评估地中海贫血(thalassemia,TM)患者心肌和肝脏铁沉积,探讨肝脏T2*、血清铁蛋白(serum ferritin,SF)预测心铁过载价值。材料与方法应用3.0 T磁共振梯度多回波序列扫描基因确诊并满足要求的地中海贫血患者113例,测量其心肌和肝脏T2*值,所有受试者扫描前后7 d、间隔1 w实验室两次检测血清铁蛋白。对心肌T2*、肝脏T2*、SF分度诊断并应用秩相关分析3者间的关系,采用受试者工作特征曲线(receiver operating characteristic curve,ROC曲线),评价肝脏T2*<0.70 ms、SF>2500 μg/L时预测心铁过载及SF>300 μg/L预测肝铁过载诊断效能及最佳阈值。结果113例TM患者的铁沉积分度诊断如下:心肌正常94例,轻度6例,中度10例,重度3例;肝脏正常13例,轻度31例,中度29例,重度25例,极重度15例;血清铁蛋白正常1例,轻度48例,中度17例,重度35例,极重度12例。秩相关分析显示心肌T2*-肝脏T2*(rs=0.267,P=0.004)、心肌T2*-SF (rs=-0.63,P=0.000)、肝脏T2*-SF (rs=-0.641,P=0.000)三者间轻中度相关但无规律性。以心肌T2*<10 ms诊断心铁沉积异常,肝脏T2*<0.70 ms、SF>2500 μg/L预测心铁过载准确性分别为0.788和0.833,敏感度分别为80.0%、73.3%,特异性分别为70.4%、63.3%;以肝脏T2*<3.57 ms诊断肝铁过载,SF>300 μg/L预测肝铁过载ROC曲线下面积为0.719,敏感度为94.0%,特异性为15.4%。结论在一定范围内,MRI T2*扫描可直接定量体内器官铁沉积,心铁过载、肝铁沉积、SF三者间轻中度相关但无规律性;以肝脏T2*、血清铁蛋白预测心肌铁异常价值较低,而血清铁蛋白预测肝铁过载尚不可靠。
地中海贫血;磁共振成像;血清铁蛋白;心肌;铁过载
地中海贫血(thalassemia,TM)为常染色体缺陷导致的一或多种珠蛋白数量不足或缺乏,造成红细胞易被破坏的溶血性贫血。张之南等[1]将其分为α型、β型和遗传性胎儿血红蛋白持续存在综合征(hereditary persistence of fetal hemoglobin,HPFH),α-TM和β-TM进一步分重型、中间型、轻型与静止型。因重型α-TM死于宫内或早产,轻型、静止型和HPFH常不需处理,而中间型及β-重型TM常由于反复输血而引起铁沉积和内脏损害,心力衰竭为其死亡的最重要因素[2]。
多项研究[3-5]证实,磁共振成像(magnetic resonance imaging,MRI)可在一定范围内准确评价水模或心铁、肝铁浓度,现有少数以1.5 T MR文献[3,6]认为以SF、肝铁预测心铁沉积不可靠或准确度中等偏低。此外,磁共振在心肌微血管阻塞、心功能及细胞间质容积分数等评估亦具有重要意义[7]。然而,超高场强下和基因确诊的中间型及β-重型TM中体内SF、肝铁对心铁沉积诊断效能及SF预测肝铁过载的研究鲜有报告,笔者就此探讨TM体内肝脏T2*、血清铁蛋白预测心肌铁过载价值,以期为临床提供相关依据。
1 材料与方法
1.1 材料
随机选取2014年6月至2015年7月我院血液科117例TM患者磁共振心肌、肝脏T2*扫描,扫描前后7 d、间隔1 w完成两次实验室血清铁蛋白检测及记录其平均值。纳入标准:(1)基因诊断血红蛋白H病、中间型或重型β-TM;(2)反复多次输(全)血且达到10 U (1 U=200 ml)、未进行规律去铁治疗。排除标准:SF资料不完整、严重心律失常、幽闭恐惧、交流困难及其他原因不能完成MRI有效序列。试验获我院伦理委员会批准,志愿者或其家属知情并签署同意书。
1.2 设备与方法
Philips 3.0 T MR扫描仪、体部16通道线圈,头先进仰卧位、呼气后屏气和/或心舒中末期采集受试者肝门上一层肝实质、心室中部短轴位T2*序列图像,肝脏T2*成像前扫描冠状、横断位T2WI及横断位T1WI (参数略),心肌T2*成像前扫描左室标准横断位-两腔心-四腔心电影序列(参数略)并确定短轴位层面,MRI T2*参数设置:TR=200 ms,FA=20°,肝脏12回波序列TEmin/max(ms)=0.6~1.3/7.8~16.0,心肌8回波序列TEmin/max(ms)=1.1/12.6,回波间隙为默认最小设置,余参数见表1。
1.3 数据处理
SF数据来自实验室检测两次平均值且前后检测变化不大于10%,肝脏、心肌T2*值由受良好培训的医师使用CMRtools和/或结合Excel处理获得。心肌感兴趣区(region of interest,ROI)位于室间隔,肝脏取左右叶实质4~5个ROI (30~50 mm2)且避开伪影及肉眼可见胆管、血管,曲线拟合度要求不小于0.99,取3次平均值。
1.4 体内铁沉积标准参照文献[8-9]及水模实验[5]拟定
心肌(单位:ms):0级(正常):T2*≥10.0,1级(轻度):7.0≤T2*<10.0,2级(中度):5.0≤T2*<7.0,3级(重度):T2*<5.0;肝脏(单位:ms):0级(正常):T2*≥3.57,1级(轻度):1.41≤T2*<3.57,2级(中度):0.70≤T2*<1.41,3级(重度):0.47≤T2*<0.70,4级(极重度):T2*<0.47;血清铁蛋白(单位:μg/L):0级(正常):SF男性≤300、女性≤200,1级(轻度):0级<SF≤1500,2级(中度):1500<SF≤2500,3级(重度):2500<SF≤5000,4级(极重度):SF≥5000。
1.5 统计方法

表1MRI T2*序列扫描参数Tab.1Parameters of MRI T2*protocols
2 结果
117例患者剔除2例严重心率失常,1例不能配合,1例拟合度未达标,共纳入113例,男61例、女52例,年龄(21.6±13.8)岁(5.0~68.0岁),成功率为96.6%(113/117)。其中铁沉积情况:(1)肝脏正常13例,轻度31例,中度29例,重度25例,极重度15例;(2)心肌正常94例,轻度6例,中度10例,重度3例;(3)血清铁蛋白正常1例,轻度48例,中度17例,重度35例,极重度12例。
多回波T2*WI满足定量要求,心肌T2*测量均由CMRtools完成,肝T2*计算由CMRtools完成70例(约61.9%),另外43例需协同Excel测算(约38.1%)。心肌T2*、肝脏T2*、SF中位数分别为21.81(1.88~36.17) ms、1.00(0.36~10.36) ms、1591.0(200.0~14673.0) μg/L,心肌T2*-肝脏T2*(rs=0.267,P=0.004)、心肌T2*-SF (rs=-0.463,P=0.000)、肝脏T2*-SF (rs=-0.641,P=0.000)轻中度相关但无规律性(图1~3)。
心肌T2*<10 ms为标准诊断心铁异常,以肝T2*<0.70 ms、SF>2500 μg/L预测心铁过载准确性分别为0.788和0.833,敏感度分别为80.0%和73.3%,特异性分别为70.4%和63.3%;以肝T2*<3.57 ms诊断肝铁过载,SF>300 μg/L预测肝铁过载准确性为0.719,敏感度为94.0%,特异性为15.4%(图4)。
3 讨论

图1女,17岁,脾切除术后重型β-TM患者,Cardiac T2*=6.67 ms (A),Liver T2*=6.22 ms (B),SF=1479.0 μg/L,提示心铁与肝铁、SF 三间者均不一致图2男,40岁,中间型TM病例,Cardiac T2*=7.38 ms (A),Liver T2*=1.33 ms (B),SF=2566 μg/L,显示心肌与肝铁、SF不平行,肝铁与SF水平相一致Fig. 1A 17-year-old female patient with β-TM major after surgery of spleen, of cardiac T2*(A), liver T2*(B), SF were 6.67 ms, 6.22 ms, 1479.0 μg/L, respectively. No agreements amongst cardiac T2*, liver T2*, SF were found.Fig. 2A 40-year-old male subject with TMinter, of cardiac T2*(A), liver T2*(B), SF were 7.38 ms, 1.33 ms, 2566.0 μg/L, respectively. It demonstrates that no accordance between MIC with LIC, and SF as well, but LIC matches SF.
地中海贫血反复输血患者红细胞被吞噬后,体内产生铁沉积将不可避免地影响肝脏、心脏等功能,其中心力衰竭为患者的致命因素,因此心脏与肝脏体内铁含量精准、早期监测对改善生活品质、提高患者存活期具有重要意义,不仅预防心铁和肝铁过载发生、加剧,还可逆转早期心肌病及早中期肝纤维化。肝脏作为体内储存铁的主要部位[10]已经证实且MRI定量技术也已经被认可为心铁和肝铁沉积诊断的可靠手段[11-12]及心功能评估的金标准[7],可替代穿刺活检以降低创伤、出血、胆瘘等发生率,同时提高准确性、可重复性、受检者耐受性及指导临床去铁治疗[13]。
体内铁定量MRI原理[14]主要是应用自旋或梯度多回波序列采集信号,反映细胞内铁离子、含铁血黄素等顺磁性物质造成质子周围磁环境波动、加速质子失相位,采取一定函数模型计算其时间与信号变化斜率即可获得自旋-自旋弛豫值(T2或T2*),顺磁性物质浓度越大、组织弛豫值越低,根据此原理可重复、无创性测量心铁和肝铁浓度。龙莉玲等[4]证实在一定范围内,使用3.0 T MRI定量肝铁沉积具有可行性,肝铁沉积(liver iron concentration,LIC)与R2(即1/T2)高度相关(r=0.948,P<0.05)。彭鹏等[3,6]以肝铁浓度>15 mg/g预测输血依赖患者心铁沉积准确性为0.771,敏感度为42.2%,特异度为89.7%[3]。而以SF>2500 μg/L或LIC>15 mg/g预测β-重型TM心铁过载准确性分别为0.652和0.775,敏感度分别为90.9%和100%,特异度分别为16.0%和20%[6]。
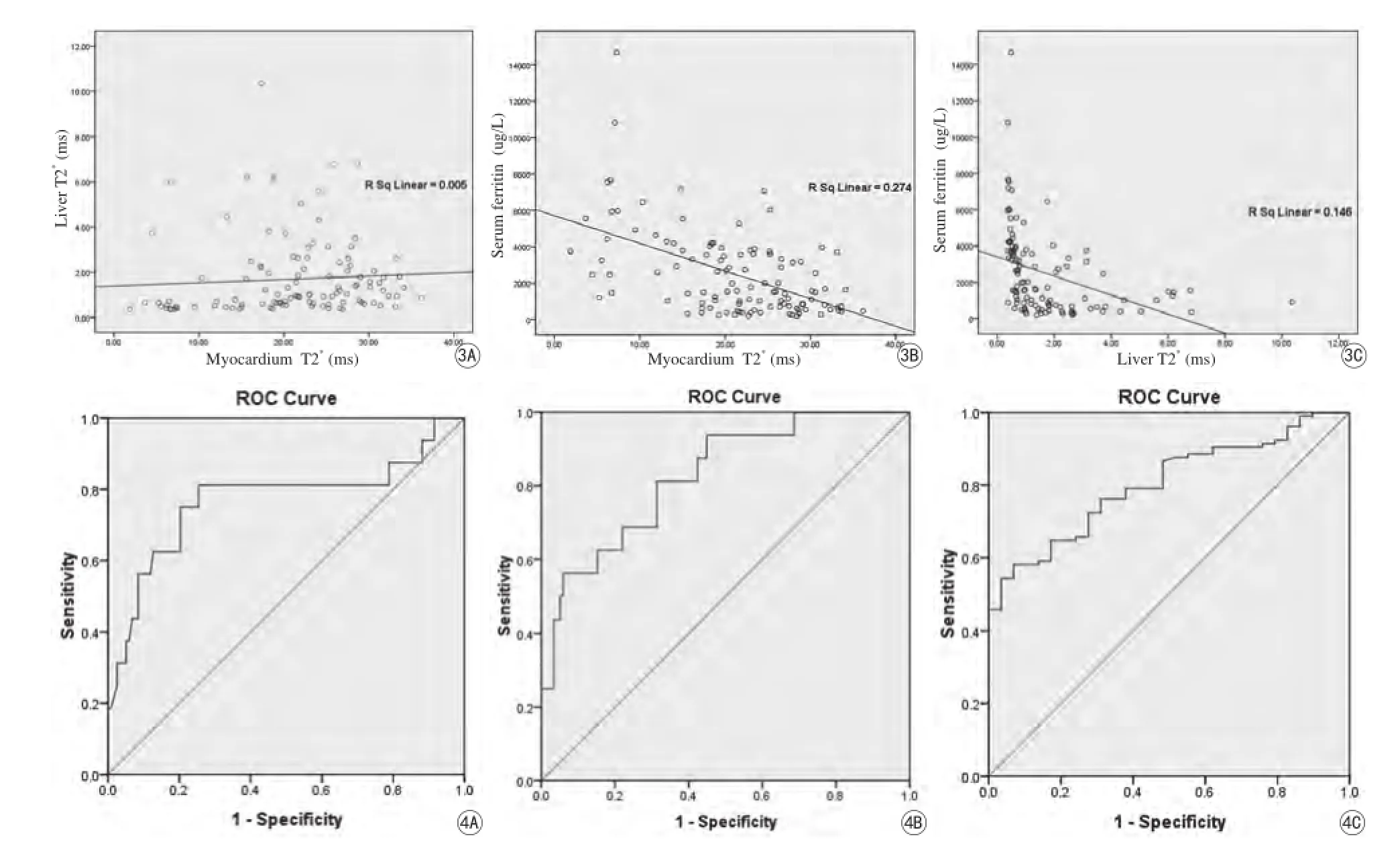
图3113例TM中心肌-肝T2*(A)、心肌T2*-SF (B)、肝脏T2*-SF (C)之间散点图。A:113例TM中心肌-肝T2*散点图,rs=0.267,P=0.004,R2=0.005;B:113例TM中心肌T2*-SF散点图,rs=-0.463,P=0.000,R2=0.274;C:113例TM中肝脏T2*-SF散点图,rs=-0.641,P=0.000,R2=0.146图4ROC图:以肝T2*<0.70 ms (A)、SF>2500 μg/L (B)为界值,肝铁沉积预测心铁过载准确性分别为0.788和0.833,敏感度分别为80.0%和73.3%,特异性分别为70.4%和63.3%;以SF>300 ug/L (C)为阈值,SF预测肝铁过载准确性为0.719,敏感度为94.0%,特异性为15.4%Fig. 3Scatter plots of hepatic T2*(A), SF (B) against cardiac T2*, and SF (C) against hepatic T2*with the linear fit (solid line), for 113 TM patients. A: Scatter plot of cardiac-hepatic T2*for patients, rs=0.267, P=0.004, R sq linear=0.005; B: Scatter plot of cardiac T2*-SF for patients, rs=-0.463, P=0.000, R sq linear=0.274; C: Scatter plot of hepatic T2*-SF for patients, rs=-0.641, P=0.000, R sq linear=0.146.Fig. 4ROC curve: with an area under the ROC curve of liver T2*<0.70 ms (A), SF>2500 μg/L (B) as diagnosis critical points, the sensibilities were 80.0% and 73.3%, the specificities were 70.4% and 63.3%, and the accuracies were 0.788 and 0.833 in the prediction of cardiac excess iron. Moreover, with an area under the ROC curve of SF>300 μg/L (C) as diagnosis critical points, the sensibility was 94.0%, the specificity was 15.4%, the accuracy was 0.719 in the prediction of liver iron deposition.
本研究纳入基因确诊的113例TM被试应用3.0 T MR前瞻性扫描,结果显示,中间型与β-重型TM体内心肌T2*与肝脏T2*、SF均呈轻度相关且无明显规律,以肝脏T2*<0.70 ms、SF>2500 μg/L预测心铁过载准确性分别为0.788和0.833,敏感度分别为80.0%、73.3%,特异性分别为70.4%、63.3%;以SF>300 μg/L预测肝铁过载ROC曲线下面积为0.719,敏感度为94.0%,特异性为15.4%。提示诊断效能中等偏低,敏感性和特异性均难于达到医学定量检测要求,因此笔者认为以肝铁、血清铁蛋白预测心铁或以血清铁蛋白预测肝铁均尚不十分可靠,这些结果与彭鹏等[3,6]报道基本一致,而两者不全相同之处在于笔者应用3.0 T超高场强MR仪并选择基因诊断的113例中间型与β-重型TM受试者进行研究,这是本实验的创新点,后者则以1.5 T设备为基础研究58例反复输血治疗的TM或103例β-重型TM患者。由此可见,不同病例选择可能导致诊断效能不完全一致,因为患者基因分型、输血量和频率、输血开始年龄与时间长短、是否去铁治疗及治疗规律性、有无脾切史等均将影响体内铁严重程度与分布,而对于不同型号、厂商或场强MR扫描仪,肝铁、血清铁蛋白预测心铁过载或血清铁蛋白预测肝铁含量价值尚未达到医学精确影像定量要求(即准确性、敏感度与特异性均超过85%)却可能是相似的,故笔者建议,鉴于MRI已经成为铁定量的最可靠手段,临床上应尽可能采用行之有效的MRI T2*技术定量肝或心铁过载,以替代有创性心肌或肝组织活检减少并发症,避免使用血清铁蛋白预测心铁或肝铁含量和心功能变化,同时也不应该以肝铁来预测心铁或心功能,此外,在疗效评估和要求反复检测时MRI T2*技术也可发挥积极作用。
实验数据收集还发现,TM被试铁过载严重64例仅凭CMRtools计算难于获得准确结果,此时还须结合Excel测算肝脏T2*,证明超高场强MR仪对少量铁检出敏感的同时存在低估严重病例铁含量的缺陷,这是铁沉积超高强场实际应用需要提醒的注意事项。对于问题的解决方法,研究中依据T2WI和T1WI预判肝铁过载程度,正常和轻中度异常者应用TEmin/max(ms)=1.3/16.8、黑肝现象明显病例(提示含铁量高)则采用TEmin/max(ms)=0.6/7.8序列扫描,在处理中如发现CMRtools曲线拟合未达0.99时协同Excel测量即可,此亦为研究创新发现之处。黄海波等[5]报道认为,3.0 T MR优化首回波T2*序列可显著增加定量扫描准确度,根据Wood等[15]报告,一般组织可测量最小T2值大约为最短TE的5/7即越小首回波值可检测更大铁浓度阈值。
需要指出的是,业内标准肝脏和心肌T2*参考值目前均基于1.5 T扫描获得[8-9],而广泛认可的3.0 T铁过载标准尚未确定,故此实验心铁分度初定约为1.5 T参考值的1/2,肝铁沉积则依据本中心M R扫描仪水模实验结果即PhC=7.008R2*+0.036[5],这也是此次研究将肝T2*直接代表铁浓度而未转换为LIC的重要原因。
综上所述,实验被试体内心肌T2*与肝脏T2*、SF均呈轻度相关且无明显规律,临床上以肝铁、血清铁蛋白预测心铁或以血清铁蛋白预测肝铁均尚不十分可靠、诊断效能中等偏低。研究不足之处及展望:MR可直接精确定量心肌、肝脏铁沉积,但以下因素将对结果产生影响:言语不理解、呼吸不配合、严重心律失常等,同时严重肝铁扫描CMRtools计算肝T2*不准确。此外,幽闭恐怖、神经刺激、金属置入等导致技术应用受限,受最小回波限制与磁敏感影响,3.0 T铁含量阈值小于1.5 T机型。但随着软硬件性能提高,这些因素当可逐步解决,MRI精确铁定量与疗效评定将迎来新的高度并为科研和临床提供更可信的依据。
[References]
[1] Zhang ZN, Sheng D. Diagnositc and effect-therapying criteria of hematopathy (Ver.3). Beijing: Science Press, 2007: 29-34.张之南, 沈悌. 血液病诊断与疗效标准. 3版. 北京: 科学出版社, 2007: 29-34.
[2] Lekawanvijit S, Chattipakorn N. Iron overload thalassemiccardiomyopathy: iron status assessment and mechanisms of mechanical and electrical disturbance due to iron toxicity. Can J Cardiol, 2009, 25(4): 213-218.
[3] Peng P, Huang ZK, Long LL, et al. The relationship between heart and liver iron in thalassemia: A quantitative analysis using MRI. Zhonghua Fang She Xue Za Zhi, 2012, 46(3): 244-247.彭鹏, 黄仲奎, 龙莉玲, 等. 地中海贫血患者心脏、肝脏铁沉积的MRI定量研究. 中华放射学杂志, 2012, 46(3): 244-247.
[4] Long LL, Peng P, Huang ZK, et al. Liver iron quantification by 3.0 T MRI: calibration on a rabbit model. Chin J Magn Reson Imaging, 2012, 3(6): 451-455.龙莉玲, 彭鹏, 黄仲奎, 等. 铁超负荷模型3.0 T MRI定量肝铁沉积可行性研究. 磁共振成像, 2012, 3(6): 451-455.
[5] Huang HB, Zhou YL, Li ZZ, et al. Feasibility of multiple-echo GRE with parameters optimized protocol at 3.0 T MRI. Chin J Magn Reson Imaging, 2015, 6(7): 529-534.黄海波, 周亚丽, 李致忠, 等. 前瞻性3.0 T MRI梯度多回波序列参数优化可行性研究. 磁共振成像, 2015, 6(7): 529-534.
[6] Peng P, Long LL, Huang ZK, et al. Correlation study between MR quantitative cardiac iron accumulated and serum ferritin, liver iron concentration in patients with β-thalassemiamajor. Zhonghua Fang She Xue Za Zhi, 2012, 46(11): 993-997.彭鹏, 龙莉玲, 黄仲奎, 等. β-重型地中海贫血MR定量心脏铁沉积与血清铁蛋白、肝铁浓度相关性研究. 中华放射学杂志, 2012, 46(11): 993-997.
[7] Chen XY, Zhao SH. Progress and clinical application of cardiovascular magnetic resonance. Chin J Magn Reson Imaging, 2015, 6(2): 86-89.陈秀玉, 赵世华. 心血管磁共振临床应用及进展. 磁共振成像, 2015, 6(2): 86-89.
[8] Kerk P, Roughton M, Porter JB, et al. Cardiac T2*magnetic resonance for predication of cardiac complications in thalassemia magor. Circulation, 2009, 120(20): 1961-1968.
[9] Fischer R, Harmatz PR. Non-invasive assessment of tissue iron overload. Hematology, 2009, 1(1): 215-221.
[10] Liu SX, Wang Y, Li CG, et al. A multiple-center clinical study on quantitative T2*magnetic resonance imaging of iron deposition of liver, pancreas and heart of beta-thalassemia major patients. Chin J Prac Pediatrics, 2014, 29(11): 845-848.刘四喜, 王缨, 李长钢, 等. 重型β地中海贫血患者肝脏、胰腺和心脏铁负荷磁共振成像T2*的多中心研究. 中华实用儿科杂志, 2014, 29(11): 845-848.
[11] Zhang Q, Hou B, Wang L, et al. Significance of magnetic resonance imaging in the detection of iron overload. Natl Med J China, 2013, 93(44): 3506-3509.张倩, 侯波, 王璐, 等. 磁共振成像技术定量检测铁过载的临床意义. 中华医学杂志, 2013, 93(44): 3506-3509.
[12] Aessopos A, Fragdimitri C, Karabatsos F, et al. Cardiac magnetic resonance Imaging R2*assessmentsand analysis of historical parameters in patients with transfusion- dependent thalassemia. Haemetologica, 2007, 92(1): 131-132.
[13] Meloni A, Positano V, Ruffo GB, et al. Improvement of heart iron with preserved patterns of iron store by CMR-guided chelation therapy. Eur Heart J Cardiovasc Imaging, 2015, 16(3): 325-334.
[14] Yang ZH, Feng F, Wang XY. A guide to technique of magnetic resonance imaging. Beijing: People's Military Medical Press, 2014: 303.杨正汉, 冯逢, 王霄英. 磁共振成像技术指南. 北京: 人民军医出版社, 2014: 303.
[15] Wood JC, Ghugre N. Magnetic resonance imaging assessment of excess iron in thalassemia, sickle cell disease and others iron overload diseases. Hemoglobin, 2008, 32(1-2): 85-96.
Value of liver T2*and SF to predict myocardial iron concentration patients with thalassemia
LI Da-chuang1, HUANG Hai-bo1*, YIN Xiao-lin2, ZHOU Ya-li2, GUAN Jun1, QIN Ming1, HUANG Gui-xiong1
1Department of Medical Imaging, 303rdHospital of PLA, Nanning 530021, China
2Department of Haematology, 303rdHospital of PLA, Nanning 530021, China
ACKNOWLEDGMENTSThis work was part of Guangxi Natural Science Foundation of China (No. 2014GXNSFBA118187, 2015GXNSFAA139164).
Objective:To quantify the MIC, liver iron concentration (LIC) in TM patients and discuss the value of liver T2*, SF to predict the MIC.Materials and Methods:Study protocol was approved by local ethics committee; informed consent was obtained. A total of 113 TM patients diagnosed by gene were enrolled. A multiple fast-field echo (mFFE) within a single breath-hold was performed using a 3.0 Tesla MR unit to acquire 8 or 12 T2*weighted images in the heart or liver. T2*values of myocardium and liver were quantified based on mFFE T2*protocol by a well-trained physician respectively, SF was obtained twice within 7 days before and after MRI. Spearman rank correlation was applied to analyze the relationships among the MIC, LIC and SF. The ROC curve was drawn to predict the possibility of using liver T2*<0.70 ms, SF>2500 μg/L as an index of cardiac iron deposition, and the possibility of using SF>300 μg/L as an index of liver iron overload.Results:A total of 113 patients, the grades of body iron deposition as following: nineteen out of 113 were found to have myocardial excess iron, including 3 severe cases, 10 moderate cases, and 6 mildcases; 100 out of 113 were found to be liver excess iron, including 15 very severe cases, 25 severe cases, 29 moderate cases, and 31 mild cases; 112 out of 113 patients were found to be abnormal SF, including 12 very severe cases, 35 severe cases, 17 moderate cases, and 48 mild cases. There was weakly or moderate correlation between myocardial T2*and liver T2*(rs=0.267, P=0.004), myocardial T2*and SF (rs=-0.463, P=0.000), as well as between liver T2*and SF (rs=-0.641, P=0.000), but no clear regularity. To predict cardiac iron deposition with myocardial T2*<10 ms as diagnostic criteria, the accuracies, sensibilities and specificities were 76.9%, 75% and 77.1% for the index of liver T2*<0.70 ms, 82.7%, 68.8% and 68.6% for SF>2500 μg/L, respectively. Moreover, to predict liver excess iron with liver T2*<3.57 ms as standard setting, the accuracy, sensibility and specificity were respectively 80.2%, 92.4% and 20.7% for the index of SF>2500 μg/L.Conclusion:Within a certain limits, MRI T2*technique could directly quantify the MIC and LIC, there was weakly or moderate correlation among MIC, LIC and SF, but no clear regularity. Using LIC or SF as an indirect index to predict cardiac excess iron were low valuable, meanwhile, using SF to predict liver iron overload was not reliable in clinical.
Thalassemia; Magnetic resonance imaging; Serum ferritin; Myocardium; Iron overload
Huang HB, E-mail:jackie000528@163.com
Received 9 Sep 2016, Accepted 26 Oct 2016
广西壮族自治区自然科学基金(编号:2014 GXNSFBA118187,2015GXNSFAA139164)
1.解放军第303医院医学影像科,南宁530021
2.解放军第303医院血液科,南宁530021
黄海波,Email:Jackie000528@163. com
2016-09-09
接受日期:2016-10-26
R445.2;R556.6
A
10.12015/issn.1674-8034.2016.12.004
李大创, 黄海波, 尹晓林, 等. 地中海贫血患者肝脏T2*、血清铁蛋白预测心肌铁过载价值研究. 磁共振成像, 2016, 7(12): 909-914.*
猜你喜欢
科学(2022年4期)2022-10-25
世界科学技术-中医药现代化(2020年2期)2020-07-25
沉积与特提斯地质(2019年1期)2019-07-16
中成药(2018年12期)2018-12-29
中成药(2017年6期)2017-06-13
南方文学(2016年4期)2016-06-12
物理化学学报(2015年7期)2015-12-30
中国塑料(2015年11期)2015-10-14
医学研究杂志(2015年4期)2015-06-10
天津科技大学学报(2015年3期)2015-04-16