
不同性别高血压患者脉搏波传导速度影响因素研究*
2016-05-07 02:35:54张鑫洪必莹陈晓平施迪
西部医学 2016年3期
张鑫 洪必莹 陈晓平 施迪
不同性别高血压患者脉搏波传导速度影响因素研究*
张鑫 洪必莹 陈晓平 施迪
(四川大学华西医院心血管内科, 四川 成都 610041)
目的 探讨不同性别、新诊断、未接受药物治疗的原发性高血压患者脉搏波传导速度的影响因素。 方法 本研究为一项横断面研究,收集新诊断、未接受治疗的高血压患者,以性别分成两组,分别采集患者年龄、收缩压、血糖、糖化血红蛋白、尿酸、肌酐、微量蛋白尿、醛固酮、肾素、血管紧张素、颈-股动脉脉搏波传导速度(cfPWV)、颈动脉内中膜厚度。分析不同性别中上述指标与cfPWV增加的关系。结果 对所有可能引起高血压患者cfPWV增加的因素进行多元线性回归分析,发现纳入研究的所有高血压患者中年龄(t=2.296,P=0.027)和收缩压(t=2.45,P=0.018)是cfPWV增高的危险因素;男性患者中年龄(t=2.519,P=0.018)和收缩压(t=2.34,P=0.035)是cfPWV增高的危险因素,女性患者中发现年龄(t=3.536,P=0.002)、收缩压(t=2.103,P=0.042)、血尿酸水平(t=0.925,P=0.035)是cfPWV增高的危险因素。结论 除年龄、收缩压外,血尿酸是女性高血压患者cfPWV增加的危险因素,在纳入研究的男性高血压患者中血尿酸不是cfPWV增高的危险因素。
高血压; 颈-股动脉脉搏波传导速度(cfPwv); 尿酸; 女性
心血管疾病目前仍是最主要的死因之一。报道显示,心血管疾病所致死亡女性高于男性[1]。越来越多的证据显示,男性与女性之间在心血管疾病的病因、临床表现、预后方面均存在差异[2]。目前证实动脉硬化是心血管疾病、卒中、认知功能障碍的独立预测因子,动脉硬化与远期心血管事件、靶器官损害、死亡率明显相关,已成为心血管领域一个重要的标记[3~8]。因此,探索男女在动脉硬化发生发展方面是否存在一定差异势在必行。用于判定动脉硬化的指标是脉搏波传导速度,其作为一种无创性血管硬化检查指标,近年来在高血压病患者所致的心血管事件发病率及死亡率的预测评估方面得到了越来越广泛的重视。其中颈-股动脉脉搏波传导速度是测量动脉硬化的金标准[9]。本研究着重探讨了不同性别高血压患者中可能引起动脉硬化的指标与颈-股动脉脉搏波传导速度(cfPWV)的关系。
1 材料与方法
1.1 一般资料 选择2012年10月~2014年1月到四川大学华西医院心内科住院新诊断的高血压病患者为研究对象,高血压诊断满足两次测量的平均血压值收缩压≥140 mmHg和(或)舒张压≥90 mmHg或正在服用降压药物者。患者合并下列情况予以排除:①合并糖尿病患者。②近30天内服用过他汀类药物、抗血小板药物、β受体阻滞剂、ACEI、ARB及螺旋内酯。③动脉粥样硬化血管疾病患者。④慢性肾脏病患者(eGFR<60ml/min/1.73m2)。⑤中重度心脏疾病(既往有冠心病病史或NYHA心功能Ⅱ~Ⅳ级)。⑥踝臂指数(ABI)<0.9(提示外周动脉疾病)。⑦继发性高血压。⑧严重心肺功能异常。所有入组患者均签署知情同意书。
1.2 人口学资料和体格检查 通过问卷调查方式获得患者年龄、性别、既往病史、高血压病史及用药史,吸烟、饮酒史等资料。用标准天平秤测量体重,单位为千克。用有刻度的标尺测量身高。BMI通过体重/身高2计算获得。腰围测量在肚脐以上1cm的水平面上进行,皮尺直接接触皮肤,每次吸气末读数并记录测量值(精确到1cm)。血压测量规定在采血前测量,测量前至少静坐5min后,双足着地,使用标准水银血压计测坐位右上臂血压。每位入组患者测量2 次血压值,取其均值作为个体血压值,如任意相邻两次测量结果,SBP相差在8mmHg以上,或DBP在4mmHg以上,应增加测量次数,取3次数值相差在8/4mmHg以内的结果,计算平均值。心率测量要求休息5分钟以上,通过心电图检查获得平静状态下1分钟的心率。
1.3 血标本的收集及检测 所有血标本检查都在四川大学华西医院检验科完成,血标本获取都在早晨7点到8点之间,空腹12小时状态下抽取。我院检验科采用Hitachi7600全自动生化测定仪完成血脂、血糖及肝肾功能等生化指标测定。采用科迈瑞BC-5300/5380五分类血细胞分析仪完成血常规的测定。血浆醛固酮及肾素、血管紧张素Ⅱ水平的测定均取卧位测量。入组患者平卧过夜,清晨8点卧位空腹采肘静脉血2ml,肝素抗凝,离心分离,去上清液,迅速送至我院检验科测定,具体采用放射免疫分析法测定样本中肾素、血管紧张素-Ⅱ和醛固酮水平。
1.4 脉搏波传导速度测定 本试验使用Sphygmo Cor(AtCor Medicine,Sydney,Australia)脉搏波分析仪测量颈-股动脉脉搏波传导速度(cfPWV),具体测定是通过测量颈-股动脉节段的体表距离(L)和脉搏波传导时间(t)求得,计算公式为:PWV(m/s)=L/t,PWV常测定10个连续搏动,取其平均值。入组患者颈动脉内中膜厚度测量由本院超声科专业超声医师完成,为保证结果的可靠性,减少系统误差,所有患者颈动脉彩超检查均由同一个超声医师完成。

2 结果
2.1 研究人群基线特点 纳入研究的117例高血压患者均满足高血压的诊断标准,均为新诊断并未接受治疗者。其中男性高血压患者67例,平均年龄(46.75±17.90)岁,女性高血压患者50例,平均年龄(47.81±15.79)岁。两组间年龄、空腹血糖、甘油三脂、胆固醇、微量蛋白尿、hs-CRP、肾素-血管紧张素-醛固酮、脉搏波传导速度、颈动脉内中膜厚度等指标无明显统计学差异(P>0.05)。男女性患者间体重指数(BMI)、尿酸存在统计学差异(P<0.05),见表1。

表1 男女高血压患者基线数据±s)
注:Age:年龄;BMI:体重指数;SBP:收缩压;DBP:舒张压; HR:心率;cfPWV:颈股动脉脉搏波传导速度;FBG:空腹血糖;UA:尿酸;Cr:肌酐; TG:甘油三酯;TC:总胆固醇;LDL-C:低密度脂蛋白胆固醇;HDL-C:高密度脂蛋白胆固醇;ALD:醛固酮;ATⅡ;血管紧张素Ⅱ;PRA:血浆肾素活性;ARR:醛固酮血浆肾素活性比;IMT:内中膜厚度;hs-CRP:高敏C反应蛋白;HbA1c:糖化血红蛋白;MAU:尿微量白蛋白;①P<0.05
2.2 男女高血压患者各自cfPWV与各临床指标的相关性分析 男性高血压患者的cfPWV主要与年龄(R=0.357,P=0.003)、平均收缩压(R=0.331,P=0.005)、卧位醛固酮水平(R=0.284,P=0.02)及糖化血红蛋白(R=0.281,P=0.021)相关,与体重指数、脉压、肌酐及尿微量白蛋白等水平无关(均P>0.05)。与男性高血压患者不同,女性高血压患者的cfPWV主要与年龄(R=0.582,P<0.001)、平均收缩压(R=0.360,P=0.031)、尿酸(R=0.399,P=0.024)、肌酐水平(R=0.461,P=0.012)相关,而与体重指数、血脂、血糖及糖化血红蛋白等指标无明显相关性,见表2。
表2 男女高血压患者各自cfPWV与各临床指标的相关性分析
Table 2 Analysis of the correlation between cfPWV and clinical indicators in patients with hypertension
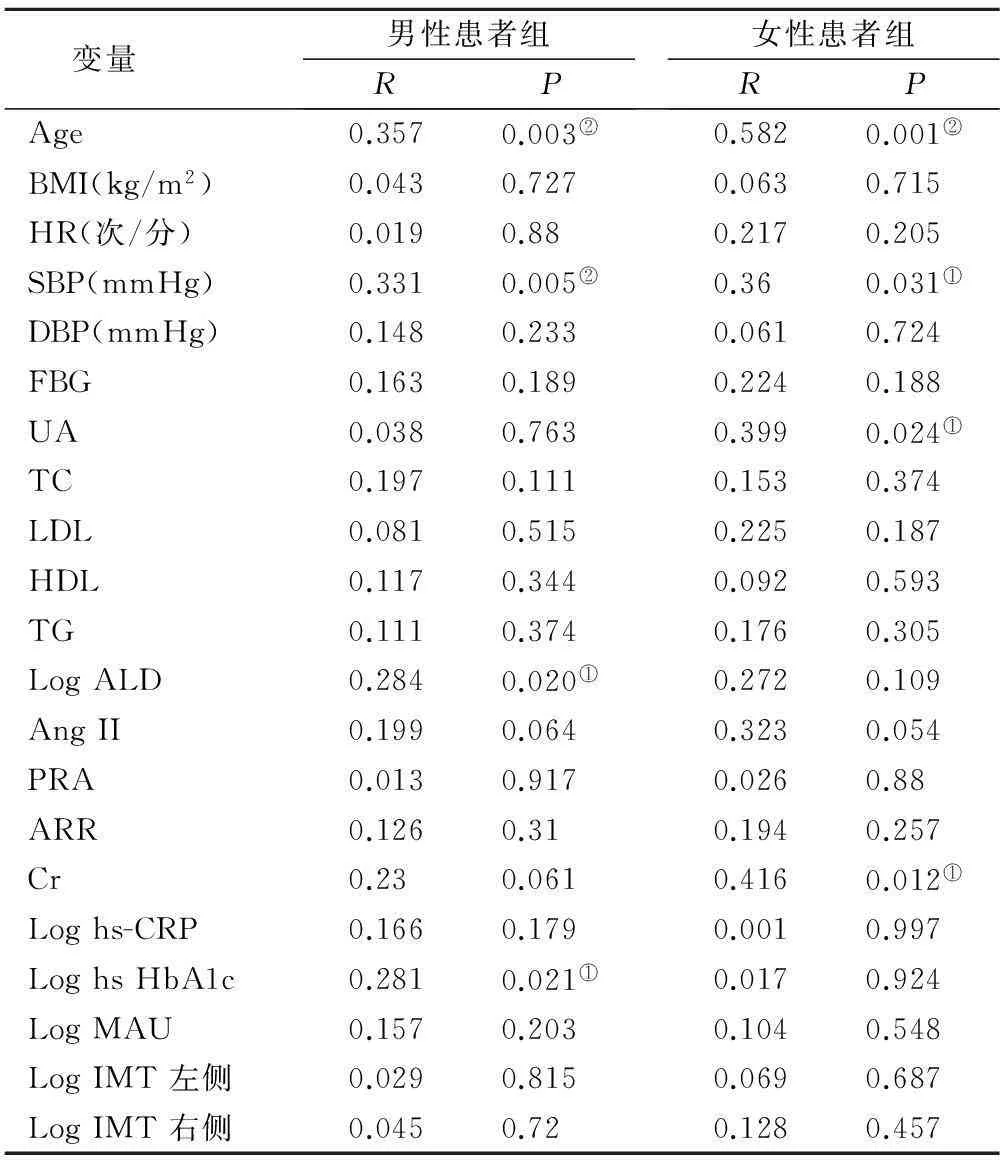
变量男性患者组RP女性患者组RPAge0.3570.003②0.5820.001②BMI(kg/m2)0.0430.7270.0630.715HR(次/分)0.0190.880.2170.205SBP(mmHg)0.3310.005②0.360.031①DBP(mmHg)0.1480.2330.0610.724FBG0.1630.1890.2240.188UA0.0380.7630.3990.024①TC0.1970.1110.1530.374LDL0.0810.5150.2250.187HDL0.1170.3440.0920.593TG0.1110.3740.1760.305LogALD0.2840.020①0.2720.109AngII0.1990.0640.3230.054PRA0.0130.9170.0260.88ARR0.1260.310.1940.257Cr0.230.0610.4160.012①Loghs-CRP0.1660.1790.0010.997LoghsHbA1c0.2810.021①0.0170.924LogMAU0.1570.2030.1040.548LogIMT左侧0.0290.8150.0690.687LogIMT右侧0.0450.720.1280.457
注:①P<0.05;②P<0.01
2.3 男女高血压人群各自cfPWV危险因素的多元线性回归分析 对所有可能和高血压患者cfPWV相关的因素(包括年龄、体重指数、平均收缩压、卧位醛固酮水平、肌酐、尿微量白蛋白、糖化血红蛋白)进行多元线性回归分析显示,年龄和平均收缩压是高血压患者cfPWV的危险因素(均P<0.05)。年龄、平均收缩压、血尿酸为女性高血压患者cfPWV的危险因素(均P<0.05),见表3。
3 讨论
动脉硬化与心血管危险因素密切相关,被认为是总死亡率、心血管死亡率、心血管疾病及致死或非致死性冠脉事件的独立预测因子之一。目前被证实动脉硬化与年龄、糖尿病、高脂血症、吸烟等危险因素密切相关。心血管疾病的病因、病理学、临床表现及预后在不同性别存在差异。因此,探讨不同性别高血压患者在动脉硬化的影响因素方面是否存在差异,对动脉硬化的防治及降低患者心血管死亡风险具有重要意义。
表3 男女高血压患者各自cfPWV与各临床指标的多元线性回归分析
Table 3 Multivariate linear regression analysis of cfPWV and clinical indicators in patients with hypertension

变量男性患者组tP女性患者组tP总体tPAge2.5190.015①3.5360.002②2.2960.027①SBP2.340.035①2.1030.042①2.450.018①LogALD1.5480.1190.160.8740.490.626Cr0.1380.8911.9890.0570.7490.458LogMAU0.610.5441.5780.1271.3020.308LogHbA1c1.4660.0620.4570.6521.8110.077BMI0.8340.4080.0170.8960.310.758UA1.1230.4160.9250.035①1.0280.626
注:①P<0.05,②P<0.01
3.1 总体高血压患者脉搏波传导速度的影响因素分析 已被证实的高血压人群中影响PWV的因素仅有血压和年龄两个因素,我们的研究中经过对所有纳入研究的高血压对象,对cfPWV的可能影响因素进行多元线性回归分析,也再次证实了在高血压患者及男性患者中影响脉搏波传导速度的指标只有年龄和收缩压水平。而女性患者除了年龄、收缩压外,cfPWV还与血尿酸水平相关。
3.2 女性高血压患者脉搏波传导速度的影响因素分析 女性高血压患者cfPWV增加的危险因素有年龄、收缩压、血尿酸,其中年龄、收缩压已在既往的研究中得以证实。关于血尿酸与cfPWV的相关研究如下,lin纳入福建省某少数民族,年龄在20~79岁的群体研究中发现,血尿酸水平在男性及女性群体均与baPWV密切相关[10]。Liang在一项3772例中国人群中发现,独立于传统心血管危险因素外,血尿酸水平和动脉僵硬度增加存在剂量依赖相关关系[11]。Vlachopoulos在基于新诊断、未接受治疗的高血压患者研究中发现,cfPWV和血尿酸水平相关[12]。我们对可能引起高血压患者动脉僵硬度增加的因素进行多元线性回归发现,在女性患者中除既往研究已证实的年龄及收缩压外,血尿酸水平与cfPWV存在相关。研究结果提示了血清尿酸参与了动脉硬化、动脉损伤的过程。血尿酸与动脉硬化之间的关系可能有下列机制参与:血尿酸升高会刺激肾脏血管收缩,激活肾素-血管紧张素系统。既往研究证实了肾素、血管紧张素、醛固酮与动脉僵硬度相关[11, 13, 14],其中醛固酮影响血管硬化的可能机制,目前认为是过量的醛固酮激素损伤血管内皮功能,引起血管炎症及心肌纤维化[15, 16];高尿酸可以减少内皮细胞产生一氧化氮,从而导致内皮细胞功能障碍及降低血流介导的血管扩张功能[17~19];血尿酸可以促进血管平滑肌细胞增殖,并促进血小板源生长因子及单核细胞趋化蛋白-1的表达,从而引起血管损伤[20~22];尿酸代谢涉及黄嘌呤脱氢酶/黄嘌呤氧化酶的参与,会伴随产生超过氧化物、活性氧自由基,导致血管收缩及血管损伤[23~25]。此外,血尿酸还可以通过血小板激活而引发的血栓效应,促进低密度脂蛋白的过氧化[26],进而激活炎症通路等机制介导血管硬化[17, 27]。
3.3 男性高血压患者脉搏波传导速度的影响因素分析 在本研究中我们发现,血尿酸与cfPWV仅在女性患者中存在相关关系,而在男性患者并未发现上述关系。并且在本研究纳入的男性患者中,经过对所有因素多元线性回归仅发现年龄和收缩压是cfPWV增高的危险因素。这种血尿酸在不同性别所致的血管损害差异提示女性患者对尿酸所致的器官损害更为敏感。Ishizaka报道了在日本人群中PWV和血尿酸水平正相关,在不同性别之间以血尿酸四分位分组探讨与BaPWV的关系,并调整年龄、血脂、体重指数、收缩压、甘油三脂、血糖及是否吸烟等因素后,发现女性患者在相同血尿酸四分位水平时发生BaPWV增高的风险越大[28]。Fang在台湾某大学附属医院的健康体检中心调查血尿酸水平和动脉硬化中发现,仅在女性研究对象中发现正常高限尿酸水平与BaPWV相关[29]。尿酸水平在不同性别所造成的血管损害差异的研究还包括:尿酸与沉默性脑梗死风险及尿酸与颈动脉阻力指数研究[30, 31]。一项长达23年的随访显示,特别在女性患者中,血尿酸水平增高与较早的心血管死亡相关[32]。这种尿酸在心血管损害上的性别差异其具体机制目前尚不清楚。全基因组学研究显示,尿酸代谢受基因控制,推测尿酸所致器官损害的性别差异可能由基因差异造成[33]。这种差异或许是由于性激素的不同造成,雌激素有促尿酸排泄的效应,研究证实停经后由于雌激素降低,会伴随出现血尿酸水平升高。药物干预实验发现以性激素替代疗法会降低绝经期妇女的血尿酸[34, 35]。总的来说,关于性别在尿酸所致的血管损害机制尚不明确,还需要更多的临床试验或基础研究来探讨。
4 结论
在高血压患者中,年龄、收缩压是cfPWV增加的危险因素,而在女性高血压患者中血尿酸水平也是cfPWV增加的危险因素,在纳入研究的男性高血压患者中血尿酸不是cfPWV增高的危险因素。说明血尿酸或许参与了女性高血压患者的动脉硬化过程。
[1]Charakida M, Masi S, Deanfield JE. The Year in Cardiology 2012: focus on cardiovascular disease prevention[J]. European heart journal, 2013, 34(4):314-317.
[2]Mitchell GF, Guo CY, Benjamin EJ,etal. Cross-sectional correlates of increased aortic stiffness in the community: the Framingham Heart Study[J]. Circulation, 2007, 115(20):2628-2636.
[3]Mitchell GF, Hwang SJ, Vasan RS,etal. Arterial stiffness and cardiovascular events: the Framingham Heart Study[J]. Circulation, 2010, 121(4):505-511.
[4]Mattace-Raso FU, van der Cammen TJ, Hofman A,etal. Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam Study[J]. Circulation, 2006, 113(5):657-663.
[5]Vlachopoulos C, Aznaouridis K, O’Rourke MF,etal. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: a systematic review and meta-analysis[J]. European heart journal, 2010, 31(15):1865-1871.
[6]Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis[J]. Journal of the American College of Cardiology, 2010, 55(13):1318-1327.
[7]Coutinho T, Turner ST, Kullo IJ. Aortic pulse wave velocity is associated with measures of subclinical target organ damage[J]. JACC Cardiovascular imaging, 2011, 4(7):754-761.
[8]Blacher J, Pannier B, Guerin AP,etal. Carotid arterial stiffness as a predictor of cardiovascular and all-cause mortality in end-stage renal disease[J]. Hypertension, 1998, 32(3):570-574.
[9]Lehmann ED. Clinical value of aortic pulse-wave velocity measurement[J]. Lancet, 1999, 354(9178):528-529.
[10] Lin Y, Lai X, Chen G,etal. Association among serum uric acid, cardiovascular risk, and arterial stiffness: a cross-sectional study in She ethnic minority group of Fujian Province in China[J]. Journal of endocrinological investigation, 2012, 35(3):290-297.
[11] Liang J, Li Y, Zhou N,etal. Synergistic effects of serum uric acid and cardiometabolic risk factors on early stage atherosclerosis: the cardiometabolic risk in Chinese study[J]. PloS one, 2012, 7(12):e51101.
[12] Vlachopoulos C, Xaplanteris P, Vyssoulis G,etal. Association of serum uric acid level with aortic stiffness and arterial wave reflections in newly diagnosed, never-treated hypertension[J]. American journal of hypertension, 2011, 24(1):33-39.
[13] Sulikowska B, Johnson RJ, Odrowaz-Sypniewska G,etal. Uric acid, renal vasoconstriction and erythropoietin relationship in IgA nephropathy revealed by dopamine-induced glomerular filtration response[J]. Kidney & blood pressure research, 2012, 35(3):161-166.
[14] Park S, Kim JB, Shim CY,etal. The influence of serum aldosterone and the aldosterone-renin ratio on pulse wave velocity in hypertensive patients[J]. Journal of hypertension, 2007, 25(6):1279-1283.
[15] Schmidt BM, Schmieder RE. Aldosterone-induced cardiac damage: focus on blood pressure independent effects[J]. American journal of hypertension, 2003, 16(1):80-86.
[16] Duprez DA. Role of the renin-angiotensin-aldosterone system in vascular remodeling and inflammation: a clinical review[J]. Journal of hypertension, 2006, 24(6):983-991.
[17] Khosla UM, Zharikov S, Finch JL,etal. Hyperuricemia induces endothelial dysfunction[J]. Kidney international, 2005, 67(5):1739-1742.
[18] Tsai WC, Huang YY, Lin CC,etal. Uric acid is an independent predictor of arterial stiffness in hypertensive patients[J]. Heart and vessels, 2009, 24(5):371-375.
[19] Choi YJ, Yoon Y, Lee KY,etal. Uric acid induces endothelial dysfunction by vascular insulin resistance associated with the impairment of nitric oxide synthesis[J]. FASEB journal: official publication of the Federation of American Societies for Experimental Biology, 2014, 28(7):3197-3204.
[20] 张艳,刘露.高血压患者血浆 Hcy与颈动脉粥样硬化的关系分析[J].陕西医学杂志,2013,42(12):1592-1593.
[21] Corry DB, Eslami P, Yamamoto K,etal. Uric acid stimulates vascular smooth muscle cell proliferation and oxidative stress via the vascular renin-angiotensin system[J]. Journal of hypertension, 2008, 26(2):269-275.
[22] Kanellis J, Watanabe S, Li JH,etal. Uric acid stimulates monocyte chemoattractant protein-1 production in vascular smooth muscle cells via mitogen-activated protein kinase and cyclooxygenase-2[J]. Hypertension, 2003, 41(6):1287-1293.
[23] Many A, Hubel CA, Roberts JM. Hyperuricemia and xanthine oxidase in preeclampsia, revisited[J]. American journal of obstetrics and gynecology, 1996, 174(1 Pt 1):288-291.
[24] White CR, Brock TA, Chang LY,etal. Superoxide and peroxynitrite in atherosclerosis[J]. Proceedings of the National Academy of Sciences of the United States of America, 1994, 91(3):1044-1048.
[25] Vara D, Pula G. Reactive oxygen species: physiological roles in the regulation of vascular cells[J]. Current molecular medicine, 2014, 14(9):1103-1125.
[26] Schlotte V, Sevanian A, Hochstein P,etal. Effect of uric acid and chemical analogues on oxidation of human low density lipoprotein in vitro[J]. Free radical biology & medicine, 1998, 25(7):839-847.
[27] Karbowska A, Boratynska M, Kusztal M,etal. Hyperuricemia is a mediator of endothelial dysfunction and inflammation in renal allograft recipients[J]. Transplantation proceedings, 2009, 41(8):3052-3055.
[28] Ishizaka N, Ishizaka Y, Toda E,etal. Higher serum uric acid is associated with increased arterial stiffness in Japanese individuals[J]. Atherosclerosis, 2007, 192(1):131-137.
[29] Fang JI, Wu JS, Yang YC,etal. High uric acid level associated with increased arterial stiffness in apparently healthy women[J]. Atherosclerosis, 2014, 236(2):389-393.
[30] Heo SH, Lee SH. High levels of serum uric acid are associated with silent brain infarction[J]. Journal of the neurological sciences, 2010, 297(1-2):6-10.
[31] Cipolli JA, Ferreira-Sae MC, Martins RP,etal. Relationship between serum uric acid and internal carotid resistive index in hypertensive women: a cross-sectional study[J]. BMC cardiovascular disorders, 2012, 12:52.
[32] Juraschek SP, Tunstall-Pedoe H, Woodward M. Serum uric acid and the risk of mortality during 23 years follow-up in the Scottish Heart Health Extended Cohort Study[J]. Atherosclerosis, 2014, 233(2):623-629.
[33] Kolz M, Johnson T, Sanna S,etal. Meta-analysis of 28,141 individuals identifies common variants within five new loci that influence uric acid concentrations[J]. PLoS genetics, 2009, 5(6):e1000504.
[34] 李军,石理,陈曦,等.ET技术监测非洛地平对高血压患者动脉弹性功能变化的研究[J].西部医学,2010,22(12):2207-2209.DOI:10.3969/j.issn.1672-3511.2010.12.007.
[35] Wiacek M, Zubrzycki IZ, Bojke O,etal. Menopause and age-driven changes in blood level of fat- and water-soluble vitamins[J]. Climacteric: the journal of the International Menopause Society, 2013, 16(6):689-699.
欢迎订阅2016年《西部医学》杂志,《西部医学》为月刊,全铜版纸印刷,全年一套(12期)180元。国内订阅可在当地邮局订购,国内邮发代号:62-243;海外发行代号:BM 2902;也可汇款或转账到编辑部订购,本刊编辑部随时接受订购、补订、增订业务。联系电话:028-85570072/85588403。
Impact factors of pulse wave velocity in hypertensive patients of different genders
ZHANG Xin,HONG Biyin,CHEN Xiaoping,etal
(DepartmentofCardiology,WestChinaHospital,SichuanUniversity,Chengdu610041,China)
Objective To observe different impact factors of pulse wave velocity in newly diagnosed and never treated hypertensive patients of different gender. Methods Newly diagnosed and never treated hypertensive patients were divided into two groups by gender. We collect some data such as age, systolic blood pressure, fasting blood-glucose, glycosylated hemoglobin, uricacid, creatinine,microalbuminuria, Aldosterone, renin, angiotensin II, carotid femoral pulse wave velocity (cfPWV)and carotid intima-media thickness by carotid ultrasonography. The correlation was analyzed between the parameter mentioned before and cfPWV in different gender.Results The multiple linear regression analysis shows that age(t=2.296,P=0.027)and systolic blood pressure(t=2.45,P=0.018)were the risk factors of cfPWV increasing in all subjects of our study. In male group, age(t=2.519,P=0.018)and systolic blood pressure(t=2.34,P=0.035)are the risk factors of cfPWV increasing. In addition, age, systolic blood pressure and uric acid are the risk factors of cfPWV increasing in female group.Conclusion Other than ageand systolic blood pressure, uric acidare the risk factors of cfPWV increasing in female with hypertension of our study, but not the risk factor of cfPWV increasing in male group of our study.
Hypertension; cfPWV; Uric acid; Female
国家自然科学基金(30971269;81370374);国家十二五科技支撑计划(2011BAI11B04)
陈晓平,教授,E-mail:971979713@qq.com
R 5441.1
A
10.3969/j.issn.1672-3511.2016.03.013
2015-11-02; 编辑: 母存培)
猜你喜欢
中老年保健(2022年4期)2022-08-22 03:00:52
茶道(2022年3期)2022-04-27 00:15:46
昆明医科大学学报(2021年6期)2021-07-31 07:39:58
基层中医药(2021年1期)2021-07-22 06:56:44
现代临床医学(2021年2期)2021-03-29 05:33:00
金桥(2018年2期)2018-12-06 09:30:14
基层中医药(2018年8期)2018-11-10 05:31:58
大众电视(蓝天下)(2018年8期)2018-10-26 01:00:30
益寿宝典(2018年5期)2018-01-28 09:59:49
电子制作(2017年14期)2017-12-18 07:07:50
