颈椎前路融合术后邻近节段退变的翻修手术
2016-04-05 04:59:42李杰朱悦王丰刘欣春焦鹰
中国医科大学学报 2016年1期
关键词:颈椎
李杰,朱悦,王丰,刘欣春,焦鹰
(中国医科大学附属第一医院骨科,沈阳110001)
颈椎前路融合术后邻近节段退变的翻修手术
李杰,朱悦,王丰,刘欣春,焦鹰
(中国医科大学附属第一医院骨科,沈阳110001)
摘要目的探讨颈椎邻椎病患者翻修手术方式及疗效。方法对2007年至2014年我院收治的7例颈椎前路融合术后出现邻椎病而行翻修手术治疗的患者进行回顾分析。其中颈椎前路翻修手术患者3例,后路翻修手术患者4例。采用改良JOA评分(27分法)及VAS评分进行评价。结果颈椎前路间盘切除融合术治疗患者3例,翻修术后内固定物位置良好,随访未见钢板螺钉松动,植骨块移位等;颈椎后路单开门椎管扩大成形术治疗患者4例,翻修术后无感染等并发症发生。与术前相比,颈椎前路和后路患者在术后随访结束时颈椎JOA评分均明显升高,VAS评分均明显减少。结论颈椎邻椎病翻修术式的选择应遵循兼顾减压及尽可能保留颈椎活动度的原则,翻修术后可取得满意的疗效。
关键词颈椎;邻椎病;翻修手术
网络出版地址
网络出版时间:
Revision Surgery Following Adjacent Segment Diseaseafter Anterior Cervical Decompressionand Fusion
LIJie,ZHUYue,WANGFeng,LIUXin⁃chun,JIAOYing
(Departmentof Orthopedics,The First Hospital,China Medical University,Shenyang110001,China)
Abstract Objective Toanalyzetherevisionsurgeryandevaluatethecurativeeffectofadjacentsegmentdiseaseafteranteriorcervicaldecompres⁃sion and fusion.Methods A retrospective analysis was carried out.Seven cases suffered from cervical revision surgery following adjacent segment disease after anterior cervical decompression and fusion admitted in our hospital during 2007⁃2014 were recruited for the study.The 3 of the 7 pa⁃tients underwent anterior surgery,while the other 4 patients had posterior surgery.The curative was evaluated by the modified JOA and VAS scoring method.Results There were 3 patients underwent anterior cervical decompression and fusion,the internal fixation items locates in good position,andthepostoperativefollow⁃updidnotseesteelscrewloosening,bonegraftblockshift,etc.4patientshadposterioropen⁃doorlaminoplastysurgery,and there was no intraoperative complication among all the revision patients.The JOA and VAS score of all the revision patients become better after therevisionsurgery.Conclusion Itisnecessarytoconsiderdecompressionandretainingcervicalactivitysoastoselectthesuitablerevisionsurgery ofadjacentsegmentdisease.Revisionsurgerycouldachievesatisfactoryresult.
Keywords cervical;adjacent segment disease;revision surgery
颈椎前路融合术是治疗颈椎病的有效方式,具有良好的临床疗效。但是,随着颈椎前路融合术治疗的病例不断增加和随访时间的延长,颈椎邻椎病作为颈椎融合术后的一种远期并发症越来越受到临床医生的关注,少部分邻椎病患者需手术治疗,颈椎邻椎病翻修术式的选择值得研究。本研究对我院2007年1月至2014年2月的7例颈椎前路融合术后出现邻椎病而行翻修手术治疗的患者进行了回顾分析,旨在探讨颈椎邻椎病的翻修手术方式和疗效。
1 材料与方法
1.1一般资料
回顾分析2007年1月至2014年2月我院颈椎前路融合术后邻近节段退变而行颈椎翻修手术的7例患者。其中,男6例,女1例;年龄45~74岁,平均57岁。首次手术后患者再次出现双上肢疼痛、麻木,双下肢麻木、行走不稳等神经学症状最短5年11个月,最长为22年,平均11年9个月。首次手术融合节段为:单节段C5、6患者2例,双节段C4、5,C5、6患者4例,多节段C3、4,C4、5,C5、6患者1例。术前颈椎X线检查结果显示首次手术内固定物位置良好、牢固并且植骨融合,颈椎MRI检查发现融合节段后方未见明显脊髓受压,单纯融合节段近端或远端出现间盘突出,明显脊髓受压的患者4例,其中1例局部明显骨化;融合节段近端及远端均出现间盘突出,明显脊髓受压的患者3例。所有患者均接受了3~6个月的保守治疗,未见明显好转。
1.2手术方式
颈椎翻修手术方式包括颈椎前路手术和颈椎后路手术。颈椎前路翻修手术采用颈椎间盘切除融合固定术(图1),其中2例患者首次手术未置入前路钛板,1例患者首次置入了前路钛板,翻修时取出;颈椎后路手术采用颈椎后路单开门椎管扩大成形术(图2)。
1.3评估方法
翻修术后随访时间2个月至6年4个月,平均24个月。翻修手术前及随访结束时采用改良JOA评分(27分法)及VAS评分进行评价。用改善率评估手术前后功能改善及疼痛缓解情况。
2 结果
颈椎前路间盘切除融合术治疗患者3例,翻修术后内固定物位置良好,随访未见钛板螺钉松动、植骨块移位等;颈椎后路单开门椎管扩大成形术治疗患者4例,翻修术后无感染等并发症发生。与术前相比,颈椎前路和后路患者在术后随访结束时颈椎JOA评分明显升高,VAS评分明显减少,见表1。
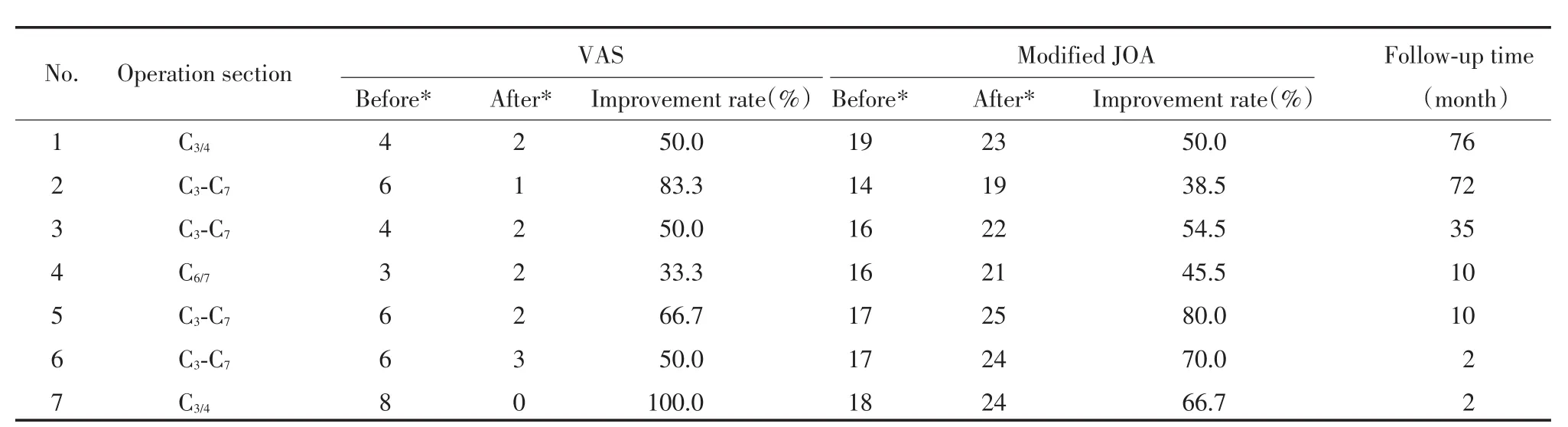
表1 患者翻修术前及随访结束时颈椎改良JOA及VAS评分Tab.1 Modified JOA and VAS scoring before revision surgery and in the end of follow⁃up visit
3 讨论
3.1邻椎病的发病机制
目前研究邻椎病的发病机制可能与以下几个方面有关:(1)融合邻近节段负荷增大。椎间盘压力升高,并且融合节段越多,内固定强度越大,椎间盘压力增高越明显[1]。(2)融合邻近节段活动度增加。融合节段的活动度消失,转移到相邻节段,引起相邻节段出现过度活动、应力增加[2,3]。(3)颈椎融合术后颈椎生理曲度的改变,导致邻近节段退变加速[4]。同时,患者自身的情况(年龄、骨质等)可能也是加速邻椎病发生的重要因素。还有一些研究[5]认为邻椎病的发生可能是自然退变的过程,与融合手术无关。
3.2邻椎病的翻修手术
Teramoto等[6]随访发现首次术后10年,50%的患者颈椎MRI检查发现融合邻近节段退变,但仅6.7%的患者需翻修手术治疗。有研究[7]显示颈椎前路融合术后10年以上,有超过25%的患者出现伴有临床症状的相邻节段退变,但行翻修手术治疗的患者比例远低于此。Hilibrand等[8]对374例进行颈椎融合手术的患者进行21年随访,发现有症状的融合邻近节段退变的年发生率为2.9%,而总的发生率为14.2%。Carola等[9]报道因颈椎邻椎病而行翻修手术的比例为7%。1篇基于台湾11年人口资料的研究[10]发现颈椎邻椎病翻修手术患者占同期颈椎前路融合术患者的比例为0.8%。我院2007年1月至2014年2月行颈椎前路融合术的患者1 042例,因邻椎病而行翻修手术患者7例,比例为0.7%。
3.3翻修手术方式
颈椎邻椎病的翻修手术方式包括颈椎前路手术和后路手术的方式。颈椎前路手术包括颈椎间盘切除融合术和颈椎人工间盘置换术。颈椎间盘切除融合术能够彻底解除前路致压物的压迫,减压充分,疗效好。但会降低颈椎的活动度,可能再次发生邻椎病,同时部分翻修术后的患者出现吞咽困难等并发症[11,12]。颈椎人工间盘置换术能有效的保留颈椎活动度,但部分患者术后出现邻近节段退变加速及异位骨化,同时有研究[13]认为邻近椎体融合是颈椎人工间盘置换术的禁忌证。颈椎后路手术包括椎板成形术和椎板切除融合术。椎板成形术适用于多节段减压及邻近节段骨化明显的患者,同时能够保留颈椎的活动度,但并未彻底解除致压物的压迫,间接减压,影响减压效果[14]。椎板切除融合术同样适用于多节段减压及邻近节段骨化明显的患者,但会降低颈椎的活动度,与颈椎前路翻修手术相比,术中失血多,术后感染等并发症发生率高[15]。在本组患者中,对于只存在融合节段上或下单侧邻近节段退变并且没有明显骨化的3例患者采取颈椎前路间盘切除融合固定术;对于融合节段上下邻近节段均有退变或有明显骨化的4例患者采取颈椎后路单开门椎管扩大成形术。
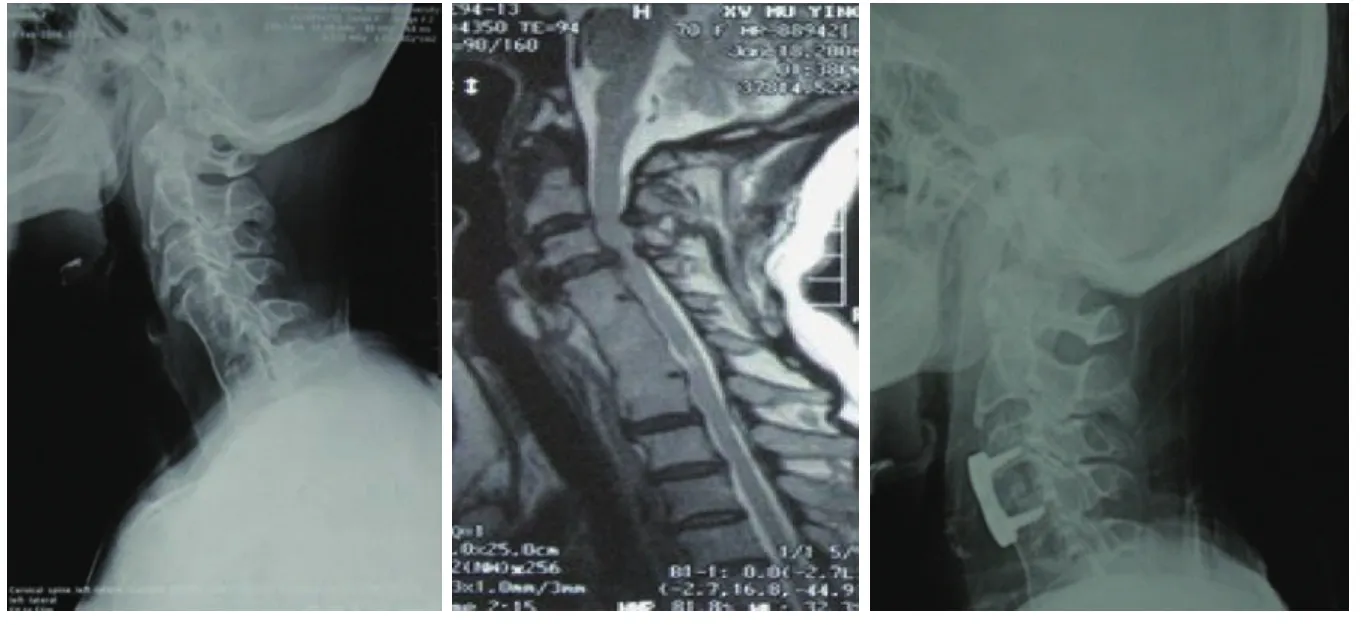
图1 颈椎前路翻修患者影像Fig.1 Imaging performance of patient underwent anterior surgery
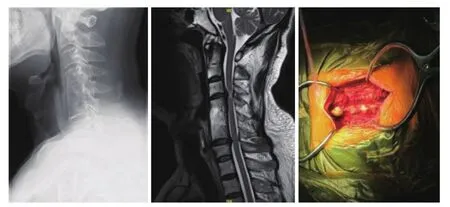
图2 颈椎后路翻修患者影像Fig.2 Imaging performance of patient underwent posterior surgery
颈椎邻椎病翻修术式的选择应遵循兼顾减压及尽可能保留颈椎活动度的原则。本研究认为融合节段近端或远端单侧间盘明显突出,采用颈椎前路间盘切除融合术;融合节段近端及远端同时出现间盘明显突出或局部明显骨化,采用颈椎后路单开门椎管扩大成形术。翻修术后可取得满意的疗效。
参考文献:
[1]Bastian L,Lange U,Knop C,et al.Evaluation of the mobility of adja⁃cent segments after posterior thoracolumbar fixation:a biomechani⁃cal study[J].Eur Spine J,2001,10(4):295-300.
[2]Elsawaf A,Mastronardi L,Roperto R,et al.Effect of cervical dynam⁃ics on adjacent segment degeneration after anterior cervical fusion with cages[J].Neurasurg Rev,2009,32(2):215-224.
[3]Ragab A,Escarcega AJ,Zdeblick TA.A quantitative analysis of strain at adjacent segments after segmental immobilization of the cervical spine[J].J Spinal Disord,2006,19(6):407-410.
[4]Lotz JC,Chin JR.Intervertebral disc cell death is dependent on the magnitude and duration of spinal loading[J].Spine,2000,25(12):1477.
[5]Ishihara H,Kanamori M,Kawaguchi Y,et al.Adjacent segment dis⁃ease after anterior cervical interbody fusion[J].Spine J,2004,4(6):624-628.
[6]Teramoto T,Ohmori K,Takatsu T,et al.Long⁃term results of the an⁃terior cervical spondylodesis[J].Neuiosugery,1994,35(1):64-68.
[7]Rihn JA,Lawrence J,Gates C,et al.Adjacent segment disease after cervical spine fusion[J].Instr Course Lect,2009,58:747-756.
[8]Hilibrand AS,Carlson GD,Palumbo MA,et al.Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis[J].J Bone Joint Surg Am,1999,81(4):519-528.
[9]van Eck CF,Regan C,Donaldson WF.The revision rate and occur⁃rence of adjacent segment disease after anterior cervical discectory and fusion:a study of 672consecutive patients[J].Spine,2014,39(26):2143-2147.
[10]Wu JC,Liu L,Wen⁃Cheng H,et al.The incidence of adjacent seg⁃ment disease requiring surgery after anterior cervical diskectomy and fusion:estimation using an 11⁃year comprehensive nationwide database in Taiwan[J].Neurosugery,2012,70(3):594-601.
[11]Chen Y,He Z,Yang H,et al.Anterior cervical diskectomy and fu⁃sion for adjacent segment disease[J].Orthopedics,2013,36(4):e501-508.
[12]Arnold P,Boswell S,McMahon J.Threaded interbody fusion cage for adjacent segment degenerative disease after previous anterior cervical fusion[J].Surg Neurol,2008,70(4):390-397.
[13]Auerbach JD,Jones KJ,Fras CI,et al.The prevalence of indica⁃tions and contraindication to cervical total dicsreplacement[J].Spine,2008,8(5):711-716.
[14]Matsumoto M,Nojiri K,Chiba K,et al.Open⁃door laminoplasty for cervical myelopathy resulting from adjacent⁃segment disease in pa⁃tients with previous anterior cervical decompression and fusion[J].Spine,2006,31(12):1332-1337.
[15]Bydon M,Xu R,De la Garza⁃Ramos R,et al.Segment disease after anterior cervical discectomy and fusion:incidence and clinical out⁃comes of patients requiring anterior versus posterior repeat cervical fusion[J].Surg Neurol Int,2014,5(Suppl 3):S74-78.
(编辑于溪)
收稿日期:2015-02-07
通信作者:朱悦,E-mail:zhuyuedr@163.com
作者简介:李杰(1986-),男,医师,硕士.
Doi:10.12007/j.issn.0258-4646.2016.01.017
中图分类号R459.9
文献标志码A
文章编号0258-4646(2016)01-0073-04
猜你喜欢
大自然探索(2024年1期)2024-02-29 09:11:26
保健医苑(2022年1期)2022-08-30 08:40:00
保健医苑(2022年6期)2022-07-08 01:25:34
世界最新医学信息文摘(2021年12期)2021-06-09 08:35:56
现代临床医学(2019年6期)2019-12-07 06:03:32
中学生数理化·中考版(2018年12期)2019-01-31 06:19:04
中国生殖健康(2019年10期)2019-01-07 01:21:20
华人时刊(2017年19期)2017-11-21 22:12:27
中华骨与关节外科杂志(2017年1期)2017-05-17 06:11:18
中国中西医结合外科杂志(2013年3期)2013-03-11 20:05:02