
阿托伐他汀钙片、瑞舒伐他汀钙片与氟伐他汀钠胶囊治疗高龄冠心病患者临床疗效的对比研究
2016-02-07 01:35李冠兰
实用心脑肺血管病杂志 2016年12期
方 玲,李冠兰
·疗效比较研究·
阿托伐他汀钙片、瑞舒伐他汀钙片与氟伐他汀钠胶囊治疗高龄冠心病患者临床疗效的对比研究
方 玲,李冠兰
目的 比较阿托伐他汀钙片、瑞舒伐他汀钙片与氟伐他汀钠胶囊治疗高龄冠心病患者的临床疗效。方法 选取2013年4月—2015年10月三峡大学人民医院收治的高龄冠心病患者244例,根据治疗方法分为A组86例、B组93例、C组65例。A组患者予以阿托伐他汀钙片治疗,B组患者予以瑞舒伐他汀钙片治疗,C组患者予以氟伐他汀钠胶囊治疗;3组患者均连续治疗6个月。比较3组患者治疗前后血脂指标〔总胆固醇(TC)、三酰甘油(TG)、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇(LDL-C)〕,治疗期间死亡情况(心血管不良事件病死率、脑血管不良事件病死率、总病死率)及丙氨酸氨基转移酶(ALT)、血肌酐(Scr)和肌酸激酶(CK)异常情况。结果 治疗前后3组患者TC、TG、HDL-C、LDL-C水平比较,差异无统计学意义(P>0.05);3组患者治疗后TC、LDL-C水平均低于治疗前(P<0.05)。3组患者心血管不良事件病死率、脑血管不良事件病死率、总病死率比较,差异无统计学意义(P>0.05)。3组患者治疗期间ALT、Scr、CK异常率比较,差异无统计学意义(P>0.05)。结论 阿托伐他汀钙片、瑞舒伐他汀钙片与氟伐他汀钠胶囊治疗高龄冠心病患者的临床疗效相当,均可有效改善患者血脂代谢,且安全性均较高。
冠心病;老年人,80以上;瑞舒伐他汀钙片;阿托伐他汀钙片;氟伐他汀钠胶囊;治疗结果
方玲,李冠兰.阿托伐他汀钙片、瑞舒伐他汀钙片与氟伐他汀钠胶囊治疗高龄冠心病患者临床疗效的对比研究[J].实用心脑肺血管病杂志,2016,24(12):59-62.[www.syxnf.net]
FANG L,LI G L.Comparative study for clinical effect in treating elderly patients with coronary heart disease among atorvastatin calcium tablets,rosuvastatin calcium tablets and fluvastatin sodium capsules[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2016,24(12):59-62.
近年来,随着我国人口老龄化进程加剧,冠心病发病率呈逐年上升趋势,严重影响人们的生活质量及生命安全[1]。动脉粥样硬化(AS)是冠心病的危险因素,可造成血管内皮细胞功能损伤,导致血栓形成[2]。他汀类药物具有调节血脂、抑制炎性反应、稳定粥样硬化斑块、改善血管内皮细胞功能、延缓AS进程、保护神经元和抗血栓等作用[3-4]。高龄患者由于身体功能较差,常合并多种基础疾病,故治疗时应谨慎,以保证用药安全[5]。本研究旨在比较阿托伐他汀钙片、瑞舒伐他汀钙片与氟伐他汀钠胶囊治疗高龄冠心病患者的临床疗效,现报道如下。
1 资料与方法
1.1 纳入与排除标准 纳入标准:(1)符合冠心病的诊断标准[6];(2)首次发病,且需要长期使用他汀类药物治疗;(3)年龄≥80岁。排除标准:(1)对他汀类药物过敏患者;(2)伴有严重心、肝、肾功能不全患者;(3)伴有心肌疾病患者;(4)存在恶性肿瘤患者;(5)合并自身免疫性疾病患者;(6)合并甲状腺功能亢进症或甲状腺功能减退症患者。
1.2 一般资料 选取2013年4月—2015年10月三峡大学人民医院收治的高龄冠心病患者244例,根据治疗方法分为A组86例、B组93例、C组65例。3组患者性别、年龄、体质指数、吸烟率、糖尿病发生率、高血压发生率、卒中病史阳性率比较,差异无统计学意义(P>0.05,见表1),具有可比性。本研究经医院医学伦理委员会审核批准,患者及其家属均签署知情同意书。
1.3 治疗方法 A组患者予以阿托伐他汀钙片(辉瑞制药有限公司生产,国药准字H20051408)20 mg口服,1次/晚;B组患者予以瑞舒伐他汀钙片(阿斯利康制药有限公司生产,国药准字J20120006)10 mg口服,1次/晚;C组患者予以氟伐他汀钠胶囊(商品名:来适可,北京诺华制药有限公司生产,国药准字H20010518)40 mg口服,1次/晚。3组患者均连续治疗6个月。
1.4 观察指标 比较3组患者治疗前后血脂指标〔总胆固醇(TC)、三酰甘油(TG)、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇(LDL-C)〕,治疗期间死亡情况(心血管不良事件病死率、脑血管不良事件病死率、总病死率)及丙氨酸氨基转移酶(ALT)、血肌酐(Scr)和肌酸激酶(CK)异常发生情况。分别采集患者治疗前后清晨空腹静脉血5 ml,3 500 r/min离心15 min,采用贝克曼库尔特AU680全自动生化分析仪检测TC、TG、HDL-C、LDL-C、ALT、Scr、CK水平;ALT>49 U/L为异常,Scr>106 μmol/L为异常,CK>200 U/L为异常。
2 结果
2.1 血脂指标 治疗前后3组患者TC、TG、HDL-C、LDL-C水平比较,差异无统计学意义(P>0.05);3组患者治疗后TC、LDL-C水平低于治疗前,差异有统计学意义(P<0.05,见表2)。
2.2 治疗期间死亡情况 3组患者治疗期间心血管不良事件病死率、脑血管不良事件病死率、总病死率比较,差异无统计学意义(P>0.05,见表3)。
2.3 治疗期间ALT、Scr、CK异常情况 3组患者ALT、Scr、CK异常率比较,差异无统计学意义(P>0.05,见表4)。
表3 3组患者治疗期间病死率比较〔n(%)〕
Table 3 Comparison of fatality rate among the three groups during the treatment
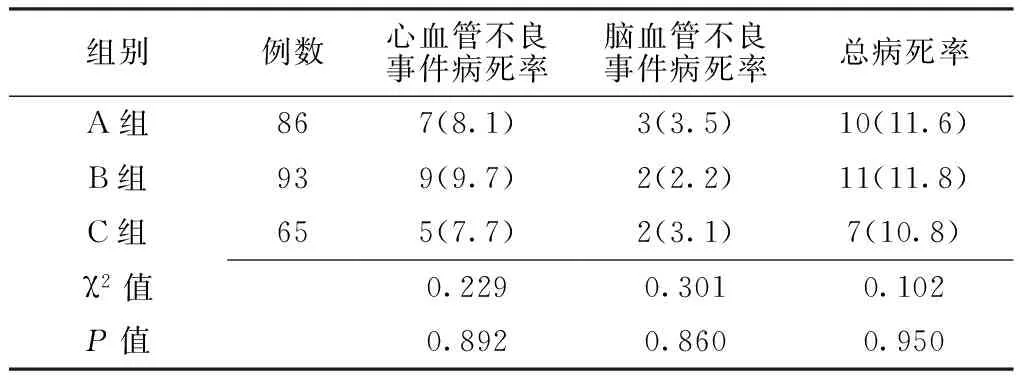
组别例数心血管不良事件病死率脑血管不良事件病死率总病死率A组867(8.1)3(3.5)10(11.6)B组939(9.7)2(2.2)11(11.8)C组655(7.7)2(3.1)7(10.8)χ2值0.2290.3010.102P值0.8920.8600.950

表1 3组患者一般资料比较
注:a为F值

表2 3组患者治疗前后血脂指标比较
注:TC=总胆固醇,TG=三酰甘油,HDL-C=高密度脂蛋白胆固醇,LDL-C=低密度脂蛋白胆固醇;与治疗前比较,aP<0.05
表4 3组患者治疗期间ALT、Scr、CK异常率比较〔n(%)〕
Table 4 Comparison of incidence of ALT abnormity,Scr abnormity and CK abnormity among three groups during the treatment
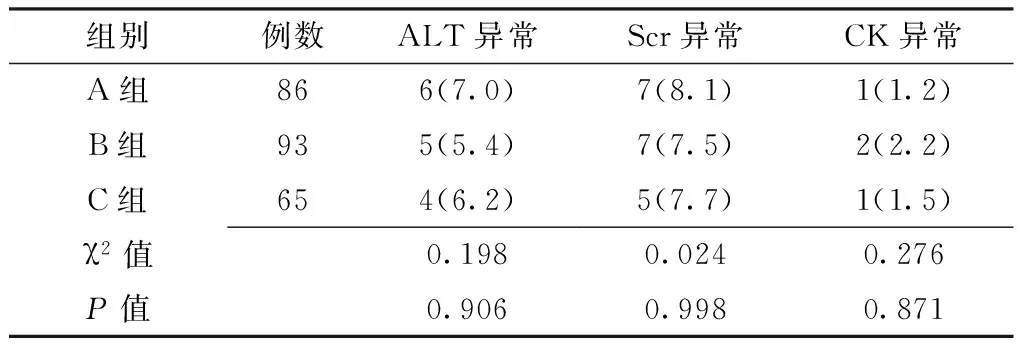
组别例数ALT异常Scr异常CK异常A组866(7.0)7(8.1)1(1.2)B组935(5.4)7(7.5)2(2.2)C组654(6.2)5(7.7)1(1.5)χ2值0.1980.0240.276P值0.9060.9980.871
注:ALT=丙氨酸氨基转移酶,Scr=血肌酐,CK=肌酸激酶
3 讨论
AS的主要病理改变为内皮细胞功能损伤、脂质聚集、纤维粥样斑块形成等,其是冠心病的危险因素[7]。冠心病是由于冠状动脉粥样硬化造成管腔狭窄或阻塞导致心肌缺血、缺氧而引起的心脏病,是AS导致脏器病变的最常见类型,也是严重威胁人们生命、健康的常见病[8]。研究表明,高血压、高脂血症、糖尿病、年龄、吸烟等是冠心病的危险因素[9]。
他汀类药物是羟甲基戊二酸单酰辅酶A(HMG-CoA)还原酶抑制剂,可通过竞争性抑制内源性胆固醇合成限速酶HMG-CoA还原酶而阻断细胞内羟甲戊酸代谢途径而减少细胞内胆固醇合成,从而反馈性刺激细胞膜表面(主要为肝细胞)LDL-C受体,使LDL-C受体数量及活性增加[10]。阿托伐他汀钙片是脂溶性他汀类药物,具有起效快、持续时间长等特点[11]。瑞舒伐他汀钙片是人工合成的水溶性他汀类药物,具有多种代谢途径,具有吸收、见效快,安全性高的特点,其降脂效果较好。氟伐他汀钠胶囊主要作用于肝脏,可将HMG-CoA转化为3-甲基-3,5-二羟戊酸,具有抑制内源性胆固醇合成,降低肝细胞内胆固醇含量,刺激低密度脂蛋白(LDL)受体分泌,提高LDL微粒摄取,降低血浆TC水平等作用。研究表明,氟伐他汀钠可降低TC、TG、LDL-C水平,提高HDL-C水平[12]。本研究结果显示,治疗前后3组患者TC、TG、HDL-C、LDL-C水平间无差异,3组患者治疗后TC、LDL-C水平低于治疗前,与既往研究结果一致[12-13]。提示阿托伐他汀钙片、瑞舒伐他汀钙片及氟伐他汀钠胶囊对高龄冠心病患者均具有改善血脂代谢作用,可有效降低TC、LDL-C水平,且对LDL-C 水平正常或偏低的高龄患者可发挥抗炎、稳定斑块、改善血管内皮细胞功能、抑制动脉平滑肌细胞增殖等作用[14]。
他汀类药物具有调脂、抗AS的作用,但我国冠心病患者他汀类药物基础用量严重不足,尤其是高龄患者[15]。研究表明,冠心病患者院外服用他汀类药物的依从性较差、药品费用较高、缺乏个体化治疗指导[16]。本研究结果显示,3组患者治疗期间心血管不良事件病死率、脑血管不良事件病死率、总病死率和ALT、Scr、CK异常率间无差异,提示阿托伐他汀钙片、瑞舒伐他汀钙片及氟伐他汀钠胶囊治疗高龄冠心病患者的安全性较高。
综合上述,阿托伐他汀钙片、瑞舒伐他汀钙片与氟伐他汀钠胶囊治疗高龄冠心病患者的临床疗效相当,均可有效改善患者血脂代谢,且安全性均较高。但本研究为回顾性研究,存在一定选择偏倚,且观察时间较短,未分析其成本-效益,有待于在今后的研究中进一步完善。
[1]陈伟伟,高润霖,刘力生,等.中国心血管病报告2013概要[J].中国循环杂志,2014(7):613-615.
[2]YANG G,WANG Y,ZENG Y,et al.Rapid health transition in China,1990—2010:findings from the Global Burden of Disease Study 2010[J].Lancet,2013,381(9882):1987-2015.
[3]Writing Group Members,MOZAFFARIAN D,BENJAMIN E J,et al.Executive Summary:Heart Disease and Stroke Statistics-2016 Update:A Report From the American Heart Association[J].Circulation,2016,133(4):447-454.
[4]NISSEN S E,TUZCU E M,SCHOENHAGEN P,et al.Statin therapy,LDL cholesterol,C-reactive protein,and coronary artery disease[J].N Engl J Med,2005,352(1):29-38.
[5]MASSARO M,ZAMPOLLI A,SCODITTI E,et al.Statins inhibit cyclooxygenase-2 and matrix metalloproteinase-9 in human endothelial cells:anti-angiogenic actions possibly contributing to plaque stability[J].Cardiovasc Res,2010,86(2):311-320.
[6]中华医学会心血管病学分会.慢性稳定性心绞痛诊断与治疗指南[J].中华心血管病杂志,2007,35(3):195-206.
[7]PREISS D,SESHASAI S R,WELSH P,et al.Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy:a meta-analysis[J].JAMA,2011,305(24):2556-2564.
[8]SAVARESE G,GOTTO A M J R,PAOLILLO S,et al.Benefits of statins in elderly subjects without established cardiovascular disease:a meta-analysis[J].J Am Coll Cardiol,2013,62(22):2090-2099.
[10]KELLICK K A,BOTTORFF M,TOTH P P,et al.A clinician′s guide to statin drug-drug interactions[J].J Clin Lipidol,2014,8(3 Suppl):S30-46.
[11]BAIGENT C,LANDRAY M J,REITH C,et al.The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection):a randomised placebo-controlled trial[J].Lancet,2011,377(9784):2181-3292.
[12]冯雪茹,张婧薇,刘梅林,等.瑞舒伐他汀对中国颈动脉粥样硬化患者内中膜厚度和安全性的荟萃分析[J].中华心血管病杂志,2014,42(3):247-253.
[13]Expert Dyslipidemia Panel of the International Atherosclerosis Society Panel members.An International Atherosclerosis Society Position Paper:global recommendations for the management of dyslipidemia-full report[J].J Clin Lipidol,2014,8(1):29-60.
[14]YANG W,XIAO J,YANG Z,et al.Serum lipids and lipoproteins in Chinese men and women[J].Circulation,2012,125(18):2212-2221.
[15]STONE N J,ROBINSON J G,LICHTENSTEIN A H,et al.2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults:a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines[J].J Am Coll Cardiol,2014,63(25 Pt B):2889-2934.
[16]NOHARA R,DAIDA H,HATA M,et al.Effect of intensive lipid-lowering therapy with rosuvastatin on progression of carotid intima-media thickness in Japanese patients:Justification for Atherosclerosis Regression Treatment(JART)study[J].Circ J,2012,76(1):221-229.
(本文编辑:李洁晨)
Comparative Study for Clinical Effect in Treating Elderly Patients with Coronary Heart Disease among Atorvastatin Calcium Tablets,Rosuvastatin Calcium Tablets and Fluvastatin Sodium Capsules
FANGLing,LIGuan-lan.
DepartmentofCardiology,thePeople′sHospitalofChinaThreeGorgesUniversity,Yichang443000,China
LIGuan-lan,DepartmentofCardiology,thePeople′sHospitalofChinaThreeGorgesUniversity,Yichang443000,China;E-mail:liguanlancv@163.com
Objective To compare the clinical effect in treating elderly patients with coronary heart disease among atorvastatin calcium tablets,rosuvastatin calcium tablets and fluvastatin sodium capsules.Methods A total of 244 elderly patients with coronary heart disease were selected in the People′s Hospital of China Three Gorges University from April 2013 to October 2015,and they were divided into A group(n=86),B group(n=93)and C group(n=65)according to therapeutic methods.Patients of A group received atorvastatin calcium tablets,patients of B group received rosuvastatin calcium tablets,while patients of C group received fluvastatin sodium capsules;all of the three groups continuously treated for 6 months.Blood liquids index(including TC,TG,HDL-C and LDL-C)before and after treatment,fatality rate caused by adverse cardiovascular events or adverse cerebrovascular events,total fatality rate,abnormity of ALT,Scr and CK during the treatment were compared among the three groups.Results No statistically significant differences of TC,TG,HDL-C or LDL-C was found among the three groups before or after treatment(P>0.05);after treatment,TC and LDL-C of the three groups were statistically significantly lower compared with those before treatment(P<0.05).No statistically significant differences of fatality rate caused by adverse cardiovascular events or adverse cerebrovascular events,or total fatality rate was found among the three groups during the treatment(P>0.05).No statistically significant differences of incidence of ALT abnormity,Scr abnormity or CK abnormity was found among the three groups during the treatment(P>0.05).Conclusion Atorvastatin calcium tablets,rosuvastatin calcium tablets and fluvastatin sodium capsules have similar clinical effect in treating elderly patients with coronary heart disease,all of them can effectively adjust the blood lipid metabolism,with relatively high safety.
Coronary disease;Aged,80 and over;Suvastatin calcium tablets;Atorvastatin calcium tablets;Atorvastatin calcium;Treatment outcome
443000湖北省宜昌市,三峡大学人民医院心内科
李冠兰,443000湖北省宜昌市,三峡大学人民医院心内科;E-mail:liguanlancv@163.com
R 541.4
B
10.3969/j.issn.1008-5971.2016.12.015
2016-09-18;
2016-12-19)
猜你喜欢
临床骨科杂志(2022年3期)2022-11-24
世界科学技术-中医药现代化(2021年5期)2021-11-05
现代畜牧科技(2021年4期)2021-07-21
中华养生保健(2020年8期)2021-01-14
环境与生活(2019年1期)2019-09-10
中国卫生标准管理(2015年8期)2016-01-15
中国卫生标准管理(2015年6期)2016-01-14
医学研究杂志(2015年4期)2015-06-10
中国卫生标准管理(2015年17期)2015-01-26
当代医学(2014年36期)2014-07-31
