
滑膜增生型腕管综合征的手术治疗
2014-07-05 13:14:06李建强姜保国陈建海付中国王天兵
中华肩肘外科电子杂志 2014年2期
李建强 姜保国 陈建海 付中国 王天兵
滑膜增生型腕管综合征的手术治疗
李建强 姜保国 陈建海 付中国 王天兵
目的探讨滑膜增生型腕管综合征(carpal tunnel syndrome,CTS)的临床表现、手术治疗方法及疗效。方法对2004年10月至2010年10月收治的63例(75侧)经保守治疗3个月无效的滑膜增生型CTS患者行腕横韧带切开减压、腕管内滑膜清除、正中神经松解治疗,术后将切除滑膜进行病理学检查。以Kelly标准评价手术效果。结果术后46例(50侧)患者获得随访,随访时间为3~12个月,平均4.6个月;病理学检查显示:正中神经周围纤维结缔组织水肿变性,滑膜组织增生,淋巴细胞、浆细胞浸润;术后3个月行神经电生理检查50侧,正中神经运动传导速度、感觉传导速度、运动远端潜伏期、感觉远端潜伏期与术前比较差异有统计学意义(t=-6.095、-2.935、15.895、16.011,P均<0.05);按照Kelly标准:优32侧,良14侧,一般4侧,差0侧。结论夜间因滑膜充血肿胀剧烈导致麻木疼痛加剧,以及神经电生理检查显示正中神经运动、感觉传导速度降低程度较轻,是滑膜增生型CTS的典型临床表现;切断腕横韧带的同时行腕管内滑膜切除是治疗滑膜增生型CTS的有效方法。
腕管综合征;神经电生理检查;腕管切开减压;正中神经松解术
腕管综合征(carpal tunnel syndrome,CTS)是周围神经卡压性疾病中最常见的一种,是正中神经在腕管内受到压迫所产生的一组临床综合征[1],腕横韧带坚韧、近侧缘增厚是压迫正中神经的主要因素。正常情况下,腕管内存在大量的肌腱滑膜,对肌腱起到营养和润滑作用。但是,由于肌腱滑膜过度增生,甚至出现充血、水肿等炎症反应会导致或加重对正中神经的压迫,并对神经产生炎性刺激。CTS的主要临床表现是桡侧三个半手指麻木和疼痛,疼痛向手部和前臂放射,拇指对掌功能受限,大鱼际肌萎缩,握力和捏力减弱[2]。而滑膜增生型CTS由于滑膜在夜间充血加重,回流停滞,会出现明显的夜间疼痛、麻木,甚至在夜间的固定时间麻醒,这是滑膜增生型CTS的典型症状。很多患者在麻醒后通过活动手指、手腕促进了腕管内滑膜的回流,降低腕管内压力以缓解疼痛。所以在临床上会出现静息状态下临床表现与活动后电生理检查结果不能够完全符合的现象。自2004年10月至2010年10月北京大学人民医院创伤骨科共收治滑膜增生型CTS患者63例(75侧),采用腕管切开、腕横韧带切断、滑膜切除、正中神经松解的方法进行治疗,取得了良好的治疗效果,报道如下。
材料和方法
一、一般资料
本组患者63例(75侧),其中男性16例,女性47例;年龄40~82岁,平均年龄62岁;右侧36例,左侧15例,双侧12例;病程最长8年,最短3个月。出现症状至就诊的时间为3周至2年。发病原因:49例为长期慢性损伤所致,14例由代谢免疫性疾病所致(多为双侧),例如类风湿性关节炎、痛风、干燥综合征等。所有患者无明确腕部外伤、骨折、脱位病史,无腕部肿物。患者症状主要为腕部疼痛、麻木和握、捏无力,夜间常常痛醒,有时可向肘部和肩部放射,不停甩手后症状可改善。查体:腕部Tinel征阳性,桡侧3个半手指掌侧感觉异常、大鱼际肌不同程度的萎缩。术前行神经电生理检测,包括正中神经运动传导速度、感觉传导速度、运动远端潜伏期和感觉远端潜伏期。本组患者术前均接受过非甾体抗炎药,局部理疗和腕管内注射等保守治疗,保守治疗后临床症状均有不同程度的缓解,但多数因症状复发或反复发作,严重影响患者的生活质量来我院要求手术治疗。63例(75侧)患者均行腕横韧带切开减压、腕管内滑膜切除、正中神经松解治疗。
二、手术方法
患者均采用臂丛神经阻滞麻醉,麻醉成功后患者取平卧位,患肢外展,上气囊止血带,压力300mmHg,常规消毒铺无菌巾,鱼际纹中点至腕横纹做长约3cm弧形切口,切开皮肤、皮下组织及掌腱膜层。首先在腕横纹水平切开腕横韧带,并直视下向近端切开腕横韧带,切开腕横韧带时严格防止损伤深层的正中神经,直至全部切断腕横韧带,在鱼际纹中点及其以远注意损伤正中神经返支。术中见腕横韧带明显增厚,正中神经在腕横韧带下方受压,神经变扁,外膜增厚,受压部色泽暗淡,可见神经营养血管中断现象,周围有疤痕,腕管内屈指深、浅肌腱被大量滑膜组织包裹。在切断腕横韧带之后,分离正中神经,根据神经受到卡压及增生情况决定是否行神经外膜松解。如果行神经外膜松解,用显微手术剪松解神经增生的组织,纵行切开病变上下端的神经外膜,直至显露正常柔软的神经,从而完成彻底松解。严格保护正中神经,分离腕管内的屈指深、浅肌腱,仔细切除增生、病变的滑膜组织。松止血带,严格创面止血,留置引流条,缝合掌腱膜层及全层缝合切口皮肤。将所切除的肌腱周围滑膜组织送病理检查。
三、术后处理
术后24h内拔除引流条,在医生指导下进行手指的屈曲和背伸活动,防止肌腱黏连,夜间将患侧肢体抬高减轻肿胀;术后14d伤口拆线;口服甲钴胺片3周;手术4~6周后完全正常活动。
四、疗效判断标准
术后3个月以Kelly标准评价手术效果,优:症状完全消失;良:症状明显缓解;一般:症状轻度减轻或者持续;差:症状不变或加重。并进行神经电生理检测。
五、统计学分析
采用SPSS统计学软件,使用配对样本t检验分析,P<0.05为差异有统计学意义。
结 果
共计46例患者(50侧)获得3个月以上的临床随访,术后随访时间平均为4.6个月,术后第1天手麻、胀痛症状均有不同程度减轻,夜间麻醒症状消失。手术切口愈合良好,没有出现感染、长期不愈合等并发症,无瘢痕挛缩,术后3~12个月无复发。所有患者术后未出现正中神经、掌浅弓、正中神经返支损伤等并发症。
术中可见周围滑膜组织明显增生,压迫正中神经,术后病理检查显示:正中神经周围纤维结缔组织水肿变性,滑膜组织增生,淋巴细胞、浆细胞浸润(图1、2)。

图1 滑膜组织明显增生

图2 纤维结缔组织水肿变性,滑膜组织增生,淋巴细胞、浆细胞浸润
术前电生理检测显示正中神经运动、感觉传导速度无明显减低,分别为(48.32±3.68)m/s、(46.32±3.68)m/s;术后3个月行神经电生理检查50侧,正中神经运动、感觉传导速度分别是(51.64±2.70)m/s、(50.11±3.47)m/s,较术前加快,差异有统计学意义(t=-6.095、-2.935,P均<0.05);正中神经运动远端潜伏期由(4.38±0.40)ms缩短为(3.47±0.27)ms,感觉远端潜伏期由(5.12±0.36)ms缩短为(4.14±0.31)ms,差异有统计学意义(t=15.895、16.011,P均<0.05)(表1)。
按照Kelly标准,术后优32侧,夜间痛、手指麻木完全消失;良14侧,夜间痛、手指麻木较前明显缓解,未完全消失;一般4侧;差0侧,优良率为96%(表2)。
表1 术前、术后正中神经电生理比较(±s)
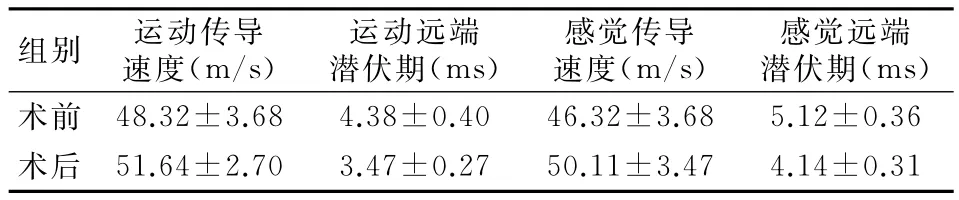
表1 术前、术后正中神经电生理比较(±s)
组别 运动传导速度(m/s)运动远端潜伏期(ms)感觉传导速度(m/s)感觉远端潜伏期(ms)术 前 48.32±3.68 4.38±0.40 46.32±3.68 5.12±0.36术 后 51.64±2.70 3.47±0.27 50.11±3.47 4.14±0.31

表2 术后临床疗效评价(Kelly)
讨 论
滑膜增生型CTS是临床上较为常见的疾病,多发于40~60岁的女性。腕管是腕掌部的一个骨纤维管,拇长屈肌和4根屈指浅肌腱、4根屈指深肌腱及正中神经通过此管进入手部。腕管由腕骨和腕横韧带构成。正常腕管内压为20~30mmHg,腕关节在完全屈伸位时腕管内压力升至94~110mmHg。正中神经传导速度的正常范围是MNCV=53.7m/s、SNCV=57.5m/s[3]。X 线片可了解腕骨部位有无骨、关节病理改变。在临床上,开放手术行腕横韧带切开、正中神经松解被认为是治疗的金标准[4]。而近年来随着内窥镜的普及和微创外科理念的深入,有很多患者接受了内窥镜微创治疗[5-6]。然而内窥镜治疗的原理是切断腕横韧带从而减轻对正中神经的压迫作用,无法进行腕管内滑膜的切除及正中神经的外膜松解。所以对于滑膜增生、滑膜的炎性反应刺激正中神经所引起的CTS,则需要通过开放手术进行腕横韧带的切断、滑膜的切除及正中神经外膜松解,从根本上解决正中神经受到压迫和刺激的所有因素[7]。本组病例主要为中老年患者,与年轻患者相比较,中老年患者少有腕管内骨性突起或外生肿物压迫,大多为腕部长期劳损和免疫性、代谢性疾病患者,腕管内肌腱、滑膜增生、肥厚,容积变小,压力增高。其表现为由于组织缺血、缺氧,炎性物质释放而产生较为严重的正中神经支配区疼痛症状。同时由于血流的淤滞、手指活动的减少,腕管内滑膜的充血、肿胀会在夜间明显加重,而在白天减轻,从而出现夜间麻木、胀痛等症状明显加重,甚至出现夜间麻醒病史。对于此类CTS患者腕管彻底减压的治疗意义尤其重要。该病在病变的初期表现为正中神经的水肿和充血,逐渐由于压迫性缺血而造成神经内的纤维化、神经轴突压缩和髓磷脂鞘的消失,最后神经组织转为纤维组织,其神经内管消失并被胶原组织代替,成为不可逆的改变导致肌肉组织在失去神经营养时出现局部萎缩的现象[8]。CTS分为3个时期。早期:腕横韧带肥厚,单纯卡压,症状较轻,无正中神经病理形态改变;中期:多由长期卡压,慢性损伤,代谢性疾病所致腕管内肌腱、滑膜及神经水肿,纤维增生,出现无菌性炎症引起的神经症状,此时正中神经病变是可逆的,减压后可恢复正常;晚期:运动和感觉均明显减退,正中神经纤维化,部分脱髓鞘变和轴突退行变,此时为不可逆损害。因此,提高CTS疗效的关键是早诊断、早治疗。尤其是老年患者,腕管内滑膜增生组织长期刺激,神经受卡压后,神经变性出现早,术后神经水肿恢复慢。
CTS手术治疗的主要目的是通过探查针对所见病变,采取相应措施,以增加腕管容积或减少腕管内容物体积,从而达到减少腕管内压力,解除正中神经受压的目的[9]。本组所选择的63例(75侧)患者均为腕横韧带压迫相对较轻,腕管内滑膜增生较重的患者,其中46例患者(50侧)获得3个月以上的临床随访。如表1所示,术前电生理检查显示神经传导速度降低相对较轻,而临床症状重,有明显的夜间麻醒病史。术中见明显的滑膜增生肥厚(图1),通过切开肥厚的腕横韧带,清除滑膜增生组织,增大腕管内容积而起到减压的目的。术后正中神经运动、感觉传导速度较术前改善,运动远端潜伏期、感觉远端潜伏期较术前缩短(表1)。术后随访显示,患者症状明显好转,优良率为92%(表2)。
内窥镜视下腕管松解术是近年来治疗CTS的一种新的方法,由于其切口小,局麻下就可以完成,所以被广大的患者所接受。但是,由于这种手术方法只能完成对于腕横韧带的切断,无法行腕管内广泛的滑膜清除及正中神经的松解,所以手术的范围受到了很大的限制,常常因为腕横韧带的松解不完全、滑膜清理不够彻底,而需要再次手术。此外内窥镜下腕管松解术还易于造成尺动脉、掌浅弓及第三指总神经损伤。这些因素都限制了内窥镜的使用[8,10]。
总结本组46例(50侧)滑膜型CTS患者住院资料:滑膜型CTS临床上以夜间痛、麻木、握物无力、桡侧三个半指掌侧感觉异常为主。神经电生理检查提示:神经源性损害,神经传导速度减慢,但是降低并不明显,行腕横韧带切开减压、腕管内滑膜切除、正中神经松解治疗可以取得良好的效果。
[1]刘华,董晖,杜永军.腕管综合征治疗分析[J].国际骨科学杂志,2011,32(6):400-401.
[2]林泉,刘志刚,于光.正中神经返支卡压及易损伤部位的解剖学基础[J].中国临床解剖学杂志,2005,23(1):76-78.
[3]顾雁浩,张凯莉,朱艺,等.探讨腕管综合征电生理分期的定量指标[J].中华手外科杂志,2004,20(3):145-147.
[4]顾玉东,王澍寰,侍德.手外科手术学[M].上海:复旦大学出版社,2010:530-531.
[5]陈彬,杨小辉,首家保,等.改良内窥镜微创治疗腕管综合征的疗效观察[J].现代中西医结合杂志,2012,21(4):371-372.
[6]史其林,薛峰,王金武,等.腕管综合征在内窥镜视下手术与常规手术的疗效比较[J].中华手外科杂志,2000,16(3):26-29.
[7]顾玉东,陈德松,史其林,等.腕管综合征128例分析[J].中华手外科杂志,2006,22(5):283-285.
[8]孟国成,陈立科,陈四华,等.三种手术方式治疗腕管综合征的临床优劣分析[J].中华手外科杂志,2011,27(4):246-247.
[9]郭建平,李立森,王玉发,等.老年腕管综合征的诊治[J].中国老年学杂志,2006,26(12):1718-1719.
[10]顾玉东,史其林,孙贵新.内窥镜下松解腕管综合征的神经并发症[J].中华手外科杂志,2003,19(3):151-152.
Surgical treatment of synovial hyperplasia carpal tunnel syndrome
LiJianqiang,JiangBaoguo,Chen Jianhai,FuZhongguo,WangTianbing.DepartmentofTraumaandOrthopedics,PekingUniversity People′sHospital,PekingUniversitytrafficMedicineCenter,Beijing100044,China
:WangTianbing,Email:wantianbing@medmail.com.cn
BackgroundCarpal tunnel syndrome is the most common compressive peripheral neuropathy,which is a couple of clinical syndromes caused by the oppression of the median nerve in the carpal tunnel.The tough of the transverse carpal ligament and thickness of its edge are the major factors in the oppression of the median nerve.Under normal circumstances,there is a large amount of tendon synovial in the carpal tunnel,which plays a role of nutrition and lubrication to the nerve.However,the tendon synovial hyperplasia,or even congestion and edema can cause or aggravate the oppression of the median nerve.Also,it will cause an inflammatory stimulate to the nerve.The major clinical manifestations of carpal tunnel syndrome are numbness and pain of three and a half fingers of the radial side.Usually,the pain radiates to the hand and forearm,accompanied with dysfunction of thumb opposition,thenar muscle atrophy and decreased grip and pinch strength.But in the synovial hyperplasia carpal tunnel syndrome,because of increased congestion at night and reflux disorder,there will be a significant night pain and numbness,which sometimes even makes the patients awake at a fixed time at night.These are the typical symptoms of synovial hyperplasia carpal tunnel syndrome.When the patients wake up,many will activate the fingers and wrists to relieve the pain,which promotes the synovial reflux in the carpal tunnel and reduces the pressure of carpal tunnel.As such reasons,there will be a phenomenon that clinical manifestations in the resting state do not fully meet the electrophysiological examination after activity.Patients who were diagnosed as synovial hyperplasia carpal tunnel syndrome were admitted to our hospital.We performed transverse carpal ligament release,carpal tunnel decompression,synovial tissue removal and median nerve release.The purpose of this study is to describe clinical characteristics of synovial hyperplasia carpal tunnel syndrome andanalyzes the outcome of treatment method adopted in this study.MethodsThere were 63patients(75 sides,left of 27cases and right of 48cases;51cases of one-side and 12cases bilateral;16males and 47females;aged 40-82years,mean 62years old;course of disease differ from 3months to 8years)included in the group.The time between onset of symptoms to treatment time differed from 3weeks to 2years.The etiology of the disease was as follows:49cases caused by chronic injury,14cases caused by autoimmune diseases(mostly bilateral)such as rheumatoid arthritis,gout,Sjogren syndrome and so on.There was no patient with a history of wrist trauma,fracture or dislocation.Also,there was no wrist tumor.The main symptoms of patients were wrist pain,numbness,weakness of grip and pinch and wake up at night caused by pain,which may radiated to the elbow and shoulder and had a relief by shaking the involved hands.The examination is as follows:wrist Tinel sign positive,paresthesia of three and a half fingers of the radial side and thenar muscle atrophy.The preoperative neurophysiological testing includes median nerve motor conduction velocity,sensory conduction velocity,motor distal latency and sensory distal latency.All patients
conservative treatment like preoperative non-steroidal anti-inflammatory drugs,local physical therapy and carpal tunnel drug injections.The treatment received a varying relief but soon the symptoms recurred,which affected the quality of life of patients so much that they came to the hospital to receive surgery.All patients underwent severing of transverse carpal ligament,synovial removal of the carpal tunnel and release of the median nerve.Procedures:All patients were narcotized with brachial plexus anesthesia,and then we will make the patient supine,limb abduction.Use the tourniquet and turn the pressure at 300mmHg.Disinfection and drape routinely,and then make an arc-shaped incision between the midpoint of thenar crease to the wrist crease line,which is 3cm long.After cutting the skin,subcutaneous tissue and fascia layer of the palm,cut the transverse carpal ligament at the level of the wrist crease line.We should cut the transverse carpal ligament proximally under direct vision.In the process,we should prevent damage to the underlying median nerve until the transverse carpal ligament is fully cut.At the midpoint thenar crease and beyond care should be taken to avoid damage to the recurrent branch of the median nerve.During the operation,we can see:the transverse carpal ligament thickened;median nerve is compressed under the transverse carpal ligament;the nerve becomes flat and the outer membrane thickened;the color of the compressed part is dark;visible neurovascular interruption;nerve surrounded by scars;flexor digitorum deep tendons and flexor digitorum superficial tendons are wrapped by a large amount of synovial tissue.After cutting the transverse carpal ligament,separate the median nerve and decide whether to release the outer membrane according to degree of nerve entrapment and hyperplasia.If releasing the outer membrane of nerve is decided,release the hyperplasia tissue around the nerve using microsurgical scissors,cut the involved out membrane of median nerve longitudinally until soft normal nerve is revealed,which means a complete release.Protect the median nerve strictly;separate the flexor digitorum deep tendons and flexor digitorum superficial tendons;carefully remove the hyperplastic lesions of synovial tissue.Loose the tourniquet,stanch strictly,indwell drainage strip,suture the fascia layer of the palm and then make a full thickness suture.The resected synovial tissue surrounding the tendon should be sent to receive a pathologic examination.Postoperative treatment:Drainage strip should be removed within 24hours after surgery;do the finger flexion and dorsiflexion activities under the guidance of a doctor to prevent tendon adhesions;elevate the affected limb at night to reduce swelling;stitches the wound 14days after surgery;take methycobal for 3weeks;exercise normally 4-6weeks after surgery.Clinical criteria:We use the Kelly standard to evaluate the effect of treatment 3months after surgery.The details are as follows:excellent:the symptoms disappeared completely;good:the symptoms were relieved significantly;general:symptoms become mild or continued;poor:symptoms unchanged or be worse.All patients received neurophysiological testing during follow-up.Statistical Analysis:The data is statistically analyzed using SPSS software.We use two independent samples t-test analysis and makeP<0.05significant differences.ResultsThere are a total of 46patients(50sides)who received a more than 3months clinical follow-up and the average time of follow-up is 4.6months.The symptoms of hand numbness,pain all hada varying relief and the symptom of anesthesia at night disappeared.The Incision healed well,and there was no long-term complications such as infection and nonunion.There was no scar contracture.No one complained of recurrence 3-12months after operation.No patient was present with injury of median nerve,the superficial palmar arch or recurrent branch of the median nerve.During the operation,we can see the synovial tissue hyperplasia around the median nerve,which cause the compression of the median nerve.The postoperative pathological examination shows edema and degeneration of the fibrous connective tissue around the median nerve,hyperplasia of the synovial tissue,infiltration of the lymphocyte and plasma cells.Preoperative electrophysiological tests showed there is no significant reduction of median nerve motor or sensory conduction velocity,(48.32±3.68)m/s and(46.32±3.68)m/s,respectively.There are 50sides which received electrophysiological tests 3months after operation and the tests showed that the median nerve motor and sensory conduction velocities were bigger than the preoperative velocities,(51.64±2.70)m/s and (50.11±3.47)m/s,respectively.There is a significant difference(t=-6.095,-2.935,allP<0.05).The median nerve motor distal latency of(4.38±0.40)ms is reduced to (3.47±0.27)ms,and the sensory distal latency of(5.12±0.36)ms is reduced to (4.14±0.31)ms,with a significant difference(t=15.895,16.011,allP<0.05).According to the Kelly standard,there are 32sides of excellent,whose night pain and numbness of the fingers disappeared completely;there are 14sides of good,whose night pain,numbness of the fingers relieved significantly than before but not completely disappeared;there are 4sides of general and no side of poor.Over all,the proportion of excellent is 92%.ConclusionsAs a summary,from the data of this 46 patients(50sides)with synovial hyperplasia carpal tunnel syndrome,we can see that the main clinical manifestations of synovial hyperplasia carpal tunnel syndrome are pain,numbness and inability to grip at night,paresthesia of three and a half fingers in the radial sides.The neurophysiological examinations show neurogenic damage,mild decrease of nerve conduction velocity.The way of transverse carpal ligament revering,synovial removal within the carpal tunnel and median nerve release therapy can achieve a good result.
Carpal tunnel syndrome; Nerve electrophysiological examination; Carpal transverse ligament severing;Median nerve release
2014-03-11)
(本文编辑:李静)
10.3877/cma.j.issn.2095-5790.2014.02.007
卫生公益性行业科研专项(201002014);教育部创新团队(IRT1201)
100044 北京大学人民医院创伤骨科 北京大学交通医学中心
王天兵,Email:wangtianbing@medmail.com.cn
李建强,姜保国,陈建海,等.滑膜增生型腕管综合征的手术治疗[J/CD].中华肩肘外科电子杂志,2014,2(2):103-108.
猜你喜欢
舰船科学技术(2022年10期)2022-06-17 06:26:42
建材发展导向(2021年14期)2021-08-23 00:57:20
广东医科大学学报(2020年6期)2020-02-06 06:00:58
西南石油大学学报(自然科学版)(2019年4期)2019-11-04 00:34:28
中国组织化学与细胞化学杂志(2016年3期)2016-02-27 11:15:41
江西理工大学学报(2015年3期)2015-12-22 05:26:22
实用手外科杂志(2015年4期)2015-08-27 01:54:22
天津医科大学学报(2015年3期)2015-06-05 12:21:49
西南军医(2015年4期)2015-01-23 01:19:30
西南医科大学学报(2014年6期)2014-03-20 15:43:47
