
双排锚钉桥式缝合在肱骨大结节骨折中的应用
2014-07-05 13:14:09张少战黄长明傅仰攀董辉详甘志勇
中华肩肘外科电子杂志 2014年2期
张少战 黄长明 傅仰攀 董辉详 甘志勇
双排锚钉桥式缝合在肱骨大结节骨折中的应用
张少战 黄长明 傅仰攀 董辉详 甘志勇
目的探讨双排锚钉在肱骨大结节骨折有限切开复位内固定中应用的临床价值。方法自2010年3月至2013年3月,对10例单独大结节骨折患者通过有限切开复位,双排锚钉桥式缝合内固定治疗肱骨大结节移位骨折。术后随访,复查X线片评价复位情况,以Constant评分和UCLA评分评价肩关节功能。结果所有患者术后均获得解剖复位。在平均12.3个月的随访中,X线片显示复位无丢失,骨折获得愈合,Constant评分平均90.3分,UCLA评分平均32.2分。结论双排锚钉内固定治疗单纯移位的肱骨大结节骨折效果可靠。
肱骨骨折,大结节;锚钉
肱骨近端骨折占全身骨折的5%,其中单独的肱骨大结节骨折占20%[1],可伴或不伴盂肱关节脱位,在Neer分型上属于2部分肱骨近端骨折,在AO分型上为11-A1.2或11-A1.3。自2010年3月至2013年3月对10例肱骨大结节撕脱骨折患者采用双排锚钉缝合方法进行内固定,取得了较好效果。
材料和方法
一、一般资料
肱骨大结节骨折患者10例,其中男性4例,女性6例,年龄41~63岁,平均48.2岁。致伤原因:摔伤8例,车祸2例,其中伴盂肱关节前脱位3例。伤后肩关节X线片提示肱骨大结节骨折移位均>0.5cm。
二、方法
盂肱关节脱位患者均急诊予局麻下手法复位。所有患者于伤后2~21d,平均10d获得有限切开复位,双排锚钉内固定手术。具体术式为:肩关节前外侧纵向经三角肌入路,切口避免超过肩峰远侧5cm,以免造成腋神经损伤。通过旋转肩关节充分暴露大结节骨块及骨折床,清理骨床,临时复位骨折块,选择置钉点,于骨床近端偏前、后侧接近肱骨头关节面分别拧入Twinfix锚钉2枚作为内侧锚钉,通过缝针或过线器将缝线带过骨折块近端附着之肩袖组织,打结固定,于骨床远端内外侧拧入footprint锚钉作为外侧锚钉,将内侧锚钉之尾线成编织状覆盖卡入footprint锚钉内(图1、2)。术后予颈腕吊带悬吊固定2周,期间开始肩关节被动钟摆练习。6周后开始外展、前屈过90°练习。

图1 内排锚钉置入后准备装入Footprint锚钉
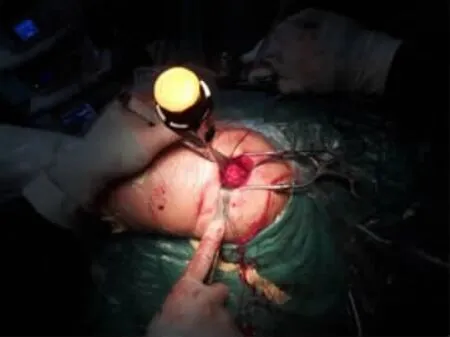
图2 外排Footprint置入
三、随访及评价方法
本组所有患者均获得门诊随访,术后随访时间7~18个月,平均12.3个月。术后及随访时拍摄普通肩关节正侧位X线片评价复位及愈合情况。以肩关节Constant评分与加州大学洛杉矶分校肩关节UCLA评分评价肩关节功能,采用SPSS 13.0软件计算均值。
结 果
术中发现,10例患者中有5例骨折块为粉碎性骨折,骨块之间为骨膜、肩袖软组织附着,故骨块彼此之间均无明显分离。所有10例患者骨折范围均不超过大结节,骨块厚度均不超过0.8cm。所有患者伤口均获得一期愈合。肩关节X线片均提示:术后骨折端获解剖复位(图3)。术后随访无复位丢失,均获骨性愈合。随访终末Constant评分平均90.3分(85~100分),UCLA 评分平均32.2分(28~35分)。

图3 术后X线片示骨折端已获解剖复位
讨 论
肱骨大结节骨折向外上方移位,使肩峰下间隙变窄,可能引起肩部撞击症和肩袖撕裂[2]。早在1959年McLaughlin即指出大结节上移0.5cm即应手术治疗,Platzer等[3]认为移位<0.5cm 的大结节骨折可不需手术治疗。Park等[4]于1997年提出,对于运动员或需要手臂过头的体力劳动者,大结节骨块发生0.3cm的移位也应当手术复位。肱骨大结节骨折畸形愈合,可能影响肩袖及三角肌力量,从而影响肩关节旋转功能及外展等[5]。大结节撕脱骨折可伴随着肩袖损伤,可引起将来骨折愈合后的疼痛[6]。Kim等[7]一组X线片上平均移位为2.3mm的肱骨大结节骨折患者的关节镜手术中,发现其后期慢性疼痛与肩袖部分损伤有关。手术治疗大结节撕脱骨折,可以处理肩袖损伤,避免肩峰下撞击[8]。目前一般认为单独的肱骨大结节骨折移位>0.5cm具有手术指征,对于活动要求高的年轻人或运动员手术指征可进一步放宽,当然这仍有争议[9]。
对于大结节骨折,传统的术式有空心钉或螺钉固定。我们既往在术中发现因大结节骨折片较薄弱,单纯依靠螺钉钉尾压迫致骨片碎裂,导致固定不可靠或术中固定失效。而对于粉碎性大结节骨折,不论是空心钉或螺钉均将无法获得有效固定。也有应用钢板及微型钢板固定,同样存在骨片碎裂问题,若采用“跨越”固定,可能出现肩峰撞击的风险。为克服这些问题,曾有人应用编织缝合肩袖经骨隧道固定方法治疗大结节骨折,但经骨道固定易出现缝线在骨隧道的磨损致固定失败;也有人应用空心钉固定结合锚钉方法,但对于大结节粉碎性骨折不适用,也同样面临着骨片劈裂致空心钉失效情况。
大结节骨折可被认为是肩袖的撕脱骨折[10]。不论是关节镜下修补或是开放性修补,锚钉缝合已成为公认的修补肩袖损伤的有效固定,因而应用锚钉缝合完全可满足维持大结节骨折复位的力学要求。有实验表明,在大结节骨折,应用锚钉的力学稳定性优于单纯应用螺钉或空心钉[11],也优于经骨道固定[12]。现有研究认为双排锚钉桥式缝合修补肩袖损伤有助于增大肩袖附着面积,从而有利于肩袖损伤修复[13-14]。所以双排锚钉缝合可应用于大结节骨折,我们在临床上也获得了满意效果。
锚钉缝合公认的薄弱点在于缝线断裂、钉尾线孔破坏及螺钉拔出。锚钉的置入应注意指向撕脱方向,以期减小缝线的拔出角,减少锚钉的拔钉应力。一般认为应使缝线方向与锚钉纵轴垂线的夹角(即拔出角)<45°。锚钉缝线对于肩袖肌腱的切割可能是固定失败的另一重要原因[15]。可以通过增加缝合的针数来分担减小相应的切割力量。通过增加锚钉数是一种方法,但是有限的骨床不可能置入过多锚钉,锚钉之间的距离过近,将造成骨质的进一步丢失,而造成锚钉脱拔或是骨折。那么通过增加单枚锚钉的缝线数就成为一种选择。Twinfix具有两根互不干扰的尾线,可满足上述要求。有力学研究表明,2枚双线锚钉较3枚单线锚钉可能更强[16]。通过骨床近、远端的双排锚钉置入,在撕脱骨块表面缝线交织成网状均匀将骨折块压向骨床更有利于术后骨折块复位的维持。双排锚钉可分担应力,具有更好的力学可靠性,较单排锚钉更具有优势[17-19]。
我们的体会是,双排锚钉固定可应用于肱骨大结节撕脱骨折,耗材较昂贵,加重患者的经济负担,但是对于粉碎性肱骨大结节骨折仍是不错的选择。另外,对于要求将来取出内固定的患者,锚钉将不适用。有文献指出,在骨质疏松患者肩袖修补术或大结节骨折内固定术中应用锚钉固定存在锚钉拔出的可能[20],故对于骨质疏松患者应用锚钉固定有一定的顾虑。
目前关节镜下双排锚钉修复肩袖损伤已日益成熟,那么作为肩袖撕脱骨折的大结节骨折也可在关节镜下行复位双排锚钉固定。肩关节镜下手术手术切口较小,软组织剥离更少,术后黏连发生更少,当然这需要有更精巧的肩关节镜技术[21]。
[1]Gruson KI,Ruchelsman DE,Tejwani NC.Isolated tuberosity fractures of the proximal humerus:current concepts[J].Injury,2008,39(3):284-298.
[2]Fahmy A,Antonakopoulos N,Khan A.Acromial impression fracture of the greater tuberosity with massive rotator cuff tear:this need not be a nightmare[J].BMJ Case Rep,2011,3521.
[3]Platzer P,Kutscha-Lissberg F,Lehr S,et al.The influence of displacement on shoulder function in patients with minimally displaced fractures of the greater tuberosity[J].Injury,2005,36(10):1185-1189.
[4]Park TS,Choi IY,Kim YH,et al.A new suggestion for the treatment of minimally displaced fractures of the greater tuberosity of the proximal humerus[J].Bull Hosp Jt Dis,1997,56(3):171-176.
[5]Bono CM,Renard R,Levine RG,et al.Effect of displacement of fractures of the greater tuberosity on the mechanics of the shoulder[J].J Bone Joint Surg Br,2001,83(7):1056-1062.
[6]George MS.Fractures of the greater tuberosity of the humerus[J].J Am Acad Orthop Surg,2007,15(10):607-613.
[7]Kim SH,Ha KI.Arthroscopic treatment of symptomatic shoulders with minimally displaced greater tuberosity fracture[J].Arthroscopy,2000,16(7):695-700.
[8]Yin B,Moen TC,Thompson SA,et al.Operative treatment of isolated greater tuberosity fractures:retrospective review of clinical and functional outcomes[J].Orthopedics,2012,35(6):e807-e814.
[9]Mattyasovszky SG,Burkhart KJ,Ahlers C,et al.Isolated fractures of the greater tuberosity of the proximal humerus:a long-term retrospective study of 30patients[J].Acta Orthop,2011,82(6):714-720.
[10]Bahrs C,Lingenfelter E,Fischer F,et al.Mechanism of injury and morphology of the greater tuberosity fracture[J].J Shoulder Elbow Surg,2006,15(2):140-147.
[11]Lin Chengli,Hong CK,Jou IM,et al.Suture anchor versus screw fixation for greater tuberosity fractures of the humerus- -a biomechanical study[J].J Orthop Res,2012,30(3):423-428.
[12]Salata MJ,Sherman SL,Lin EC,et al.Biomechanical evaluation of transosseous rotator cuff repair:do anchors really matter[J].Am J Sports Med,2013,41(2):283-290.
[13]Baums MH,Geyer M,Büschken M,et al.Tendon-bone contact pressure and biomechanical evaluation of a modified suture-bridge technique for rotator cuff repair[J].Knee Surg Sports Traumatol Arthrosc,2010,18(7):992-998.
[14]Zhang Q,Ge H,Zhou J,et al.Single-row or double-row fixation technique for full-thickness rotator cuff tears:ameta-analysis.PLoS One,2013,8(7):e68515.
[15]Barber FA,Drew OR.A biomechanical comparison of tendon-bone interface motion and cyclic loading betweensinglerow,triple-loaded cuff repairs and double-row,suturetape cuff repairs using biocomposite anchors.Arthroscopy,2012,28(9):1197-1205.
[16]Kamath GV,Hoover S,Creighton RA,et al.Biomechanical analysis of a double-loaded glenoid anchor configuration:can fewer anchors provide equivalent fixation[J].Am J Sports Med,2013,41(1):163-168.
[17]Baums MH,Spahn G,Buchhorn GH,et al.Biomechanical and magnetic resonance imaging evaluation of a single-and double-row rotator cuff repair in an in vivo sheep model[J].Arthroscopy,2012,28(6):769-777.
[18]Kulwicki KJ,Kwon YW,Kummer FJ.Suture anchor loading after rotator cuff repair:effects of an additional lateral row[J].J Shoulder Elbow Surg,2010,19(1):81-85.
[19]Baums MH,Buchhorn GH,Gilbert F,et al.Initial load-tofailure and failure analysis in single-and double-row repair techniques for rotator cuff repair[J].Arch Orthop Trauma Surg,2010,130(9):1193-1199.
[20]徐圣康,罗斌,赵猛,等.Anchor结合Krackow缝合法在肱骨大结节骨折及肩袖损伤中应用的疗效观察[J/CD].中华临床医师杂志(电子版),2012,6(13):3793-3794.
[21]Wang Yongping,Zhao Jinzhong,Huangfu Xiaoqiao,et al.Arthroscopic reduction and fixation for isolated greater tuberosity fractures[J].Chin Med J,2012,125(7):1272-1275.
Double-row suture anchor fixation of displaced greater tuberosity fractures
ZhangShaozhan,Huang Changming,FuYangpan,DongHuixiang,GanZhiyong.DepartmentofOrthopaedicWard2,the 174thHospitalofPeople′sLiberationArmy,OrthopedicsCenterofNanjinMilitaryDistrict,Xiamen361003,China
:HuangChangming,Email:huangchm123@163.com
BackgroundAmong the proximal humeral fractures,the incidence of isolated fractures has been reported to be approximately 14%to 21% .In addition,during rotator cuff injury,as a result of a strong pulling power,fractures of the greater tuberosity occur frequently during avulsion fracture of the rotator cuff.Particularly,a strong external rotation power acts on the greater tuberosity,and thus avulsion fracture may occur during anterior shoulder dislocation.Some authors have reported that greater tuberosity fractures were associated with approximately 10%to 30%of shoulder joint dislocation cases.Several arthroscopic and open techniques utilizing screws,wire or sutures through bone have been described for reduction and internal fixation of the greater tuberosity to the proximal humerus.But these are often inadequate in the presence of comminution and may prevent accurate restoration of the tuberosity-head relation.Bhatia have performed open reduction–internal fixation by use of the double-row suture anchor fixation technique in 21cases of comminuted and displaced fractures of the greater tuberosity,and the long-term results suggest a satisfactory outcome in most patients.However,the retrospective study or follow-up data about the surgical treatment of displaced humeral greater tuberosity fractures is still very limited.The purpose of this retrospective study is to evaluate the therapeutic outcomes of the open reduction and internal fixation using double-row fixation with suture anchors for the treatment of humeral greater tuberosity fractures.MethodsThe study included 10patients with isolated greater tuberosity fractures.The cases were reviewed at a mean post-operative follow-up duration is 12.3months(range from 7to 18months)from 2010to 2013.The average age of the patients was 48.2years old(range:41to 63years old),including 4males and 6 females.Among them,3patients were associated with anterior dislocation of the shoulder joint.All radiographs were examined by a single observer.The displacement was more than 5mm in X-ray plain film.All patients were operated by a single surgeon and with the same surgical technique.All the patients were treated by double-row anchor suture fixation through a mini-open approach and the operations were carried out in 2to 21days after trauma.The skin incision was made in Langer’s linesjust medial to the anterolateral aspect of the acromion.The deltoid was split from the anterolateral corner of the acromion distally for 4-5cm,without detaching the origin of the deltoid.The greater tuberosity fragment with the attached cuff was located and tagged with traction sutures through the cuff tendon.After the fractured bone surface on the proximal humerus was cleared of soft tissue,and two anchors(TwinFix)were inserted at the proximal margin of the humeral fracture surface.The strands of each suture were passed through the tendinous part of the attached cuff.The sutures were tied as mattress sutures with the arm in a neutral position.A second row of suture-anchors was passed distal to the humeral fracture surface.Two sutures were passed through the tendon between the first row of mattress sutures and the bone fragments.The strands from these two sutures were used to buttress the greater tuberosity fragments to the proximal humerus by tying these to four strands from the second row of anchors.The arm was suspended by a strap for 2weeks postoperatively,during which the shoulder started to do the pendulum exercise passively.Then they were required to do the abduction and flexion exercise over 90°after 6weeks.The patients were evaluated by interview,physical examination,and radiographs at 7-18months,with a mean follow-up of 12.3months.Details of complications and additional procedures were obtained from the clinical and operative records of the patients.The reductions and healing condition of the fractures were assessed by X-ray examination postoperatively.Then we use the Constant Score and UCLA shoulder rating scale to evaluate the function of shoulders.ResultsAccording to the intro-operative findings in the ten patients,five of them were communicated fracture,and there were soft tissues,such as periosteal membrane and rotator cuff,connecting the fractured fragments.Therefore,there is not significant separation between the fragments if the soft tissue around was properly protected during the exposure of fracture site.Moreover,the affected fracture area of the ten patients did not go over the greater tuberosity and the thickness of all the fracture fragments was within 0.8cm.All the patients’wound got healed.The X-ray showed an anatomic reduction with no re-displacement during the follow-up.Radiographic union of the tuberosity below the level of the articular surface of the humeral head was seen in all of 10 fractures.There was no heterotopic bone formation in any patient.All patients with radiographic union were satisfied with the outcome and the overall mean Constant score was 90.3and the final mean UCLA score was 32.2.There were no neurological complications,infections or complications of wound healing.ConclusionsGreater tuberosity fracture are well described and frequently discussed.They can be considered as an avulsion fracture of the rotator cuff.Suture anchors have recognized as an effective fixation of rotator cuff injury.The double-row anchors are more mechanically reliable,compared with single-row anchors.This technique has several advantages:First,biomechanical and clinical evaluation of the double-row fixation technique in arthroscopic rotator cuff repair has demonstrated significantly better biomechanical properties and structural outcome compared to other techniques;Second,proximal mattress sutures accurately restore the tuberosity-head relationship by approximating the bone-tendon junction to the proximal edge of the humeral fracture surface;Third,proximal fixation repairs the partial-thickness articular-surface tears of the supraspinatus tendon which may be associated with greater tuberosity fractures;Fourth,distal sutures serve as a tension band to effectively buttress the tuberosity fragments against the humeral fracture surface.The application of double-row anchors is clinically effective to treat the displaced greater tuberosity fractures.With the development of arthroscopic techniques,the outcome of double-row anchor suture fixation under arthroscopy is really to be expected.
Humerus fractures,greater tuberosity;Anchors
2014-01-16)
(本文编辑:李静)
10.3877/cma.j.issn.2095-5790.2014.02.003
361003 厦门,南京军区骨科中心 解放军一七四医院骨二科
黄长明,Email:huangchm123@163.com
张少战,黄长明,傅仰攀,等.双排锚钉桥式缝合在肱骨大结节骨折中的应用[J/CD].中华肩肘外科电子杂志,2014,2(2):80-84.
猜你喜欢
人人健康(2022年4期)2022-11-25 11:12:58
运动精品(2022年1期)2022-04-29 08:58:08
中华养生保健(2020年4期)2020-11-16 01:31:00
瞭望东方周刊(2015年46期)2016-04-01 00:25:55
体育科技(2016年2期)2016-02-28 17:06:03
中华肩肘外科电子杂志(2016年3期)2016-01-23 07:18:59
转化医学电子杂志(2015年4期)2015-12-27 12:17:00
实用手外科杂志(2015年3期)2015-08-27 01:53:20
实用手外科杂志(2015年1期)2015-08-27 01:51:58
中国医疗美容(2015年1期)2015-07-12 10:06:37
