
An overview of travel-associated central nervous system infectious diseases: risk assessment, general considerations and future directions
2014-03-22 13:01:24MortezaIzadiArmanIshaqiMohammadAliIshaqiNematollahJonaidiJafariFatemehRahamatyAbdolaliBanki
Morteza Izadi, Arman Is’haqi, Mohammad Ali Is’haqi, Nematollah Jonaidi Jafari, Fatemeh Rahamaty, Abdolali Banki
1Baqiyatallah Hospital, Baqiyatallah University of Medical Sciences, Tehran, Iran
2Department of Neurology, Tehran University of Medical Sciences, Tehran, Iran
3Department of Infectious Diseases, Rasoul Akram Hospital, Iran University of Medical Sciences, Tehran Iran
4Department of Neurology, Baqiyatallah University of Medical Sciences, Tehran, Iran
An overview of travel-associated central nervous system infectious diseases: risk assessment, general considerations and future directions
Morteza Izadi1*, Arman Is’haqi2, Mohammad Ali Is’haqi3, Nematollah Jonaidi Jafari1, Fatemeh Rahamaty1, Abdolali Banki4
1Baqiyatallah Hospital, Baqiyatallah University of Medical Sciences, Tehran, Iran
2Department of Neurology, Tehran University of Medical Sciences, Tehran, Iran
3Department of Infectious Diseases, Rasoul Akram Hospital, Iran University of Medical Sciences, Tehran Iran
4Department of Neurology, Baqiyatallah University of Medical Sciences, Tehran, Iran
PEER REVIEW
Peer reviewer
Dr. Xiaobo Liu, Department of Vector Biology and Control, State Key Laboratory for Infectious Diseases Prevention and Control, National Institute for Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Changbai Road, Changping District, Beijing 102206, P. R. China.
Tel: (+86) 134 0117 8048
Fax: (+86) 010 5890 0739
E-mail: liuxiaobo@icdc.cn
Comments
This is a valuable review work in which authors highlighted some important aspects of travel-related illnesses from a neurological point of view. These aspects mainly includes risk assessment, general considerations and future directions. Recommendations with regard to knowledge gaps, and state-of-the-art research are made. Given an increasing number of international travelers, novel dynamic ways are available for physicians to monitor the spread of CNS infections.
Details on Page 594
Nervous system infections are among the most important diseases in travellers. Healthy travellers might be exposed to infectious agents of central nervous system, which may require in-patient care. Progressive course is not uncommon in this family of disorders and requires swift diagnosis. An overview of the available evidence in the field is, therefore, urgent to pave the way to increase the awareness of travel-medicine practitioners and highlights dark areas for future research. In November 2013, data were collected from PubMed, Scopus, and Web of Knowledge (1980 to 2013) including books, reviews, and peer-reviewed literature. Works pertained to pre-travel care, interventions, vaccinations related neurological infections were retrieved. Here we provide information on pre-travel care, vaccination, chronic nervous system disorders, and post-travel complications. Recommendations with regard to knowledge gaps, and state-of-the-art research are made. Given an increasing number of international travellers, novel dynamic ways are available for physicians to monitor spread of central nervous system infections. Newer research has made great progresses in developing newer medications, detecting the spread of infections and the public awareness. Despite an ongoing scientific discussion in the field of travel medicine, further research is required for vaccine development, state-of-the-art laboratory tests, and genetic engineering of vectors.
Travel medicine, Infectious diseases, Nervous system disorders
1. Introduction
An estimate of 938 million people had international travels in 2010 with an increase of 3% in 2013[1]. Travellers are inevitably exposed different illnesses[2]. Therefore there is an increasing number of travelers that need risk assessment prior to their travel in order to perform suitable precautions and avoid complications during overseas travels. Such illnesses, albeit self-limiting to a large extent, affect up to a three-quarter of young travelers[3]. Moreover,individuals traveling to resource-limited destinations should be encouraged to seek pre-travel advice and risk assessment; mainly because the risk for illness is increased in such regions with limited advanced medical care[4,5] and more than a half of them do not seek pre-travel advices[2]. Thus, primary care physicians should be equipped with appropriate knowledge of destination-specific diseases, routine vaccines, chemoprophylaxis regimens, and selftreatment regimens for infectious and non-infectious illnesses[5,6]. In complex travelers, practitioners should advise on seeking specialized travel-medicine care, as travellers might not be aware of them.
More importantly, central nervous system (CNS) may be affected by various travel-associated pathogens[7]. CNS disorders may also need a comprehensive risk assessment, which involves detailed data gathering strategies[8,9]. Equally important are people affected with chronic CNS disorders (e.g.multiple sclerosis, epilepsy, brain tumors, post-surgical complications andetc.) that may require more comprehensive pre-travel care. All of these conditions need state-of-the-art travel health prevention and intervention strategies. However, data on travel-associated health problems in general, and neurological disorders in particular, are scarce and further work is urgently needed to organize the current evidence and shed light on the areas that require further research. Complicating factors such as increasing number of travellers, drug resistant organisms and newly emergent infections poses a major challenge with respect to travel-medicine interventions[10].
Therefore, an review need to be set out to the state-ofthe-art evidence in the field, to present comprehensive overview on important CNS diseases in travel and finally to provide invaluable insights regarding research areas underrepresented in the current literature of the travel medicine.
2. Pre-travel risk assessment
Risk assessment is the process of gathering detailed information on host factors, travel characteristics and environmental factors. Travellers’ underlying conditions (e.g.chronic conditions), season of travel, destination (including region, types of available accommodation, and season of travel), purpose of travel and duration, social history, risk-taking behaviors and previous travel experience that all should be assessed and properly addressed[2]. All the required information should be collected at least 6-8 weeks from the scheduled travel. It starts even before face-to-face consultation by filling a relevant questionnaire[11]. Previous health record obtained in general practice may also be helpful. Risk assessment largely determines the nature of advice needed for the travellers and whether intervention would be necessary.
Familiarity, visibility and controllability of a hazard determines its risk that should be weighed against the cost of intervention in travel medicine[11]. Risk-assessment includes both the assessment of risk of the destination (Table 1) and the risk of the individual traveller (Table 2). This should be addressed from prevention to education and a final management[11]. High-risk travellers with regard to important CNS infections can be found in Table 2. Figure 1 shows the crosstalk between hazards, exposures, susceptibility of the individual traveller that necessitates risk assessment, risk management and appropriate travel medicine intervention. Environmental factors are dynamic processes and travellers should seek new information through available real-time resources (See Table 2 for further details). Notwithstanding in a survey of 2 000 travellers, 70% had not sought pre-travel advice[12] and most of those who seek advice do so with usual practitioners who are not travel-medicine experts[13]. Even when travellers seek pre-travel advice, their adherence to travel medicine recommendations remain=s suboptimal[14]. Future research should address refined strategies to increase pre-travel care awareness. Moreover, more accessible and affordable pre-travel care (e.g.through social media) could eventually reduce travel associated morbidity and mortality[15].

Table 1 Environmental risk factors (with respect to neurological infections).
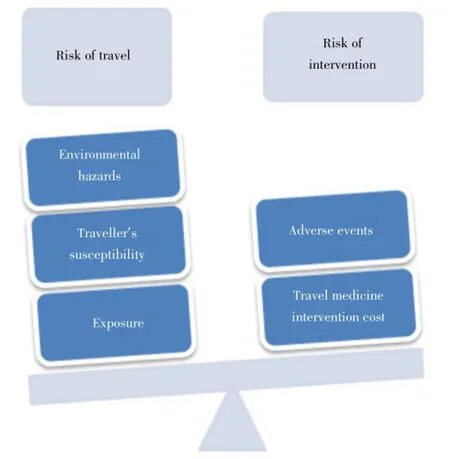
Figure 1. Risks of travel should be weighed against risk of intervention.
Risks associated with mode of travel play an important role in the risk assessment. Pre-existing neurological conditions, recent neurosurgical interventions and mental impairmentall require consultation prior to fly with commercial aircrafts. Long flights can predispose travellers to barotrauma, jet lag, deep vein thrombosis, panic attacks, claustrophobia and increase the effect of alcohol on passengers[11]. Also, prolonged exposure to infectious agents plays an important role in person-to-person transmissions in longer flights.
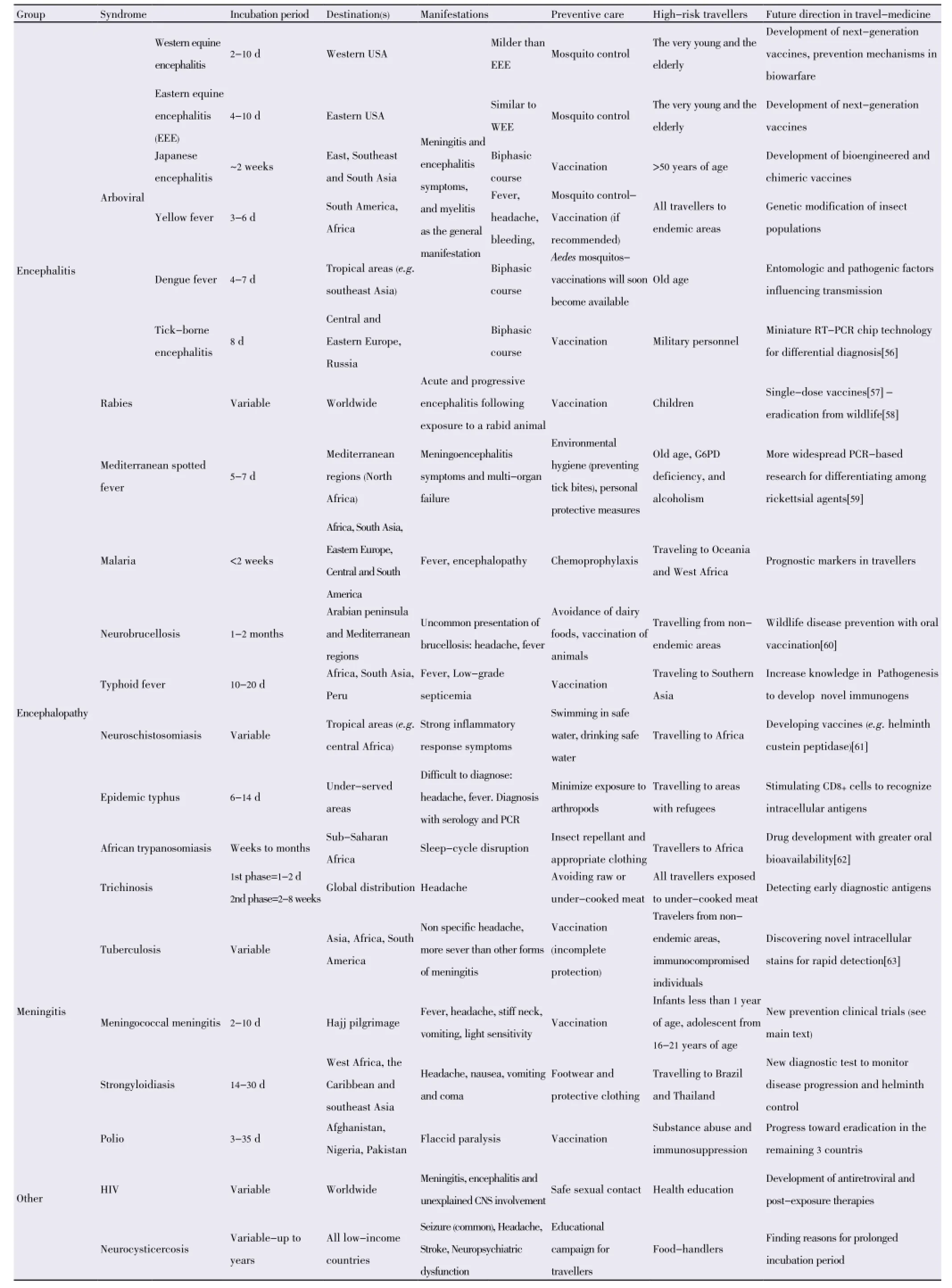
Table 2 Notable travel-associated CNS infectious diseases.
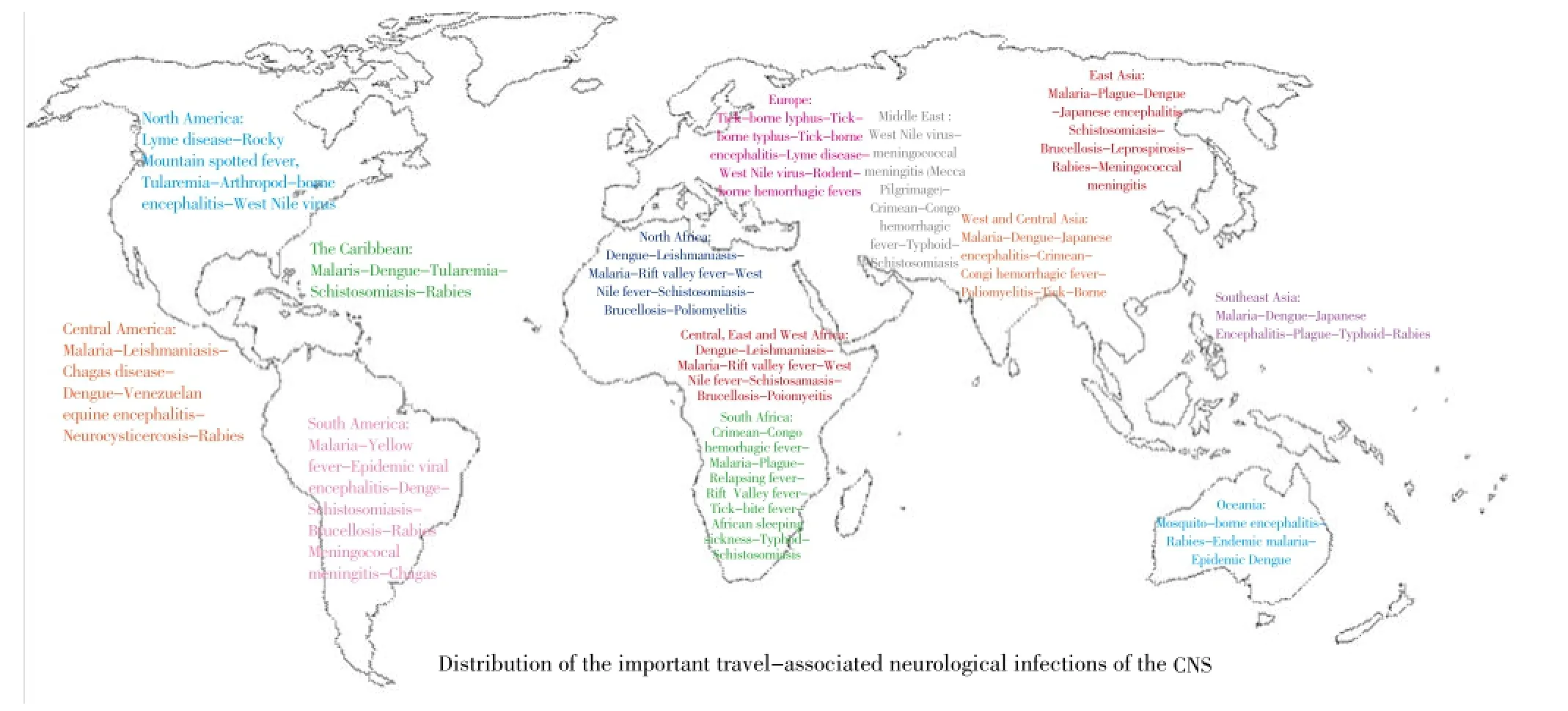
Figure 2. Common CNS infections and their geographical distribution.
3. Vaccination
Pre-travel evaluation of travellers often addresses vaccination that depends on the risk of travellers’ health, itinerary and destination. Vaccine-preventable sicknesses are shown in Table 2. Guidelines are available for required vaccines based on specific destinations[16] as well as season of the planned travel. Decision of taking vaccines might depend on various factors: duration of the stay, availability of post-exposure care (e.g., rabies immunoglobulin), age, and the purpose of travelling. All travellers should be up to date with regard to routine vaccinations. A recent study showed that approximately a third of travellers need pretravel consultation for completing routine vaccination (Yellow fever is the most frequently administered vaccine, followed by hepatitis A, typhoid fever, and meningococcal vaccine)[17]. Meningoccal meningitis is the most common CNS-vaccine preventable disease seen in unvaccinated travellers (0.04-200 per 100 000 unvaccinated persons)[18]. Individuals travelling to ‘meningitis belt’ in Africa in dry season are strong candidates for receiving the vaccine[19]. High-risk individuals for invasive meningitis should receive conjugate tetravalent vaccine (or pentavalent vaccine if available)[19]. Conjugate vaccines are preferable to polysaccharide vaccines as they provide a longer immunization and decreases the rate of nasopharyngeal shedding of the bacteria[20].
Dengue is the most common arthropod-borne virus in the world[21]. Dengue fever is common in returning individuals from Southeast Asia, a GeoSentinel survey showed that the possibility of infection with dengue fever in this group was more than that with malaria[22]. Several vaccines are underdevelopment and until such time preventive measures play the most important role[21]. Live attenuated viral vaccines that need to address all four subtypes of this virus introduce new challenges that have previously hampered the efforts of researchers. Vaccines that passed the latest stages of clinical trials have successfully addressed the challenge of minimal pathogenicity and maximal immunogenicity among all serotypes[21]. Chimera Vax is a promising vaccine that introduces 4 recombinant viruses on yellowfever virus backbone[23]. This vaccine can induce ample immunogenicity with administration at 0, 6 and 12 months to dengue 1 to 4 with a good safety profile[21,24].
Typhoid fever, tick-borne encephalitis, rabies and Japanese encephalitis may also be seen in unvaccinated travellers[18]. Between 1973 and 2008 only 55 cases were reported in non-endemic countries with an estimated risk of less than 1 in 1 million travellers[25]. Despite its rare prevalence in returning travellers, its serious consequences have increase the researchers’ interest in vaccination. Vaccination against Japanese encephalitis should be recommended to all long-term and repeat travellers and to expatriates going to areas of Asia where the disease is endemic[26] although the proportion of high-risk travellers that receive Japanese encephalitis vaccine remains low[27].
The GeoSentinle survey on 320 cases from 1988 to 2005 showed that animal bites are not uncommon in returning travellers with short travel duration, especially when traveling to Asia[28]. Pre-exposure vaccinations remain controversial and depend on endemicity in the destination and availability of medical care in the destination country[29]. Intra-dermal route of pre-exposure vaccination may be beneficial for travellers[29].
Influenza remains the most common vaccine preventable disease in travellers[30]. Influenza and pneumococcal vaccines should also be considered among older travellers[31]. Yellow fever vaccination for travellers to non-endemic areas is not generally recommended. However, travellers with increased risk of mosquito bites and prolonged travellers necessitates vaccination in a small group of travellers[30]. Although yellow fever vaccine provides important protection for travellers to endemic or epidemic areas, in older adults, the risks and benefits associated with the vaccination should be weighed against each other (age associated thymus involution)[32].
4. Special considerations for people affected with longterm CNS conditions
The number of travellers with chronic underlying neurological conditions or older age is on the rise. Approximately 20% of travellers are high-risk individuals that suffer from other comorbidities[33] with more than twotimes as frequent travel-related illnesses as seen in healthy individuals[33]. Most of high-risk travellers travelled to destinations with higher risk for malaria and typhoid fever, and among different neurological disorders, multiple sclerosis and other demyelinating diseases, myasthenia gravis merits special consideration.
Patients receiving immunosuppressive or immunomodulatory treatments could be affected with skin infections more often than others[34] and they require special advice on using live attenuated virus vaccines with regard to the serious sideeffects[35]. Severe immuno-compromised patients should not receive live vaccines. Patients with multiple sclerosis can receive immunization in the presence of strong indication following risk-benefit analysis, although this should be 4-6 weeks after the beginning of a relapse[8]. High-risk individuals should be referred to specialized travel-medicine clinics for further evaluation on whether they should receive vaccination[33]. Patients with epilepsy should take ample sleep and avoid fluorquinolone antibiotics[36].
Patients on special treatments (e.g., warfarin following sinus venous thrombosis or stroke) require drug interaction analysis to make sure that concomitant travel-related medications (e.g., malaria chemoprophylaxis) are safe. Warfarin might have interaction with malarial chemoprophylaxis and patients taking warfarin should start receiving chemoprophylaxis at least 1 week in advance of their scheduled travel[37]. Flights can cause headache and further research is needed to determine the relationship between flight-associated headaches and migraine[38]. Travel-medicine practitioners should ask about the history of thymus disorders (myasthenia gravis and thymectomy). A history of thymus disorder is a contraindication to yellow fever vaccination and affected individuals should seek other ways of prevention such as insect repellents[32]. Travel-medicine practitioners must take extra caution when advising on breast-feeding women for yellow fever vaccination, because it can be transmitted via breastfeeding[30].
4.1. Elderly population
Elderly population is an ever increasing agegroup in most nations. Increasing age is associated with certain neurological conditions such as dementia, Parkinson’s disease, stroke and Alzheimeir’s disease. In 2004, approximately 3 million American adults with 65 years of age or older traveled abroad[39]. This age-group are referred to travel-medicine clinics more frequently[39]. Flight diversions due to neurological emergencies constitute 20% of all emergencies seen during the flight (rank only second to cardiac emergencies)[40,41]. Cognitively impaired individuals are more susceptible to delirium in longer flights and should avoid dehydration (e.g.consuming coffee or alcohol) as well as hypnotic medications. Pre-travel risk assessment plays an important role in these cases to determine whether the elderly patients need an accomplice for the duration of travel or not[31].
4.2. Pediatric population
Children are less likely to receive pre-travel medical advice but are more likely to seek medical care after travel and require hospitalization[42]. They should be approached based on the specific age group with respect to destinationspecific illnesses. Neurological complications are very unlikely in children, although post-vaccination side effects, such as acute disseminated encephalomyelitis might be more common[42].
5. Malarial risk of CNS involvement
Malaria can manifest as cerebral variant that is known as “black-water fever”. High-risk areas for travellers include: Central and South America, Africa and Southeast Asia. This condition is most commonly caused byPlasmodium falciparum. High-risk populations are travellers without chemoprophylaxis, pregnant women and children. It usually presents with headache, chills, nausea, vomiting and myalgia. Severe cases can present with stupor and coma[10]. Residents of malaria-endemic areas show high prevalence of asymptomaticPlasmodium falciparumparasitemia, therefore positive blood film in comatose patients does not prove that coma is due to malaria[43]. Although newer markers such as malaria retinopathy and HRP2 sound promising, future researches should focus on developing more specific biomarkers useful for differential diagnosis[43,44]. Additionally, certain travellers (e.g.Canadian born travellers to endemic areas) are exposed to more severe symptoms and higher parasite density; this warrants further investigations into identification of prognostic markers (e.g.IL-20)[45]. The results of such efforts can help travel medicine to perform a better risk-assessment in travellers.
6. Post-travel consultation
Despite the emphasis on pre-travel consultation and administration of suitable prophylaxis, illnesses also occur in returning travellers[46]. Approximately 8% of travellers seek medical care during or after travelling[22,47]. A detailed history plays an important role for defining the cause; it should include: travel itinerary, pretravel consultation (immunization and chemoprophylaxis), duration of travel, exposures and underlying conditions[47]. The most important diagnostic clue seems to be traveller’s destination[22]. The highest risk areas that cause illnesses in travellers are Asia and sub-Saharan Africa[48]. A large survey showed that common vaccine-preventable diseases in returning travellers are: typhoid and paratyphoid fever, influenza, and viral hepatitis[49]. Fever is a common symptom among returning travellers[48] and when it is associated with CNS involvement it raises the possibility of the following diagnoses: Meningococcal meningitis, malaria, Japanese encephalitis, West-Nile encephalitis, trypanosomiasis and rabies[47]. Infections presenting with mental status changes require inpatient medical care and infectious diseases specialist consultation, other illnesses can be treated on an outpatient basis.
7. Neurobiological epidemics: bioterrorism
From a neurological perspective agents for bioterrorism might include: botulinum toxin, Venezuellan equine encephalitis, anthrax, smallpox, Q-fever, and tularemia[50,51]. Signs and symptoms constitute a broad range from headache and meningitis to encephalopathy and seizure. Interested readers have been referred to an excellent review by Ostebaueret al.with further details on this issue[50]. In general, travel-medicine practitioners should be able to recognize the event and differentiate it from other causes of unusual epidemics[51-53]. Disease occurrence in unusual age, rapid increase in incidence, concurrent animal deaths and high level of suspicion could help care-givers to discriminate bioterrorism and other causes of disease outbreaks[51].
8. Conclusions
In this review, the important aspects of travel-related illnesses from a neurological point of view has been highlighted. Neurological infections that affect international travellers are numerous and require skilled travel-medicine caregivers. Destination of the individuals is amongst the most important factors for addressing the interventions that might be needed for each traveller. Comprehensive assessment both before and after the intended travel could help to prevent or reduce morbidity, mortality and cost of intervention. Individuals with underlying and chronic neurological conditions should also be born in mind as they usually need extra assessment and sometime different medications before their travel. It is also underscored that future directions on a disease-by-disease basis warrants further research. State-of-the-art vaccines, genetic engineering of vectors, real-time monitoring of disease outbreaks and increasing knowledge of the public are important challenges in the future of travel medicine.
Conflict of interest statement
We declare that we have no conflict of interest.
Acknowledgements
This work is supported by the Baqiyatallah University of Medical Sciences Chancellor of Research (grant number
45387).
Comments
Background
Nervous system infections are among the most important diseases in travelers. Healthy travelers might be exposed to infectious agents of CNS, which may require in-patient care. An overview of the available evidence in the field is, therefore, urgent to pave the way to increase the awareness of travel-medicine practitioners and highlights dark areas for future research.
Research frontiers
The authors collected and reviewed related information from varieties of sources, such as PubMed, Scopus, and Web of Knowledge that including books, reviews, and peerreviewed literature. Works pertained to pre-travel care, interventions and vaccinations that related neurological infections were retrieved. The current study could provide information on pre-travel care, vaccination, chronic nervous system disorders and post-travel complications. Recommendations with regard to knowledge gaps and state-of-the-art research are also made.
Related reports
Data were collected from PubMed, Scopus, and Web of Knowledge (1980 to 2013) that including books, reviews, and peer-reviewed literature. Works pertained to pretravel care, interventions, vaccinations related neurological infections were retrieved.
Innovations and breakthroughs
The authors reviewed the state-of-the-art evidence in the field, present comprehensive overview on important CNSdiseases in travel, and finally to provide invaluable insights regarding research areas under-represented in the current literature of the travel medicine.
Applications
Comprehensive assessment both before and after the intended travel could help to prevent or reduce morbidity, mortality and the cost of intervention. Individuals with underlying and chronic neurological conditions should also be born in mind, as they usually need extra assessment and sometime different medications before their travel.
Peer review
This is a valuable review work in which authors highlighted some important aspects of travel-related illnesses from a neurological point of view. These aspects mainly includes risk assessment, general considerations and future directions. Recommendations with regard to knowledge gaps, and state-of-the-art research are made. Given an increasing number of international travelers, novel dynamic ways are available for physicians to monitor the spread of CNS infections.
首先,影响产品价格浮动的因素有很多,如产品成本、市场需求等,而影响产品成本的因素又包含了原材料、技术研发、人力、物流等等,随着技术升级,生产率提高,产品成本自然呈现下降趋势;另一方面,考虑到省空间、美观需求、集多功能于一体、多件套价格等因素,越来越多的消费者认为购买嵌入式一体机更实用、更合适,市场需求加大,更多企业开始研发生产嵌入式一体机产品。因此,成本降低、供应增加,产品均价下降;消费升级,需求提升,零售量大幅增长。
[1] U.S. Department of Commerce. Office of Travel and Tourism Industries (OTTI). U.S. travel abroad declined two percent in 2010. Washington, D.C., USA: OTTI; 2010. [Online] Available from: http://travel.trade.gov/outreachpages/download_data_ table/2010_Outbound_Analysis.pdf. [Accessed on 22 October, 2013].
[2] Ryan ET, Kain KC. Health advice and immunizations for travelers. N Engl J Med 2000; 342(23): 1716-1725.
[3] Fhogartaigh CN, Sanford C, Behrens RH. Preparing young travellers for low resource destinations. BMJ 2012; 345: e7179.
[4] Simons H, Wong CS, Stillwell A. Travel risk assessment and risk management. Nurs Times 2012; 108(20): 14-16.
[5] Schwartz BS, Larocque RC, Ryan ET. In the clinic. Travel medicine. Ann Intern Med 2012; doi: 10.7326/0003-4819-156-11-201206050-01006.
[6] Izadi M, editor. Travel medicine: a country-to-country guide. New York: Nova Science Publishers Inc; 2013.
[7] Awada A, Kojan S. Neurological disorders and travel. Int J Antimicrob Agents 2003; 21(2): 189-192.
[8] Giovanetti F. Travel medicine interventions and neurological disease. Travel Med Infect Dis 2007; 5(1): 7-17.
[9] García HH, Gonzalez AE, Rodriguez S, Tsang VC, Pretell EJ, Gonzales I, et al. Neurocysticercosis: unraveling the nature of the single cysticercal granuloma. Neurology 2010; 75(7): 654-658.
[10] Han MH, Zunt JR. Neurologic aspects of infections in international travelers. Neurologist 2005; 11(1): 30-44.
[11] Leggat PA. Risk assessment in travel medicine. Travel Med Infect Dis 2006; 4(3-4): 127-134.
[12] Dijkshoorn H, Schilthuis HJ, van den Hoek JA, Verhoeff AP. [Travel advice on the prevention of infectious diseases insufficiently obtained by indigenous and non-native inhabitants of Amsterdam, the Netherlands]. Ned Tijdschr Geneeskd 2003; 147(14): 658-662. Dutch.
[13] Salit IE, Sano M, Boggild AK, Kain KC. Travel patterns and risk behaviour of HIV-positive people travelling internationally. CMAJ 2005; 172(7): 884-888.
[14] Duval B, De Serre G, Shadmani R, Boulianne N, Pohani G, Naus M, et al. A population-based comparison between travelers who consulted travel clinics and those who did not. J Travel Med 2003; 10(1): 4-10.
[15] Bacaner N, Stauffer B, Boulware DR, Walker PF, Keystone JS. Travel medicine considerations for North American immigrants visiting friends and relatives. JAMA 2004; 291(23): 2856-2864.
[16] Centers for Disease Control and Prevention (CDC). Traveler’s Health. Atlanta, GA: CDC; 2013. [Online] Available from: http:// wwwnc.cdc.gov/travel/destinations/list. [Accessed on 22 October, 2013].
[17] Hagmann S, Benavides V, Neugebauer R, Purswani M. Travel health care for immigrant children visiting friends and relatives abroad: retrospective analysis of a hospital-based travel health service in a US urban underserved area. J Travel Med 2009; 16(6): 407-412.
[18] Dijkstra JA, Chappuis F, Loutan L. Vaccine-preventable diseases in long-term expatriates. J Travel Med 2005; 12(Suppl 1): S47-57.
[19] Cramer J, Wilder-Smith A. Meningococcal disease in travelers: update on vaccine options. Curr Opin Infect Dis 2012; 25(5): 507-517.
[20] Harrison LH, Pelton SI, Wilder-Smith A, Holst J, Safadi MA, Vazquez JA, et al. The global meningococcal initiative: recommendations for reducing the global burden of meningococcal disease. Vaccine 2011; 29(18): 3363-3371.
[21] Ratnam I, Leder K, Black J, Torresi J. Dengue fever and international travel. J Travel Med 2013; 20(6): 384-393.
[22] Freedman DO, Weld LH, Kozarsky PE, Fisk T, Robins R, von Sonnenburg F, et al. Spectrum of disease and relation to place of exposure among ill returned travelers. N Engl J Med 2006; 354(2): 119-130.
[23] Guy B, Barrere B, Malinowski C, Saville M, Teyssou R, Lang J. From research to phase III: preclinical, industrial and clinical development of the Sanofi Pasteur tetravalent dengue vaccine. Vaccine 2011; 29(42): 7229-7241.
[24] Lang J. Recent progress on sanofi pasteur’s dengue vaccine candidate. J Clin Virol 2009; 46(Suppl 2): S20-24.
[25] Hills SL, Griggs AC, Fischer M. Japanese encephalitis in travelers from non-endemic countries, 1973-2008. Am J Trop Med Hyg 2010; 82(5): 930-936.
[26] Burchard GD, Caumes E, Connor BA, Freedman DO, Jelinek T, Jong EC, et al. Expert opinion on vaccination of travelers against Japanese encephalitis. J Travel Med 2009; 16(3): 204-216.
[27] Duffy MR, Reed C, Edelson PJ, Blumensaadt S, Crocker K, Griggs A, et al. A survey of US travelers to Asia to assess compliance with recommendations for the use of Japanese encephalitis vaccine. J Travel Med 2013; 20(3): 165-170.
[28] Gautret P, Schwartz E, Shaw M, Soula G, Gazin P, Delmont J, et al. Animal-associated injuries and related diseases among returned travellers: a review of the GeoSentinel SurveillanceNetwork. Vaccine 2007; 25(14): 2656-2663.
[29] Gautret P, Parola P. Rabies vaccination for international travelers. Vaccine 2012; 30(2): 126-133.
[30] Chen LH, Hill DR, Wilder-Smith A. Vaccination of travelers: how far have we come and where are we going? Expert Rev Vaccines 2011; 10(11): 1609-1620.
[31] Gautret P, Gaudart J, Leder K, Schwartz E, Castelli F, Lim PL, et al. Travel-associated illness in older adults (>60 y). J Travel Med 2012; 19(3): 169-177.
[32] Barwick Eidex R, Yellow Fever Vaccine Safety Working Group. History of thymoma and yellow fever vaccination. Lancet 2004; 364(9438): 936.
[33] Hochberg NS, Barnett ED, Chen LH, Wilson ME, Iyer H, MacLeod WB, et al. International travel by persons with medical comorbidities: understanding risks and providing advice. Mayo Clin Proc 2013; 88(11): 1231-1240.
[34] Wieten RW, Leenstra T, Goorhuis A, van Vugt M, Grobusch MP. Health risks of travelers with medical conditions--a retrospective analysis. J Travel Med 2012; 19(2): 104-110.
[35] Kotton CN. Vaccination and immunization against travel-related diseases in immunocompromised hosts. Expert Rev Vaccines 2008; 7(5): 663-672.
[36] Mieske K, Flaherty G, O’Brien T. Journeys to high altitude--risks and recommendations for travelers with preexisting medical conditions. J Travel Med 2010; 17(1): 48-62.
[37] Loefler I. Mefloquine and anticoagulant interaction. J Travel Med 2003; 10(3): 194-195.
[38] Potasman I, Rofe O, Weller B. Flight-associated headachesprevalence and characteristics. Cephalalgia 2008; 28(8): 863-867.
[39] Reed CM. Travel recommendations for older adults. Clin Geriatr Med 2007; 23(3): 687-713.
[40] Goodwin T. In-flight medical emergencies: an overview. BMJ 2000; 321(7272): 1338-1341.
[41] Dowdall N. “Is there a doctor on the aircraft?” Top 10 in-flight medical emergencies. BMJ 2000; 321(7272): 1336-1337.
[42] Hagmann S, Neugebauer R, Schwartz E, Perret C, Castelli F, Barnett ED, et al. Illness in children after international travel: analysis from the GeoSentinel Surveillance Network. Pediatrics 2010; 125(5): e1072-1080.
[43] Beare NA, Lewallen S, Taylor TE, Molyneux ME. Redefining cerebral malaria by including malaria retinopathy. Future Microbiol 2011; 6(3): 349-355.
[44] Kariuki SM, Gitau E, Gwer S, Karanja HK, Chengo E, Kazungu M, et al. The value of Plasmodium falciparum HRP2 and malaria retinopathy in distinguishing cerebral malaria from other acute encephalopathies in Kenyan children. J Infect Dis 2013; doi: 10.1093/infdis/jit500.
[45] MacMullin G, Mackenzie R, Lau R, Khang J, Zhang H, Rajwans N, et al. Host immune response in returning travellers infected with malaria. Malar J 2012; 11: 148.
[46] Horvath LL, Murray CK, Dooley DP. Effect of maximizing a travel medicine clinic’s prevention strategies. J Travel Med 2005; 12(6): 332-337.
[47] Centers for Disease Control and Prevention (CDC). Fairley JK. General approach to the returned traveler. Atlanta, GA: CDC; 2013. [Online] Available from: http://wwwnc.cdc.gov/travel/ yellowbook/2014/chapter-5-post-travel-evaluation/generalapproach-to-the-returned-traveler [Accessed on 22 October, 2013]
[48] Leder K, Torresi J, Libman MD, Cramer JP, Castelli F, Schlagenhauf P, et al. GeoSentinel surveillance of illness in returned travelers, 2007-2011. Ann Intern Med 2013; 158(6): 456-468.
[49] Boggild AK, Castelli F, Gautret P, Torresi J, von Sonnenburg F, Barnett ED, et al. Vaccine preventable diseases in returned international travelers: results from the GeoSentinel Surveillance Network. Vaccine 2010; 28(46): 7389-7395.
[50] Osterbauer PJ, Dobbs MR. Neurobiological weapons. Neurol Clin 2005; 23(2): 599-621.
[51] Busl KM, Bleck TP. Treatment of neuroterrorism. Neurotherapeutics 2012; 9(1): 139-157.
[52] Atlas RM. The medical threat of biological weapons. Crit Rev Microbiol 1998; 24(3): 157-168.
[53] Berns KI, Atlas RM, Cassell G, Shoemaker J. Preventing the misuse of microorganisms: the role of the American Society for Microbiology in protecting against biological weapons. Crit Rev Microbiol 1998; 24(3): 273-280.
[54] Smith G. Food- and water-borne disease: using case control studies to estimate the force of infection that accounts for primary, sporadic cases. Epidemics 2013; 5(2): 77-84.
[55] Kollaritsch H, Paulke-Korinek M, Wiedermann U. Traveler’s diarrhea. Infect Dis Clin North Am 2012; 26(3): 691-706.
[56] Liao CS, Lee GB, Liu HS, Hsieh TM, Luo CH. Miniature RT-PCR system for diagnosis of RNA-based viruses. Nucleic Acids Res 2005; 33(18): e156.
[57] Pengsaa K, Limkittikul K, Sabchareon A, Ariyasriwatana C, Chanthavanich P, Attanath P, et al. A three-year clinical study on immunogenicity, safety, and booster response of purified chick embryo cell rabies vaccine administered intramuscularly or intradermally to 12- to 18-month-old Thai children, concomitantly with Japanese encephalitis vaccine. Pediatr Infect Dis J 2009; 28(4): 335-337.
[58] Tordo N, Foumier A, Jallet C, Szelechowski M, Klonjkowski B, Eloit M. Canine adenovirus based rabies vaccines. Dev Biol (Basel) 2008; 131: 467-476.
[59] Jensenius M, Fournier PE, Raoult D. Tick-borne rickettsioses in international travellers. Int J Infect Dis 2004; 8(3): 139-146.
[60] Cross ML, Buddle BM, Aldwell FE. The potential of oral vaccines for disease control in wildlife species. Vet J 2007; 174(3): 472-480.
[61] El Ridi R, Tallima H, Selim S, Dommelly S, Cotton S, Santana BG, et al. Cysteine peptidases as schistosomiasis vaccines with inbuilt adjuvanticity. PLoS One 2014; 9(1): e85401.
[62] Behera R, Thomas SM, Mensa-Wilmot K. New chemical scaffolds for human african trypanosomiasis lead discovery from a screen of tyrosine kinase inhibitor drugs. Antimicrob Agents Chemother 2014; doi: 10.1128/AAC.01691-13.
[63] Feng GD, Shi M, Ma L, Chen P, Wang BJ, Zhang M, et al. Diagnostic accuracy of intracellular mycobacterium tuberculosis detection for tuberculous meningitis. Am J Respir Crit Care Med 2014; 189(4): 475-481.
10.12980/APJTB.4.2014APJTB-2014-0065
*Corresponding author: Dr. Morteza Izadi, Health Research Center, Baqiyatallah University of Medical Sciences, Tehran, Iran.
Tel: +98 9124 537658
Fax: +98 6624 9535
E-mail: morteza.66.izadi@gmail.com
Foundation Project: Supported by the Baqiyatallah University of Medical Sciences Chancellor of Research (grant number 45387).
Article history:
Received 26 Jun 2014
Received in revised form 27 Jun, 2nd revised form 7 Jul, 3rd revised form 19 Jul 2014
Accepted 11 Aug 2014
Available online 28 Aug 2014
猜你喜欢
纺织服装周刊(2019年5期)2019-02-26 19:17:10
现代营销(创富信息版)(2018年2期)2018-02-10 05:20:39
家庭影院技术(2017年9期)2017-09-26 03:41:36
家用电器(2017年6期)2017-07-03 14:31:45
销售与市场·渠道版(2016年3期)2016-04-20 21:48:07
橡胶工业(2015年9期)2015-08-29 06:40:46
中国洗涤用品工业(2015年11期)2015-02-28 19:03:09
辞书研究(2012年4期)2012-04-01 14:33:57
 Asian Pacific Journal of Tropical Biomedicine2014年8期
Asian Pacific Journal of Tropical Biomedicine2014年8期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- Adult Klebsiella pneumoniae meningitis in Qatar: clinical pattern of ten cases
- Iron-chelating and anti-lipid peroxidation properties of 1-(N-acetyl-6-aminohexyl)-3-hydroxy-2-methylpyridin-4-one (CM1) in longterm iron loading β-thalassemic mice
- Digestive fungal flora in asymptomatic subjects in Bobo-Dioulasso, Burkina Faso
- Glucose-6-phosphate dehydrogenase (G6PD) deficiency is associated with asymptomatic malaria in a rural community in Burkina Faso
- GC/GCMS analysis of the petroleum ether and dichloromethane extracts of Moringa oleifera roots
- An efficient method in breaking of dormancy from Bunium persicum (Boiss) Fedtsch seeds: a valuable herb of Middle East and Central Asia