保留关节的瘤段切除酒精灭活再植术治疗股骨远端骨肉瘤的临床疗效
2014-02-13 08:27于秀淳许宋锋徐明袁冶苏情
中国骨与关节杂志 2014年2期
于秀淳 许宋锋 徐明 袁冶 苏情
保留关节的瘤段切除酒精灭活再植术治疗股骨远端骨肉瘤的临床疗效
于秀淳 许宋锋 徐明 袁冶 苏情
目的探讨保留关节的瘤段切除酒精灭活骨再植术治疗股骨远端骨肉瘤的临床疗效,分析常见并发症的发生原因并提出治疗策略。方法2004 年 1 月至 2011 年 5 月,采用保留关节的瘤段切除酒精灭活再植术治疗股骨远端骨肉瘤 10 例。男 7 例,女 3 例;年龄 15~24 岁,平均 20.1 岁,中位年龄 21 岁;左股骨下段 6 例,右股骨下段 4 例;Enneking 分期 II B 期 9 例,III 期 1 例;术后疗效评价采用 MSTS 功能评分和 ISOLS 复合移植物影像评分。结果10 例术后切口均 I 期愈合。随访 12~110 个月,平均随访 34 个月,1 例 13 个月局部复发并全身多发转移而死亡。3 例分别于术后 9、12、24 个月因全身多处转移而死亡。3 例患者 ( 30% ) 于术后 2~9 个月因灭活骨骨折而行切开复位、植骨、环抱器内固定术,1 例于术后半年死亡;1 例术后 4 个月骨折处愈合,再次术后 48 个月无异常。另 1 例再次术后 13 个月再次出现骨折而行切开复位、植骨、钢板内固定术,术后半年骨愈合良好,随访 12 个月出现关节不稳及膝关节屈曲受限。ISOLS 影像评分28~34 分,平均 31 分 ( 87% );MSTS 肢体功能评分 19~28 分,平均 23 分 ( 77% )。结论在严格掌握适应证的前提下,应用保留关节的酒精灭活再植术治疗股骨远端干骺端骨肉瘤是一种可行的手术方式,具有保留关节的重要结构、瘤段骨与宿主骨匹配良好、无排异反应等优点。灭活骨骨折是该手术最常见的并发症,灭活骨自身骨质改变和内固定方式选择不当是导致骨折发生的主要原因。应用钢板内固定及延长外固定时间是降低灭活骨骨折的有效措施。
骨肉瘤;股骨;骨肿瘤;再植术;干垢端
在膝关节周围骨肉瘤保肢治疗中,因肿瘤性假体置换术具有切除肿瘤彻底、术后肢体功能恢复期短、近期疗效满意等优点而被临床广泛应用,但是随着患者生存期的不断延长,与肿瘤假体相关的并发症如感染、松动、断裂等[1-3]会逐步增加,尤其是年轻的成年患者,因肢体活动强度大,假体失败率会更高。在临床工作中,许多学者发现部分骨肉瘤患者的病变位于干骺端,由此提出了保留骨骺的保肢术或保留关节的保肢术,通过临床应用和长期随访发现该手术设计不仅仅是保留肢体,更重要的是保留了自身的关节与功能,克服了肿瘤假体修复骨缺损的缺点,达到了肿瘤性骨缺损生物学重建的目的。我们在总结儿童保留骨骺灭活再植经验[4]的基础上,2004 年 1 月至 2012 年 5 月,采用保留关节的瘤段切除酒精灭活再植术治疗 10 例股骨远端骨肉瘤患者,术后平均随访 3 年,现就该手术方法的适应证、手术过程中的注意事项,并发症、肢体功能报告如下。
资料与方法
一、一般资料
对本组 10 例股骨远端骨肉瘤患者在新辅助化疗支持下,行保留关节的瘤段切除酒精灭活再植术。年龄 15~24 岁,平均 20.1 岁,中位年龄 21 岁;男 7 例,女 3 例;左股骨下段 6 例,右股骨下段4 例;Enneking 分期 II B 期 9 例,III 期 1 例;所有患者均经术前穿刺活检诊断为骨肉瘤。明确诊断后应用 DIA 方案化疗,具体的应用时间与剂量同以前文献报道。化疗前后均通过 MRI 检查确定肿瘤边界(表1 )。
为便于手术适应证的选择,参照以前所提出的骨肉瘤与骨骺相关性的影像学分型标准,依据化疗前 MRI 肿瘤与股骨髁最高点连线 ( Insall 线 ) 的距离分为三种类型 (图1 ):I 型为肿瘤下界位于 Insall线上方至少 1 cm,II 型为肿瘤临近 Insall 线,III 型为肿瘤已穿破 Insall 线侵至股骨髁部。本组患者均为 I 型。
二、手术方法
在硬膜外麻醉或全麻下手术。患者采用平卧位,大腿根部扎气囊止血带。取膝前内侧纵弧形切口,逐层切开皮肤、皮下组织及筋膜,沿股直肌与股内侧肌之间切开并向两侧牵开。切开膝内侧支持带及关节囊,将股直肌、髌骨、膑韧带牵向外侧,骨内侧肌牵向内侧,在骨膜外及肿瘤外正常组织中显露股骨下段。将股骨牵开器插入股骨两侧,以保护周围软组织。在病变近端距肿瘤边界 2~3 cm 处切开骨膜,向近端作骨膜下剥离 ( 远端勿剥离 )。用线锯截断股骨,仔细分离后切断股骨后侧的骨膜,钝性分离股后侧的血管神经至窝,结扎至肿瘤内的血管。向前提起股骨远侧断端,将附着于股骨下段的肌肉切断,切断腓肠肌内外侧头在股骨后髁处的附着点。确定股骨远端内外股骨髁最高点连线并在术中应用 C 型臂 X 线机予以证实。依据术前MRI 在距肿瘤下界 1 cm 处确定股骨远端截骨平面并截断股骨,应用无菌玻片作涂片,以细胞学证实无肿瘤细胞存在。松解止血带,彻底止血。瘤床以42 ℃ 蒸馏水浸泡 30 min,以消灭可能引起的肿瘤细胞种植。将切下的瘤段骨瘤壳较薄处开窗,刮除肿瘤组织、骨髓组织及骨外的软组织,并在瘤骨上按照设定螺钉部位与方向预先钻孔道备用。用 99%酒精浸泡 30 min 后,生理盐水反复冲洗。将灭活瘤段骨壳回植,应用髓内钉固定,以螺钉交叉固定保留的股骨髁;或应用股骨远端钢板固定。骨缺损处以含有阿霉素 ( adriamycin,ADM ) 的骨水泥填充,20 g 骨水泥 / 10 mg ADM。彻底冲洗切口后,逐层关闭,放置引流管 1 根。以长腿石膏托或下肢支具固定。
三、术后处理
常规应用抗生素预防感染。引流管拔除的时间以引流量<50 ml / 24 h 来确定。石膏托固定期间指导患者行下肢功能锻炼。术后 12~14 天拆线并开始术后化疗,剂量与药物以术后肿瘤细胞坏死率确定。术后 8 周拆除外固定,开始膝关节功能锻炼,并扶双拐下地,需要扶拐 4 个月左右。
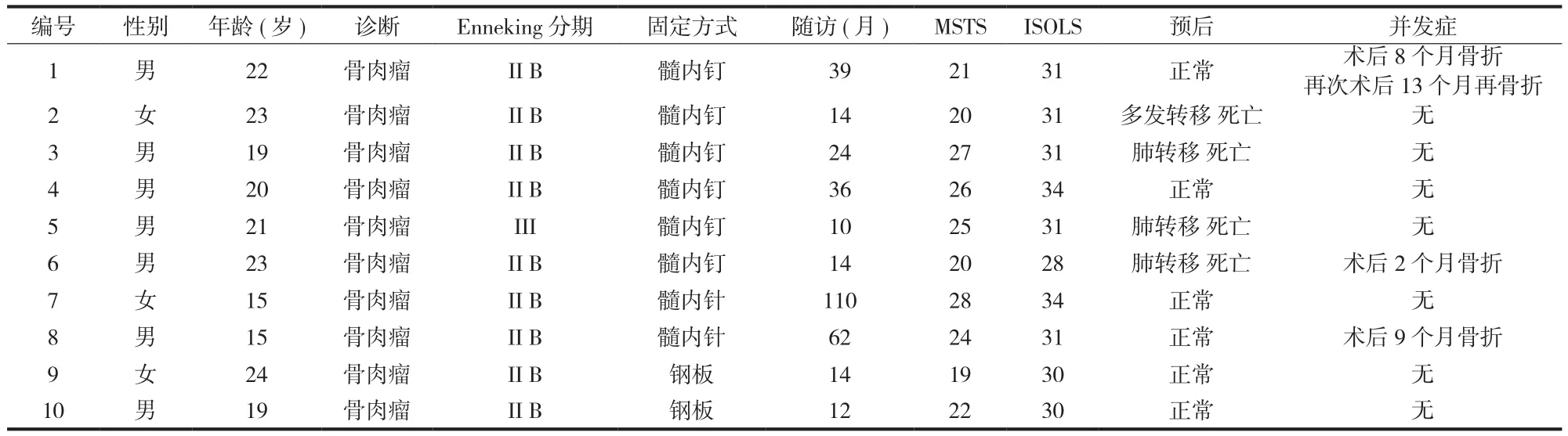
表1 一般资料及随访结果Tab.1 The general data of the patients and the follow-up results
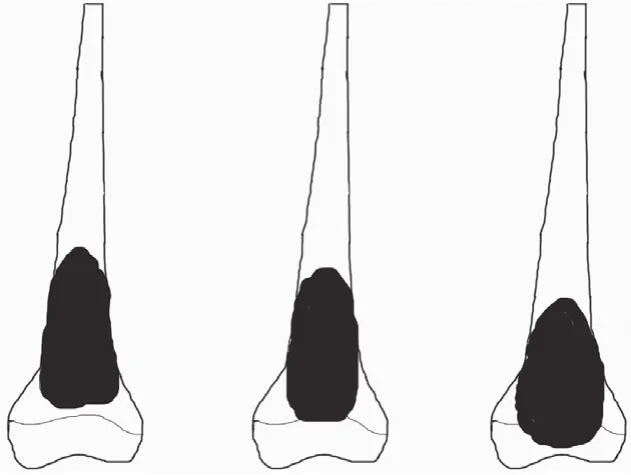
图1 MRI 分型 I、II、III 型 ( 从左至右 ),I 型为肿瘤下界位于Insall 线上方至少 1 cm,II 型为肿瘤临近 Insall 线,III 型为肿瘤已穿破 Insall 线至软骨下骨Fig.1 Type I, II and III according to the MRI classifcation ( from left to right ). Type I: The lowest boarding of tumor was located at least 1cm over the Insall line. Type II: The tumor was located near the Insall line. Type III: The tumor had grown across the Insall line to the subchondral bone
四、随访与疗效评价
参照 NCCN 骨肿瘤治疗指南进行门诊随访,第1~2 年内每 3 个月 1 次,第 3 年每 4 个月 1 次,第4~5 年每 6 个月 1 次,后每年 1 次。包括体检、胸片、手术部位 X 线片、肢体功能评价等。
应用 MSTS 肢体功能评分[5]评估患者术后肢体功能,评估指标分疼痛、功能、心理承受、支持物、行走、步态 6 项,每项 5 分。摄 X 线片以ISOLS 影像评分标准[6]评估灭活骨体内情况,评估指标包括骨重建、界面、锚定、植入体、融合、吸收、骨折、短缩、内固定 9 项,每项 4 分。
结 果
一、一般情况与肿瘤学随访结果
本组 10 例术后切口均 I 期愈合,未出现感染、切口渗出、皮肤坏死等手术并发症。随访 12~110个月,平均随访 34 个月。1 例 III 期患者化疗后肺部结节无变化,术后 13 个月局部复发并全身多发转移而死亡。3 例 II B 期患者分别于术后 9、12、24 个月出现全身多处转移而死亡。其余 6 例至最近随访时均无瘤生存 (图2 )。
二、术后并发症与肢体功能
3 例患者 ( 30% ) 于术后 2~9 个月因灭活骨骨折、髓内钉弯曲或断裂而再次行切开复位、植骨、环抱器内固定术,1 例于术后半年因出现肺转移而死亡;1 例术后 4 个月骨折处愈合,再次术后 48 个月,无异常 (图3 )。另 1 例再次术后 13 个月再次出现原骨折处远端骨折而行切开复位、植骨、钢板内固定术,术后半年骨愈合良好。再次随访 12 个月出现关节不稳及膝关节屈曲受限。本组未出现感染、脱位、肢体短缩等并发症。末次随访 ISOLS 影像评分 28~34 分,平均 31 分 ( 87% );MSTS 肢体功能评分 19~28 分,平均 23 分 ( 77% )。
讨 论
股骨远端是骨肉瘤最好发的部位。目前,对于该部位肿瘤切除后的骨缺损的修复与重建的方法异体骨、人工假体置换、复合假体重建等多种方式,但均存在不同的优缺点,如异体骨的吸收、肿瘤假体的松动、晚期深部感染等,上述并发症的发生明显影响长期生存患者的肢体功能与生活质量。鉴于上述原因,我们对于位于股骨干骺端的儿童骨肉瘤患者应用保留骨骺的灭活再植术予以保肢治疗,通过长期随访发现该方法具有手术操作简单、保留自身关节结构与功能等优点。在此基础上我们对于位于股骨远端干骺端的骨肉瘤应用保留关节的灭活再植术予以治疗,该手术是指对于位于股骨远端内外侧髁连线以近的骨肉瘤在可以保留 Insall 线以远股骨关节软骨及软骨下骨的前提下,将扩大切除的肿瘤骨段,彻底去除肿瘤组织并经过 99% 无水酒精浸泡灭活后 30 min,原位回植并借助各种内固定方式恢复膝关节的连续性和完整性。其杀灭肿瘤的原理在于酒精使瘤壳变性坏死,待周围血管长入时,肿瘤细胞已发生坏死[7]。目的在于不影响保肢肿瘤学治疗结果的前提下,尽量保留自身关节结构以利于肢体功能的恢复,达到股骨远端肿瘤性骨缺损生物学重建的目的。本组 10 例,术后随访平均 34 个月,仅 1 例复发,复发率为 10%,与文献报道的术后复发率无明显差异,证实了该手术方法的临床应用可行性与安全性。
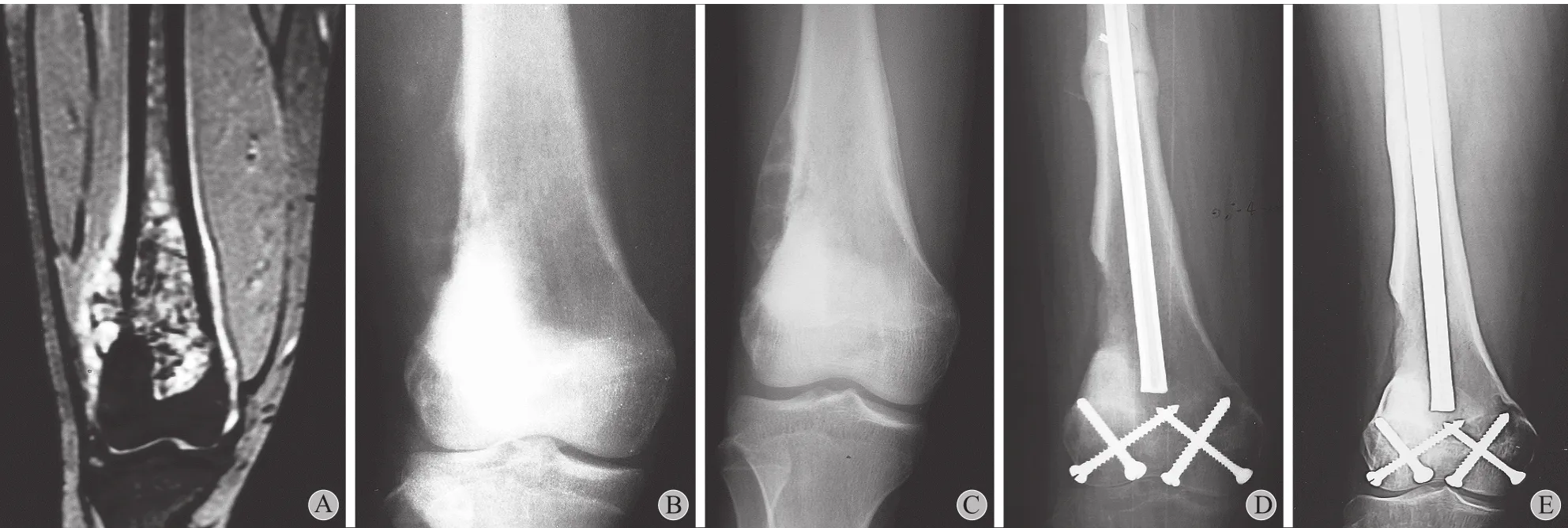
图2 例 7 患者,女,15 岁。股骨远端骨肉瘤行保留关节的灭活再植术 A:化疗前 MRI 示股骨远端髓腔内高低混杂信号,肿瘤远端与Insall 线紧密相邻,为 II 型;B:化疗前 X 线片示股骨远端呈溶骨性骨质破坏,外侧骨皮质破坏严重,形成局部软组织肿块,有骨膜反应;C:化疗后 X 线片示股骨远端呈溶骨性骨质破坏较化疗前明显减轻,软组织肿块影消失,外侧骨膜恢复连续性;D:行保留关节灭活再植术后 2 个月,见股骨远端与保留关节处已骨质以愈合,骨干部位有骨痂形成,但骨干间存在间隙;E:术后 110 个月随访骨质愈合良好,关节间隙正常Fig.2 Case 7. A 15-year-old female patient with osteosarcoma in the distal femur was treated with alcohol-inactivated autograft replantation with articulation preservation A: The MRI before the chemotherapy showed intramedullary high and low mixed signal in the distal femur. The tumor was located near the Insall line which was classifed as Type II; B: The X-ray before the chemotherapy showed osteolytic bone destruction in the distal femur, in accompany with severe destruction of the lateral cortical bone, local soft tissue masses and periosteal reaction; C: The X-ray after the chemotherapy showed signifcantly relieved osteolytic bone destruction in the distal femur, in accompany with the disappearance of local soft tissue masses and the restoration of the continuity of the lateral periosteum; D: At 2 months after the operation, the X-ray showed bone callus in the diaphysis, clearance between the diaphyses and bone healing in the conjunction between the host bone and the inactivated bone; E: At 110 months after the operation, the X-ray showed complete bone healing and normal joint space

图3 例 8 患者,男,15 岁。股骨远端骨肉瘤行保留关节的灭活再植术 A:化疗前 MRI 示股骨远端髓腔内高低混杂信号,软组织内可见异常高信号,肿瘤远端与 Insall 线与骨骺间有 2 cm 距离,为 I 型;B:化疗前 X 线片示股骨远端呈溶骨性骨质破坏,内侧骨皮质破坏并形成局部软组织肿块,有骨膜反应;C:化疗后 X 线片示股骨远端呈溶骨性骨质破坏较化疗前明显减轻,软组织肿块影消失,内侧骨膜恢复连续性并钙化;D:行保留关节灭活再植术后 2 周,见股骨远端与保留关节处复位,骨干连接部位有异体骨板;E:术后 9 个月外伤后骨折,X 线片示股骨远端与保留关节处已骨质愈合,骨干连接部位碎裂,异体骨板与骨干处分离;F:再次术后 30 个月 X 线片示骨质愈合良好,关节间隙正常Fig.3 Case 8. A 15-year-old male patient with osteosarcoma in the distal femur was treated with alcohol-inactivated autograft replantation with articulation preservation A: The MRI before the chemotherapy showed intramedullary high and low mixed signal and abnormally high signal in the soft tissues in the distal femur. The lowest boarding of tumor was located 2cm over the Insall line which was classifed as Type I; B: The X-ray before the chemotherapy showed osteolytic bone destruction in the distal femur, in accompany with severe destruction of lateral cortical bone, local soft tissue masses and periosteal reaction; C: The X-ray after the chemotherapy showed signifcantly relieved osteolytic bone destruction in the distal femur, in accompany with the disappearance of local soft tissue masses and the restoration of the continuity of the lateral periosteum; D: At 2 weeks after the operation, the X-ray showed the restoration of the conjunction between the host bone and the inactivate bone and allogeneic bone sheets in the diaphysis connection part; E: At 9 months after the operation, the patient had fractures because of injuries. The X-ray showed bone healing in the conjunction between the host bone and the inactivated bone, the fragmentation in the diaphysis connection part and the breakage of allogeneic bone sheets from the diaphysis; F: At 30 months after the reoperation, the X-ray showed complete bone healing and normal joint space
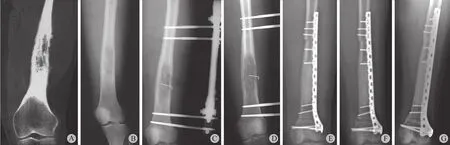
图4 例 9 患者,女,24 岁。股骨远端骨肉瘤行保留关节的灭活再植术 A:确诊前 CT 三维重建示股骨远端髓腔内呈溶骨性骨质破坏,软组织肿胀,肿瘤远端与 Insall 线距离 8 cm,为 I 型;B:确诊前 X 线片示股骨远端呈溶骨性骨质破坏,无局部软组织肿块,有骨膜反应;C:当地医院误诊为骨髓炎行病灶刮除外固定术后,病灶范围较术前增大,病灶内可见克氏针影;D:化疗后 X 线片示病变范围较化疗前无明显变化;E:行保留关节灭活再植钢板内固定术后 2 周,见股骨远端与保留关节处及骨干处复位良好;F:术后 3 个月 X 线片示股骨远端与保留关节及骨干处有骨痂形成,但仍然存在间隙;G:术后 10 个月 X 线片示骨质愈合良好,关节间隙正常Fig.4 Case 9. A 24-year-old female patient with osteosarcoma in the distal femur was treated with alcohol-inactivated autograft replantation with articulation preservation A: The pre-diagnostic CT 3-D reconstruction showed intramedullary osteolytic bone destruction in the distal femur and soft tissue swelling. The lowest boarding of tumor was located 8 cm over the Insall line which was classifed as Type I; B: The pre-diagnostic X-ray showed osteolytic bone destruction in the distal femur, in accompany with severe destruction of lateral cortical bone, periosteal reaction and no local soft tissue masses; C: She was misdiagnosed as osteomyelitis and treated with lesion debridement and external fxation in the local hospital. The lesion range was extended and the Kirschner pin could be seen; D: The X-ray after the chemotherapy showed no signifcant changes of the lesion range; E: At 2 weeks after the operation, the X-ray showed the restoration of the conjunction between the host bone and the inactivated bone; F: At 3 months after the operation, the X-ray showed bone callus in the conjunction between the host bone and the inactivated bone; G: At 10 months after the operation, the X-ray showed good bone healing and normal joint space
保留关节的酒精灭活再植术的优点是手术简便、费用低廉,灭活骨能保持骨干的连续性,减少对骨组织活性和生物力学性能的影响,有利于骨的重建。灭活的瘤细胞可作抗原,刺激免疫系统,增强免疫功能。保留自身关节结构可以提高关节的稳定性。由于该手术方法是一种修复肿瘤性骨缺损的生物学重建的方式与方法,因此可以避免机械性修复肿瘤性骨缺损并发症的发生。酒精灭活再植术的出现和应用,使骨肉瘤患者在得到肿瘤控制的同时保留自身关节,部分患者甚至获得长期良好的肢体功能[8-9]。即使由于并发症原因取出灭活骨,也将大大推迟接受人工关节置换的时间。本组 10 例,除 4 例于术后 12~24 个月内因肺转移而死亡外,余6 例无转移和复发,尽管 1 例因灭活骨骨折反复手术致膝关节屈曲受限,至末次随访时 MSTS 肢体功能评分 19~28 分,平均 23 分 ( 77% )。
与任何修复肿瘤性骨缺损的生物学重建方法一样,保留自身关节的保肢术依然存在骨折延迟愈合或不愈合、内固定松动断裂、局部皮肤坏死、早期骨力学强度不够易发生骨折等并发症。灭活骨骨折为本组最常见的手术并发症,3 例分别于术后 2~18 个月因轻微外力导致灭活骨骨折,均发生于髓内针固定而且位于骨干连接的部位, 均再次行切开复位、植骨、环抱器内固定术,1 例于术后半年因出现肺转移而死亡,1 例术后 4 个月骨折处愈合,至今再次术后 48 个月无异常。另 1 例术后 8 个月再次出现原骨折处远端骨折,再次行切开复位、植骨、钢板内固定术,术后半年骨愈合良好。再次随访 12 个月存在关节不稳及膝关节屈曲受限。提示我们尽管环抱器可以达到其固定部位的稳定性,但由于灭活骨的生物力学性能降低及骨愈合与替代时间延长,在环抱器的远端容易产生应力集中而导致再次骨折的发生,这是导致 2 例再次骨折的主要原因,因此对于灭活骨骨折患者在强调及时行切开复位、充分植骨的同时,应用适当的钢板予以固定。我们以往的临床观察发现酒精灭活自体瘤骨回植术后 2 个月出现大量骨痂[10],术后 6 个月可以达到骨性愈合[11]。因此,我们不建议患者早期进行患肢负重功能锻炼,术后 8 周开始肢体锻炼,应用支具固定 3~6 个月,以促进灭活骨与宿主骨完全愈合。此外,本组 2 例应用钢板螺钉固定的患者无骨折发生且移植骨愈合良好 (图4 ),显示了将髓内针固定改变为钢板螺钉固定可能会预防灭活骨骨折的发生。
Manfrini 等[12]认为,若术前检查未发现骨骺被侵袭,可行保留骨骺的恶性骨肿瘤保肢术。借鉴此思路,我们通过术前 MRI 检查明确肿瘤与干骺端的关系,按照肿瘤与股骨髁最高点连线 ( Insall 线 )的关系分为三种类型 (图1 ):I 型为肿瘤下界位于Insall 线上方至少 1 cm,II 型为肿瘤临近 Insall 线,III 型为肿瘤已穿破 Insall 线至股骨髁部。选择 Insall线的原因是:( 1 ) Insall 线接近骨骺线;( 2 ) 术中容易定位;( 3 ) 保留内外侧副韧带并维持关节稳定性;( 4 ) 自 Insall 线近端处截骨后所保存的股骨髁部可以应用股骨远端解剖钢板或锁定钢板固定,有利于截骨部位的骨愈合。
本组临床结果提示该手术的适应证是:( 1 ) 肿瘤必须位于骨的干骺端,为 I 型且无病理性骨折;( 2 ) 术前必须通过 MRI 检查明确肿瘤未侵袭股骨髁,术后病理组织学予以证实;( 3 ) 必须严格遵循新辅助化疗的治疗原则,在有效化疗的保护下进行该手术;( 4 ) 该手术必须由熟练掌握恶性骨肿瘤保肢技术的医生完成。禁忌证是肿瘤与整个股骨髁部密切接触、侵袭股骨髁 ( 分型中的 II 型和 III 型 ) 和病理性骨折。
该手术过程中需要注意的主要问题:( 1 ) 术前通过 MRI 确定截骨平面,肿瘤下界 1 cm 截骨;( 2 ) 截除瘤骨去除软组织后、酒精灭活前,应当以钻头按照设定螺钉的部位与方向预先钻孔道备用;( 3 ) 灭活骨固定时应当从保留的股骨髁部向灭活骨拧入,而非反方向,以保持灭活骨壳的完整性尽量减少复发的可能性[4];( 4 ) 内固定方式可以选择选择髓内钉+交叉螺钉或股骨远端解剖钢板固定,以后者为首选;( 5 ) 近端宿主骨-灭活骨结合部可使用自体髂骨或异体骨板以丝线固定,形成皮质外植骨,利于早期骨愈合。
本组资料提示在严格掌握适应证的前提下,应用保留关节的酒精灭活再植术治疗股骨远端干骺端的骨肉瘤是一种可行的选择,具有保留关节的重要结构、瘤段骨与宿主骨匹配良好、无排异反应、避免了人工假体置换的远期并发症,实现了肿瘤性骨缺损的生物学重建,尽管会出现以灭活骨骨折为代表的并发症,但经过积极的治疗仍会取得良好的临床疗效,其远期疗效有待进一步随访观察。
[1] Heisel C, Kinkel S, Bernd L, et al. Megaprostheses for the treatment of malignant bone tumours of the lower limbs. Int Orthop, 2006, 30(6):452-457.
[2] Frink SJ, Rutledge J, Lewis VO, et al. Favorable long-term results of prosthetic arthroplasty of the knee for distal femur neoplasms. Clin Orthop Relat Res, 2005, 438:65-70.
[3] Plotz W, Rechl H, Burgkart R, et al. Limb salvage with tumor endoprostheses for malignant tumors of the knee. Clin Orthop Relat Res, 2002, 405:207-215.
[4] 于秀淳, 刘晓平, 周银, 等. 保留骨骺灭活再植术治疗儿童骨肉瘤应注意的问题. 中华小儿外科杂志, 2007, 28(8): 422-425.
[5] Enneking WF, Dunham W, Gebhardt MC, et al. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res, 1993, 286:241-246.
[6] Poffyn B, Sys G, Van Maele G, et al. Radiographic analysis of extracorporeally irradiated autografts. Skeletal radiology, 2010, 39(10):999-1008.
[7] 于秀淳, 刘晓平, 周银, 等. 保留骨骺灭活再植术治疗儿童股骨远端骨肉瘤. 中国矫形外科杂志, 2007, 15(11):811-813.
[8] Sung HW, Wang HM, Kuo DP, et al. EAR method: an alternative method of bone grafting following bone tumor resection (a preliminary report). Semin Surg Oncol, 1986, 2(2):90-98.
[9] 丁易, 牛晓辉, 刘巍峰, 等. 酒精灭活再植术在骨肿瘤治疗中的应用. 中华骨科杂志, 2011, 31(6):652-657.
[10] Wodajo FM, Bickels J, Wittig J, et al. Complex reconstruction in the management of extremity sarcomas. Curr opin oncol, 2003, 15(4):304-312.
[11] 许宋锋, 于秀淳, 徐明, 等. 自体骨复合假体在下肢骨肿瘤保肢治疗中的应用. 中国骨肿瘤骨病, 2010, 9(6):476-480.
[12] Manfrini M, Gasbarrini A, Malaguti C, et al. Intraepiphyseal resection of the proximal tibia and its impact on lower limb growth. Clin Orthop Relat Res, 1999, 358:111-119.
( 本文编辑:王永刚 )
ObjectiveTo investigate the clinical outcomes of alcohol-inactivated autograft replantation with articulation preservation in the treatment of osteosarcoma in the distal femur, to analyze the occurrence of common complications and to propose the treatment strategies.MethodsFrom January 2004 to May 2011, 10 patients with osteosarcoma in the distal femur were treated with alcohol-inactivated autograft replantation with articulation preservation. There were 7 males and 3 females, with an average age of 20.1 years old and a median age of 21 years old ( range; 15-24 years ). Neoplasms were located in the left distal femur in 6 cases, and in the right distal femur in 4 cases. According to the Enneking staging system, 9 patients were identifed as stage II B and 1 patient as stage III. The postoperative outcomes were evaluated according to the Musculoskeletal Tumor Society ( MSTS ) rating scale, and the International Society of Limb Salvage ( ISOLS ) composite graft scores were calculated.ResultsAll the 10 cases were healed by primary intention. The mean follow-up period was 34 months ( range; 12-110 months ). One patient died of local recurrence and systemic multiple metastases 13 months after the operation, and 3 patients died of systemic multiple metastases at 9, 12 and 24 months after the operation respectively. Three patients ( 30% ) experienced the second operation of open reduction, bone implantation and internal fxation with the embracing fxator at 2-9 months after the operation because of inactivated bone fractures. One of them died at 6 months after the operation. One got bone healing at 4 months after the operation with no abnormal signs during the 48-month follow-up. One of the above 3 patients experienced the third operation of open reduction and bone implantation with plate internal fxation because of the fractures 13 months after the second operation, who got bone healing at 6 months after the operation but had joint instability and limited knee fexion during the 12-month follow-up. The mean ISOLS score was 31 points (87%) ( range; 28-34 points ). The mean MSTS functional score was 23 points ( 77% ) ( range; 19-28 points ).ConclusionsBasedon the premise that the indications are strictly mastered, alcohol-inactivated autograft replantation with articulation preservation is a feasible operation method in the treatment of osteosarcoma in the distal femoral metaphysis, with the advantages of preserving important joint structures, good matching between the tumor-bearing bone and the host bone and no immunologic rejection. The inactivated bone fracture is the most common complication. The main causes of fractures are the change of inactivated bone quality and the inappropriate choice of internal fxation. The fracture rate will be signifcantly decreased if plate fxation is chosen and the time of external fxation is prolonged.
Osteosarcoma; Femur; Bone neoplasms; Replantation; Dry scale end
10.3969/j.issn.2095-252X.2014.02.010
R738.1
250031济南军区总医院骨病科
2013-12-23 )
Clinical outcomes of alcohol-inactivated autograft replantation with articulation preservation for osteosarcoma in the distal femur
YU Xiu-chun, XU Song-feng, XU Ming, YUAN Ye, SU Qing. Department of Orthopedics, the General Hospital of Jinan Military Region, Jinan, Shandong, 250031, PRC
猜你喜欢
人人健康(2022年4期)2022-11-25
昆明医科大学学报(2022年1期)2022-02-28
中华骨与关节外科杂志(2021年12期)2021-08-31
临床骨科杂志(2021年3期)2021-06-24
中华养生保健(2020年10期)2021-01-18
中华肩肘外科电子杂志(2020年1期)2020-08-24
World Journal of Clinical Cases(2020年7期)2020-04-23
医学新知(2019年4期)2020-01-02
中国现代药物应用(2019年24期)2020-01-01
腹腔镜外科杂志(2016年10期)2016-06-01