
Cross-sectional study of executive functioning in children with developmental coordination disorders
2012-07-10 03:27:59ShengZHUGuangzhengTANGJianfeiSHI
上海精神医学 2012年4期
Sheng ZHU, Guangzheng TANG, Jianfei SHI*
Cross-sectional study of executive functioning in children with developmental coordination disorders
Sheng ZHU1, Guangzheng TANG2, Jianfei SHI2*
Background:Children with developmental coordination disorder (DCD) have multiple impairments in movement, learning, and the activities of daily living. Studies from other countries have associated these impairments with cognitive function, particularly executive functioning, but these findings have not been confirmed in China.
Aim:Compare the executive functioning of children with DCD with that of normal children.
Methods:The Wisconsin Card Sorting Test (WCST) was administered to 39 children who met DSM-IV criteria of DCD identified at the Seventh People’s Hospital of Hangzhou from March 2008 through March 2010. The WCST was also administered to a control group of 39 randomly selected children from one elementary school in Hangzhou.
Results:The total responses on the WCST and the number of non-perseverative errors for cases and controls were similar, but cases had significantly more errors, more perseverative responses and more perseverative errors; moreover, they completed fewer categories than controls and required more trials to complete the first category.
Conclusion:Our study confirms previous studies which show significantly impaired executive functioning in patients with DCD. Collectively, these studies suggest that the deficits in executive functioning of children with DCD significantly impair their intellectual and social development.
1. Introduction
Developmental Coordination Disorder (DCD) is a common childhood developmental disorder with a reported prevalence of 5%-8% characterized by movement disorders that affecting the individual’s daily activities and learning ability. The age of onset is usually 6 to 12 years of age and it affects boys twice as commonly as girls. DCD is more common in children who were preterm infants or had other perinatal risk factors.[1]The children also have behavioral problems, disordered attention and neuropsychological maladjustment.[2]In a fMRI study Flouris and colleagues[3]found that DCD is associated with an immature cerebral cortex. Studies in other countries have identified impaired executive functioning in children with DCD (including impaired abstract generalization, cognitive shifting, problem solving and impulse control),[3,4]but there have been no studies about executive functioning among children with DCD in China.
2. Subjects and Methods
2.1 Subjects
2.1.1 Case group
The identification of cases and controls is shown in Figure 1. All children treated at the child psychology outpatient department of the Seventh People’s Hospital of Hangzhou from March 2008 to March 2010 who met DSM-IV[5]diagnostic criteria of DCD were potential participants in the study. The diagnosis was made by two attending-level child psychiatrists who were supervised by an associate-professor in child psychiatry. Detailed physical and psychiatric examinations were conducted to rule out subjects with comorbid neurological diseases (e.g. cerebral palsy, paralysis, muscular dystrophy, etc.), other mental diseases (e.g. mental retardation, pervasive developmental disorders, attention deficit and hyperactivity disorder, etc.), and color blindness. A total of 45 cases met the inclusion criteria but 6 cases were not able to complete the study. Parents of all casesprovided oral informed consent to participate. The 39 subjects who completed the study included 28 boys and 11 girls with a mean (sd) age of 8.1 (0.5) years (range 6-11 years).
2.1.2 Control group
One public elementary school in the Xia Cheng District of Hangzhou was randomly selected and then 50 students at the school in grades 1 to 5 were randomly selected using simple random methods. Teachers notified the parents of the selected students who were then contacted by phone by the researchers to explain the purpose and potential risks of the study. After obtaining oral consent and detailed developmental history information from the parents, current academic functioning information was obtained from teachers and a 1-on-1 clinical examination was conducted by an attending-level child psychiatrist to screen out children with DCD, other neurological conditions, mental disorders or color blindness. The remaining ‘normal’ students were the pool of potential controls. The resulting 39 controls included 28 boys and 11 girls with a mean age of 8.0 (0.7) years. There were no significant differences in the gender or age of the cases and controls.

Figure 1. Flowchart for the study
2.2 Evaluation
The Wisconsin Card Sorting Test[6,7](WCST ) is a well validated method for assessing executive functioning that has been employed extensively in China. It is one of the few neuropsychological tests able to detect regional brain damage in the frontal lobe, particularly frontal dorsolateral lesions.[8]The test directly assesses respondents’ ability to classify, generalize, store information, and change perspectives based on new information. These skills reflect different aspects of cognitive functioning: generalization, working memory, attention, and cognitive shifting. The WCST can be employed in both adults and children and with patients who have mental illnesses or brain damage. It has been used in several studies of children with mental disorders in China.[9,10]
There are many potential outcome measures from the WCST but the most frequently reported results include the number of categories completed, the total errors committed, and the number of perseverative responses. Previous studies in China have shown that these WCST measures have good test re-test reliability.[11]
In the current study a computerized version of the WCST was employed. The test was completed individually in a quiet room using a portable computer. All subjects were given the same standardized instructions by a clinical researcher who observed the subject while he or she completed the test. During the test, respondents sorted the 128 cards according to the number, color and shape of images on the cards; the test ended when the subject successfully sorted cards according to 6 predetermined categories or sorted a total of 128 cards. The mean time for completing the test in these subjects was 35 minutes. The WCST software automatically generated the outcome variables for each test.
2.3 Statistical analysis
SPSS 16.0 statistical software was used to analyze the results. Variables compared between the groups include: number of categories completed, total responses, total correct responses, total errors, perseverative responses, perseverative errors, non-perseverative errors, completed categories and trials to complete the first category. The mean values for these measures were compared between groups using t-tests.
The study was approved by the ethical review board of the Seventh People’s Hospital of Hangzhou.
3. Results
As shown in Table 1, the total responses on the WCST and the number of non-perseverative errors for cases and controls were similar, but cases had significantly more errors, perseverative responses and perseverative errors and required more trials to complete the first category. Conversely, the control group had more correct responses and completed more categories than the case group.
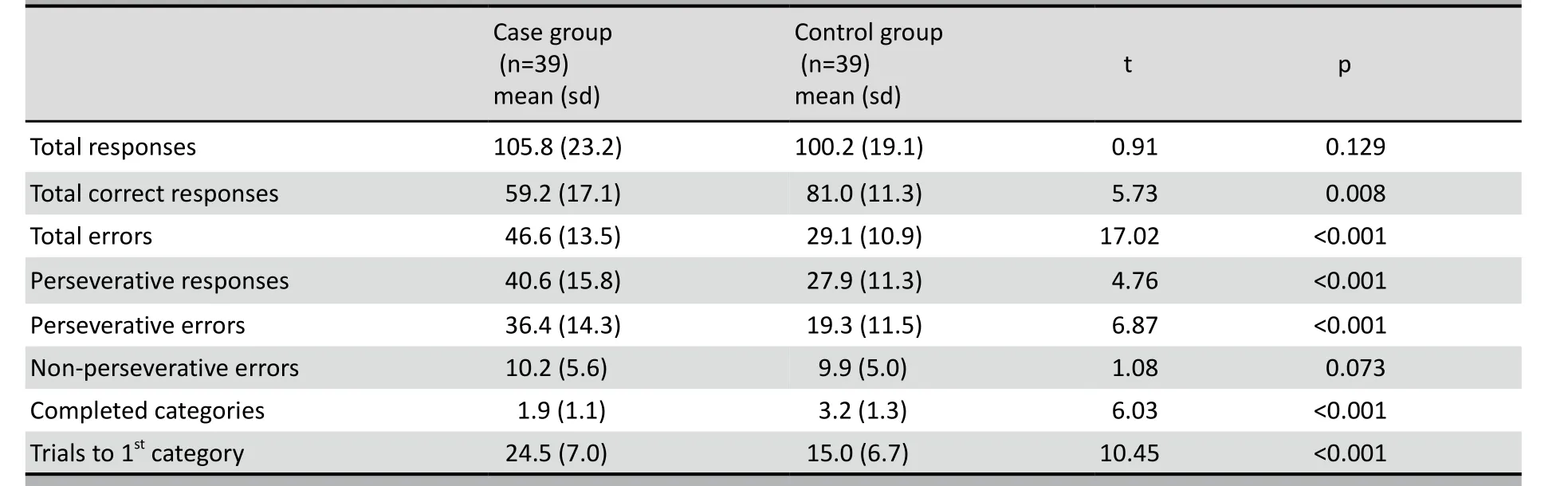
Table 1. Comparison of WCST results between case group and control group
4. Discussion
4.1 Main findings
This controlled trial from China confirms studies on cognitive functioning in children with DCD from other countries.[3,4]On almost all measures derived from the WCST, children with DCD performed less well than children of a similar age randomly selected from the community.
4.2 Limitations
The subjects in this study all attended a single hospital clinic so it is uncertain how representative they are of all children in China with DCD. The controls came from a single school in Hangzhou so it is possible that they are not representative of all non-affected children in China, but they were randomly selected from a randomly selected elementary school in one of the five districts in Hangzhou so they probably are representative of children 6-11 years of age in Hangzhou. The assessment of executive functioning was limited to a single instrument (WCST) so some components of executive functioning were not assessed. No other measures of cognitive or social function were assessed so it is not possible to directly relate these cognitive deficits to social or academic impairments. The sample size was relatively small so it was not possible to conduct subgroup analysis (e.g., by gender) that may have provided more insight into the factors that are associated with cognitive impairments in children with DVD.
4.3 Implications
Many studies have investigated the neurobiological basis of executive dysfunction in children with DCD. The majority of these studies find an association between deficits in executive functioning and abnormal brain development. Most researchers believe that the prefrontal cortex and the region adjacent to the prefrontal cortex are the neuroanatomical sites related to executive funiction, but the neuroimaging studies of Querne and colleagues[12]identified other brain areas (e.g., brain regions related to attention) that may also be involved in executive functioning.
The WCST is the neuropsychological measure that best reflects executive functioning. It has been reported[13]that the number of completed categories and the number of correct responses on the WCST reflects children’s abstract generalization capabilities; that the number of perseverative errors reflects problems in the plasticity of concept formation; thatthe total number of perseverative responses reflect cognitive flexibility; and that the number of trials needed to complete the first category reflects the ability to form an initial concept. Our study confirms previous studies from other locations[4,13,14]which have found that children with DCD are significantly impaired in all of these areas. Collectively, these studies suggest that the deficits in executive functioning of children with DCD will significantly impair their intellectual and social development.
Conflict of interest
The authors report no conflict of interest related to this paper.
Funding
The study was supported by the Seventh People’s Hospital of Hangzhou.
1. Kirby A, Sugden DA. Children with developmental coordination disorders. R Soc Mad 2007; 100(4): 182-186.
2. Chen YW, Tseng FC, Hu FC, Cermak SA. Psychosocial adjustment and attention in children with developmental coordination disorder using different motor tests. Res Dev Disabil 2009; 30(6): 1367-1377.
3. Flouris AD, Faught BE, Hay J, Cairney J. Exploring the origins of developmental disorders. Dev Med Child Neurol 2005; 47(7): 436-440.
4. Dewey D, Kaplan BJ, Crawford SG, Wilson BN. Developmental coordination disorder: associated problems in attention, learning, and psychosocial adjustment. Hum Mov Sci 2002; 21(5-6): 905-918.
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association, 1994.
6. Beijing Haisiman Technology Development Company. User Manual of the Wisconsin Card Sorting Test Analysis System (WCST). Beijing, 1999.
7. Gao YJ, Qu HR, Mao FQ. A study on the executive function and working memory ability in patients with social phobia. Chin J Behav Med & Brain Sci 2011; 20(6): 513-515. (in Chinese)
8. Demakis GJ. A meta-analytic review of the sensitivity of the Wisconsin Card Sorting Test to frontal and lateralized frontal brain damage. Neuropsychology 2003; 17(2): 255-264.
9. Jin Y. Study of neuropsychological mechanism and early screening tools of social cognitive disability of children with Autism Spectrum Disorders. 2008 Doctoral Thesis, Central South University. http://cdmd.cnki.com.cn/Article/CDMD-10533-2008164580.htm [accessed 14 June, 2012]
10. He SH, Jing J. The experiment of Wisconsin Card Sorting Test in children with attention deficit hyperactivity disorder. Chinese Journal of Practical Pediatrics 2003; 21(7): 515-517. (in Chinese)
11. Tan YL, Zou YZ, Qu Y, Guo XF. Stability of commonly used measures in the Wisconsin Card Sorting Test. Chinese Ment Health J 2002; 16(12): 831-833. (in Chinese)
12. Querne L, Berquin P, Vernier-Hauvette MP, Fall S, Deltour L, Meyer ME, et al. Dysfunction of the attentional brain network in children with developmental coordination disorder: a fMRI study. Brain Res 2008; 1244: 89-102.
13. Visser J. Developmental coordination disorder: a review of research on subtypes and comorbidities. Hum Mov Sci 2003; 22(4-5): 479-493.
14. Wuang YP, Su CY, Su JH. Wisconsin Card Sorting Test performance in children with developmental coordination disorder. Res Dev Disabil 2011; 32(5): 1669-1676.
背景发育性协调运动障碍(developmental coordination disorder,DCD)患儿存在明显的运动能力、学习和日常生活能力的下降。国外研究表明,患儿的这些能力下降与其认知功能尤其是执行功能的受损有关,但国内尚无此类研究来证实这些结果。
目的比较发育性协调运动障碍患儿与正常儿童的执行功能。
方法对2008年3月至2010年3月在杭州市第七人民医院就诊并符合DSM-IV发育性协调运动障碍诊断的39例患儿采用威斯康星卡片分类测验(Wisconsin Card Sorting Test,WCST)进行评估。另外,在杭州某小学随机抽取39名健康儿童作为对照组,同样对他们进行WCST评估。
结果两组在WCST的总应答数及非持续错误数相似,但是研究组的错误应答数、持续性应答数和持续性错误数均显著高于对照组。另外,研究组患儿完成分类数低于对照组,完成第一个分类所需的应答数也高于对照组。
结论本研究证实了先前一些研究的结果,即发育性协调运动障碍患儿存在明显的执行功能缺陷。所有这些研究均提示,患儿的执行功能缺陷显著影响了其智能和社会功能的发展。
发育性协调运动障碍儿童执行功能的横断面研究
朱盛1唐光政2施剑飞2*
1浙江省瑞安第五人民医院 浙江瑞安
2杭州市第七人民医院 浙江杭州
*通信作者: shijf659293@sina.com
2011-12-31; accepted: 2012-03-28)
10.3969/j.issn.1002-0829.2012.04.002
1The Fifth People’s Hospital of Ruian, Wenzhou, Zhejiang, China
2The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang, China
*Correspondence: shijf659293@sina.com
猜你喜欢
中国神经精神疾病杂志(2022年3期)2022-07-14 02:23:42
世界科学技术-中医药现代化(2021年8期)2021-12-21 07:04:52
小天使·三年级语数英综合(2020年9期)2020-12-23 04:50:18
小天使·二年级语数英综合(2019年10期)2019-11-08 07:19:36
小天使·二年级语数英综合(2019年9期)2019-11-08 06:46:34
中华家教(2018年7期)2018-08-01 06:32:38
快乐作文·低年级(2016年7期)2016-09-22 18:54:19
中国医药科学(2015年24期)2016-03-07 15:32:46
文学少年(原创儿童文学)(2016年16期)2016-02-28 17:50:19
中国当代医药(2015年7期)2015-03-01 02:01:09
- 上海精神医学的其它文章
- Prevention and management of missing data during conduct of a clinical study
- Cross-sectional assessment of the factors associated with occupational functioning in patients with schizophrenia
- Event-related potentials during mental rotation tasks in patients with first-episode depression
- Meta-analysis of studies in China about changes in P300 latency and amplitude that occur in patients with schizophrenia during treatment with antipsychotic medication
- Research in China on the molecular genetics of schizophrenia
- Psychiatric symptoms in an individual with tuberous sclerosis