肾肿瘤解剖评分联合肾周脂肪粘连评分对囊性肾肿物患者围手术期结果的预测价值分析
2025-02-14 00:00:00王宝陈博宏黄昊翔冯聪曾津陈炜吴大鹏
机器人外科学 2025年1期
摘要 目的:评估肾肿瘤解剖评分联合肾周脂肪粘连评分对接受机器人辅助肾部分切除术的囊性肾肿物(cRM)患者围手术期结果的预测价值。方法:回顾性分析两家三甲医院于2016年3月—2020年12月接受机器人辅助肾部分切除术的50例cRM患者的围手术期资料。评估患者RENAL、术前解剖特征分类(PADUA)、梅奥粘连概率(MAP)、肾周脂肪粘连(APF)评分,以切缘阴性、热缺血时间lt;20 min、无严重术中或术后并发症的MIC“三连胜”视为达到最佳手术结果。统计患者达成MIC情况,通过受试者操作特征曲线(ROC)曲线分析评估各评分系统及组合评分模型对MIC达成的预测价值,选取最优模型进行列线图分析,通过校准曲线、临床决策曲线以及Hosmer-Lemeshow检验来评估列线图的预测性能。结果:肾肿瘤解剖评分中PADUA评分系统略优于RENAL评分系统(AUC:0.782 Vs 0.720),肾周脂肪粘连评分中MAP评分系统略优于APF评分系统(AUC:0.629 Vs 0.525),但差异均无统计学意义(Pgt;0.05)。PADUA评分与MAP评分的组合评分模型(AUC=0.822)预测能力优于任何一种单一评分模型或组合评分模型,通过校准和决策曲线分析证实临床应用价值显著。结论:PADUA评分与MAP评分的组合评分模型在cRM患者术后MIC达成中表现出卓越的预测能力,可为此类患者接受机器人辅助手术的风险评估和术前决策提供有力支持。
关键词 囊性肾肿物;机器人辅助肾部分切除术;肾肿瘤解剖评分;肾周脂肪粘连评分
中图分类号 R737.11 文献标识码 A 文章编号 2096-7721(2025)01-0107-07
Value of renal tumor anatomy score combined with perirenal fatty adhesions score in predicting perioperative outcomes of patients with cystic renal masses
WANG Bao, CHEN Bohong, HUANG Haoxiang, FENG Cong, ZENG Jin, CHEN Wei, WU Dapeng
(Department of Urology, the First Affiliated Hospital of Xi’an Jiaotong University, Xi’an 710061, China)
Abstract Objective: To assess the value of renal tumor anatomy score combined with perirenal fatty adhesions score in predicting the perioperative period outcomes of cystic renal mass (cRM) patients who underwent robot-assisted partial nephrectomy. Methods: 50 patients with cRM who underwent robot-assisted partial nephrectomy from March 2016 to December 2020 in two tertiary hospitals were selected, and their perioperative data were analyzed retrospectively. Patients’ RENAL, preoperative aspects and dimensions used for an anatomical (PADUA), Mayo adhesive probability (MAP), and adherent perinephric fat (APF) scores, and wether the MIC “trifecta” was achieved (negative margins, thermal ischemia time lt;20 min, and no serious intraoperative or postoperative complications) were assessed. ROC curves were used to evaluate the predictive value of each scoring system and combined scoring model for MIC trifecta. The best model was selected for nomogram analysis, and the Hosmer-Lemeshow test, calibration curves, and clinical decision curves were used to evaluate the predictive performance of nomogram. Results: In the renal tumor anatomy scoring, the PADUA scoring system outperformed the RENAL scoring system by a small margin (AUC: 0.782 Vs 0.720), and in the perirenal fatty adhesions scoring, the MAP scoring system outperformed the APF scoring system by a small margin (AUC: 0.629 Vs 0.525). But none of the differences was statistically significant (Pgt;0.05). The predictive ability of the combined scoring model of the PADUA score and MAP score (AUC=0.822) was superior to any single scoring model or the combined scoring model, and the significant value of clinical application was confirmed by calibration and decision curve analysis. Conclusion: The combined scoring model of the PADUA score and MAP score showed excellent predictive ability in predicting postoperative MIC in patients with cRM, which can provide powerful support for risk assessment and preoperative decision-making for patients who will undergo robot-assisted surgery.
Key words Cystic Renal Mass; Robot-assisted Partial Nephrectomy; Renal Tumor Anatomy Score; Perirenal Fatty Adhesion Score
囊性肾肿物(Cystic Renal Mass,cRM)约占肾肿物病例的15%。Bosniak分级根据CT影像学表现对cRM进行分类和风险分层评估[1]。部分复杂性cRM(≥Bosniak ⅡF)被诊断为恶性,约4%~10%的肾癌表现为囊性改变,需要进行手术治疗[2]。尽管cRM相较于实性肾肿物(Solid Renal Mass,sRM)的病理分期和核分级较低,但对于体积较大或复杂度较高的复杂cRM,仍建议选择保留肾单位手术作为优先治疗方式。与sRM不同,切除cRM需格外小心谨慎,以避免囊肿破裂和内容物溢出[3]。凭借精准、微创等多重优势,机器人辅助技术在处理具有挑战性的cRM保肾手术中应用日益广泛[4]。
目前已有数十种评分系统用于评估肾部分切除术的复杂程度[5]。RENAL评分和术前解剖特征分类(Preoperative Aspects and Dimensions Used for An Anatomical,PADUA)评分由于计算简便、重现性高而被广泛采纳。近年来,梅奥粘连概率(Mayo Adhesive Probability,MAP)评分和肾周脂肪粘连(Adherent Perinephric Fat,APF)评分等评分系统也日益受到重视。上述评分均已被证实与sRM不良围手术期结果相关[6-9],但鲜有研究评估这些评分组合对cRM患者围手术期结果的预测效能。基于此,本研究详细探讨了单一评分与组合评分对cRM围手术期结果的预测价值,现报道如下。
1 资料与方法
1.1一般资料 本研究回顾性分析西安交通大学第一附属医院于2017年1月—2020年10月以及南昌大学第一附属医院于2016年3月—2020年
12月接受机器人辅助肾部分切除术患者的临床资料。纳入标准为单个肾肿瘤且具备完整影像学和临床资料的cRM患者。排除标准:①存在淋巴结转移;②存在血管受累或腔静脉癌栓形成;③存在远处转移;④存在肾功能障碍或肾功能衰竭;⑤年龄lt;18岁或年龄gt;80岁。最终共纳入50例cRM患者,所有手术均由经验丰富的机器人辅助手术医生主刀。
1.2数据收集 两名经验丰富的泌尿科医生根据相关文献算法[7,10-12],依据患者术前腹部CT或MRI影像数据,评估RENAL、PADUA、MAP、APF评分,对于存在分歧的评分,由高年资医生重新计算以评估最终分数。临床使用ClassIntra系统[13]进行术中并发症分类,Clavien-Dindo分级系统[14]评估患者术后3个月的并发症情况。在本研究中,达成MIC(Margin,Ischemia and Complications)“三连胜”被视为达到最佳手术结果的标准,即同时满足切缘阴性或无囊肿破裂,热缺血时间lt;20 min,无严重术中或术后并发症(ClassIntra评分gt;Ⅱ级或Clavien评分Ⅲ~Ⅳ级)。
1.3评分标准 选取RENAL评分系统和PADUA评分系统进行肾肿瘤解剖评分,选取MAP评分系统APF评分系统进行肾周脂肪粘连评分。
RENAL评分系统评估标准如下:①肿瘤最大径≤4 cm为1分,4~7 cm为2分,≥7 cm为3分;②肿瘤外凸率≥50%为1分,lt;50%外凸为2分,完全内生型为3分;③肿瘤与肾集合系统的距离≥7 mm为1分,4~7 mm为2分,≤4 mm为3分;④肿瘤与肾脏上下极的位置,完全在上下极为1分,大部在上下极为2分,gt;50%不在上下极为3分。将上述指标评分相加,可以将手术复杂性划分为低级(4~6分)、中级(7~9分)、高级(10~12分)。
PADUA评分系统评估标准如下:①肿瘤最大径≤4 cm为1分,4~7 cm为2分,gt;7 cm为3分;②肿瘤与肾脏上下极的垂直位置,位于上下极为1分,位于中部为2分;③肿瘤与肾脏内外侧的水平位置,外侧为1分,内侧为2分;④肿瘤与肾集合系统的关系,无关为
1分,有关为2分;⑤肿瘤与肾窦的关系,无关为1分,有关为2分;⑥肿瘤外凸率≥50%为1分,lt;50%外凸为2分,完全内生型为3分。将上述指标评分相加,可将手术复杂性划分为低级
(6~7分)、中级(8~9分)、高级(10~14分)。
MAP评分系统评估标准如下:①后侧肾周脂肪厚度lt;1 cm为 0分,1~2 cm为1分,≥2 cm
为2分;②肾周脂肪无条索状改变为0分,存在轻/中度条索(1型)为2分,存在严重条索(2型)为3分。MAP评分系统旨在预测术中遇到肾周脂肪粘连的可能性,将上述指标评分相加,评分总分为0~5分,分数越高表示遇到肾周脂肪粘连的概率越大。
APF评分系统评估标准如下:①后肾周脂肪厚度lt;2 cm为0分,≥2 cm为1分;②肾周脂肪无明显条索为0分,存在轻/中度条索(1型)为1分,存在严重条索(2型)为2分;③未合并糖尿病为0分,合并糖尿病为1分。将上述指标评分相加,评分总分为0~4分,分数越高表示在肾部分切除术中遇到肾周脂肪粘连的概率越大。
1.4统计学方法 在基线资料中,连续变量采用中位数(四分位数)[M(P25,P75)]表示,分类变量则使用例数(百分比)[n(%)]表示。采用受试者操作特征曲线(Receiver Operator Characteristic Curve,ROC)及曲线下面积(Area Under the Curve,AUC)评估预测性能,AUC代表模型在分类任务中的整体性能,范围为0~1,AUC值lt;0.5表示模型预测效果较差,0.5≤AUC值lt;0.7表示模型性能一般,0.7≤AUC值lt;0.9表示模型性能良好,AUC值≥0.9表明模型性能非常优秀。利用Logistic回归分析对肾肿瘤解剖评分和肾周脂肪粘连评分进行组合,并使用列线图进行直观可视化展示,通过校准曲线、临床决策曲线以及Hosmer-Lemeshow检验来评估列线图的预测性能。所有统计学分析及可视化工作均使用R-4.2.2软件完成,Plt;0.05表示差异有统计学意义。
2 结果
2.1患者基线信息 50例患者中有33例来自西安交通大学第一附属医院,17例来自南昌大学第一附属医院。患者年龄为[47(39,54)]岁,
其中男性52%,女性48%,BMI为[24.2(21.7,26.8)] kg/m2,行左侧手术和右侧手术的患者各占50%。根据美国麻醉医师协会(ASA)评分,10%的患者为ASA Ⅰ级,52%为ASA Ⅱ级,38%为ASA Ⅲ级。根据Bosniak分级显示,22%的患者为Bosniak ⅡF级,44%为Bosniak Ⅲ级,34%为Bosniak Ⅳ级。术中失血量为[100(50,200)] mL,热缺血时间为[24(18,28)] min,
16%的患者出现并发症。患者评分方面,RENAL评分为[8(7,9)]分,PADUA评分为[9(8,11)]分,MAP评分为[2(1,3)]分,APF评分为[1(1,3)]分,其中13例(26%)达到MIC标准。
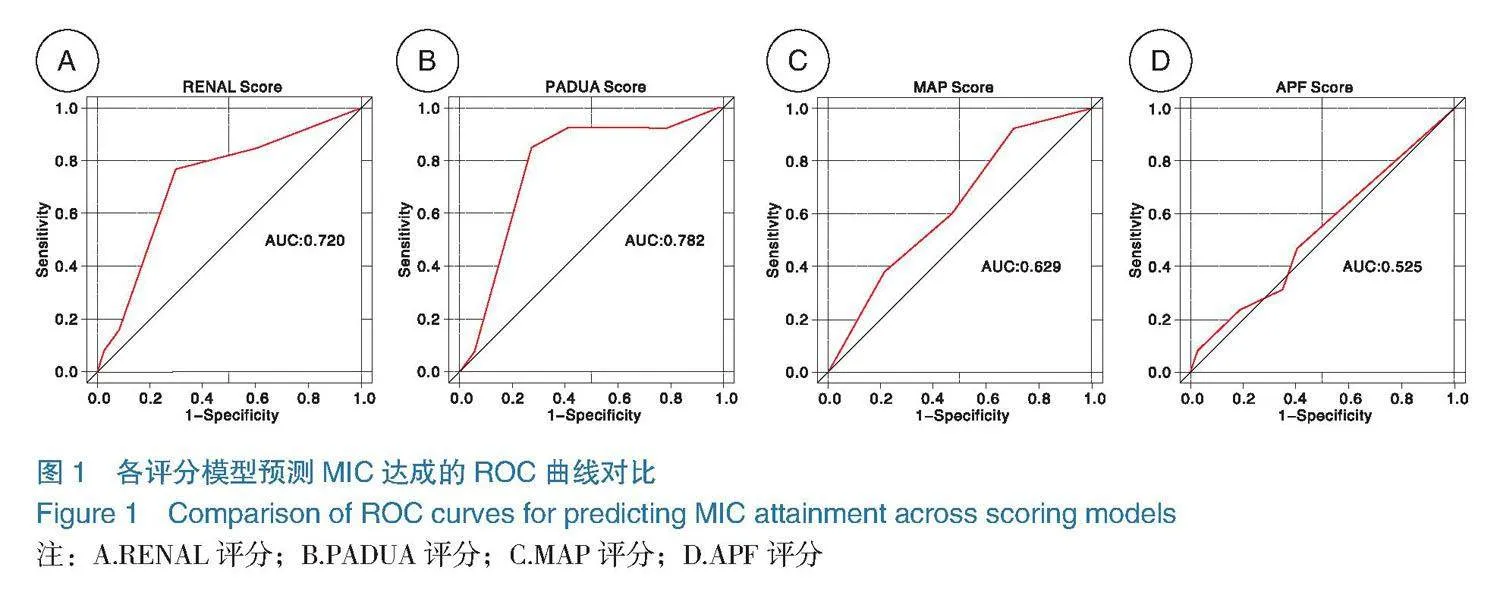
2.2各评分模型的ROC曲线分析 各评分模型对MIC达成结果的ROC曲线如图1,在评估肾肿瘤解剖评分对于MIC达成的预测方面,PADUA评分与RENAL评分在预测能力方面虽略有差异,但差异无统计学意义(Delong检验:P=0.4475gt;0.05);MAP评分在预测MIC方面的能力略优于APF评分,但二者差异也无统计学意义(Delong检验:P=0.2323gt;0.05)。
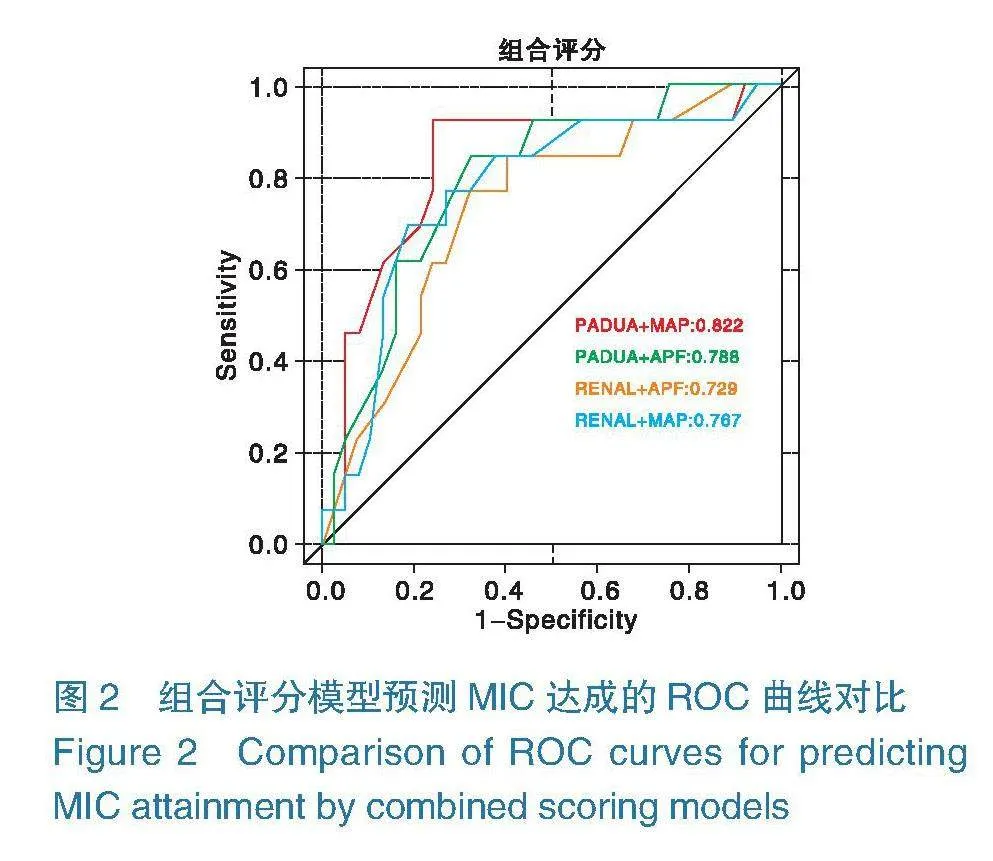
2.3组合评分模型的ROC曲线分析 各组合评分模型对MIC达成结果的ROC曲线如图2,所有组合AUC值均超过0.7,表明各组合评分模型在预测MIC达成方面具有较高的准确性,其中PADUA和MAP联合模型的AUC值最高(AUC=0.822),显示出最优的区分能力。
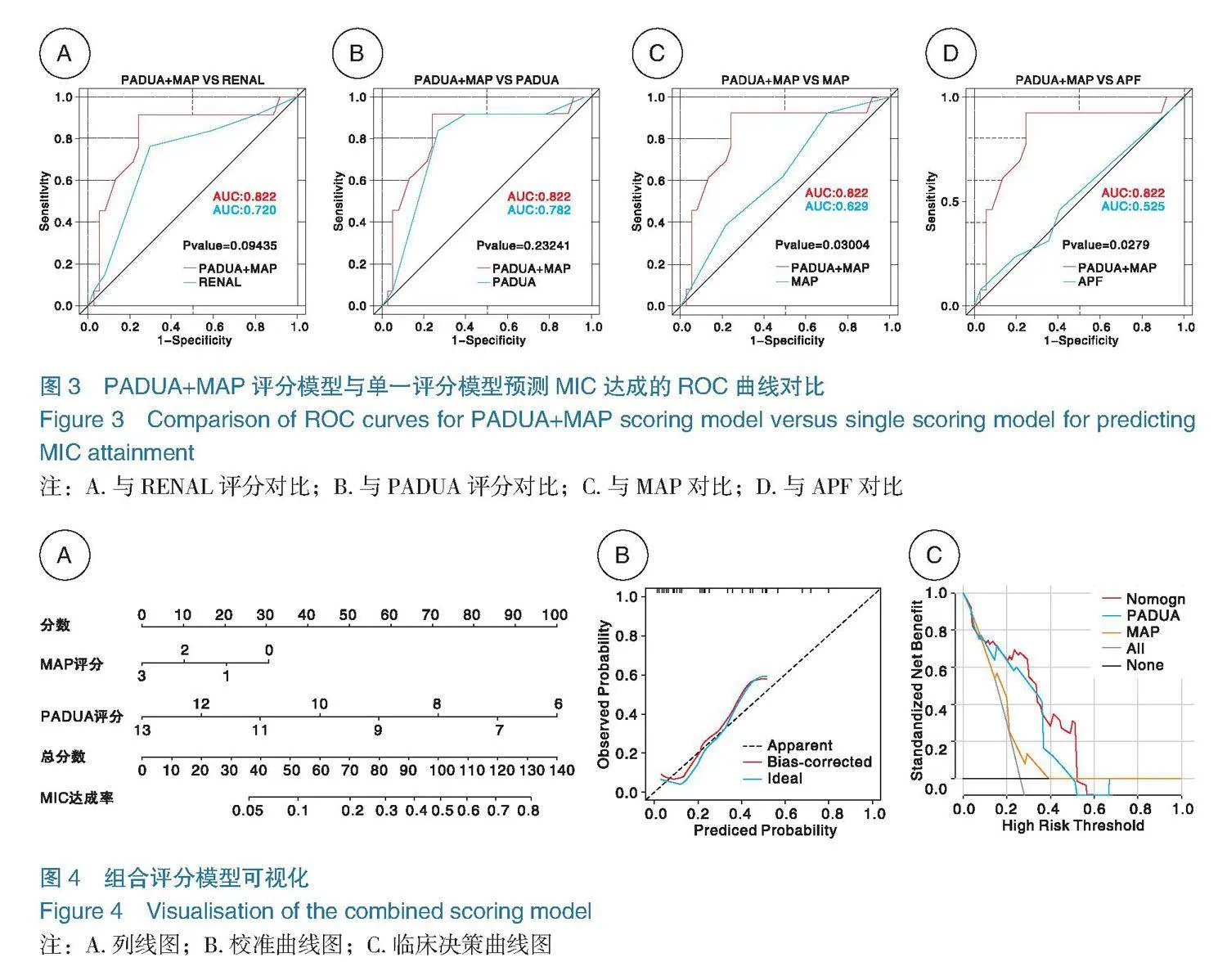
2.4组合评分模型与单一评分模型的对比分析
由上文可知,就预测cRM患者达成MIC而言,PADUA(AUC=0.782)和MAP(AUC=0.629)分别是肾肿瘤解剖评分和肾周脂肪粘连评分中较为可靠的评分模型,将这两个评分模型结合后,AUC值提高至0.822。与单一评分相比,组合评分模型优于单一的肾周脂肪粘连评分,差异有统计学意义(Plt;0.05),也优于单一的肾肿瘤解剖评分,但差异无统计学意义(Pgt;0.05),如图3。
2.5模型可视化及模型效果评价 为了使模型更加实用和通用,本研究对模型进行了直观化展示。图4A呈现了组合评分模型的列线图,其中PADUA和MAP的具体评分分别映射到评分轴上,将这些评分相加后,得到的总分再投射到带有发生概率刻度的概率轴上,从而计算得到最终的MIC发生概率。图4B的校准曲线显示,校正后的概率曲线与理想曲线拟合度较高,能够有效预测cRM患者的MIC结果。临床决策曲线分析如图4C,结果表明组合评分模型的净受益率高于任一单独评分模型。另外,Hosmer-Lemeshow检验结果显示该模型具有良好的预测能力(χ2=11.721,P=0.1641gt;0.05)。
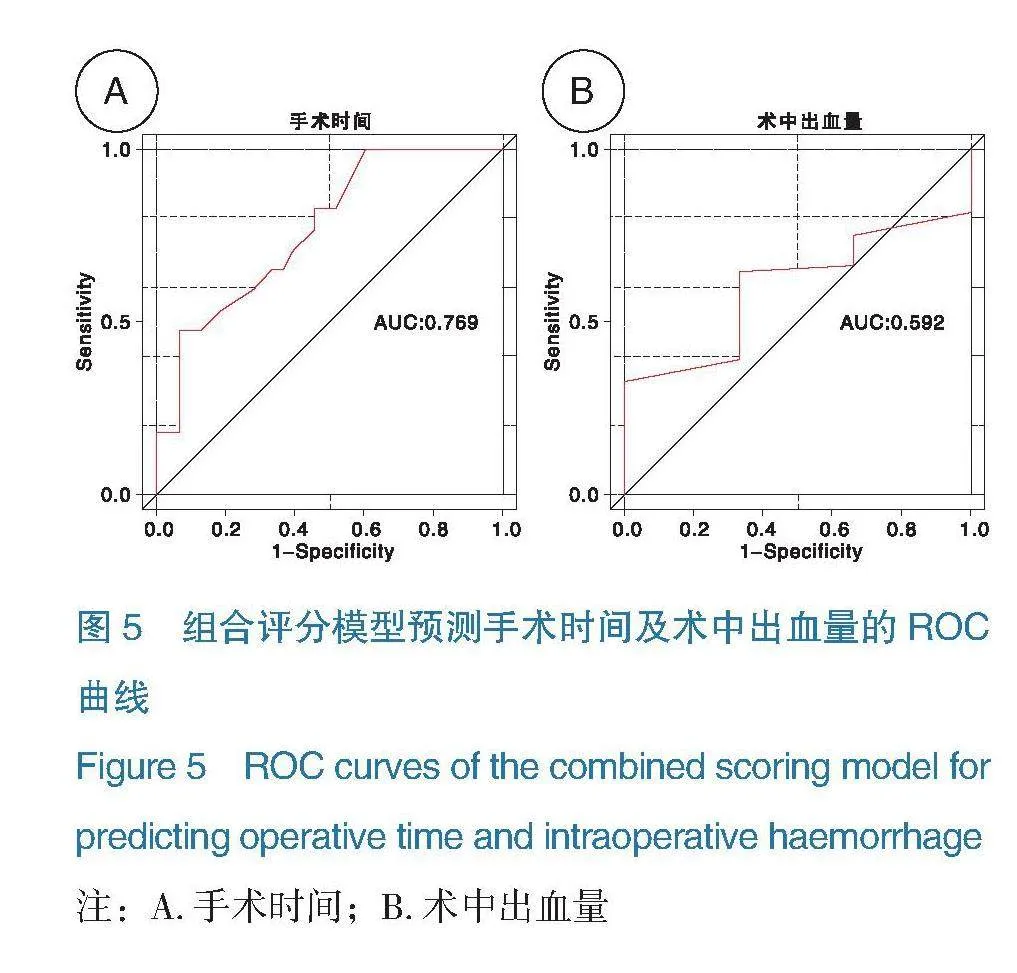
2.6组合评分模型对其他围手术期结果的预测能力 手术时间和术中出血量是cRM患者围手术期结局中除MIC之外的另外两项重要指标。本研究使用组合评分模型对手术时间是否超过
150 min及术中出血量是否超过200 mL进行ROC曲线分析(如图5)。结果显示,组合评分模型对于预测手术时间是否超过150 min具有较好的预测能力(AUC=0.769),但对于术中出血量是否超过200 mL的预测效果较差(AUC=0.592)。
图5 组合评分模型预测手术时间及术中出血量的ROC曲线
Figure 5 ROC curves of the combined scoring model for predicting operative time and intraoperative haemorrhage
注:A. 手术时间;B.术中出血量
3 讨论
肾囊性病变是一种以肾脏出现“囊性改变”为特征的常见肾脏疾病。流行病学研究显示,60岁以上人群中至少有三分之一患有某种形式的肾囊性病变[15]。复杂性cRM是一种组织形态学上具有明显异质性的肾脏病变,这种异质性体现在Bosniak分类系统中对于复杂性cRM的评判标准上[16-17]。Bosniak分类将肾囊性病变划分为Ⅰ~Ⅳ四个等级,其中恶性肿瘤的可能性随着分级的升高而显著增加。在Bosniak Ⅳ级别的病变中超过90%为恶性肿瘤[18],但传统观点认为,囊性肾细胞癌相较于实性肾细胞癌,通常具有较为温和的生物学行为和低转移风险,因此认为主动监测与消融治疗是外科手术的替代方案。然而,既往研究发现富马酸加氢酶缺陷型肾细胞癌虽具有较强的侵袭性和转移潜能,但也可表现出囊性结构改变[19],因此机器人辅助肾部分切除术仍被推荐为复杂性cRM的首选治疗手段。
目前所有复杂的肾肿瘤解剖评分系统,如PADUA和RENAL,都是基于实性肾细胞癌的主要解剖学特征设计的,旨在指导术前手术规划和咨询[3,10,20]。然而,这些评分系统并未将肿瘤的囊性状态纳入考虑因素。尽管如此,手术医生在实际操作单纯性cRM和复杂性cRM时,主观经历存在明显差异[3,21]。先前有研究发现,在Bosniak Ⅲ级的患者中,RENAL评分中的E(外突程度)和N(与肾窦或集合系统的距离)两个因素得分高,以及主刀医生经验水平较低,都是导致囊肿破裂的重要预测因
素[22]。肾周脂肪粘连是指由于炎症反应而黏附于肾实质表面的脂肪组织,会增加肾肿瘤的游离分离难度,从而加大行肾部分切除术的手术操作难度,被认为是影响肾部分切除术手术不良结局的一个关键非肿瘤相关因素[23-24]。既往已有肾肿瘤解剖评分与肾周脂肪粘连评分联合预测肾肿瘤围手术期结局的相关报道[25-26],但对于预测cRM围手术期结局的作用知之甚少。JIN D C等人[27]通过Logistic回归分析将RENAL和MAP两个评分系统结合,发现组合评分优于单一评分系统,AUC值提高到0.847,能更好地预测术中并发症,与本研究结果一致。YANG B等人[28]在一项纳入159例接受腹腔镜肾部分切除术患者的回顾性研究中,评估RENAL和MAP两种评分系统,然而该研究主要是为评估接受腹腔镜肾部分切除术的患者设计的,而非接受机器人辅助手术的cRM患者。TAN X J等人[29]也使用RENAL和MAP评分建立肾部分切除术患者术中并发症预测列线图,但同样未针对cRM患者。
本研究首先对两种主流的肾肿瘤解剖评分和两种肾肿瘤粘连脂肪评分进行cRM患者达成MIC的ROC曲线分析,结果显示PADUA评分模型和MAP评分模型在各自的评分系统中表现更佳,这与既往一项探究腹膜后入路机器人辅助肾部分切除术的研究结论相似[30]。本研究对PADUA评分模型和MAP评分模型的组合评分模型组合建立列线图,结果显示该组合评分模型对MIC达成的预测效能显著优于其他单一评分模型或组合评分模型,对未来接受机器人手术的囊性肾癌患者在术前进行风险评估具有重要意义。
本研究虽然为探讨围手术期因素与术后并发症之间的关系提供了有价值的见解,但仍存在一些需要改进之处。首先,由于本研究采用回顾性研究设计,且样本量相对有限,可能会导致选择性偏差和证据力度不足。其次,研究对象来自两家不同的医疗机构,手术操作技术的异质性可能会对结果产生一定影响。此外,该组合评分模型在预测除MIC之外的其他围手术期结局(如术中出血量)方面,预测价值相对较低。未来应开展前瞻性、多中心研究,拓展样本量,减少选择偏倚,并探讨其他可能的预测因素,从而进一步评估和改善该组合模型的临床适用性。
综上所述,本研究分析了cRM患者的基线信息和各评分系统对MIC达成的预测效能,结果显示PADUA评分与MAP评分的组合评分模型在预测MIC方面表现最佳,显著优于单一评分系统,该组合评分模型在术前风险评估中具有较高的实用性和准确性,有助于更好地预测和管理接受肾部分切除术的cRM患者的围手术期风险。
利益冲突声明:本文不存在任何利益冲突。
作者贡献声明:吴大鹏、陈炜、曾津负责设计论文框架,起草论文;王宝、陈博宏、黄昊翔、冯聪负责数据收集,统计学分析,绘制图片;王宝负责撰写文章,论文修改并最后定稿。
参考文献
[1] Graumann O, Osther S S, Karstoft J, et al. Bosniak classification system: inter-observer and intra-observer agreement among experienced uroradiologists[J]. Acta Radiol, 2015, 56(3): 374-383.
[2] Akca O, Zargar H, Autorino R, et al. Robotic partial nephrectomy for cystic renal masses: a comparative analysis of a matched-paired cohort[J]. Urology, 2014, 84(1): 93-98.
[3] Spaliviero M, Herts B R, Magi-Galluzzi C, et al. Laparoscopic partial nephrectomy for cystic masses[J]. J Urol, 2005, 174(2): 614-619.
[4] Abdel Raheem A, Alatawi A, Soto I, et al. Robot-assisted partial nephrectomy confers excellent long-term outcomes for the treatment of complex cystic renal tumors: median follow up of 58 months[J]. Int J Urol, 2016, 23(12): 976-982.
[5] Veccia A, Antonelli A, Uzzo R G, et al. Predictive value of nephrometry scores in nephron-sparing surgery: a systematic review and meta-analysis[J]. Eur Urol Focus, 2020, 6(3): 490-504.
[6] Dahlkamp L, Haeuser L, Winnekendonk G, et al. Interdisciplinary comparison of PADUA and R.E.N.A.L. scoring systems for prediction of conversion to nephrectomy in patients with renal mass scheduled for nephron sparing surgery[J]. J Urol, 2019, 202(5): 890-898.
[7] Kobayashi K, Saito T, Kitamura Y, et al. The RENAL nephrometry score and the PADUA classification for the prediction of perioperative outcomes in patients receiving nephron-sparing surgery: feasible tools to predict intraoperative conversion to nephrectomy[J]. Urol Int, 2013, 91(3): 261-268.
[8] Bier S, Aufderklamm S, Todenhöfer T, et al. Prediction of postoperative risks in laparoscopic partial nephrectomy using RENAL, Mayo adhesive probability and renal pelvic score[J]. Anticancer Res, 2017, 37(3): 1369-1373.
[9] Davidiuk A J, Parker A S, Thomas C S, et al. Prospective evaluation of the association of adherent perinephric fat with perioperative outcomes of robotic-assisted partial nephrectomy[J]. Urology, 2015, 85(4): 836-842.
[10] Ficarra V, Novara G, Secco S, et al. Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumours in patients who are candidates for nephron-sparing surgery[J]. Eur Urol, 2009, 56(5): 786-793.
[11] Davidiuk A J, Parker A S, Thomas C S, et al. Mayo adhesive probability score: an accurate image-based scoring system to predict adherent perinephric fat in partial nephrectomy[J]. Eur Urol, 2014, 66(6): 1165-1171.
[12] Borregales L D, Adibi M, Thomas A Z, et al. Predicting adherent perinephric fat using preoperative clinical and radiological factors in patients undergoing partial nephrectomy[J]. Eur Urol Focus, 2021, 7(2): 397-403.
[13] Dell-Kuster S, Gomes N V, Gawria L, et al. Prospective validation of classification of intraoperative adverse events (ClassIntra): international, multicentre cohort study[J]. Bmj, 2020, 370: m2917.
[14] Mitropoulos D, Artibani W, Biyani C S, et al. Validation of the Clavien-Dindo grading system in urology by the European Association of Urology Guidelines Ad Hoc Panel [J]. Eur Urol Focus, 2018, 4(4): 608-613.
[15] Wahal S P, Mardi K. Multilocular cystic renal cell carcinoma: a rare entity with review of literature [J]. J Lab Physicians, 2014, 6(1): 50-52.
[16] Schoots I G, Zaccai K, Hunink M G, et al. Bosniak classification for complex renal cysts reevaluated: a systematic review[J]. J Urol, 2017, 198(1): 12-21.
[17] Silverman S G, Pedrosa I, Ellis J H, et al. Bosniak classification of cystic renal masses, version 2019: an update proposal and needs assessment[J]. Radiology, 2019, 292(2): 475-488.
[18] Pruthi D K, Liu Q Q, Kirkpatrick I D C, et al. Long-term surveillance of complex cystic renal masses and heterogeneity of bosniak 3 lesions[J]. J Urol, 2019. DOI: 10.1097/JU.0000000000000144.
[19] PAN X Y, ZHANG M N, YAO J, et al. Fumaratehydratase-deficient renal cell carcinoma: a clinicopathological and molecular study of 13 cases[J]. J Clin Pathol, 2019, 72(11): 748-754.
[20] Daza J, Okhawere K E, Ige O, et al. The role of RENAL score in predicting complications after robotic partial nephrectomy[J]. Minerva Urol Nephrol, 2022, 74(1): 57-62.
[21] Yagisawa T, Takagi T, Yoshida K, et al. Surgical outcomes of robot-assisted laparoscopic partial nephrectomy for cystic renal cell carcinoma[J]. J Robot Surg, 2022, 16(3): 649-654.
[22] CHEN S Z, WU Y P, CHEN S H, et al. Risk factors for intraoperative cyst rupture in partial nephrectomy for cystic renal masses[J]. Asian J Surg, 2021, 44(1): 80-86.
[23] Khene Z E, Peyronnet B, Mathieu R, et al. Analysis of the impact of adherent perirenal fat on peri-operative outcomes of robotic partial nephrectomy[J]. World J Urol, 2015, 33(11): 1801-1806.
[24] Khene Z E, Dosin G, Peyronnet B, et al. Adherent perinephric fat affects perioperative outcomes after partial nephrectomy: a systematic review and meta-analysis[J]. Int J Clin Oncol, 2021, 26(4): 636-646.
(下转页)
(上接页)
[25] Abdallah N, Wood A, Benidir T, et al. AI-generated R.E.N.A.L.+ score surpasses human-generated score in predicting renal oncologic outcomes[J]. Urology, 2023. DOI: 10.1016/j.urology.2023.07.017.
[26] 郑亮, 陈博宏, 黄昊翔, 等.通过优化RENAL和MAP评分构建预测机器人辅助肾部分切除术围手术期结局的RP评分系统[J/OL].现代泌尿外科杂志, 1-6[2024-12-16]. http: //kns.cnki.net/kcms/detail/61.1374.R.20240829.1013.002.html.
[27] JIN D C, ZHANG J Y, ZHANG Y F, et al. A combination of the mayo adhesive probability score and the RENAL score to predict intraoperative complications in small renal masses[J]. Urol Int, 2020, 104(1-2): 142-147.
[28] YANG B, MA L L, QIU M, et al. A novel nephrometry scoring system for predicting peri-operative outcomes of retroperitoneal laparoscopic partial nephrectomy[J]. Chin Med J (Engl), 2020, 133(5): 577-582.
[29] TAN X J, JIN D C, HU J, et al. Development of a simple nomogram to estimate risk for intraoperative complications before partial nephrectomy based on the mayo adhesive probability score combined with the RENAL nephrometry score[J]. Investig Clin Urol, 2021, 62(4): 455-461.
[30] Crockett M G, Giona S, Whiting D, et al. Nephrometry scores: a validation of three systems for peri-operative outcomes in retroperitoneal robot-assisted partial nephrectomy[J]. BJU Int, 2021, 128(1): 36-45.
收稿日期:2024-08-14
编辑:张笑嫣
基金项目:陕西省重点研发计划项目(2018SF-158)
Foundation Item: Key Ramp;D Plan Project of Shaanxi Province (2018SF-158)
通讯作者:吴大鹏,Email:wudapeng@xjtufh.edu.cn
Corresponding Author: WU Dapeng, Email: wudapeng@xjtufh.edu.cn
引用格式:王宝,陈博宏,黄昊翔,等.肾肿瘤解剖评分联合肾周脂肪粘连评分对囊性肾肿物患者围手术期结果的预测价值分析[J].机器人外科学杂志(中英文),2025,6(1):107-112,117.
Citation: WANG B, CHEN B H, HUANG H X, et al. Value of renal tumor anatomy score combined with perirenal fatty adhesions score in predicting perioperative outcomes of patients with cystic renal masses[J]. Chinese Journal of Robotic Surgery, 2025, 6(1): 107-112, 117.