
Unlocking the versatile potential: Adipose-derived mesenchymal stem cells in ocular surface reconstruction and oculoplastics
2024-03-24 12:03PierLuigiSuricoAnnaScarabosioGiovanniMiottiMartinaGrandoCarloSalatiPierCamilloParodiLeopoldoSpadeaMarcoZeppieri
World Journal of Stem Cells 2024年2期
Pier Luigi Surico,Anna Scarabosio,Giovanni Miotti,Martina Grando,Carlo Salati,Pier Camillo Parodi,Leopoldo Spadea,Marco Zeppieri
Abstract This review comprehensively explores the versatile potential of mesenchymal stem cells (MSCs) with a specific focus on adipose-derived MSCs.Ophthalmic and oculoplastic surgery,encompassing diverse procedures for ocular and periocular enhancement,demands advanced solutions for tissue restoration,functional and aesthetic refinement,and aging.Investigating immunomodulatory,regenerative,and healing capacities of MSCs,this review underscores the potential use of adipose-derived MSCs as a cost-effective alternative from bench to bedside,addressing common unmet needs in the field of reconstructive and regenerative surgery.
Key Words: Stem cells;Adipose stem cell;Ocular therapy;Oculoplastics;Regenerative
INTRODUCTION
The field of oculoplastic surgery,which encompasses a wide array of procedures to enhance the form and function of the eye and its surrounding structures,has long been a domain of meticulous precision and innovative approaches.From repairing damaged ocular tissues to restoring the aesthetic aspects of periocular regions,oculoplastics demand novel solutions that promote both efficacy and safety.Mesenchymal stem cells (MSCs) emerge as a beacon of hope in this intricate landscape.These versatile cells,well-known for their regenerative abilities in various medical disciplines,hold immense promise in oculoplastics.The human eye and its adjacent tissues are an intricately interconnected system comprising muscle,adipose tissue,ocular surface,and skin.Each component plays a vital role in ocular health,appearance,and function.
In recent years,the field of regenerative medicine has witnessed a paradigm shift in the quest for innovative therapeutic strategies,particularly in the realm of ocular surface reconstruction and oculoplastics.Among the various cell types under investigation,adipose-derived MSCs have emerged as promising candidates due to their unique characteristics,including easy accessibility,abundant supply,and robust regenerative properties.This comprehensive review aims to unravel the versatile potential of MSCs in the context of ocular surface reconstruction and oculoplastics,shedding light on their mechanisms of action,preclinical and clinical applications,and the current challenges and prospects in harnessing their therapeutic efficacy.
Understanding the multifaceted roles of MSCs in ocular tissue regeneration is paramount for advancing clinical interventions and enhancing patient outcomes.The review was performed by using PubMed (https://pubmed.ncbi.nlm.nih.gov) andReference Citation Analysis(RCA) (https://www.referencecitationanalysis.com).As we delve into the intricate interplay between MSCs and the ocular microenvironment,this review will explore the molecular and cellular mechanisms underlying their immunomodulatory effects,paracrine signaling,and differentiation capacities.Furthermore,a critical examination of the existing preclinical studies and clinical trials will provide a comprehensive overview of the safety and efficacy profiles of MSC-based therapies,paving the way for a nuanced understanding of their translational potential in the field of ophthalmology.
MSCs
In 2006,the Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy issued a position statement with the intent of providing clarity regarding the terminology “multipotent mesenchymal stromal cells”.They established specific criteria for the identification of MSCs,requiring that these cells exhibit characteristics such as adherence to plastic surfaces,clonogenic ability,the presence of certain cell surface markers (CD73,CD90,CD105),and the absence of hematopoietic and endothelial markers (CD45,CD34,CD14,CD11b,CD79α,CD19,HLA-DR)[1].Additionally,these MSCs must demonstrate the potential forin vitrodifferentiation into mesodermal cell lineages[2,3].
MSCs,renowned for their remarkable plasticity,have long been a subject of interest due to their potential for tissue repair and regeneration[4,5].These versatile cells can be harvested from a wide array of sources,including bone marrow,nervous tissue,adipose tissue,amniotic fluid,placenta,and the Wharton’s jelly of the umbilical cord[6-11].MSCs possess an impressive capacity for self-renewal,maintaining their characteristics over multiple passages without significant alteration[12,13].
MSCs exhibit the unique ability to differentiate into various mesenchymal lineages,encompassing adipocytes,chondrocytes,and osteocytes[14].Notably,it has been demonstrated that specific MSC-like cells from both mice and humans can be induced to differentiate into cells of neuroectodermal and endodermal lineages,including neurons,endothelial cells,and hepatocytes[15-18].
Furthermore,MSCs exhibit a notable inclination to target areas of tissue injury or inflammation upon intravenous administration[19-21].This characteristic enhances their appeal,particularly in the context of tissue repair and the maintenance of immune homeostasis.Their substantial immunoregulatory capacities,which involve the secretion of antiinflammatory factors,empower MSCs to finely tune both innate and adaptive immune responses,ultimately facilitating a state of immunosuppression[19,22].
Interestingly,MSCs are known to secrete numerous substances into the medium in which they are cultured[23].This cocktail of secretions is referred to as the MSC secretome and comprises soluble factors (cytokines,chemokines,growth factors,immunomodulatory proteins,and mitogenic factors) and membrane-bound vesicles (microvesicles and exosomes)[24].MSCs-secretome treatment has been successfully and safely tested in several fields such as wound healing,myocardial infarction,liver injury,cerebral ischemic disease,spinal cord injury,lung diseases,urologic disorders,ocular diseases inflammatory arthritis,and bone defects[25-33].
ADIPOSE-DERIVED MSCs
Adipose tissue offers a more abundant supply of MSCs and is relatively easier to access compared to bone marrow,making it an appealing choice for clinical applications.However,it’s worth noting that reports suggest variations in the properties of MSCs derived from these two tissue sources.Inconsistencies in the findings across studies can be attributed to the diversity in cell preparations,which may result from differences in extraction methods,culture conditions,as well as the age and gender of the donors[34,35].
Adipocytes represent only 25% of the total number of cells in fat tissue,despite accounting for 80% to 90% of its volume.The remaining 75% of the cells,known as the stromal vascular fraction (SVF),are rich in adipose-derived stem cells,endothelial cells,granulocytes,monocytes,macrophages,and lymphocytes[35-37].
However,the significant advantage of adipose tissue lies in its potential to yield a substantially higher number of stem cells -estimated to be 100 to 500-fold greater than that obtained from bone marrow aspirate[38].This characteristic has piqued the interest of plastic surgeons,and various methods for isolating cells from lipoaspirate or fat tissue have become available[39,40].
In plastic surgery,procedures involving stem cell-containing tissue transplants,such as fat grafts,cell-enriched lipoaspirate,or the so-called SVF,are typically performed in the operating theatre.However,this approach often hinders the in-depth characterization of MSCs within the cell or tissue graft,including immunophenotyping,differentiation potential,assessment of senescence,and determining the proportional contribution of stem cells to the graft as a whole[40].
In addition,it has been demonstrated that the abundance of colony-forming unit-fibroblast in the adipose-derived MSCs is significantly greater than in that of bone marrow-derived MSCs,suggesting again their stronger potential in the field of plastic surgery[41].Despite these advantages of adipose-derived MSCs,there is still a need for further research toward standardized clinical procedures.
ADIPOSE-DERIVED MSCs IN PLASTIC SURGERY
Adipose stem-cell regenerative and anti-inflammatory properties make them a promising candidate in plastic surgery.Numerous applications are described,in particular in the tissue regeneration field[42,43].MSCs are capable of enhancing the survival and integration of fat grafts in procedures like lipofilling or fat transfer improving graft retention and promoting better tissue integration[44].As already mentioned,MSCs play a certain role in tissue repair and wound healing[43].Their ability to modulate the immune response and stimulate the formation of new blood vessels can contribute to improved healing outcomes in plastic surgery procedures.These staminal cells also have anti-inflammatory properties,which can be beneficial in reducing inflammation and promoting a more favorable healing environment.This is particularly relevant in procedures where inflammation can impact outcomes,such as tissue reconstruction or scar revision like breast surgery[45].Moreover,the regenerative properties of MSCs may contribute to minimizing scar formation[46].Research suggests that MSCs can modulate the collagen production and remodeling process,potentially leading to less noticeable scars[47].
MSCs demonstrated to play a role also in the cosmetic area of plastic surgery for their potential to stimulate collagen production and improve skin quality[42,48].In procedures involving bone or cartilage reconstruction,such as craniofacial surgery or rhinoplasty,MSCs may be used to enhance the regenerative capacity of the implanted tissues.Otherwise,it is important to note that while there is promising research in these areas,the use of MSCs in plastic surgery is still an evolving field and more clinical studies are needed to establish the safety and efficacy of these approaches.
APPLICATION OF ADIPOSE-DERIVED MSCs IN OCULOPLASTICS
Adipose-derived MSCs do have a great potential for application in oculoplastics surgery.This encompasses a variety of subfields starting with eyelid reconstruction,going through lacrimal gland development,and ending with cosmetic surgery.Possible applications may be potentially endless.Stem cell biology in oculoplastic is still at the beginning of its path but is already a central topic[49] (Table 1).
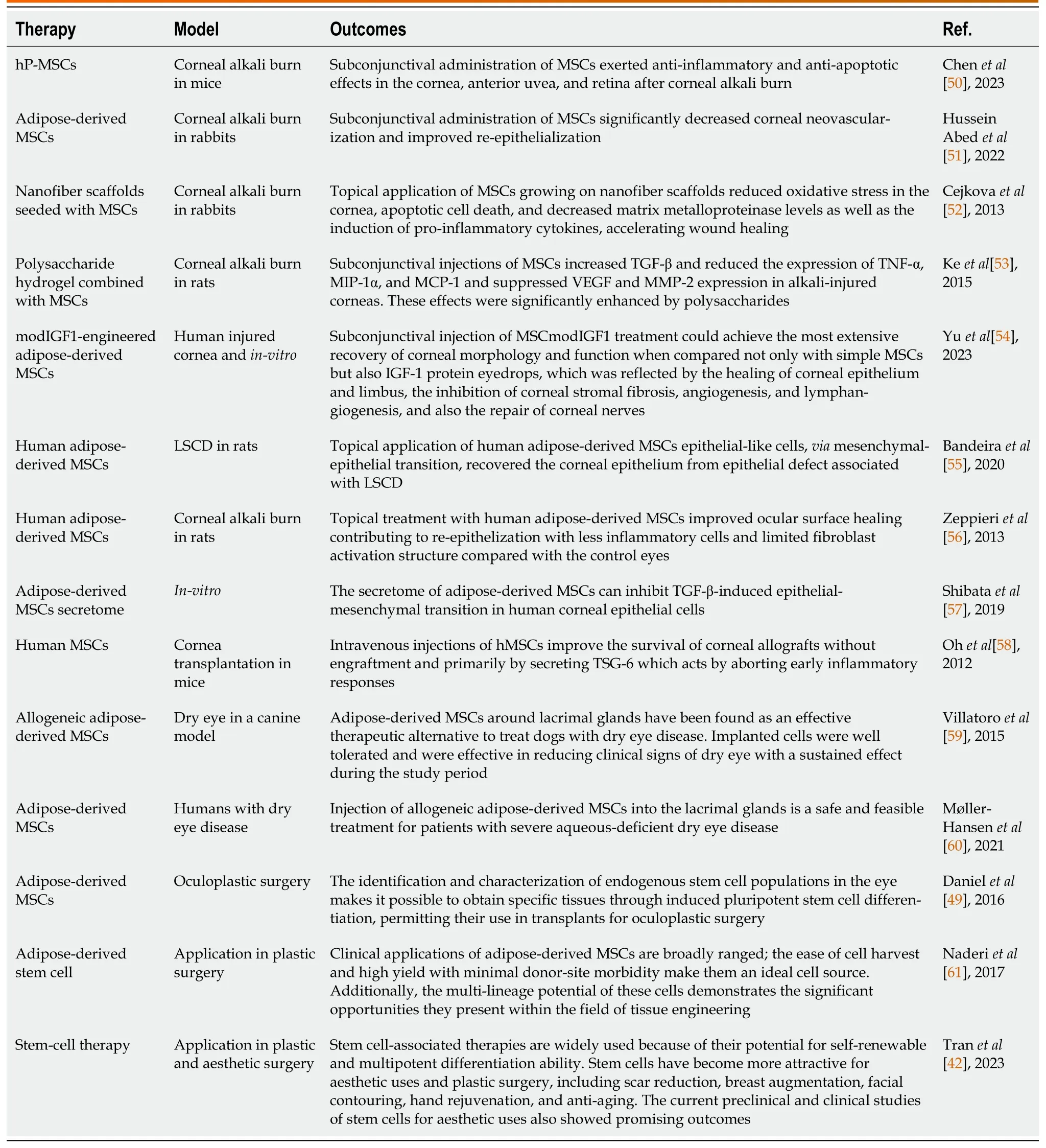
Table 1 Studies included from literature about mesenchymal stem cells applications in ocular and periocular reconstructive surgery
Stem cells mean regeneration.This concept is extremely interesting in the ocular area in which we find highly specialized tissue that is difficult to replace in other ways.In plastic surgery the main concept is “like-to-like”reconstruction or replacement.This is our mantra whenever a flap is raised and set.What if there are no similar tissues?Stem cells may be the only appropriate answer.And adipose-derived MSCs are incredibly important in the topic.Due to the high variety of applications these may have in oculoplastic,in our review two main chapters have been identified: (1)Ocular surface reconstruction;and (2) Periocular.
In ocular surface MSCs have shown great promise in the treatment of ocular surface disorders.These cells may have anti-inflammatory and regenerative properties,making them potential candidates for conditions like dry eye syndrome or chemical burns affecting the ocular surface[49].Periocular applications are even wider but probably even less explored.
It is important to note that while the potential applications of stem cells in oculoplastic are promising,research in this field is ongoing,and many aspects,including safety and long-term effectiveness,are still being explored.Additionally,ethical considerations and regulatory frameworks surrounding the use of stem cells need to be carefully addressed.As with any medical advancement,the translation of stem cell research into clinical practice requires rigorous testing and validation through well-designed clinical trials before becoming standard treatments.
OCULAR SURFACE RECONSTRUCTION
The ocular surface constitutes a complex system perpetually exposed to a multitude of stimuli capable of disturbing its equilibrium.Damage to the ocular surface can arise from various sources,including external factors such as mechanical traumas,chemical burns,adverse effects of topical medications,or may result from inflammatory processes that encompass conditions such as mucous membrane pemphigoid (MMP),Stevens-Johnson Syndrome,and graft-versus-host disease,all of which can engender substantial damage to the ocular surface,particularly affecting corneal transparency[62-66].Such damage may also extend to the associated ocular structures,involving the conjunctiva and eyelids,resulting in cicatricial alteration of the ocular surface[62].
An additional and formidable consequence of these alterations to the ocular surface is the impairment of limbal stem cells located in the corneal limbus,a condition known as limbal stem cell deficiency (LSCD)[67].Impairment of these stem cells’ regenerative capacity can lead to conjunctivalization of the cornea,resulting in the loss of transparency and,consequently,visual function,requiring optimization of the ocular surface by a wide range of treatments from medical management to eyelid,corneal,and conjunctival reconstruction[68].
Corneal transplantation and stem cell transplantation stand as pivotal surgical procedures within ocular surface reconstruction,addressing a range of conditions and playing a critical role in vision restoration[69,70].However,they can be characterized by a risk of rejection,a challenge that poses complexity in managing the postoperative phase[71,72].
Furthermore,akin to other organs within the human body,the ocular surface undergoes the natural aging process,which can manifest in various forms,with the most common disorder being dry eye syndrome[73].These aging processes can have a significant impact on patients’ quality of life.In this complex field,MSCs represent a promising novel regenerative approach to such a wide range of pathologies,requiring more in-depth characterization of their function in the different clinical subsets[74].
Chemical injuries
Chemical injuries to the cornea are the most common type of ocular and periocular injury and can vary widely in severity[75,76].These injuries range from minor damage that affects only the outer layer of the corneal surface to more severe burns that penetrate deep into the layers of the cornea[77],resulting in inflammation,scarring,and impairment of vision[76].Consequently,immediate assessment and treatment of chemical burns are crucial to restore and preserve ocular surface integrity[78].Notably,alkali burns are particularly concerning.Unlike acid burns,alkalis penetrate the tissues by causing membrane lipid saponification and collagen matrix denaturation,leading to tissue necrosis and further damage by disrupting the balance between pro-oxidant and antioxidant substances[79].
MSCs,when transferred to the damaged corneal surface,ameliorate alkali-induced oxidative damage,reducing apoptosis,matrix metalloproteinases,and pro-inflammatory cytokines[50].Moreover,adipose-derived MSCs showed the ability to suppress corneal inflammation and neovascularization while significantly expediting corneal healing following alkali burn in various animal models[50,51,80].
It has been reported that MSCs,when combined with polysaccharide scaffold demonstrated an additive effect[81].This effect was observed in the upregulation of anti-inflammatory cytokines,specifically transforming growth factor beta(TGF-β),and antiangiogenic cytokine thrombospondin 1[53].Moreover,adipose-derived MSCs have been associated with a concurrent downregulation of pro-inflammatory cytokines like tumor necrosis factor alpha (TNF-α),chemotactic factors such as macrophage inflammatory protein-1alpha and monocyte chemoattractant protein-1 (MCP-1),as well as proangiogenic factors like vascular endothelial growth factor (VEGF) and MMP-2,showing promising result for a new therapeutic use of MSCs[52,82].
Using anin vivomouse model of ocular injury,it has been shown that MSCs have the capacity to restore corneal transparency by secreting high levels of hepatocyte growth factor (HGF) and subsequently inhibiting myofibroblast generation.Interestingly,in the same study HGF alone was able to restore corneal transparency,an observation that supports the rationale of using specific MSC-secreted factors to treat ocular diseases[83].
Hence,in addition to their primary anti-inflammatory role in the context of chemical burns,the regenerative function of adipose-derived MSCs has been demonstrated in promoting the regeneration of the corneal epithelium[54].Specifically,adipose-derived MSCs have clearly shown this regenerative potential[54,55,84-86].
LSCD
In the treatment of unilateral limbal stem cell loss,autologous limbal cell transplantation has been widely validated as a therapeutic option[87].However,in cases of bilateral damage,allogeneic limbal cell transplantation is indicated[68],however,it presents a high risk of rejection and requires prolonged systemic immunosuppressive therapy[88].Therefore,within this field,MSCs have been demonstrated to offer a genuine alternative to these limitations[89].Specifically,adipose-derived MSCs have been shown to be modulated to promote wound healing and reduce inflammation[86,90].It has been demonstrated that adipose-derived MSCs topically administrated in a rat corneal burn model rapidly reach the corneal epithelium and stroma after the application of the cells[56].Human adipose-derived MSCs,when transplanted onto the ocular surface of rabbits with partial and total LSCD models,promoted the expression of corneal epithelial cell markers such as CK3 and E-cadherin,and the limbal epithelial cell markers CK15 and p63[86].Adipose-derived MSCs exhibited good tolerance,migrated to inflamed areas,diminished inflammation,and hindered the progression of corneal neovascularization and opacity,enhancing the corneal healing process.
Interestingly,priming human adipose-derived MSCs with a specific medium optimized for limbal stem cell conditions enhanced their ability to improve corneal wound healing,suppressing inflammation with the downregulation of proinflammatory TNF-α,MMP-2,interleukin (IL)-6,and MCP1.The fact that MSCs function in a paracrine contextdependent manner makes it promising to enhance their capacityin vitroto improve the healing of ocular surface wounds[90].
When examining thein vitrodifferentiation of MSCs into corneal epithelial and limbal stem cells,it has been demonstrated that adipose-derived MSCs exhibit a foundational expression of corneal epithelial cell markers like ABCG2,p63,CK12,and CK16[91,92].Moreover,several studies have indicated their differentiation into these cells in response to specific media[90,93].
Another concept that has to be investigated regarding the mechanism of MSCs function is the epithelial-mesenchymal transition (EMT).EMT refers to the transformation of polarized epithelial cells into mesenchymal-or myofibroblast-like cells[94,95].This process contributes to tissue homeostasis maintenance.However,a prolonged inflammatory state or excessive EMT can lead to tissue fibrosis in organs,as often observed in the context of LSCD[96].There is also evidence suggesting the involvement of EMT in ocular surface diseases such as pterygium[97] and corneal subepithelial fibrosis[95].Therefore,suppressing EMT on the ocular surface could be an effective treatment for EMT-related ocular surface diseases to maintain homeostasis.In this regard,it has been demonstrated that the adipose-derived secretome attenuated TGF-β1-induced EMT phenotypes in corneal epithelial cells[57].
Similarly,in the realm of reducing fibrosis in skin wound healing,it has been shown that the paracrine action of MSCs delivered by microspheres could serve as a promising strategy to boost tissue repair and curb excessive TGF-β mediated fibrosis in cutaneous wound healing[98],suggesting a multifaceted and promising role in harnessing the potent paracrine action of adipose-derived MSCs in ocular and periocular applications[99].
Corneal transplantation
Due to their immunomodulatory traits,MSCs offer potential in corneal allograft transplantation which remains a main procedure in the field of ocular surface reconstruction.While corneal allografts boast high survival rates due to immune privilege,the risk of immune rejection remains the primary cause of graft failure[71,100].
Moreover,MSCs’ paracrine function shows promising potential in corneal transplantation by influencing the environment and immunoregulation adipose-derived MSCs secrete growth factors such as platelet-derived growth factor,VEGF,HGF,and TGFβ1[101,102].These factors induce neovascularization,beneficial in ischemic conditions[103,104] but concerning in avascular corneal transplants,elevating the risk of rejection[72].Despite adipose-derived MSCs also secreting IL-6 and IL-8,their impact,including the potential for rejection responses,appears to vary based on the environment,underlining the contextual influence of adipose-derived MSCs therapy and its role in suppressing inflammation and immune reaction signaling[93].Across several investigations,the several routes of administration of adiposederived MSCs topically[105],subconjunctivally[106],using amniotic membranes,or utilizing other substrates like contact lenses have been established[105,106].
Human adipose-tissue MSCs have been proven to be effective in restoring and enhancing corneal and limbal epithelial cell function in animal LSCD models[74,86,105].These results indicate that MSCs contribute to the recovery of the corneal epithelium with paracrine mechanism rather than by a trans-differentiation process.Moreover,given the lowimmunogenic proprieties of adipose-derived MSCs,they appear to be a potential solution for complex cases of ocular surface failure that require transplantation,representing a cost-effective alternative to the current therapies.
Various evidence suggests a preventive role of MSCs in corneal transplant rejection.Infusing MSCs with cyclosporine post-surgery extends graft survival by inhibiting T helper type 1 (Th1) cytokine production and enhancing regulatory T cell immunosuppressive function[107].Another study highlighted pre-surgical MSC administration’s ability to diminish surgery-related inflammation,extending graft survival by reducing rejection immune response[58].However,a pig-to-rat corneal transplantation model showed no benefit from MSC infusion,potentially due to increased Th2 cytokine production[108].Despite the need for further studies,applying adipose-derived MSCs as cell therapy for graft-rejection prevention remains a promising area to explore,potentially extendable to fields like skin transplantation,particularly relevant in oculoplastic practice[109].
Ocular surface ageing
The ocular surface undergoes the effects of aging due to continual exposure to environmental elements and various irritants and dry eye disease (DED) is the most prevalent age-related ocular surface condition,which poses challenges in treatment,demanding a multifaceted therapeutic approach[110,111].In the elderly,the immune system often exhibits a chronic,mild inflammatory condition known as inflammaging[73,112].This state is linked to the dysregulation of the immune system referred to as immunosenescence[113,114].Additionally,it reduces the resilience and capacity of aged bodies to withstand internal or external stressors.In this scenario,although oculoplastic procedures aid in the anatomical,mechanical,and aesthetic restoration of the ocular and periocular region,they can stress the ocular surface,especially in older individuals[115].Consequently,stabilizing the ocular surface before and after any ophthalmic,ocular,or periocular procedure becomes crucial[115-117].Current treatment approaches predominantly encompass artificial tear replacement therapy,anti-inflammatory interventions,and localized immunosuppressive strategies[118].
While the exact pathogenesis of DED remains not entirely comprehended,it is acknowledged that inflammation and the breakdown of ocular surface immunoregulation significantly contribute to the advancement of the disease[119,120].Considering the ability of MSCs to aid in tissue repair by suppressing inflammation,recent investigations have delved into the therapeutic prospects of MSCs within the realm of DED[121].Previous studies have shown that the number of conjunctival goblet cells increases after treatment with adipose-derived MSCs in animal dry eye models[122,123].
Studies have shown that adipose-derived MSCs can significantly promote lacrimal gland regeneration and increase tear secretion[124].Injecting adipose-derived MSCs into the lacrimal glands of dogs with dry eyes led to an improvement in dry eye signs and good tolerance[59,125].A clinical trial in which allograft adipose derived-MSCs were administered into the lacrimal glands of patients with severe lacrimal defects.The results similarly showed that MSCs are well tolerated and promote improvement in ocular surface signs and symptoms[60].Additionally,derived-MSCs exosomes treated dry eye in a murine model and have been able to decrease pro-inflammatory cytokines,promote corneal epithelial repair,and increase tear secretion by inhibiting pro-inflammatory and apoptotic pathways[126].
Finally,it has also been shown that therapy using MSCs conditioned media may enhance the effectiveness of dry eye treatment through the suppression of inflammation and apoptosis,as well as by encouraging tear secretion and fostering the proliferation of corneal epithelial cells,highlighting the potential of MSCs secretome[31].
Further studies are necessary to validate adipose-derived MSCs therapy in the domain of the ocular surface.However,by consolidating these outcomes,they may potentially play a significant role as a therapy that amalgamates a multidisciplinary approach in the treatment of the ocular surface,particularly intriguing in the field of oculoplastic surgery.
PERIOCULAR SURGERY
Applications
The application of stem cells in the periocular area involves various techniques[49,127].First of all,stem cell or stem cellderived products may be applied topically to the skin in the periocular region[128].This could involve the use of creams,gels,or serums containing stem cells or their derivatives.The idea is that these products may stimulate skin regeneration,improve elasticity,and contribute to a more youthful appearance[128].MSCs can be injected directly into the periocular tissues.This may be done using various injection techniques,such as microinjections or more targeted approaches.The injected stem cells could potentially contribute to tissue regeneration and the improvement of skin quality.These therapies may be combined with other cosmetic or reconstructive procedures in the periocular area.For example,these could be applied in conjunction with eyelid surgery to enhance the overall aesthetic outcome and promote better tissue healing[129,130].Promoting wound healing after periocular surgeries or injuries may become a game changer in this field,particularly in reducing the retraction effect.
Indications
The periocular region,which includes the area around the eyes,eyebrows,and temples,is of particular interest in the field of regenerative medicine and stem cell research.The periocular application of stem cells holds promise for various therapeutic purposes,including both cosmetic and reconstructive procedures.
Cosmetic
As previously mentioned,stem cells stand for regeneration.The cosmetic field has itself a regenerative effort: Restoring something that time had changed.Therefore,stem cell treatment may become a cornerstone.
Rejuvenation
The regenerative properties of stem cells could contribute to skin renewal,reducing wrinkles,and improving skin elasticity.This might involve the application of stem cells directly to the skin or in conjunction with other cosmetic procedures.In particular eyelid rejuvenation is one of the most frequently requested procedures[49,131].
Scar treatment
In the last decade,numerous procedures have been proposed to improve scars.There in the periocular region may be particularly challenging to treat because of the highly functional demand.Surgery is commonly useful to major retraction areas but stem cell treatment may be also explored.The regenerative properties of stem cells could aid in tissue repair and promote a more natural and aesthetically pleasing outcome[43,46,129].
Hair restoration
For individuals experiencing hair loss in the eyebrows or eyelashes,stem cells might be investigated for their role in promoting hair follicle regeneration and improving hair density in the periocular area[132,133].
Reconstructive
Similarly,reconstructive surgery is deeply connected to stem cell treatment.MSCs have already demonstrated their capacity to stimulate wound healing,neovascularization,and tissue regeneration[43,44,61,134].These,through fat grafting,are already a well-established procedure to improve radiotherapy-damaged skin.The same principle may also be applied to ocular/periocular cancers.In these patients,good skin quality is essential to be able to wear an ocular prosthesis when needed.Eyelid malposition correction may be combined with fat grafting to improve the outcome and to apply a regenerative boost[135].In some cases,micro fat grafting applied to the upper lid seems to improve levator palpebrae superioris muscle in mild ptosis[130].This application needs to be explored.
OTHER KINDS OF MSCs
MSCs are highly heterogeneous multipotent stromal cells that can be found in various tissues throughout the body.Autologous adult stem cells have consistently served as the primary cell type employed in various applications due to their immuno-compatibility,and their utilization poses minimal ethical concerns[136].This stands in stark contrast to the use of embryonic stem cells (ESCs),umbilical cord MSCs (UCMSCs),and induced pluripotent stem cells (iPSCs),each of which has encountered substantial limitations in clinical practice[137].These constraints primarily revolve around issues concerning cellular regulation and the potential for teratoma formation,ethical dilemmas,immunogenicity (in the case of ESCs),genetic manipulation complexities (associated with iPSCs),and difficulties related to the long-term preservation of UCMSCs[138,139].In this review,we included studies about different sources of MSCs to support the wide array of functions that MSCs can potentially express in the field of ocular surface reconstruction and oculoplastics.However,the main focus stays on adipose-derived MSCs,since adipose tissue offers a more abundant supply of MSC cells and is relatively easier to access compared to other sources[38].
ACCELERATING THE CLINICAL USE OF MSCs
As of today,the primary issue in the application of MSCs appears to be their inability to survive at the site of administration.We should likely focus on this aspect to assess their actual clinical efficacy.Various factors contribute to this challenge and understanding them is crucial for developing strategies to enhance the survival and therapeutic potential of MSCs in clinical settings.Further investigation into the survival mechanisms,interaction with the host microenvironment,and optimization of delivery methods may provide valuable insights for addressing this critical concern in MSCbased therapies.Various clinical trials are ongoing.
CONCLUSION
In conclusion,this review illuminates the versatile potential applications of adipose-derived MSCs in oculoplastics,emphasizing their ease of harvesting,cost-effectiveness,safety,and efficacy.While the current evidence suggests their promising role in various clinical scenarios,further studies are warranted to elucidate the precise mechanisms of action and functions of MSCs,particularly in the context of wound healing,inflammation,and regenerative and reconstructive procedures in ophthalmology and plastic surgery.Optimizing and standardizing protocols for the application of MSCbased cell therapy will be crucial for unlocking their full therapeutic potential in addressing the intricate challenges posed by ocular surface and periocular conditions.Moreover,the main issue to untangle consists of their effective survival in the donor area.Many unsatisfactory clinical results may be due to the poor survival rate.Further high-quality basic and clinical studies are needed to finally be able to apply MSCs successfully in our daily clinical practice.
FOOTNOTES
Co-first authors:Pier Luigi Surico and Anna Scarabosio.
Author contributions:Surico PL and Scarabosio A contributed equally to the manuscript as co-first authors.Surico PL,Scarabosio A,Miotti G,Grando M,Salati C,Parodi PC,Spadea L,and Zeppieri M wrote the outline;Surico PL and Scarabosio A did the research and writing of the manuscript;Miotti G,Grando M,Salati C,Parodi PC,Spadea L,and Zeppieri M assisted in the writing of the paper;Zeppieri M was responsible for the conception and design of the study and completed the English and scientific editing (a native English speaking MD,PhD);Surico PL,Scarabosio A,Miotti G,Grando M,Salati C,Parodi PC,Spadea L,and Zeppieri M assisted in the editing and making critical revisions of the manuscript;and all authors provided the final approval of the article.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Italy
ORCID number:Giovanni Miotti 0000-0003-3185-7595;Martina Grando 0000-0002-1877-3621;Carlo Salati 0000-0003-4736-5296;Pier Camillo Parodi 0000-0002-4677-8198;Leopoldo Spadea 0000-0002-1190-3956;Marco Zeppieri 0000-0003-0999-5545.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Yuan YY
 World Journal of Stem Cells2024年2期
World Journal of Stem Cells2024年2期
- World Journal of Stem Cells的其它文章
- Multiple pretreatments can effectively improve the functionality of mesenchymal stem cells
- Cellular preconditioning and mesenchymal stem cell ferroptosis
- Therapeutic utility of human umbilical cord-derived mesenchymal stem cells-based approaches in pulmonary diseases: Recent advancements and prospects
- Crosstalk between Wnt and bone morphogenetic protein signaling during osteogenic differentiation
- Human pluripotent stem cell-derived kidney organoids: Current progress and challenges
- Recent progress in hair follicle stem cell markers and their regulatory roles