
Vitamin D deficiency among outpatients and hospitalized patients with diabetic foot ulcers: A systematic review and meta-analysis
2023-11-18 08:47:38HyderOsmanMirghani
World Journal of Meta-Analysis 2023年5期
Hyder Osman Mirghani
Abstract
Key Words: Vitamin D deficiency; Diabetic foot ulcer; Outpatient; Hospitalized patients; Diabetic foot syndrome
INTRODUCTION
Diabetes mellitus (DM) is an epidemic globally.DM is a morbid disease with many complications including microvascular and microvascular disease.Diabetic foot syndrome (DFS) is defined as peripheral neuropathy, limited joint mobility, peripheral arterial disease, immunopathy, ulceration, and Charcot arthropathy[1].The combination of FS elements provides an environment for unrecognized injury, foot infection, and possible amputation[2].DFS is characterized by peripheral arterial disease,but the symptoms are masked by the accompanying peripheral neuropathy.The pathology varies from pre-ulcerative callouses, ulceration, and necrosis developing at the site of high pressure (deformities of the toes and feet).Patient education and feet inspection are mandatory because repetitive trauma might pass unnoticed due to the loss of pain sensation[3].DFS is a common complication of diabetes with a great economic burden; DTS substantially affects the patient's quality of life and leads to premature death.In addition, patients with DFS are prone to psychiatric disease[4].
There are nearly 40 classifications for DFS, with wide variation depending on the availability of resources and geographical variations.It is recommended to use classification in light of specific indications.Few classifications have been validated for use; the site, ischemia, neuropathy, bacterial infection, area, and depth (SINBAD) is six questions with yes or no answers with a maximum of six points.SINBAD score is better for communication between clinicians[5].While, the Infectious Diseases Society of America/International Working Group on Diabetic Foot, and wound depth, ischemia, and foot infection scoring are better for infection and perfusion respectively[6,7].The spectrum of DFS varies from minor erythema to tissue necrosis and lower limb deformity and amputation [8].The mortality of DFS is comparable to breast and lung cancer.Five-year mortality for minor and major amputations,Charcot, and DF ulcer (DFU) were 56.6%, 46.2%, 30.5%, 29%, respectively.The pooled mortality from breast, all cancer, and lung cancer were 9%, 30%, and 80% respectively[9].
The lifetime of developing FUs among patients with diabetes varies between 19% and 34% with nearly two-thirds of recurrence in 5 years, and 1 in 5 patients with moderate to severe FUs resulting in amputation.The majority of lower extremities amputations are preceded by FUs and three amputations occur every minute due to diabetes.Patients with FUs had a 2.5 times mortality rate compared to their counterparts[10,11].
25-hydroxyvitamin D (25(OH)D) is present in almost all immune cells and is a major immunomodulatory hormone.In addition, the vitamin is a potent endothelial membrane stabilizer[12].Due to its antiinflammatory effects, the active form of vitamin D plays an important role in inflammatory diseases including rheumatic disorders, and a growing piece of evidence is present regarding its effects on infectious diseases[13].Vitamin D deficiency is common; larger studies suggest that in Europe, 40% and 13% of the population are vitamin D-deficient and severely deficient, respectively[14].Vitamin D deficiency is associated with vascular diseases including DM, hypertension, and dyslipidemias[15].
The small number of included studies, including studies published by the same authors and including poster presentations[16,17], limits the previous meta-analysis on vitamin D deficiency and diabetic septic foot.Therefore, this meta-analysis investigated vitamin D levels among patients with the diabetic septic foot.
MATERIALS AND METHODS
Eligibility criteria
The studies were eligible if they compared the level of vitamin D among patients with DFU and their counterparts without DFUs and they are randomized controlled trials or case-control studies,prospective and retrospective cohorts, and cross-sectional studies.Case reports, case series, and animal and experimental studies were excluded.
Outcomes measures
The primary outcome was the level of vitamin D among patients with DFUs.
Vitamin D assessment methods
Vitamin D measurement varied between the included studies.References 18, 19, 21, and 23 used the enzyme-linked immunosorbent assay; references 20, 22, and 25 used radioimmunoassays; references 24,26, and 28 used the electrochemiluminescence immunoassay; reference 27 used liquid chromatographytandem mass spectrometry; and reference 29 used the chemiluminescence assay.
Setting and DFU definition
All of the studies used outpatients except 18, 24, 28, and 29, in which hospitalized patients were included.
Information sources and search
The researcher searched PubMed, MEDLINE, and Cochrane Library, EBSCO, and Google Scholar using the keywords DFU, DFS, diabetic septic foot, vitamin D level, 25-hydroxy vitamin D, vitamin D status,and vitamin D deficiency.The search engine was set for articles published during the period from inception to October 2022.A predetermined table was used to collect study information including author name, year of publication, country, age, sex, patient’s number in the control and interventional groups, duration of diabetes, hemoglobin A1c (HbA1c) in the intervention and control groups, vitamin D level among patients with FUs and control groups (Figure 1 and Tables 1-3).
Data analysis
The RevMan (version 5.4) system for meta-analysis was used, and the data were all continuous.We pooled data from 12 studies to compare vitamin D levels among patients with and without diabetic septic foot; a subanalysis was done to compare vitamin D among hospitalized patients.Random effect was used because significant heterogeneity was observed.Funnel plots were used to assess lateralization.P< 0.05 was considered statistically significant.
RESULTS
The current meta-analysis included 12 studies including 7619 patients.The included studies were seven cross-sectional, three prospective, and two retrospective studies; nine were published in Asia and three were from Europe[18-29].The included studies were of good quality as assessed by the Newcastle Ottawa Scale[30].Vitamin D was lower among patients with DFUs [odds ratio (OR): -5.77, 95%confidence interval (CI): -7.87 to -3.66;χ2was 84.62; mean difference, 9;I2for heterogeneity, 89%;P<0.001, andPfor overall effect < 0.001] (Figure 2).Vitamin D level was low when a subanalysis was conducted including only hospitalized patients with diabetes septic foot (OR: -6.32; 95%CI: -11.66 to -0.97;χ2was 19.39; mean difference, 2;I2for heterogeneity, 90%;P= 0.02) (Figure 3).Vitamin D level was lower among patients with DFUs after including studies that controlled for age, sex, duration of diabetes, and HbA1c (OR: -6.32; 95%CI: -923 to -3.42;χ2was 18.72; mean difference, 4;I2for heterogeneity, 79%;P< 0.001) (Figure 4).
DISCUSSION
In the present meta-analysis, vitamin D levels were lower among patients with DFUs compared to their counterparts without FUs (OR: -5.77; 95%CI: -7.87 to -3.66).There were no differences between hospitalized patients and outpatients.The results remained robust when including studies that controlled for age, sex, duration of diabetes, and HbA1c.The quality of the included studies was good[30].The current findings were in line with a narrative review including three studies[31].The present findings were similar to the first meta-analysis published by Dai and colleagues in 2019.Daiet al[16] found an association between vitamin D levels and DFUs.However, Kotaet al[32] included studies published by the same authors and some were poster presentations.Yammineet al[33] found similar results.Importantly, Yammine and colleagues included poster presentations, studies published by the same authors, and studies that assessed Charcot’s joints[34].In addition, the previous meta-analysis included Zubairet al[35] study in which vitamin D median was reported and not the mean ± standard deviation.A recently published meta-analysis reported similar findings to our results.However, the substantial heterogeneity including posters, research by the same authors, and different primary outcomes limited their results[17].The main strength of this meta-analysis is the subanalysis on vitamin D among hospitalized patients.Although a single measurement is not enough during stress, the results remain robust even among admitted patients[36].
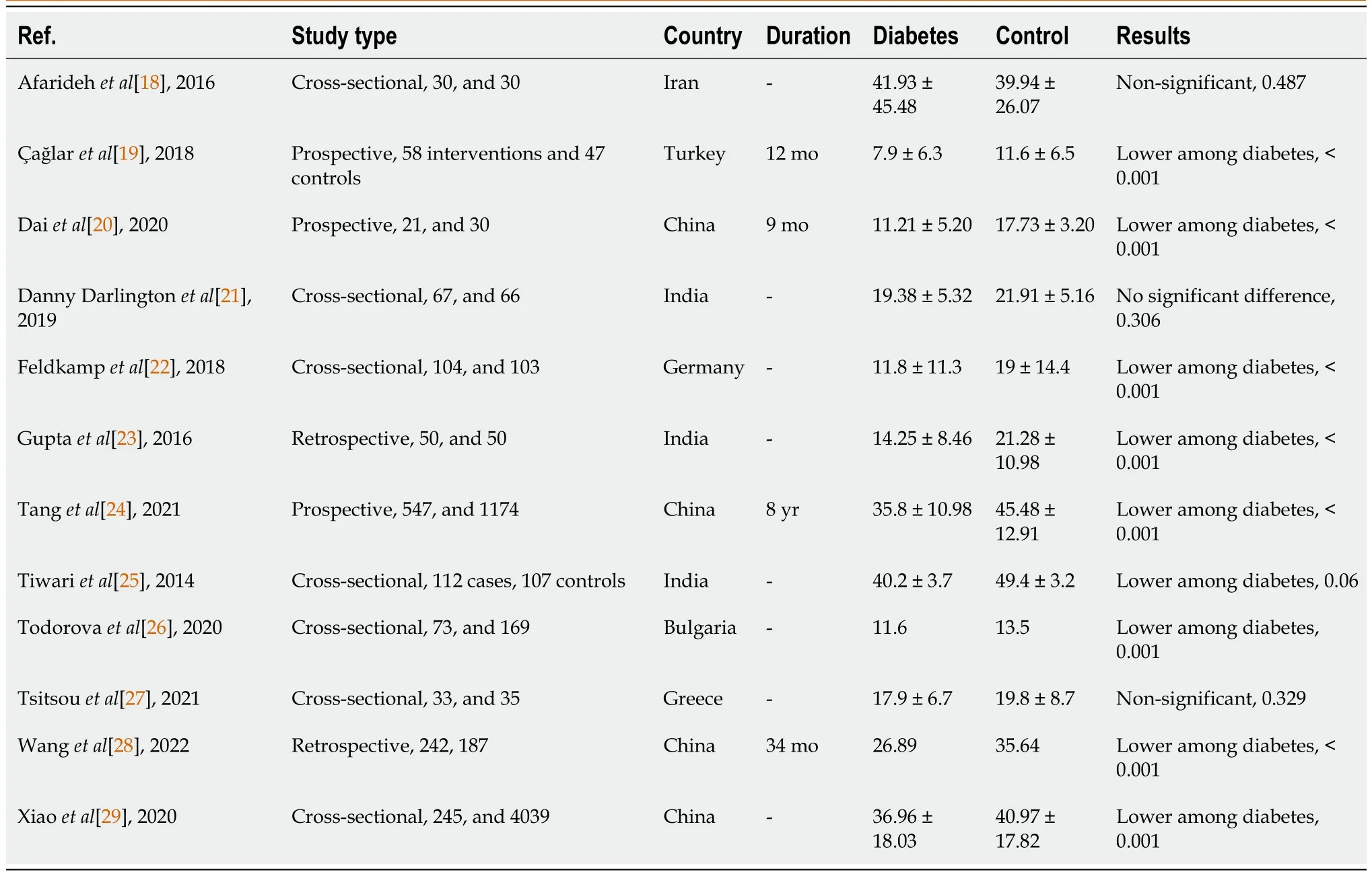
Table 1 Basic characteristics of patients with and without diabetic foot ulcers
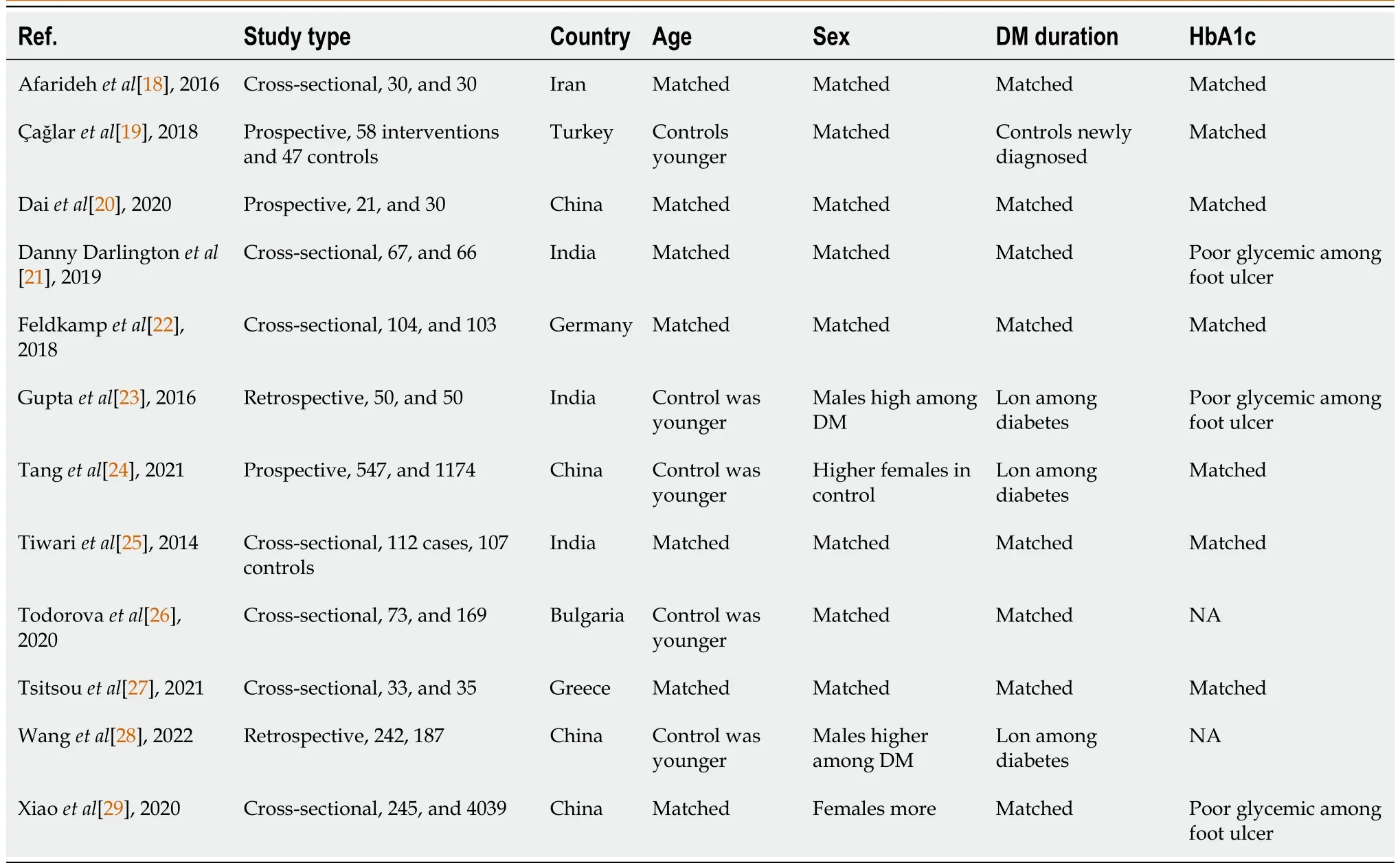
Table 2 Age, sex, duration of diabetes, and hemoglobin of patients with and without diabetic foot ulcers
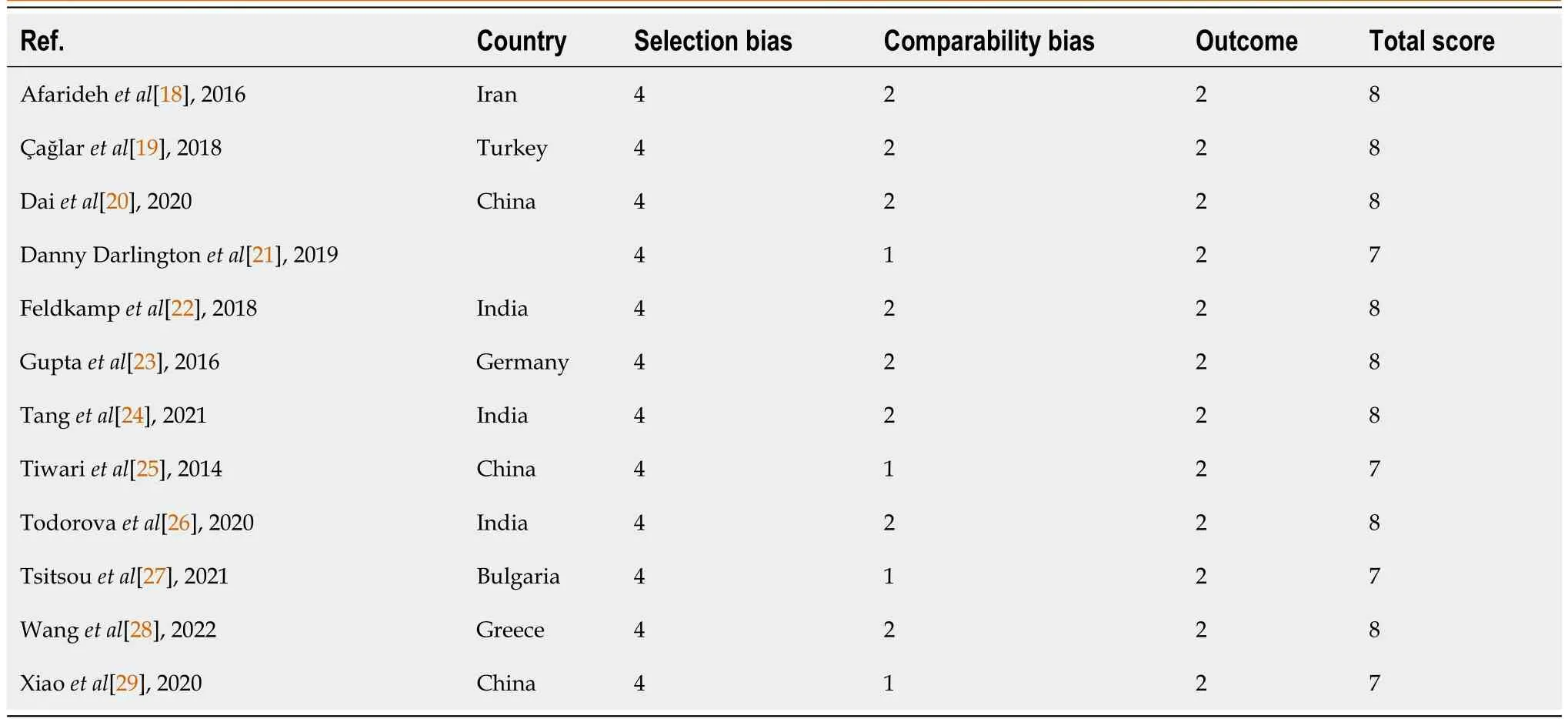
Table 3 Newcastle Ottawa scale risk of bias of the included studies

Figure 1 Vitamin D levels among diabetic patients with and without diabetic foot ulcer.
Vitamin D has been considered a magic bullet and cures many chronic disorders.However, the results were obtained from observational studies.The findings of lower FUs among patients with higher vitamin D may not prove causality.Other confounders might explain the lower vitamin D levels among patients with DFUs including a healthier diet, good exposure to sunlight, and physical activity[37,38].In addition, vitamin D improves glycemic control among patients with diabetes[39,40].Thus, high vitamin D may indirectly protect against DFUs by improving glycemic control.

Figure 2 Vitamin D level among diabetic patients with and without septic foot.
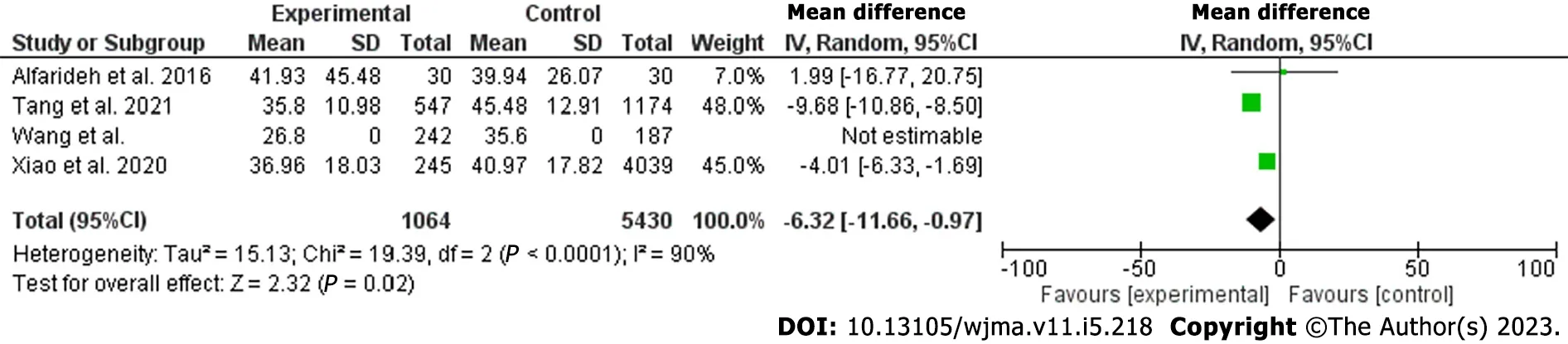
Figure 3 Vitamin D level among diabetic patients with and without septic foot (hepatized).
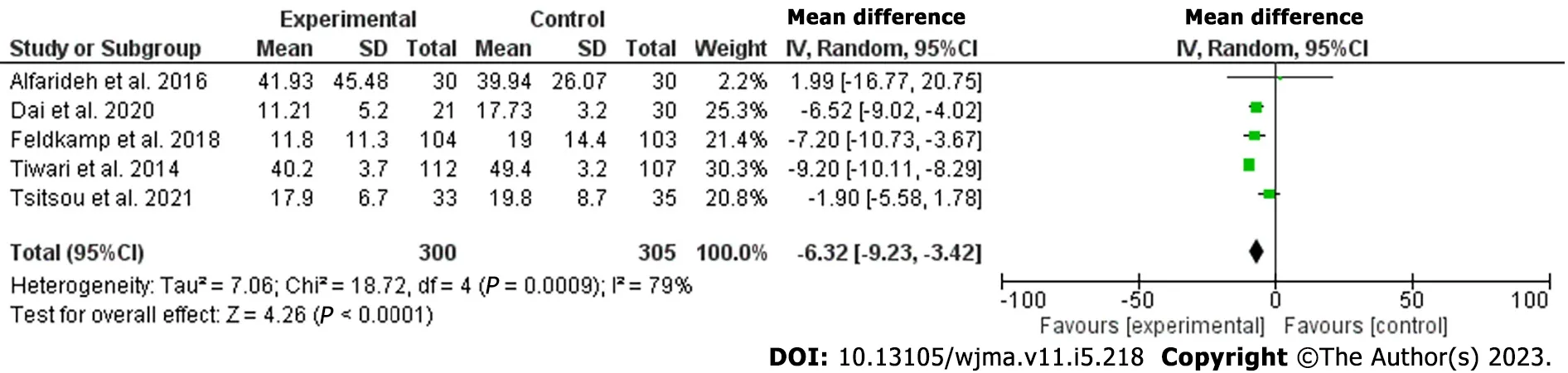
Figure 4 Vitamin D level among diabetic patients with and without septic foot (controlling for age, sex, duration of diabetes, and hemoglobin).
Osteoblasts (bone formation) and osteoclasts (bone resorption) orchestrate bone remodeling.Osteoclasts genesis activation is through receptor activator of tumor necrosis factor (RANK-osteoprotegerin), ultimately leading to osteolysis and destruction of bone tissue.This pathway is of great therapeutic and clinical implications.Medications that influence different levels of RANK-osteoprotegerin are bisphosphonates, calcitonin, and denosumab.Denosumab is encouraging for the treatment of Charcot diabetic foot.However, bisphosphonates have been evaluated recently due to the adverse events.Calcitonin efficacy is limited[41,42].
In this review, some of the included studies were not matched for age, duration of diabetes, duration of diabetes, or HbA1c.The young age of control subjects, their good glycemic control, and the short duration of diabetes might increase their risk of DFUs.
Vitamin D supplementation and diabetic septic foot
Although, the association between low vitamin D levels and diabetic septic foot was documented.However, the effect of vitamin D therapy on DFUs is unclear.In addition, it is not clear if the relationship is correlated or causal[43].A double-blinded randomized controlled trial showed that highdose vitamin D supplementation (170 μg/d) was superior to low doses (20 μg/d) on diabetic ulcer healing[44].A recent review showed that vitamin D improved diabetic septic foot healing, an effect mediated by the remodeling and proliferation of cells involved.In addition, vitamin D suppresses proinflammatory responses, enhances antimicrobial peptides, and enhances anti-inflammatory effects[45].The review by Papaioannou and colleagues, which included 34 studies[46], supported the above findings.A randomized controlled trial published in Asia showed that vitamin D supplementation reduced ulcer length, width, and depth[47].A recent review of the literature concluded that vitamin D supplementation might slow the progression of neural damage.In addition to the adjuvant role in neuropathic pain and cardiovascular autonomic neuropathy among patients with type 2 diabetes[48].
The current meta-analysis strength is that we included observational studies excluding poster presentations, studies published by the same authors, and studies that used the median of vitamin D.The limitation of this study was the substantial heterogeneity.
CONCLUSION
Vitamin D levels were lower among patients with DFUs compared to their counterparts without ulcers.A low level was observed among hospitalized patients.Randomized control trials investigating the association of vitamin D and DFs and assessing the role of vitamin D supplementation are needed.
ARTICLE HIGHLIGHTS

ACKNOWLEDGEMENTS
The author would like to acknowledge the Saudi Digital Library for the free access of the databases.
FOOTNOTES
Author contributions:Mirghani HO contributed to the concept and design, literature search, data analysis and interpretation, and manuscript drafting.
Conflict-of-interest statement:The authors have no conflicts of interest to declare.
PRISMA 2009 Checklist statement:The author has read the PRISMA 2009 Checklist, and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Saudi Arabia
ORCID number:Hyder Osman Mirghani 0000-0002-5817-6194.
S-Editor:Liu JH
L-Editor:Filipodia
P-Editor:Yu HG
 World Journal of Meta-Analysis2023年5期
World Journal of Meta-Analysis2023年5期
- World Journal of Meta-Analysis的其它文章
- Evidence relating cigarette, cigar and pipe smoking to lung cancer and chronic obstructive pulmonary disease: Meta-analysis of recent data from three regions
- Diabetes mellitus: An overview of the types, prevalence, comorbidity, complication, genetics, economic implication, and treatment
- Haploidentical hematopoietic stem cell transplantation as promising therapy in the improved survival of pediatric patients with leukemias and myelodysplasias
- Real-world effectiveness of mRNA COVID-19 vaccines in the elderly during the Delta and Omicron variants: Systematic review
- Pulmonary cytomegalovirus infection: A case report and systematic review
- Advances in the mechanism of action of metformin in pituitary tumors